
Abstract
Intra-labyrinthine schwannomas are rare. We present a case of a 50-year-old male with non-serviceable unilateral sensorineural hearing loss and tinnitus. CE-MRI revealed an enhancing signal in the basal turn of left cochlea suggestive of a schwannoma. A trans-mastoid standard facial recess approach was used for tumor excision. At one year follow up, patient is disease free.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Schwannomas commonly involve the cochleo-vestibular nerve complex in the internal auditory canal (IAC). IAC schwannomas grow along path of least resistance and commonly involve the cerebellopontine angle. However, a purely intra-labyrinthine location for schwannomas is rare and very few have been reported in the literature [1, 2]. Making a treatment decision is tricky in these cases as most patients present with serviceable hearing loss and are not much symptomatic [3]. Various surgical approaches have been described to address purely cochlear schwannomas.
In this report, we present a case of cochlear schwannoma having profound hearing loss which was managed surgically via a facial recess approach.
Along with this, we have also reviewed literature on intra-labyrinthine schwannomas.
Case Report
A 50 year old male with no known comorbidities, presented to our outdoor department with complaints of left sided impairment of hearing and tinnitus for the past two years. He also complained of left side facial weakness for the past 6 years which had gradually improved to almost normalcy over course of time. He did not complain of a discharging ear, vertigo or headache. On examination he had normal looking tympanic membrane and no obvious facial weakness. On testing with tuning forks, he reported no response in his left ear. Patient’s pure tone audiogram and Brainstem Evoked Response Audiometry (BERA) revealed profound hearing loss in his left ear and normal hearing in his right ear. Stapedial reflex was absent in the left ear. A CEMRI-Brain was obtained with emphasis on cerebellopontine angles with 3-D reconstruction of inner ear.
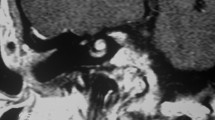
T1W contrast images (Fig. 1a) revealed an enhancing signal in the basal turn of the left cochlea starting just adjacent to round window and ending midway along the length of the basal turn. A provisional diagnosis of an intracochlear schwannoma was made.

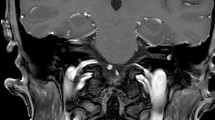
Pre-operative contrast enhanced MRI (a) and post-operative contrast enhanced MRI (b). Preoperative CEMRI showing an enhancing signal in the basal turn of left cochlea ( red arrow). Post operative CEMRI showing lack of enhancing signal in left cochlear basal turn signifying complete tumor excision (yellow arrow)
Patient was given options of wait and watch, gamma knife therapy and surgical excision of the tumour. He opted for surgical excision of the tumour after considering the facts that surgical excision is the only way to possible permanent cure; gamma knife therapy would only make the tumour static and that he does not have any serviceable hearing in his left ear.
Since the tumour was limited to the lower half of basal turn of cochlea, we opted for a standard posterior tympanotomy-facial recess approach. A standard cortical mastoidectomy was performed. The facial recess was identified. It was gradually widened between chorda tympani and the facial nerve (Fig. 2a). The round window niche was visualised and bony overhangs were drilled to expose the round window membrane (Fig. 2b). The round window membrane was opened using a right angled hook. On opening into the basal turn, a soft, pinkish gelatinous mass was seen occluding the lumen (Fig. 2c). Using 1 mm diamond burr, the bone around the mass was drilled to further expose it. A dissection plane was gradually built around the mass and it was excised in toto. The lumen distal to the mass was found free of tumour(Fig. 2d). Although there was no CSF leak, it was considered safe to plug the lumen with fat.

Intra-operative view showing facial recess approach (a). Posterior tympanotomy (black arrow) with exposed short process of incus (marked with asterix) and round window (arrow head). Magnified view of bulging pinkish grey tumor (black arrow) seen though round window (b). Dissection of tumor excision using otological micro instruments (c). Empty basal turn (black arrow) after tumor excision (d)
Patient recovered well in the post-operative period with only mild vertiginous symptoms which resolved over three days. A standard course of intravenous third generation cephalosporins was started for a period of three days.
Patient’s follow up MRI after one year showed no abnormal enhancement in the left cochlearbasal turn (Fig. 1b).
Discussion
Intra-labyrinthine schwannomas (ILS) are a rare occurrence. Study by Van Abel et al. showed majority (50%) of Intralabyrinthine schwannomas are intracochlear whereas mixed vestibulocochlear types are least common (11.8%) [3]. Kennedy et al. classified ILS into seven different types summarized in Table 1. Radiological diagnosis of ILS is difficult and expertise in the field of temporal bone imaging is required. The main differential diagnosis is labyrinthitis, however, an inflammation of the labyrinth would have an MR signal which is more pronounced & diffuse and not as focal and sharp as in our case.
Our case belonged to the intracochlear variety with extent limited only to the basal turn of cochlea. Various case series recommend a wait and watch policy for these tumours unless patients develop vertigo or non-serviceable hearing loss or in conditions when patients refuse surgery [4, 5]. Another modality of treatment is gamma knife therapy. It avoids an incision however only makes the tumour static but does not offer a permanent cure. The young patient in this case report, presented to us with non-serviceable hearing loss, hence a surgical excision was deemed fit after thorough discussion with the patient and his family.
Many surgical approaches have been described for cochlear lesions including trans-labyrinthine, trans-cochlear (microscopic or endoscopic) [6, 7]. All these series claim excellent outcomes and results with these approaches. Recently trans-canal, trans-cochlear approaches have also been described for intracochlear schwannomas [8]. However, these approaches expose the inner ear to the external ear with possible risk of labyrinthitis or meningitis. For purely intracochlear lesions, a transmastoid facial recess approach is suitable. To the best our knowledge, this is the first time that a facial recess approach has been described for extirpation of a cochlear schwannoma. Our patient recovered uneventfully in the post-operative period with no complications. One year after the surgeryfollow up MRI was done, he is disease free clinically as well as radiologically (Fig. 1b) and reports subjective improvement in his tinnitus also.
Conclusion
Contrast enhanced MRI for inner ear and cerebellopontine angle in case of a unilateral sensorineural hearing loss is indispensable. Important differentials can be a nerve sheath tumor, labyrinthitis, trauma, etc. Management strategy has to decided keeping in mind the nature of the disease, audiological assessment and last but not the least; patient’ s wish.
References
Kennedy RJ, Shelton C, Salzman KL, Davidson HC, Harnsberger HR (2004) Intralabyrinthine schwannomas: diagnosis, management, and a new classification system. Otol Neurotol 25(2):160–167. https://doi.org/10.1097/00129492-200403000-00014
Elias TGA, Perez Neto A, Zica ATS, Antunes ML, Penido NO (2019) Different clinical presentation of intralabyrinthine schwannomas - a systematic review. Braz J Otorhinolaryngol 85(1):111–120
Van Abel KM, Carlson ML, Link MJ, Neff BA, Beatty CW, Lohse CM, Eckel LJ, Lane JI, Driscoll CL (2013) Primary inner ear schwannomas: a case series and systematic review of the literature. Laryngoscope 123(8):1957–1966
Covelli E, Volpini L, Filippi C, Tarantini S, Marrone V, Monini S, Barbara M (2017) Intralabyrinthine vestibular schwannoma responsive to intratympanic gentamicin treatment. J Int Adv Otol 13(2):285–288
Magliulo G, Colicchio G, Romana AF, Stasolla A (2010) Intracochlear schwannoma. Skull Base 20(2):115–118
Bento RF, Gebrim EM, Magalhães AT, Pereira LV, Fonseca AC (2016) Minimally invasive surgery for intracochlear schwannoma removal and simultaneous cochlear implantation. Int Arch Otorhinolaryngol 20(3):271–4
Krueger WW, Kemper JV (2000) Cochlear schwannomas. Skull Base Surg 10(2):87–88
Marchioni D, De Rossi S, Soloperto D, Presutti L, Sacchetto L, Rubini A (2018) Intralabyrinthine schwannomas: a new surgical treatment. Eur Arch Otorhinolaryngol 275(5):1095–1102. https://doi.org/10.1007/s00405-018-4937-0
Author information
Authors and Affiliations
Corresponding author
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Aggarwal, K., Kairo, A.K., Bhalla, A.S. et al. Cochlear Schwannoma: A Usual Pathology in an Unusual Site. Indian J Otolaryngol Head Neck Surg 74 (Suppl 3), 3861–3864 (2022). https://doi.org/10.1007/s12070-021-02687-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12070-021-02687-6