
Abstract
Background
For nearly half of the period between 1999 and 2019, rates of rural overdose death surpassed those in urban areas. Despite this substantial increase, little attention has been given to rural overdose or the contextual factors that predict risk of fatal overdose in rural vs. urban communities.
Methods
Risk terrain modeling was used to assess 2016–2017 overdose deaths in two urban and two rural Ohio counties. Spatial models incorporated criminal incidents and features of the built environment that have been previously associated with fatal overdose. The efficacy of spatial models was evaluated through the Predictive Accuracy Index (PAI) and Predictive Efficiency Index (PEI*).
Results
Spatial models in rural counties were more influenced by past instances of crime, whereas risk in urban counties was determined by both crime and the built environment. Taken together, models accurately predicted 76% of 2018 overdoses. Rural models were overall more accurate, primarily in the areas predicted as having the highest risk of future overdose deaths. The predictive accuracy and efficiency of rural models varied more than those of urban models.
Conclusions
It is feasible to apply risk terrain modeling to predict fatal overdose in rural areas. Though the underlying contextual risk factors and patterns of predicted risk differ between rural and urban areas, both can be utilized to place treatment and prevention resources more accurately for targeted intervention.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
Introduction
Fatal drug overdoses have been steadily increasing in the United States since 1999 and have surged throughout the COVID-19 pandemic (Hedegaard et al., 2021; National Institute on Drug Abuse, 2022). Widespread efforts to reduce overdose mortality have included naloxone distribution, increased services to persons at risk for fentanyl exposure, and enhanced access to substance use treatment (Wilson et al., 2020). These measures alone, however, have not been sufficient to stem mortality rates as provisional data from the Centers for Disease Control and Prevention (CDC) indicate that the U.S. has recently surpassed 100,000 overdose deaths for the first time in a 12-month period (Centers for Disease Control and Prevention, 2021).
Since the onset of the opioid epidemic, a multitude of contextual risk factors have been consistently associated with overdose locations (Cerda et al., 2013; Galea et al., 2005). Most commonly, these include features of the built environment (Butz & Streetman, 2018; Chichester et al., 2020), the presence of violent crime (Carter et al., 2018) or crime associated with substance use (e.g. possession, distribution, burglaries; (Chen et al., 2022; Ertugrul et al., 2019; Martínez et al., 2008), and neighborhood-level socioeconomic factors (Johnson & Shreve, 2020; Marshall et al., 2019). Taken together, these variables, often in unison with public health data such as opioid dispensing rates and calls for EMS, have enabled more accurate identification of high-risk overdose areas (Bozorgi et al., 2021; Sadler & Furr-Holden, 2019; Sumetsky et al., 2021).
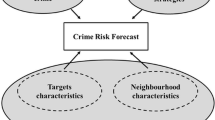
Risk Terrain Modeling (RTM) has emerged as an efficacious geospatial analytic technique for assessing the relationships between a set of theoretically related risk factors and an outcome event to predict high-risk areas (Caplan et al., 2011, 2015; Marchment & Gill, 2021). At the micro, place-level, risky places are formed by a confluence of sociodemographic and environmental factors that, when overlapped, create an environment where crime is ripe to occur (Caplan & Kennedy, 2016). By focusing on specific factors and outcome events to which they are believed to relate, RTM can test their spatial relationships and model areas where outcome events are statistically more likely (Caplan et al., 2015).
RTM has roots in broader environmental criminology, pulling core concepts and theoretical arguments from routine activities theory (Cohen & Felson, 1979) and crime pattern theory (Brantingham & Brantingham, 1993, 1995, 2013). An RTM approach relies on the broad crime generator and attractors (see Marchment and Gill, 2021), along with risky facilities (see Steinman et al. (2021), literature to assist in quantifying risk for outcomes. In short, how different features of the environment co-locate in space could create riskier environments for crime to occur. For instance, a bar by itself and a bus stop by itself could be risky but a bus stop co-located in a shared space as a bar could create an even riskier environment. That is, the combined influence of two criminogenic features creates greater risk than one feature independently. RTM assists in operationalizing and testing for these influences.
To date, RTM has largely been applied to analyzing patterns of crime in urban city centers (Fox et al., 2021; Valasik, 2018). Recent investigations, however, have expanded its use to investigate a range of events including suicide (Lersch, 2020), child maltreatment (Daley et al., 2016), and fatal drug overdose (Chichester et al., 2020; Liu et al., 2023).Footnote 1 A recent systematic review of studies utilizing RTM found that areas identified as high-risk in analyses consistently encapsulated nearly 50% of future outcome events (Marchment & Gill, 2021). In the context of fatal overdose, predicting high-risk areas allows for greater specificity in the allocation of treatment and prevention resources. Further, it highlights the contextual factors that are most closely associated with past outcome events and thus, are expected to be the best predictors of future occurrences.
The contextual risk factors that relate to fatal overdose are not consistent across environments. Within states, county-level differences in overdose trends vary greatly based on conditions such as poverty, unemployment, family instability, and disability rates (Monnat, 2018). Across the U.S., rural and urban regions have also been shown to differ in terms of the socioeconomic and built environmental factors that associate with overdose deaths (Pear et al., 2019; Wagner et al., 2019). This can be expected given the population dispersion, infrastructure, labor markets, and relative size of rural vs. urban areas. These differences have led to barriers in providing adequate treatment and prevention resources to rural regions, which have been among those most impacted by the opioid epidemic (Hedegaard & Spencer, 2021; Palombi et al., 2018), and include extended EMS response times (Gonzalez et al., 2009; Mell et al., 2017), less frequent naloxone administration (Faul et al., 2015; Kilwein et al., 2019), and lack of access to appropriate healthcare (Amiri et al., 2021; Lister et al., 2020; Moody et al., 2017). Given the abundance of structural, commercial, and cultural factors that differentiate rural substance use environments from urban, it is essential to better understand the contextual risk factors that most associate with fatal overdose in each area.
The current study seeks to fill this gap in the literature by adopting a geospatial analytic approach to examining overdose deaths that occurred in Ohio from 2016 to 2017. Like much of Appalachia, Ohio has been disproportionately affected by the opioid epidemic and has consistently ranked among the top U.S. states in overdose death rates (Hall et al., 2019, 2020). Further, through several initiatives such as the Ohio Department of Health’s Violence and Injury Prevention Section, Ohio has come to collect consistent public health data including information on decedents of fatal overdose, overdose contexts, and crime (ODH, 2022; ODPS, 2021). The aims of this study are to: (i) identify high-risk areas in two urban and two rural Ohio counties with high rates of overdose death by assessing the relationship between features of the built environment, locations of criminal incidents, and fatal overdose using Risk Terrain Modeling, (ii) identify the contextual risk factors that convey the greatest spatial influence in areas that are prone to future overdose deaths, (iii) compare contextual risk factors across urban and rural environments, and (iv) assess the efficacy of RTM in predicting actual 2018 overdoses using the Predictive Accuracy Index (PAI) and Predictive Efficiency Index (PEI*).
Methods
Risk Terrain Modeling
RTM is a geospatial analytic approach that operationalizes risk of an outcome event by examining the spatial relationship between past events and a set of theoretically related variables that are thought to confer risk (Caplan et al., 2011, 2015). Using a defined geographic area, RTM generates binary spatial layers for each risk factor that are divided into equal sized cells. Risk values are then assigned to cells based on the proximity and density of risk factors in relation to outcome events. Cells within a specified distance of risk factors or containing a point density of greater than two standard deviations are assigned a value of one. All other cells are given a value of zero. Following this, spatial layers from all included risk factors are combined to produce a composite risk terrain map in which a risk score is calculated for each cell based on the aggregation of individual spatial layers. Higher risk scores are indicative of a greater likelihood of outcome events occurring at that location in the future. Additionally, a relative risk value (RRV) is generated for each risk factor. This value indicates the degree of influence that each variable contributes relative to other factors in the model. In addition to permitting the identification of high-risk contextual factors, RTM allows for the identification of risk variation within a defined geographic area (Daley et al., 2016; Valasik, 2018; Valasik et al., 2019). To assist in the RTM approach, RTMDx, an analytical tool, is used in the current study (further discussed below).
Defining Rurality
The United States Economic Research Service’s 2010 Rural-Urban Commuting Area Codes (RUCA) were used to define rurality. RUCA codes are determined at the census tract-level by accounting for the urbanicity, commuting trends, and population density of a given tract (USDA Economic Research Service, 2020) and have been widely utilized in the literature (Green et al., 2020; Iloglu et al., 2021; Pear et al., 2019). Based on the above characteristics, tracts are designated as metropolitan (1–3), micropolitan (4–6), small town (7–9), or rural (10-10.3; (United States Department of Agriculture, 2019). RUCA codes were assigned to Ohio census tracts and used to determine rurality at the county level. Counties were coded as urban if they were entirely comprised of tracts with metropolitan RUCA codes and rural if they contained only micropolitan, small town, or rural RUCA codes (4-10.3). This is consistent with conventions used by both the U.S. Census Bureau (Ratcliffe et al., 2016) and the U.S. Federal Office of Rural Health Policy (U.S. HRSA, 2021) which define rurality as any territory outside of metro areas.
Study Areas
The current study sought to model risk of fatal overdose at the county level in Ohio. To elucidate urban – rural differences in the contextual risk factors associated with overdose deaths, two urban and two rural counties were selected for analyses. Rates of overdose per 100,000 population were examined per county. Among the five urban and rural counties with the highest rates, those with the highest number of overdoses from 2016 to 2017 were chosen. Priority was given to counties with higher counts of fatal overdoses to test the feasibility of an RTM approach across county types. Additionally, with the smaller units of analysis used in the current study, discussed below, there needs to be an adequate sample size to generate risk models. This resulted in Hamilton and Montgomery counties being selected as the urban areas of focus and Marion and Ross counties as the rural areas. A description of decedent demographics and overdose deaths per county is provided in Table 1.
Data Sources and Preparation
Fatal overdose data for this study were provided by the Ohio Department of Health’s Bureau of Vital Statistics. Accidental fatal overdoses in which any illicit substances were implicated as the primary cause of death statewide from 2016 to 2017 were obtained (N = 7,446). Overdoses at the state level are classified via International Classification of Diseases, Tenth Revision (ICD-10) codes and include cases in which fatal poisonings are attributable to benzodiazepines (T42.4), cocaine (T40.5), psychostimulants (T43.6), heroin (T40.1), natural and semisynthetic opioids (T40.2), methadone (T40.3), or fentanyl and fentanyl analogues (T40.31). Overdoses were geocoded using Esri’s ArcGIS Pro 2.7.0 based on data provided in each decedent’s death certificate. Point of Injury addresses were used as the best approximation of overdose location. Incomplete or invalid addresses led to the removal of 109 cases while a further 681 cases were removed for having overdosed while in a restrictive environment (e.g., healthcare institution, correctional facility, or inpatient substance use treatment). As this study is assessing the contextual risk factors associated with substance use environments, it was determined that overdoses occurring in these settings are not subject to the same environmental influences as those by individuals living unrestrictedly in society. This resulted in 6,656 valid cases across the state, 1,593 of which were contained in the four counties examined in analyses (See Table 1).
To assess the efficacy of RTM in correctly identifying high-risk areas, 2018 fatal overdoses were additionally obtained and prepared in an identical fashion to that described above for 2016–2017 cases. Fifty-seven decedents were removed due to incomplete or missing address data and 495 for having been identified as overdosing while in a restricted environment. Following these exclusions, 4,326 statewide cases remained, and 606 of these fell in the study areas.
Criminal incident data were obtained from the Ohio Department of Public Safety. These data are classified using the FBI’s National Incident-Based Reporting System (NIBRS) and include all incidents in which a crime was reported throughout the state from 2016 to 2017, regardless of whether an arrest was made. Specific crimes were selected for inclusion in analyses based on having been identified in the literature as a spatial risk factor for drug overdose (Carter et al., 2018; Johnson & Shreve, 2020) or substance use behavior (Gorman et al., 2005; Lum, 2008), or for having a theoretical relationship with drug overdose. Included criminal incidents and their associated NIBRS classification can be found in Table 1.
Built environmental variables were obtained from Data Axle, formerly ReferenceUSA and Infogroup, a provider for business and consumer databases containing over 15 million U.S. businesses. Data are classified based on the North American Industry Classification System (NAICS), which contains 96 categories and 317 industry groups (United States Census Bureau, 2020). NAICS is the standard used across all government agencies when classifying business establishments. NAICS data sourced from Infogroup have been widely utilized in the literature and are provided with geospatial data including latitude/longitude coordinates for easy use with geospatial platforms (D’Angelo et al., 2014; Hipp et al., 2019; Lersch, 2017). Categories of built environmental features were included based on having been identified in the literature as a spatial risk factor for fatal overdose (Butz & Streetman, 2018; Chichester et al., 2020) or drug-related crime (Gorman et al., 2005; McCord & Ratcliffe, 2007). This resulted in the selection of fifteen built environmental risk factors, thirteen of which were associated with NAICS identifiers available within Data Axle. These businesses are verified by Data Axle, but it is possible that the business closed/no longer in operation when the outcome event took place. The remaining two variables, public parks and bus stops, were geocoded using RTMDx (discussed below). RTMDx’s geocoding feature executes a successive string of searches using Google Maps data until all instances of the specified variable have been compiled. This data is then accessible for use in RTM analyses within the program. A full description of included built environmental features and criminal incidents, as well as their distribution across the study areas, can be found in Table 1.
Analytic Approach
Prior to aggregating 2016 and 2017 fatal overdose data in RTMDx, average nearest neighbor analyses were conducted to ensure that each county’s dispersion of overdoses occurred in a non-random, clustered pattern. Analyses were carried out using ArcGIS Pro 2.7.0. to determine whether the mean distance between overdose locations is significantly less than that of a randomly generated distribution. Distances between points were calculated using Manhattan distances.
The RTMDx platform was used to carry out RTM analyses. RTMDx is a diagnostic spatial analytic platform developed by the Rutgers Center on Public Security to operationalize the RTM procedure (Caplan et al., 2013). RTMDx requires the determination of several model parameters that guide the program’s execution. First, an aggravating model was utilized as both criminal incidents and built environmental features were expected to have a positive association with fatal overdose. A standard value representative of two city block lengths (1,320 ft) was selected, defining the distance at which the spatial influence of risk factors is assessed. Risk factors were assigned a standard value multiplier of three, leading the proximity of each to be tested for significance at two, four (2,640 ft), and six (3,960 ft) block increments. Variables were assessed by both proximity and density. In short, this procedure tests whether being in close proximity to a factor is risky or the density of a factor in space is risky. Finally, the spatial analysis unit, or place size, was set to 660 by 660 ft, defining the grid cell size into which spatial layers were divided. The total number of cells generated for each model is listed in Table 2.
Using the specified parameters, RTMDx assesses the spatial influence of risk factors on locations of fatal overdose sequentially at each operationalization specified in the above steps to determine a best fitting model. This is accomplished using an elastic net penalized regression model to select variables which are then fit to a Poisson regression (Caplan et al., 2015). A cross-validation procedure selects variables with a non-zero coefficient for inclusion in the penalized model. Selected factors are incorporated in a bidirectional stepwise regression to determine the model with the lowest Bayesian information criterion (Fox et al., 2021). After the final model is determined, coefficients for the remaining variables are then rescaled and applied as RRVs (Lersch, 2020). Additionally, a grid cell overlay of the study area is produced indicating the relative risk score (RRS) of each cell. These scores are akin to odds ratios as cells with the lowest predicted likelihood of future overdose are assigned a value of one.
Finalized risk terrain maps included a mean RRS (M) value and the standard deviation of RRS values (SD) in the aggregate map. These values were then used to derive tiers of anticipated risk for each county ranging from mild risk (M to M + 1 SD), to moderate risk (M + 1 SD to M + 2 SD), and high risk (greater than M + 2 SD) areas. The number of actual 2018 fatal overdoses in each county was then examined to determine the accuracy with which overdoses were predicted at each level of risk.
Following the methodology used by the National Institute of Justice in their crime forecasting challenge (NIJ, 2017), to examine RTM’s efficacy in the current study, the Predictive Accuracy Index (PAI; (Chainey et al., 2008) and Predictive Efficiency Index (PEI*; (Hunt, 2016) were used. The PAI is calculated by (n/N)/(a/A), where n is the number of correctly predicted events within a specific risk category over the total N of events. The numerator is often described as the hit rate but does not take into account the area, hence the denominator. The denominator represents the area of a specific risk category divided by the total area. The final PAI value can be interpreted in comparison to one another by identifying the higher value as being more accurate. While the PAI is designed as a metric for comparison to identify approach accuracy, it does not assess how well an approach could have predicted events. In short, the PAI identifies the accuracy level while PEI* identifies how efficient the model was in predicting events. The PEI* compares the predictive success of the model to how well the model could have theoretically predicted cases in the number of cells it included (Hunt, 2016). Values closer to one indicate more efficiency. To calculate PEI*, PAI is divided by PAI*, where PAI is the original calculated value and PAI* represents the maximum possible PAI. The resulting value ranges from zero to one. As PEI* approaches 1, the more efficient that approach is for predicting events.
Results
Results from average nearest neighbor analyses indicated that fatal overdoses in each county were significantly clustered (ps < 0.01), supporting the aggregation of overdose deaths from 2016 to 2017 in RTM analyses. RTMDx identified the best-fitting model for each county as a Negative Binomial Type II model other than for Marion County, which was fit to a Poisson model.
Figures 1 and 2 depict the composite risk maps for the urban study areas (Hamilton and Montgomery counties, respectively). The relative risk scores of each cell were determined from the Negative Binomial model. The map of Hamilton County details 1,257 cells that were identified as high risk (RRS > 35.96), 4.68% of the total study area. These high-risk areas comprise two predominant clusters, the first of which stretches north and northeast of Downtown Cincinnati and includes the neighborhoods of West End, Over-the-Rhine, Mount Auburn, Corryville, Walnut Hills, Evanston, and Avondale. The second extends west of the city and includes large portions of East and West Price Hill. These areas, as well as others depicted as high-risk in Fig. 1, have at least a 36 times greater risk of future overdose deaths than those containing no risk factors. Similarly, the composite map of Montgomery County yielded 1,344 high-risk cells (RRS > 39.23) which accounted for 4.47% of the study area and centered in two broad regions. The first of these includes a portion of Downtown Dayton and much of East Dayton, Twin Towers, Walnut Hills, Linden Heights, Belmont, and Hearthstone. The second covers neighborhoods north of the city and west of the Stillwater River including Old Dayton, Five Oaks, Riverdale, Mt. Vernon, Santa Clara, Hillcrest, and North Riverdale. Results detailing the composite risk maps generated for the study areas can be found in Table 2.

Composite risk terrain map of Hamilton County, Ohio (urban area)

Composite risk terrain map of Montgomery County, Ohio (urban area)
RTMDx identified nine variables as conveying significant risk for overdose deaths in Hamilton County. Cells within a two-city block distance of aggravated assaults saw the highest increase in risk, 2.25 times that of cells with no risk factors present. This was followed by density of burglaries or breaking and entering (RRV = 2), proximity to schools (RRV = 1.96), and proximity to robberies (RRV = 1.90). Additional risk factors, in order of decreasing RRVs, included hotels and motels, locations of vehicle theft, gas stations, convenience stores, and bars. In the final model for Montgomery County, ten variables were revealed as significant risk factors. Being within a two-block proximity to drug and narcotics violations contributed the highest relative risk, 2.53 times that of cells outside the influence of nearby risk factors. Density of burglaries was again the second-most weighted factor in the model (RRV = 2.23), followed by proximity to schools (RRV = 1.89), and proximity to bars (RRV = 1.81). Remaining factors included locations of aggravated assault, vehicle theft, murder or nonnegligent manslaughter, apartments, gas stations, and public parks. Significant spatial risk factors from each study area, including their RRV, operationalization, and spatial influence can be found in Table 2.
Figures 3 and 4 respectively illustrate the composite risk maps for Marion and Ross counties, the rural study areas. Marion County had 321 high-risk cells, only 1.22% of the overall study area. The predominant risk cluster centered in Downtown Marion, spanning north, south, and west of the city. Outside of the Marion city limits, few areas in the county were predicted as risky places save New Bloomington, which was found to have medium risk. In Ross County, 470 (1.04%) of the 45,003 cells that comprised the composite risk map were found to be high-risk. These registered as one central area that included Downtown Chillicothe as well as the area immediately west and northwest of the city center. A scattering of smaller towns in the county were also designated as high-risk including Bainbridge, Richmond Dale, Clarksburg, and Kingston.

Composite risk terrain map of Marion County, Ohio (rural area)

Composite risk terrain map of Ross County, Ohio (rural area)
RTMDx revealed three spatial risk factors as significantly contributing to future risk of fatal overdose in each of the rural models. In Marion County, two-block proximity to incidents of drunkenness carried a Relative Risk Value of 42.61. Additionally, density of murder or nonnegligent manslaughter (RRV = 11) and proximity to bars (RRV = 3.14) were found to be significant spatial risk factors. In Ross County, being within a two-block distance to areas with a high density of burglaries carried the highest risk (RRV = 19.38). Following this was density of vehicle theft (RRV = 7.99) and proximity to murder or nonnegligent manslaughter (RRV = 4.22).
Table 3 illustrates the distribution of 2018 fatal overdoses across the study areas and the number of cases that fell into RTM-predicted risk areas. Considering the urban study areas, in Hamilton County, 258 of the county’s 340 overdoses occurred in mild – high risk areas, roughly 76% of cases. Regions identified as risky by RTM occupied 21% of the total Hamilton County land area. Results for Montgomery County followed a similar pattern. Of the 2018 overdoses in the county, 165 (76%) were accurately predicted by RTM in 17% of the county’s land area. Differing though, were the percentage of cases that fell within the high vs. mild-risk areas. In Montgomery County, 47% of 2018 overdose deaths took place in high-risk areas while only 16% occurred in mild-risk areas. This opposed to Hamilton County, which had rates of 36% and 25% in the same areas, respectively. Notably, the high-risk area of the Montgomery County risk terrain map occupied only 4% of the county, meaning that nearly half of its 2018 overdoses were accounted for in an area roughly one-third the size of the city of Dayton. By comparison, only half of Hamilton County’s overdoses were covered between its high- and moderate-risk areas, which together comprised 8% of the total county area. This is reflected in the notably higher PAI associated with Montgomery County’s high-risk region, which was both more accurate and more efficient in its predictions of overdose deaths than the high-risk area of Hamilton County.
In Marion County, of the 19 overdose deaths that occurred throughout this rural county in 2018, 18 (95%) fell within RTM-predicted risky areas. Twelve of these (63%) took place in the high-risk area, which occupied only 1% of the total county landmass, and the remaining 6 were in mild-risk regions. Twenty-nine fatal overdoses occurred in Ross County in 2018, 59% of which took place in risk areas identified in risk terrain models. The PAI and PEI* of Marion County’s high- and mild-risk areas surpassed that of Ross County.
Discussion
The present study utilized risk terrain modeling to assess fatal drug overdoses occurring in two urban and two rural Ohio counties between 2016 and 2017. Spatial models identifying risky areas and significant, risk-conveying variables were developed by examining the relationship between past overdose deaths and contextual risk factors. Models were then compared to the distribution of actual 2018 overdose deaths to determine the accuracy (Predictive Accuracy Index; PAI) and efficiency (Predictive Efficiency Index; PEI*) with which RTM predicted risk of future overdose. Consistent with reports from a recent meta-analysis reviewing RTM’s effectiveness (Marchment & Gill, 2021), areas indicated as moderate- or high-risk across models accurately predicted 54% of future cases. With the inclusion of areas determined to be mildly risky, the total hit rate reached 76%. While these rates are broadly in line with the literature, the primary aim of the current study was to extend the application of RTM to rural environments to better understand and prevent fatal overdose in these communities while also comparing results to urban areas, which have historically been the focus of this methodology. Along these lines, two broad patterns emerged in the results.
The first relates to the factors identified by RTMDx as being significant predictors of overdose risk. In both urban counties (Hamilton and Montgomery), locations of criminal incidents and features of the built environment, the two categories of risk factors examined in this study, were equally represented in the results. There was notable overlap across the urban models with aggravated assault, burglary and breaking and entering, vehicle theft, bars, gas stations, and schools identified as significant in each. On the other hand, in Marion and Ross County, with the exception of bars, only variables in the criminal incident category were found to be significant in rural study areas. Murder and nonnegligent manslaughter was the only variable present in both models. Additional risk factors included burglary and breaking and entering, drug and narcotics violations, and vehicle theft. These results indicate that built environmental factors played a minimal role in shaping the risk terrain maps of the rural study areas. However, in the urban study areas, they were more numerous than criminal incidents, though less weighted in terms of relative risk values.
This pattern may be partially explained by extant research examining the differing role of social factors in rural versus urban communities. For one, rural societies have been shown to have stronger social kinship networks with greater reliance on their communities as compared to their urban counterparts (Beggs et al., 1996; Hofferth & Iceland, 1998; Turcotte, 2005). Higher social support has been identified as a buffer against deleterious mental health outcomes for persons living in rural communities (Crowell et al., 1986; Letvak, 2002; McCulloch, 1995). Rural kinship ties are so close in fact that they have played a significant role in the proliferation of prescription drug misuse due to diversion to friends and family members (Jonas et al., 2012; Keyes et al., 2014). This body of research highlights the ways in which tight-knit social networks can shape patterns of behavior and health in rural communities. By extension, it may be that crime ruptures that societal fabric in a more consequential manner in rural than in urban areas, affecting not only those immediately impacted by crime but also the social structure as a whole. As such, instances of murder, vehicle theft, drunkenness, or burglary, though not a uniquely rural phenomenon, may create a heightened vulnerability to overdose due to the rural context within which they are occurring.
Compared to rural areas, urban environments also have a broader, more complex intersectionality of factors that account for the social disorganization underlying overdose deaths. As indicated in this study, built environmental features, which may be categorized as crime generators or crime attractors (Kinney et al., 2008; Ratcliffe, 2012), played a significant role in creating the urban microenvironments that are at risk for future overdose deaths. This is consistent with a recent study of Miami-Dade County in which public parks, bus stops, schools, and additional community features were found to significantly relate to fatal drug overdose locations (Liu et al., 2023). Schools and parks, for instance, may be thought of as crime generators given that crime is more likely due to the large volume of people that they service. Conversely, bars may be more likely to attract crime because aspects of the environment present unique opportunities for it (e.g., due to drunken patrons; (Tillyer et al., 2021). Given the expansive infrastructure of urban areas, more places with overlapping or closely clustered generators and attractors exist. It may hold that rural communities, and even micropolitan cities, simply lack the built environmental framework to breed a high-risk environment based on these features alone. This indicates that factors beyond the physical or commercial features of a community are accounting for susceptibility to overdose in rural areas.
Though relatively few studies have begun identifying the spatial factors that convey risk for fatal overdose, it is unlikely that extended research in this area will yield a set of specific variables that are consistent across counties, states, or regions, whether rural or urban. When examining contextual factors that are associated with crime generally in rural areas, there is little consistency across settings and time (Arthur, 1991; Bouffard & Muftic, 2006; Kaylen & Pridemore, 2013; Li, 2011; Osgood & Chambers, 2000; Ward et al., 2018). Though less studied, the findings regarding the impact of variables such as socioeconomic factors on rural overdose deaths have been discrepant, even within the state of Ohio alone (Headley Konkel & Hoffman, 2020; Hernandez et al., 2020; Park et al., 2019; Pear et al., 2019). Contextual factors have also been shown to be worse predictors of rural crime than urban (Wells & Weisheit, 2004). Attempts to broadly categorize these relationships are made difficult by the nuances of varying population, community, and socioeconomic conditions at the neighborhood level, as alluded to by Wagner et al. (2019) in their study of neighborhood variation in fatal overdose rates in Delaware. For the purposes of spatial risk modeling, however, it may be more important to understand the classes of factors that are associated with overdose in rural or urban contexts rather than specific variables or their directionality. For instance, a prior study by the authors compared rural and urban regions of Jefferson County, AL using RTM and included only features of the built environment and indicators of community degradation (e.g., 311 calls for service) as risk factors (Chichester et al., 2020). While the variables identified as significant in that study may be relevant to understanding the overdose context of Jefferson County, they had little overlap with the built environmental features identified in the present study as conveying risk for overdose in Ohio counties. More importantly, the present study emphasized that built environmental features as a whole remain important risk factors in anticipating overdose in urban but not rural settings. Continuing to identify the classes of variables that convey risk for overdose in each setting will be essential to the extension of spatial risk modeling across counties and states.
The second pattern noted in the results relates to the proportion of actual 2018 overdoses correctly predicted in rural and urban counties across the three tiers of risk modeled in this study. Hamilton and Montgomery County were found to have consistent hit rates, with risk terrain models accounting for 76% of future overdoses in each. This was accomplished, though, by labeling relatively large portions of the total county area as risky, 21% and 17% respectively. With the overall goal of more efficiently directing limited treatment and prevention resources, covering the entirety of these areas allows fewer opportunities for targeted intervention. However, in considering only the cells identified as moderate- or high-risk, 50–60% of 2018 fatal overdoses were captured in just 7–8% of the county areas. This is reflected in the PEI* of the high-risk areas in urban models. In both counties, high-risk regions were more than twice as efficient in capturing 2018 overdoses compared to moderate risk areas, in addition to being more accurate.
The final risk terrain maps for Marion and Ross County also had several commonalities. The high-risk areas of each were most predictive of future overdose deaths with a smaller portion accounted for in areas identified as mildly at risk. Neither rural RTM correctly predicted overdoses in moderate-risk areas; however, between both models, these areas accounted for only 0.2% of total cells. There was a larger difference in overall hit rate when comparing Marion and Ross County versus Hamilton and Montgomery. However, when averaged, rural rates were at parity with urban. The most notable rural-urban difference was in the number of cells required to produce this result. The PAI of both rural models was 2–6 times that of urban models. Further, the high-risk area of Marion County was the region with the greatest efficiency across models. Though they experienced far fewer overdose deaths, rural RTMs were highly specific in their predictions, needing only 4–5% of the county area to account for a collective 76% of future overdose deaths. For this reason, it may be more effective to consider resource allocation within the entirety of at-risk cells in rural RTM maps but more efficient to target only those with moderate to high risk in urban models.
These findings have significant implications in considering the ways in which RTM can inform overdose prevention practices at the county level. For one, it presents preliminary data toward the feasibility and accuracy of RTM as an efficacious method to anticipate overdose deaths in rural settings. Though far less populous than urban environments, rural areas housed 14% of the country’s population in 2021, roughly 46 million people (Dobis et al., 2021). In 2019, their age-adjusted rate of overdose was 19.6 per 100,000 persons, only 2.4 lower than urban areas (Hedegaard & Spencer, 2021). Overdose deaths in rural communities have been exacerbated by a dearth of buprenorphine providers (DeFlavio et al., 2015; Weintraub et al., 2018), poor naloxone access (Guy et al., 2019; Tofighi et al., 2021), and extended EMS response times (Gonzalez et al., 2009; Keeffe et al., 2011). In addition to directing the placement of county naloxone distribution sites, geospatial methods such as RTM can be used to identify chain pharmacies in high-risk areas that may be used for provisioning naloxone (Banerjee, 2020). This may be especially fruitful when these efforts consider the locations of prior naloxone administrations which have been shown to cluster significantly, even in rural areas (Thurston & Freisthler, 2020). Studies have also shown the potential for improved EMS responses and quicker response times through geospatially informed models (Merchant et al., 2006; Peleg & Pliskin, 2004). Though less problematic in urban areas, the same methods can be utilized and may be considered for other overdose prevention or public health initiatives, such as needle exchange programs, locations of fentanyl test strips, general psychoeducation initiatives, or more recently, safe injection sites (Gordon, 2022).
The current study is not without limitations. For one, the use of methodologies such as RTM in a defined area such as a county boundary ignores the influence of surrounding regions and, thus, does not fully account for the influence of all contextual factors. Further, RTM is reliant on data obtained from state and county officials. The accuracy of this data, especially death certificate data related to fatal overdose, can vary substantially across the country and even within states (Slavova et al., 2019; Warner et al., 2013). Also, it is possible that discrepancies exist between the time when overdoses occurred, and the closing of new businesses as reported in Data Axle’s 2018 dataset used for this study. These businesses are verified by Data Axle, but it is possible that some businesses had ceased operating during the 2016–2017 period during which we examined overdose deaths and were thus not captured in the built environmental dataset we obtained. Despite this, county models had a hit-rate greater to or at parity with prior studies using RTM (Marchment & Gill, 2021; Valasik, 2018; Valasik et al., 2019). Finally, the use of RTMDx necessitates the specification of model parameters that guide the formation of spatial layers and ultimately the composite risk maps for each county. While there is an ample literature base informing the ideal parameters for urban settings (Caplan et al., 2011, 2015), there is little prior research guiding the application of this methodology to rural areas. For this study, the authors chose to maintain the same model parameters between both rural and urban settings; however, altering the standard value or place size would likely influence the factors found to be significant and the distribution of at-risk cells. This can be observed in comparing the results presented herein to prior studies focusing exclusively on city centers. Li et al. (2019), for instance, assessed heroin-related emergency calls in the city of Cincinnati at the block group level and noted significant built environmental features, such as public parks, that were not found to be significant risk factors in our model for Hamilton County. Though sensitivity analyses were not conducted, prior investigations by the authors have shown RTM results to be robust to variations in model parameters at the county level. However, as noted above, further research is required to determine how the scope of the study area may impact variable relationships and how model parameters should be adapted in turn.
The results of the current study emphasize the potential for spatial risk models being an efficacious strategy for anticipating areas at risk for future overdose deaths in both rural and urban communities. The data leveraged to generate risk models in this study are commonly maintained by county officials, making the annual production of such models low cost and low effort. Future studies applying RTM to counties across various states and regions will continue to shed light on the classes of variables that are associated most with fatal overdose and whether these broad categories are consistent across contexts. In sections of the study areas that were predominately identified as high risk, such as Downtown Cincinnati, future studies may be able to identify even greater variation in risk by focusing on specific city centers or neighborhoods. This may be accomplished by expanding the scope of analysis to include decedent demographic variables and markers of environmental degradation such as 311 calls for service (Li et al., 2019, 2020).
To our knowledge, this study was the first to assess whether rural RTMs are accurate predictors of future overdose. Further inquiries in this area will elucidate whether the hit-rates found in this investigation replicate to other areas and whether PAI and PEI* rates remain consistent. Future studies comparing RTM to other traditionally used geospatial methodologies such as hotspot analysis or kernel density estimation will aid in determining the approach that most comprehensively predicts future overdose cases.
Notes
The current study does not delve into the differences in spatial approaches to predict crime. There are numerous approaches to spatially predicting crime with prior studies focusing on comparisons. This is beyond the scope but there is extant literature on comparing approaches on the predictive ability (see e.g., Drawve, 2016; Ohyama & Amemya, 2018; Wheeler and Steenbeek, 2021) along with NIJ’s Crime Forecasting Challenge in general.
References
Amiri, S., McDonell, M. G., Denney, J. T., Buchwald, D., & Amram, O. (2021). Disparities in Access to Opioid Treatment Programs and Office-Based Buprenorphine Treatment across the Rural-Urban and Area Deprivation Continua: A US Nationwide Small Area Analysis. Value in Health, 24(2), 188–195. https://doi.org/10.1016/j.jval.2020.08.2098.
Arthur, J. A. (1991). Socioeconomic predictors of crime in rural Georgia. Criminal Justice Review, 16(1), 29–41. https://doi.org/10.1177/073401689101600106.
Banerjee, S. (2020). Optimizing the distribution of pharmacy-dispensed Naloxone using spatial mapping techniques in rural areas. Journal of Drug Issues, 50(4), 604–612. https://doi.org/10.1177/0022042620945673.
Beggs, J. J., Haines, V. A., & Hurlbert, J. S. (1996). Revisiting the rural-urban contrast: Personal networks in Nonmetropolitan and Metropolitan Settings1. Rural Sociology, 61(2), 306–325. https://doi.org/10.1111/j.1549-0831.1996.tb00622.x.
Bouffard, L., & Muftic, L. (2006). The rural mystique: Social Disorganization and Violence beyond Urban Communities. Western Criminology Review, 7.
Bozorgi, P., Porter, D. E., Eberth, J. M., Eidson, J. P., & Karami, A. (2021). The leading neighborhood-level predictors of drug overdose: A mixed machine learning and spatial approach. Drug and Alcohol Dependence, 229, 109143. https://doi.org/10.1016/j.drugalcdep.2021.109143.
Brantingham, P. L., & Brantingham, P. J. (1993). Nodes, paths and edges: Considerations on the complexity of crime and the physical environment. Journal of Environmental Psychology, 13(1), 3–28.
Brantingham, P., & Brantingham, P. (1995). Criminality of place: Crime generators and crime attractors. Eur. J. on Crim (3 vol., p. 5). Pol’y & Rsch.
Brantingham, P., & Brantingham, P. (2013). Crime pattern theory. In Environmental criminology and crime analysis (pp. 100–116). Willan.
Butz, J., & Streetman, A. (2018). Predicting spatial risk of Opioid Overdoses in Providence, RI (Predicting spatial risk of Opioid Overdoses in Providence. RI.
Caplan, J. M., & Kennedy, L. W. (2016). Risk terrain modeling: Crime prediction and risk reduction. Univ of California Press.
Caplan, J. M., Kennedy, L. W., & Miller, J. (2011). Risk terrain modeling: Brokering Criminological Theory and GIS methods for crime forecasting. Justice Quarterly, 28(2), 360–381. https://doi.org/10.1080/07418825.2010.486037.
Caplan, J. M., Kennedy, L. W., & Piza, E. L. (2013). Risk terrain modeling diagnostics utility user manual (version 1.0). Rutgers Center on Public Security.
Caplan, J. M., Kennedy, L. W., Barnum, J. D., & Piza, E. L. (2015). Risk Terrain Modeling for Spatial Risk Assessment Cityscape, 17(1), 7–16. http://www.jstor.org/stable/26326918.
Carter, J. G., Mohler, G., & Ray, B. (2018). Spatial concentration of opioid overdose deaths in Indianapolis: An application of the Law of Crime Concentration at Place to a Public Health Epidemic. Journal of Contemporary Criminal Justice, 35(2), 161–185. https://doi.org/10.1177/1043986218803527.
Centers for Disease Control and Prevention (2021). Drug Overdose Deaths in the U.S. Top 100,000 Annually. National Center for Health Statistics Pressroom Retrieved from https://www.cdc.gov/nchs/pressroom/nchs_press_releases/2021/20211117.htm.
Cerda, M., Ransome, Y., Keyes, K. M., Koenen, K. C., Tardiff, K., Vlahov, D., & Galea, S. (2013). Revisiting the role of the urban environment in substance use: The case of analgesic overdose fatalities. American Journal of Public Health, 103(12), 2252–2260. https://doi.org/10.2105/ajph.2013.301347.
Chainey, S., Tompson, L., & Uhlig, S. (2008). The utility of Hotspot Mapping for Predicting spatial patterns of crime. Security Journal, 21(1), 4–28. https://doi.org/10.1057/palgrave.sj.8350066.
Chen, Q., Sterner, G., Segel, J., & Feng, Z. (2022). Trends in opioid-related crime incidents and comparison with opioid overdose outcomes in the United States. International Journal of Drug Policy, 101, 103555. https://doi.org/10.1016/j.drugpo.2021.103555.
Chichester, K., Drawve, G., Giménez-Santana, A., Sisson, M., McCleskey, B., Dye, D. W., Walker, J., Mrug, S., & Cropsey, K. (2020). Pharmacies and features of the built environment associated with opioid overdose: A geospatial comparison of rural and urban regions in Alabama, USA. International Journal of Drug Policy, 79, 102736. https://doi.org/10.1016/j.drugpo.2020.102736.
Cohen, L. E., & Felson, M. (1979). Social change and crime rate trends: A routine activity approach (pp. 588–608). American sociological review.
Crowell, B. A., George, L. K., Blazer, D., & Landerman, R. (1986). Psychosocial risk factors and Urban/Rural differences in the prevalence of Major Depression. British Journal of Psychiatry, 149(3), 307–314. https://doi.org/10.1192/bjp.149.3.307.
D’Angelo, H., Fleischhacker, S., Rose, S. W., & Ribisl, K. M. (2014). Field validation of secondary data sources for enumerating retail tobacco outlets in a state without tobacco outlet licensing. Health & Place, 28, 38–44. https://doi.org/10.1016/j.healthplace.2014.03.006.
Daley, D., Bachmann, M., Bachmann, B. A., Pedigo, C., Bui, M. T., & Coffman, J. (2016). Risk terrain modeling predicts child maltreatment. Child Abuse and Neglect, 62, 29–38. https://doi.org/10.1016/j.chiabu.2016.09.014.
DeFlavio, J. R., Rolin, S. A., Nordstrom, B. R., & Kazal, L. (2015). Analysis of barriers to adoption of buprenorphine maintenance therapy by family physicians. Rural and Remote Health, 15(1), [93]-[103].
Dobis, E. A., Krumel, T. P., Cromartie, J., Conley, K. L., Sanders, A., & Ortiz, R. (2021). Rural America at a glance: 2021 edition.
Ertugrul, A. M., Lin, Y. R., & Temizel, T. (2019). T. CASTNet: Community-Attentive Spatio-Temporal Networks for Opioid Overdose Forecasting.
Faul, M., Dailey, M. W., Sugerman, D. E., Sasser, S. M., Levy, B., & Paulozzi, L. J. (2015). Disparity in naloxone administration by emergency medical service providers and the burden of drug overdose in US rural communities. Am J Public Health 105 Suppl, (3), e26–32. https://doi.org/10.2105/AJPH.2014.302520.
Fox, B., Trolard, A., Simmons, M., Meyers, J. E., & Vogel, M. (2021). Assessing the Differential Impact of Vacancy on Criminal violence in the City of St. Louis, MO. Criminal Justice Review, 46(2), 156–172. https://doi.org/10.1177/0734016821996795.
Galea, S., Rudenstine, S., & Vlahov, D. (2005). Drug use, misuse, and the urban environment. Drug and Alcohol Review, 24(2), 127–136. https://doi.org/10.1080/09595230500102509.
Gonzalez, R. P., Cummings, G. R., Phelan, H. A., Mulekar, M. S., & Rodning, C. B. (2009). Does increased emergency medical services prehospital time affect patient mortality in rural motor vehicle crashes? A statewide analysis. The American Journal of Surgery, 197(1), 30–34. https://doi.org/10.1016/j.amjsurg.2007.11.018.
Gordon, E. (2022). 51. What’s Next for Safe Injection Sites in Philadelphia? Syringe Exchange Programs and the opioid epidemic (p. 186). Government and Nonprofit Practices and Policies.
Gorman, D. M., Zhu, L., & Horel, S. (2005). Drug ‘hot-spots’, alcohol availability and violence. Drug and Alcohol Review, 24(6), 507–513. https://doi.org/10.1080/09595230500292946.
Green, T. C., Bratberg, J., Baird, J., Burstein, D., Lenz, K., Case, P., Walley, A. Y., & Xuan, Z. (2020). Rurality and differences in pharmacy characteristics and community factors associated with provision of naloxone in the pharmacy. International Journal of Drug Policy, 85, 102602. https://doi.org/10.1016/j.drugpo.2019.11.010.
Guy, G. P. Jr., Haegerich, T. M., Evans, M. E., Losby, J. L., Young, R., & Jones, C. M. (2019). Vital signs: Pharmacy-based Naloxone Dispensing - United States, 2012–2018. MMWR Morbidity and Mortality Weekly Report, 68(31), 679–686. https://doi.org/10.15585/mmwr.mm6831e1.
Hall, O. T., Hall, O. E., McGrath, R. P., & Haile, Z. T. (2019). Years of life lost due to opioid overdose in Ohio: Temporal and Geographic patterns of excess mortality. Journal of Addiction Medicine. https://doi.org/10.1097/adm.0000000000000554.
Hall, O. T., Hall, O. E., Kolodny, A., Teater, J., & McGrath, R. P. (2020). Assessment of excess mortality Associated with Drug Overdose in Ohio from 2009 to 2018. JAMA Network Open, 3(4), e202183–e202183. https://doi.org/10.1001/jamanetworkopen.2020.2183.
Headley Konkel, R., & Hoffman, C. Y. (2020). Immediate and Neighborhood Contextual Effects on Intentional, Accidental, and fatal drug overdoses in a non-urban jurisdiction. Deviant Behavior, 1–18. https://doi.org/10.1080/01639625.2020.1756457.
Hedegaard, H., & Spencer, M. R. (2021). Urban–rural differences in Drug Overdose Death Rates, 1999–2019. Centers for Disease Control and Prevention.
Hedegaard, H., Spencer, M. R., Miniño, A. M., & Warner, M. (2021). Drug Overdose Deaths in the United States, 1999–2020. National Center for Health Statistics Data Brief: Centers for Disease Control and Prevention Retrieved from https://www.cdc.gov/nchs/products/databriefs/db428.htm.
Hernandez, A., Branscum, A. J., Li, J., MacKinnon, N. J., Hincapie, A. L., & Cuadros, D. F. (2020). Epidemiological and geospatial profile of the prescription opioid crisis in Ohio, United States. Scientific Reports, 10(1), 4341. https://doi.org/10.1038/s41598-020-61281-y.
Hipp, J. R., Williams, S. A., Kim, Y. A., & Kim, J. H. (2019). Fight or flight? Crime as a driving force in business failure and business mobility. Social Science Research, 82, 164–180. https://doi.org/10.1016/j.ssresearch.2019.04.010.
Hofferth, S. L., & Iceland, J. (1998). Social capital in rural and urban communities 1. Rural Sociology, 63(4), 574–598.
Hunt, J. M. (2016). Do crime hot spots move? Exploring the effects of the modifiable areal unit problem and modifiable temporal unit problem on crime hot spot stability. American University.
Iloglu, S., Joudrey, P. J., Wang, E. A., Thornhill, T. A., & Gonsalves, G. (2021). Expanding access to methadone treatment in Ohio through federally qualified health centers and a chain pharmacy: A geospatial modeling analysis. Drug and Alcohol Dependence, 220, 108534. https://doi.org/10.1016/j.drugalcdep.2021.108534.
Johnson, L. T., & Shreve, T. (2020). The ecology of overdose mortality in Philadelphia. Health & Place, 66, 102430. https://doi.org/10.1016/j.healthplace.2020.102430.
Jonas, A. B., Young, A. M., Oser, C. B., Leukefeld, C. G., & Havens, J. R. (2012). OxyContin® as currency: OxyContin® use and increased social capital among rural Appalachian drug users. Social Science & Medicine, 74(10), 1602–1609. https://doi.org/10.1016/j.socscimed.2011.12.053.
Justice, N. I. (2017). Real-Time Crime Forecasting Challenge Posting. https://nij.ojp.gov/funding/real-time-crime-forecasting-challenge-posting#noteReferrer2.
Kaylen, M. T., & Pridemore, W. A. (2013). Social Disorganization and Crime in Rural Communities: The First Direct Test of the systemic model. The British Journal of Criminology, 53(5), 905–923. https://doi.org/10.1093/bjc/azt031.
Keeffe, C., Nicholl, J., Turner, J., & Goodacre, S. (2011). Role of ambulance response times in the survival of patients with out-of-hospital cardiac arrest. Emergency Medicine Journal, 28(8), 703. https://doi.org/10.1136/emj.2009.086363.
Keyes, K. M., Cerdá, M., Brady, J. E., Havens, J. R., & Galea, S. (2014). Understanding the rural–urban differences in nonmedical prescription opioid use and abuse in the United States. American Journal of Public Health, 104(2), e52–e59. https://doi.org/10.2105/ajph.2013.301709.
Kilwein, T. M., Wimbish, L. A., Gilbert, L., & Wambeam, R. A. (2019). Practices and concerns related to naloxone use among emergency medical service providers in a rural state: A mixed-method examination. Preventive Medicine Reports, 14, 100872. https://doi.org/10.1016/j.pmedr.2019.100872.
Kinney, J. B., Brantingham, P. L., Wuschke, K., Kirk, M. G., & Brantingham, P. J. (2008). Crime attractors, generators and detractors: Land use and urban crime opportunities. Built Environment, 34(1), 62–74.
Lersch, K. M. (2017). Risky places: An analysis of carjackings in Detroit. Journal of Criminal Justice, 52, 34–40. https://doi.org/10.1016/j.jcrimjus.2017.07.011.
Lersch, K. M. (2020). Exploring the geography of suicide threats and suicide attempts: An application of risk terrain modeling. Social Science & Medicine, 249, 112860. https://doi.org/10.1016/j.socscimed.2020.112860.
Letvak, S., & THE IMPORTANCE OF SOCIAL SUPPORT FOR RURAL MENTAL HEALTH. (2002). Issues in Mental Health Nursing, 23(3), 249–261. https://doi.org/10.1080/016128402753542992.
Li, Y. Y. (2011). Social structure and Informal Social Control in Rural Communities. International Journal of Rural Criminology. https://doi.org/10.18061/1811/51126. 1.
Li, Z. R., Xie, E., Crawford, F. W., Warren, J. L., McConnell, K., Copple, J. T., Johnson, T., & Gonsalves, G. S. (2019). Suspected heroin-related overdoses incidents in Cincinnati, Ohio: A spatiotemporal analysis. PLoS Medicine, 16(11), e1002956. https://doi.org/10.1371/journal.pmed.1002956.
Li, Y., Hyder, A., Southerland, L. T., Hammond, G., Porr, A., & Miller, H. J. (2020). 311 service requests as indicators of neighborhood distress and opioid use disorder. Scientific Reports, 10(1), 19579. https://doi.org/10.1038/s41598-020-76685-z.
Lister, J. J., Weaver, A., Ellis, J. D., Himle, J. A., & Ledgerwood, D. M. (2020). A systematic review of rural-specific barriers to medication treatment for opioid use disorder in the United States. The American Journal of Drug and Alcohol Abuse, 46(3), 273–288. https://doi.org/10.1080/00952990.2019.1694536.
Liu, M., Caplan, J. M., Kennedy, L. W., Moise, I. K., Feaster, D. J., Horigian, V. E., Roll, J. M., McPherson, S. M., & Rao, J. S. (2023). Geo-spatial risk factor analysis for drug overdose death in South Florida from 2014 to 2019, and the independent contribution of social determinants of health. Drug and Alcohol Dependence, 248, 109931. https://doi.org/10.1016/j.drugalcdep.2023.109931.
Lum, C. (2008). The geography of drug activity and violence: Analyzing spatial relationships of non-homogenous crime event types. Substance Use and Misuse, 43(2), 179–201. https://doi.org/10.1080/10826080701690573.
Marchment, Z., & Gill, P. (2021). Systematic review and meta-analysis of risk terrain modelling (RTM) as a spatial forecasting method. Crime Science, 10(1), 12. https://doi.org/10.1186/s40163-021-00149-6.
Marshall, J. R., Gassner, S. F., Anderson, C. L., Cooper, R. J., Lotfipour, S., & Chakravarthy, B. (2019). Socioeconomic and geographical disparities in prescription and illicit opioid-related overdose deaths in Orange County, California, from 2010–2014. Substance Abuse, 40(1), 80–86. https://doi.org/10.1080/08897077.2018.1442899.
Martínez, R., Rosenfeld, R., & Mares, D. (2008). Social Disorganization, Drug Market Activity, and Neighborhood Violent Crime. Urban Affairs Review, 43(6), 846–874. https://doi.org/10.1177/1078087408314774.
McCord, E. S., & Ratcliffe, J. H. (2007). A micro-spatial analysis of the demographic and criminogenic environment of Drug Markets in Philadelphia. Australian & New Zealand Journal of Criminology, 40(1), 43–63. https://doi.org/10.1375/acri.40.1.43.
McCulloch, B. J. (1995). The relationship of family proximity and social support to the mental health of older rural adults: The Appalachian context. Journal of Aging Studies, 9(1), 65–81. https://doi.org/10.1016/0890-4065(95)90026-8.
Mell, H. K., Mumma, S. N., Hiestand, B., Carr, B. G., Holland, T., & Stopyra, J. (2017). Emergency Medical Services Response Times in Rural, Suburban, and Urban Areas. JAMA Surgery, 152(10), 983–984. https://doi.org/10.1001/jamasurg.2017.2230.
Merchant, R. C., Schwartzapfel, B. L., Wolf, F. A., Li, W., Carlson, L., & Rich, J. D. (2006). Demographic, geographic, and temporal patterns of ambulance runs for suspected opiate overdose in Rhode Island, 1997–2002. Substance Use & Misuse, 41(9), 1209–1226.
Monnat, S. M. (2018). Factors Associated With County-Level differences in U.S. drug-related Mortality Rates. American Journal of Preventive Medicine, 54(5), 611–619. https://doi.org/10.1016/j.amepre.2018.01.040.
Moody, L., Satterwhite, E., & Bickel, W. K. (2017). Substance use in Rural Central Appalachia: Current status and treatment considerations. Rural Mental Health, 41(2), 123–135. https://doi.org/10.1037/rmh0000064.
National Institute on Drug Abuse (2022). Overdose Death Rates. https://nida.nih.gov/drug-topics/trends-statistics/overdose-death-rates.
Ohio Department of Public Safety (2021). Ohio Incident Based Reprting System. Retrieved from https://ocjs.ohio.gov/oibrs/links/Data_Specs.pdf.
Ohio Department of Health (2022). Violence & Injury Prevention Section. Retrieved 9/28/22 from https://odh.ohio.gov/know-our-programs/violence-injury-prevention-program/drug-overdose/.
Ohyama, T., & Amemiya, M. (2018). Applying crime prediction techniques to Japan: A comparison between risk terrain modeling and other methods. European Journal on Criminal Policy and Research, 24, 469–487.
Osgood, W. D., & Chambers, J. M. (2000). Social Disorganization outside the Metropolis: An analysis of Rural Youth Violence*. Criminology, 38(1), 81–116. https://doi.org/10.1111/j.1745-9125.2000.tb00884.x.
Palombi, L. C., St Hill, C. A., Lipsky, M. S., Swanoski, M. T., & Lutfiyya, M. N. (2018). A scoping review of opioid misuse in the rural United States. Annals of Epidemiology, 28(9), 641–652. https://doi.org/10.1016/j.annepidem.2018.05.008.
Park, C., Crawford, S., Lopez, R., Seballos, A., Clemenceau, J. R., Coy, T., Atluri, G., & Hwang, T. H. (2019). Opioid overdose in Ohio: Comprehensive Analysis of Associated socioeconomic factors (p. 19005140). medRxiv. https://doi.org/10.1101/19005140.
Pear, V. A., Ponicki, W. R., Gaidus, A., Keyes, K. M., Martins, S. S., Fink, D. S., Rivera-Aguirre, A., Gruenewald, P. J., & Cerdá, M. (2019). Urban-rural variation in the socioeconomic determinants of opioid overdose. Drug and Alcohol Dependence, 195, 66–73. https://doi.org/10.1016/j.drugalcdep.2018.11.024.
Peleg, K., & Pliskin, J. S. (2004). A geographic information system simulation model of EMS: Reducing ambulance response time. The American Journal of Emergency Medicine, 22(3), 164–170. https://doi.org/10.1016/j.ajem.2004.02.003.
Ratcliffe, J. H. (2012). How near is near? Quantifying the spatial influence of crime attractors and generators. Patterns, prevention, and geometry of crime (pp. 125–139). Routledge.
Ratcliffe, M., Burd, C., Holder, K., & Fields, A. (2016). Defining Rural at the U.S. Census Bureau. United States Census Bureau.
Sadler, R. C., & Furr-Holden, D. (2019). The epidemiology of opioid overdose in Flint and Genesee County, Michigan: Implications for public health practice and intervention. Drug and Alcohol Dependence, 204, 107560. https://doi.org/10.1016/j.drugalcdep.2019.107560.
Slavova, S., Delcher, C., Buchanich, J. M., Bunn, T. L., Goldberger, B. A., & Costich, J. F. (2019). Methodological complexities in quantifying rates of fatal opioid-related overdose. Current Epidemiology Reports, 6(2), 263–274.
Steinman, H., Drawve, G., Datta, J., Harris, C. T., & Thomas, S. A. (2021). Risky business: Examining the 80 – 20 rule in relation to a RTM framework. Criminal Justice Review, 46(1), 20–39.
Sumetsky, N., Mair, C., Wheeler-Martin, K., Cerda, M., Waller, L. A., Ponicki, W. R., & Gruenewald, P. J. (2021). Predicting the Future Course of Opioid Overdose Mortality: An Example from two US States. Epidemiology. (Cambridge Mass), 32(1), 61–69. https://doi.org/10.1097/ede.0000000000001264.
Thurston, H., & Freisthler, B. (2020). The spatio-temporal distribution of naloxone administration events in rural Ohio 2010-16. Drug and Alcohol Dependence, 209, 107950. https://doi.org/10.1016/j.drugalcdep.2020.107950.
Tillyer, M. S., Wilcox, P., & Walter, R. J. (2021). Crime generators in context: Examining ‘place in neighborhood’propositions. Journal of Quantitative Criminology, 37(2), 517–546.
Tofighi, B., Lekas, H. M., Williams, S. Z., Martino, D., Blau, C., & Lewis, C. F. (2021). Rural and small metro area naloxone-dispensing pharmacists’ attitudes, experiences, and support for a frontline public health pharmacy role to increase naloxone uptake in New York State, 2019. Journal of Substance Abuse Treatment, 129, 108372. https://doi.org/10.1016/j.jsat.2021.108372.
Turcotte, M. (2005). Social engagement and civic participation. desLibris.
United States Census Bureau (2020). Introduction to NAICS. United States Census Bureau. https://www.census.gov/eos/www/naics/.
United States Health Resources & Services Administration (2021). Defining Rural Population. https://www.hrsa.gov/rural-health/about-us/definition/index.html.
United States Department of Agriculture (2019). 2010 rural-urban commuting area (RUCA) Codes. Retrieved 7/12/2020 from https://www.ers.usda.gov/data-products/rural-urban-commuting-area-codes/documentation/.
USDA Economic Research Service (2020). Rural-Urban Commuting Area Codes. U.S. Department of Agreiculture. https://www.ers.usda.gov/data-products/rural-urban-commuting-area-codes.aspx.
Valasik, M. (2018). Gang violence predictability: Using risk terrain modeling to study gang homicides and gang assaults in East Los Angeles. Journal of Criminal Justice, 58, 10–21. https://doi.org/10.1016/j.jcrimjus.2018.06.001.
Valasik, M., Brault, E. E., & Martinez, S. M. (2019). Forecasting homicide in the red stick: Risk terrain modeling and the spatial influence of urban blight on lethal violence in Baton Rouge, Louisiana. Social Science Research, 80, 186–201. https://doi.org/10.1016/j.ssresearch.2018.12.023.
Wagner, J., Neitzke-Spruill, L., O’Connell, D., Highberger, J., Martin, S. S., Walker, R., & Anderson, T. L. (2019). Understanding Geographic and Neighborhood Variations in Overdose Death Rates. Journal of Community Health, 44(2), 272–283. https://doi.org/10.1007/s10900-018-0583-0.
Ward, K., Kirchner, E., & Thompson, A. (2018). Social Disorganization and Rural/Urban Crime Rates: A County Level comparison of contributing factors. International Journal of Rural Criminology, 4, 43–65. https://doi.org/10.18061/1811/86153.
Warner, M., Paulozzi, L. J., Nolte, K. B., Davis, G. G., & Nelson, L. S. (2013). State Variation in certifying manner of death and drugs involved in drug intoxication deaths. Academic Forensic Pathology, 3(2), 231–237. https://doi.org/10.23907/2013.029.
Weintraub, E., Greenblatt, A. D., Chang, J., Himelhoch, S., & Welsh, C. (2018). Expanding access to buprenorphine treatment in rural areas with the use of telemedicine. The American Journal on Addictions, 27(8), 612–617.
Wells, L. E., & Weisheit, R. A. (2004). Patterns of Rural and Urban Crime: A County-Level comparison. Criminal Justice Review, 29(1), 1–22. https://doi.org/10.1177/073401680402900103.
Wheeler, A. P., & Steenbeek, W. (2021). Mapping the risk terrain for crime using machine learning. Journal of Quantitative Criminology, 37(2), 445–480. https://doi.org/10.1007/s10940-020-09457-7.
Wilson, N., Kariisa, M., Seth, P., Smith, H., & Davis, N. L. (2020). Drug and opioid-involved overdose deaths - United States, 2017–2018. MMWR Morbidity and Mortality Weekly Report, 69(11), 290–297. https://doi.org/10.15585/mmwr.mm6911a4.
Funding
The authors did not receive support from any organization for the submitted work.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors have no relevant financial or non-financial interests to disclose.
Ethics approval
The study described in this manuscript was approved by University of Alabama at Birmingham’s Institutional Review Board with a Not Human Subjects Research Designation and was conducted in accordance with the ethical standards of APA.
Informed consent
As this study uses aggregate decedent data with no identifying information or imagery, informed consent was not required.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic Supplementary Material
Below is the link to the electronic supplementary material.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Chichester, K.R., Drawve, G., Sisson, M. et al. Crime and Features of the Built Environment Predicting Risk of Fatal Overdose: A Comparison of Rural and Urban Ohio Counties with Risk Terrain Modeling. Am J Crim Just 49, 230–254 (2024). https://doi.org/10.1007/s12103-023-09739-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12103-023-09739-3