
Abstract
Neoplasia of the head and the neck necessitates intervention, surgical or otherwise, as the site and stage of the pathology may dictate. The various therapeutic modalities employed and prognosis has been reviewed.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Success in treatment of head and neck neoplasia depends on the appropriate treatment of both the primary lesion and the regional lymphatics. Therapeutic modality: surgery, radiotherapy, chemotherapy or a combination is guided by the site of primary lesion, the size of tumor (T stage), the presence and number of nodal metastasis (N stage), the spread of the tumor outside the lymph node capsule and perineural invasion by the primary tumor, Marur and Foratiere [1]. Moreover aim is to initiate treatment with minimal treatment induced distortion of anatomy and physiology, which can adversely affect such basic and inter-related functions such as chewing, swallowing and speaking as well as the sense of sight, smell and hearing, Marur and Foratiere [1].
Review of Literature
Early-stage cancers (tumor stage as T1 or T2 with no nodal involvement) are best treated with surgery or radiation depending on the sub site and the expertise of the clinical team.
Intermediate-stage tumors (infiltrative tumors, poor prognosis T2 tumors or exophytic T3, N0–N1 tumors) may benefit from a combined-modality approach. The locally advanced tumors are the unfavorable infiltrative T3 or T4 primary tumors with N2 or N3 lymphadenopathy.
Patients with locally advanced tumors are best treated with concurrent chemo radiation if the tumor is unresectable, and if it is resectable but organ preservation is desired, or if they are receiving postoperative adjuvant radiation with concurrent cisplatin, as indicated, Posner [2].
In small transorally accessible cancers of the oral cavity, pharynx and larynx, surgical excision can be achieved with functional preservation of the involved organ with good oncological results, Ambrosch [3].
Microsurgical treatment, which uses endoscopic laser or robotic techniques and high resolution magnified optics, has become technically feasible and is cost saving compared to open surgical procedures or radiotherapy for early stage laryngeal cancer with acceptable voice outcome, Myers et al. [4].
Cervical lymph node disease is managed with neck dissection or irradiation, Mendenhall et al. [5].
Neck dissection of three types –
-
1.
Radical neck dissection
-
2.
Modified radical neck dissection
-
3.
Selective neck dissection
Radical Neck Dissection
In a classic radical neck dissection (RND), the superficial and deep cervical fascia with its enclosed lymph nodes (levels I to V) is removed in continuity with the sternocleidomastoid muscle, the omohyoid muscle, the internal and external jugular veins, the spinal accessory nerve, and the submandibular gland, Mendenhall et al. [5]; Watkinson [6].
Modified Radical Neck Dissection
Selective Neck Dissection
Selective neck dissections are more limited in extent and include the resection of selected lymph node levels. The types include
-
1.
Lateral—resections of lymph node level II–IV
-
2.
Posterolateral—resections of lymph node level II–V
-
3.
Anterior—resections of lymph node level VI
-
4.
Supraomohyoid—resections of lymph node level I–III
-
5.
Extended supraomohyoid—resections of lymph node level I–IV, Goefert [7] (Figs. 1, 2)
Fig. 1 
Modified radical neck dissection [6]
Fig. 2 
Selective neck dissection [6]


Radiotherapy
Mode of action—Radiation causes damage to DNA in both normal and malignant cells. Malignant cells have a lower repair capacity and a shorter cell cycle than normal cells. Thus the chances of a dose of radiation killing a malignant cell are greater than those of killing a normal cell, Bartlett [8].
-
A.
Conventional Radiotherapy—In conventional radiotherapy for head and neck cancer, the primary tumor and involved lymph nodes are irradiated with 70 Gy, delivered in single fractions of 1.8–2.0 Gy/d.
-
B.
Fractionated Radiotherapy—Recently better loco regional control has been obtained with altered fractionation, which includes
-
1.
Hyper fractionation—1.2 Gy twice daily; 81.6 Gy over the course of 7 weeks.
-
2.
Accelerated fractionation—1.6 Gy twice daily; 67.2 Gy over the course of 6 weeks.
-
3.
Accelerated fractionation with a concomitant boost—in addition to 1.6 Gy daily for 6 weeks; add on 0.4 Gy daily as a boost for the last 12 days only; 72 Gy over the course of 6 weeks, Bourhis et al. [9].
-
1.
-
C.
IMRT (Intensity-Modulated Radiotherapy)
A relatively new and advanced form of radiotherapy delivery in three-dimensional conformal fashion is intensity-modulated radiotherapy, which allows delivery of high doses of radiotherapy to clinical target organs while preserving critical normal structures and more important the salivary gland function, Eisbrusch et al. [10].
During radiotherapy shield is used to protect brain, brainstem, spinal cord, optic chiasm, eye and anterior orbit, Lincoln [11].
Chemotherapy
Mode of action—Chemotherapeutic drugs act on the rapidly dividing cells during S phase of cell cycle of DNA synthesis. Drug molecules bind covalently to DNA interrupting its replication, Bartlett [8].
Chemotherapy is widely used for management of locally advanced head and neck cancer, Cohen et al. [12]. The concept of combined modality of treatment with introduction of chemotherapy has come with goals of improved local control, survival and reduction of distant metastases. The ultimate goal is to improve therapeutic ratio, Fu [13].
Various classes of agents such as platinum compounds, antimetabolites and taxanes have shown significant single-agent activity against head and neck cancer. Taxane agents include paclitaxel and docetaxel, Coleves [14].
New drugs like cisplatin, bleomycin, vinblastine, fluorouracil (FU) introduced in the early 1980s and new combinations, essentially cisplatin- fluorouracil with very high response rates (20–70%) have led to a re-evaluation of the role of chemotherapy in the treatment of advanced head and neck squamous cell carcinoma, Stupp et al. [15].
The platinum compound cisplatin is regarded as a standard agent in combination with the radiation or with other agents. Carboplastin is well tolerated but less active than cisplatin as a component of combination regimens, De Andres et al. [16]; Forastiere al [17], although the radiosensiting properties of the two platinum agents could be comparable, Jeremic et al. [18].
Taxane-based combinations are very active and have been tested in the induction chemotherapy (chemotherapy used for the initial treatment of a disease) of locally advanced head and neck cancer, Agiris et al. [19]. Moreover, epidermal growth factor receptor (EFGR) inhibition has emerged as a novel treatment strategy for head and neck cancer and cetuximab is the first molecule targeted agent that has been introduced into standard practice, Karamouzis et al. [20].
Other ways of targeting epidermal growth factor receptor and other dysregulated molecular pathways in head and neck cancer, using monoclonal antibodies, single selective or multi-selective tyrosine kinase inhibitors and nucleic acid-directed approaches, are also being explored. The combination of epidermal growth factor receptor inhibitors with other molecule targeted agents (for example, angiogenesis inhibitors) has surfaced as a novel strategy, whereas the combination of these novel agents with chemo-radiotherapy is under investigation, Agiris et al. [21].
Chemotherapy can be given in three main sequences in combination with definitive local treatment for solid tumors –
-
(a)
Neoadjuvant chemotherapy—initial chemotherapy is designed to shrink the primary tumor, thereby rendering local therapy (surgery or radiotherapy) less destructive or more effective.
-
(b)
Concomitant chemotherapy—chemotherapy given in addition to primary treatment like radiotherapy.
-
(c)
Adjuvant chemotherapy- chemotherapy is given after surgery. It is used when there is little evidence of cancer present, but there is risk of recurrence. It has not been shown to be useful for advanced head and neck squamous cell carcinoma. The lack of biologic benefit in the adjuvant setting is perhaps more easily accepted because there is no measurable tumor and the long term tumor control must be the end point.
-
(d)
Palliative chemotherapy—given without curative intent, but simply to decrease tumor load and increase life expectancy. For these regimens, a better toxicity profile is generally expected, Rosenthal [22]. Alternating delivery of two active, non cross resistant treatments can increase the cure rate because of the possibility of each treatment extinguishing the residual resistant cell clones, avoiding the development of double resistant clones, Goldie and Coldman [23].
Recently, concomitant and alternating chemotherapy and radiotherapy has become the focus of interest. The goals of simultaneous administration of chemotherapy and radiotherapy are to enhance the radiotherapy effect and to improve loco regional control rate along with eradication of early micro metastasis, Stupp et al. [15].
Role of Antioxidants
Antioxidants levels are decreased significantly during cisplatin- based chemotherapy. Vitamin C, vitamin E and glutathione peroxidase (of which selenium is an essential constituent) are the most important natural antioxidants, which are synergistically able to interfere with the harmful reactions initiated by free radicals. The oral supplementation of vitamin C, vitamin E and selenium aids in the prevention of cisplatin-induced toxicity, Weijl [24].
Lycopene is an antioxidant and a major carotenoids. Carotenoids are basically pigments that give yellow, red, and orange vegetables and fruits, their colors. The body uses some types of carotenoids (but not lycopene) to make vitamin A, Lawenda [25].
Lycopenes help in the prevention and treatment of cancers of the lung, mouth, stomach, skin, and especially, prostate. It blocks the action of free radicals, activated oxygen molecules that can damage cells. They are given as adjuvant to chemotherapeutic drugs, Lawenda [25].
Role of Vaccines
The viral-encoded oncogenic proteins E6 and E7 represent ideal targets for immunotherapy against HPV-associated head and neck cancers. DNA vaccines have emerged as attractive approaches for immunotherapy due to its simplicity, safety, and ease of preparation. Intradermal administration of DNA vaccine via gene gun represents an efficient method to deliver DNA directly into dendritic cells for priming antigen-specific T cells. Li-PADRE-E6 represents a novel DNA vaccine for the treatment of HPV-associated head and neck cancer and other HPV-associated malignancies, Wu et al. [26].
Role of Targetted Therapy
An anti-EGFR monoclonal antibody (mAb), IMC-C225, binds competitively to the extracellular receptor site to prevent binding by natural EGFR ligands (EGF and TGF-alpha). This chimeric mAb has potent antitumour activity. It causes inhibition of cell cycle progression, induction of apoptosis, anti-angiogenesis and inhibition of metastasis, and enhances the response to chemotherapy and radiation therapy. IMC-C225 combined with chemotherapy or radiation for head and neck squamous cell carcinoma give excellent response rates in patients with recurrent or refractory disease. IMC-C225 has been well-tolerated, with skin rashes and allergic reactions being the most clinically important adverse events reported. Recommended dose is 400 mg/m2 loading dose, followed by weekly infusions of 250 mg/m2, Herbst et al. [27].
Gefitinib and Erlotinib [28] are epidermal growth factor receptor (EGFR) inhibitors, which interrupt signaling through the epidermal growth factor receptor (EGFR) in target cells. Therefore, it is only effective in cancers with mutated and overactive EGFR. The dose is 250 mg once daily, Takimoto [29].
Cetuximab (Erbitux) is indicated for the treatment of patients with squamous cell carcinoma of the head and neck in combination with platinum-based chemotherapy for the 1st line treatment of recurrent and/or metastatic disease and in combination with radiation therapy for locally advanced disease, Weijl [24].
Therapeutic Modalities of Head and Neck Neoplasia
Sinonasal Malignancy
Nasal cavity tumors are treated with surgery, irradiation or both. Surgery is indicated for early lesions and combined surgery and adjuvant irradiation for advanced lesions, Mendenhall et al. [29].
Radiotherapy is administered in two fields—anterior and lateral, with 406 MV X-rays. Dose—50–55 Gy in 20 fractions over 4 weeks or 60–65 Gy in 30–33 fractions over 6–6.5 weeks. For lymphoma, dose is 40 Gy in 20 fractions over 4 weeks, Lund [30].
For nasopharyngeal carcinomas, radiotherapy is the treatment of choice. Radiotherapy is given in two phases, with 4–6 MV photons from a linear accelerator.
-
Phase I of dose of 40 Gy in 20 fractions over 4 weeks
-
Phase II of dose of 26 Gy in 13 fractions over 2.5 weeks, Lincoln [11].
In case of recurrent nasopharyngeal tumor, intracavitary or interstitial brachytherapy is given in dose of 60 Gy (2 Gy/day), as it allow high radiation dose to be delivered to tumor while sparing normal tissues which would be irradiated beyond tolerance limits by external beam treatment.
Salivary Gland Malignancy
Parotid gland
-
Benign tumors—surgery.
-
Low-grade malignant tumors—surgery (superficial parotidectomy).
-
High-grade malignant tumors—surgery (total parotidectomy) with radiotherapy.
Facial nerve is to be preserved in every case whenever possible, but sacrificed in case of pre-operative paralyzed facial nerve or in case there is intra-operative evidence of infiltration of facial nerve, Hoille [31]; Jones [32].
Submandibular gland
-
Benign tumors—surgery.
-
Low-grade malignant tumors—surgery.
-
High-grade malignant tumors—surgery with radiotherapy.
Radiotherapy—External beam therapy with 4–6 MV X-rays, dose of 60–66 Gy in 33 fractions over 6–7 weeks, Mendenhall et al. [29].
Otological Malignancy
Glomus tympanicum tumor
Class I—surgical removal by transcanal tympanotomy.
Class II to IV—surgical removal by transmastoid approach.
Glomus jugulare tumor
Class I to IV—surgical removal by means of lateral skull base surgery.
Radiotherapy—indicated for inoperable tumors, residual tumors, recurrence after surgery or older patients (unfit for surgery), Jackson et al. [33].
Oral Cavity Malignancy
-
Early lesion (T1 or T2)—partial glossectomy with primary closure or a skin graft.
-
Advanced lesions (T2 or T3)—partial glossectomy, neck dissection and postoperative radiotherapy.
-
Advanced lesions (T4)—combined treatment surgery and radiation.
Radiotherapy—external beam therapy followed by interstitial or intraoral cone therapy. Megavoltage photons from a linear accelerator. Dose—55 Gy in 20 daily fractions over 4 weeks, Galen [34].
Hypopharyngeal Malignancy
Posterior pharyngeal wall tumor—radiotherapy or surgery or both.
Lateral pharyngeal wall tumor—radiotherapy.
Pyriform sinus tumor –
-
T1 or low volume T2 lesions—irradiation or partial laryngopharyngec-tomy.
-
High volume T2 or T3 lesions—radiotherapy with concomitant chemotherapy.
-
Advanced T4 lesions—palliative therapy.
Radiotherapy—Given in two phases with 4–6 MV X-rays.
-
Phase I of dose of 40 Gy in 20 daily fractions over 4 weeks.
-
Phase II of 26 Gy in 13 fractions over 2.5 weeks, Maran [35].
Laryngeal Malignancy
Supraglottis malignancy
-
Supraglottic T1, T2 and low volume (6 cc or less) T3 lesions—irradiation or supraglottic laryngectomy or combination.
-
Supraglottic high volume (> 6 cm) T3 or T4 lesions—irradiation and concomitant chemotherapy or total laryngectomy ± radiotherapy.
Glottic malignancy
-
Vocal cord Carcinoma in situ lesion—stripping of cord.
-
Early vocal cord lesion (T1 or T2)—radiotherapy or transoral laser excision or open partial laryngectomy.
-
Advanced vocal cord lesion (T3 or T4)—low volume cancer treated with irradiation and concomitant chemotherapy.
-
High volume cancer treated with total laryngectomy, neck dissection and postoperative radiotherapy.
Subglottic malignancy
Subglottic early lesions—treated by radiotherapy and advanced lesions by total laryngectomy and postoperative radiation therapy.
Radiotherapy—With 4–6 MV X-rays from a linear accelerator, dose—66 Gy in 33 fractions over 6.5 weeks, Gay [36].
Limit of irradiation:
-
Supraglottis—from the level of C2 down to the cricoid cartilage and anteriorly from skin to anterior margin of vertebral bodies.
-
Glottis—from thyroid cartilage to cricoids cartilage.
-
Sub glottis—from the thyroid notch to manubriosternal joint.
Thyroid Malignancy
-
Benign tumors—surgery.
-
Malignant tumors—surgery ± radioiodine therapy ± radiotherapy.
Radioiodine therapy—the isotope of iodine used for therapy is 131I, given as a drink or capsule of sodium iodide. Dose—3 GBq for ablation of a small thyroid remnant or 5.5 GBq for treatment of tumor.
Radiotherapy—given in two phases.
-
Phase I—dose of 40 Gy in 20 fractions over 4 weeks.
-
Phase II—dose of 20–26 Gy in 10–13 fractions over 2–2.6 weeks, Howards [37].
Prognosis of Head and Neck Neoplasia
Sinonasal Malignancy
The overall prognosis of sinonasal malignancy is directly related to the degree of local control, Dulguerov [38]. Absolute local control rates for all sinonasal malignancies are: Katz [39].
-
1.
50% at 5 years
-
2.
31% at 10 years
-
3.
21% at 15 years
Nasopharyngeal Malignancy
The average 5 years survival achieved by conventional radiotherapy alone is excellent for early disease: Lee [40].
-
1.
Stage 1—80–90%
-
2.
Stage 2—70–80%
-
3.
Stage 3—40–60%
-
4.
Stage 4a–b—20–40%
-
5.
Stage 4c—the median survival is only 6 months (Figs. 3, 4)
Fig. 3 
Local control rate of sinonasal malignancies [39]
Fig. 4 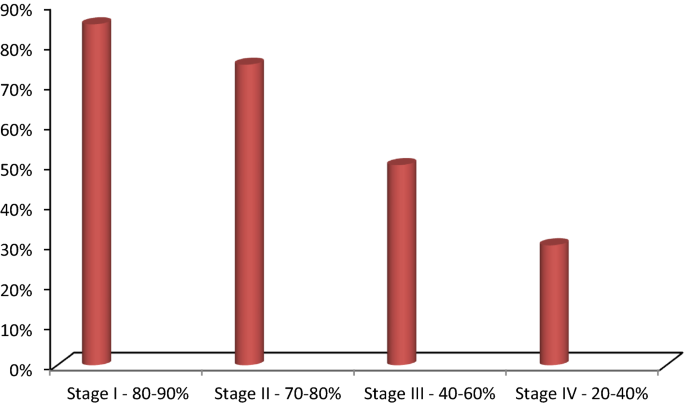
5 Years survival rate of nasopharyngeal malignancies [40]


Salivary Gland Malignancy
-
1.
Squamous cell carcinoma has a 10-year survival rate of 49%.
-
2.
Adenoid cystic carcinoma has a 57% survival at 10 years falling to 35% survival at 20 years.
-
3.
The 10-year survival for undifferentiated cancer is only 7%.
-
4.
Adenocarcinoma has a particularly poor survival of 11% at 5 years and there were no survival at 10 years, Jones [32].
Oral Cavity Malignancy
The survival rate of tongue cancer is related to tumor thickness. If the tumor is greater than 3 cm in diameter, there is most likely deep invasion of the tongue. The five survival rate is, Gonzales-Moles [41] (Figs. 5, 6).

10 Years survival rate of salivary gland malignancies [32]

5 years survival rate of oral cavity malignancies [41]
-
1.
0–3 mm thickness—86%
-
2.
4–7 mm thickness—58%
-
3.
>7 mm thickness—52%
Otological Malignancy
For temporal bone operable tumors, local control rate is 89%, Woods et al. [42].
Hypopharyngeal Malignancy
Posterior and lateral pharyngeal wall tumors have 5-years local control rates after irradiation: Hull et al. [43].
-
1.
T1 stage—93%
-
2.
T2 stage—87%
-
3.
T3 stage—61%
-
4.
T4 stage—50%
Pyriform sinus tumors have 5 year survival rates: Amdur et al. [44] (Figs. 7, 8).

5 years local control rates for hypopharyngeal malignancies [43]

5 years survival rates for pyriform sinus tumors [44]
-
1.
T1 stage—57%
-
2.
T2 stage—61%
-
3.
T3 stage—41%
-
4.
T4 stage—29%
Laryngeal Malignancy
The 5 year survival for laryngeal malignancy, Shah [45]:
-
1.
Supraglottic—51%
-
2.
Glottic—81%
-
3.
Subglottic—77%
Squamous cell carcinoma supraglottic cancer has 5 year survival rates after surgery, Shah [45] (Figs. 9, 10):

5 years survival rates for laryngeal malignancies [45]

5 years survival rates for supraglottic malignancies, after surgery [45]
-
1.
T1 stage—84%
-
2.
T2 stage—83%
-
3.
T3 stage—73%
-
4.
T4 stage—44%
Squamous cell carcinoma supraglottic cancer has 5 year local control rates after definitive radiotherapy is: Hinerman et al. [46].
-
1.
T1 stage—100%
-
2.
T2 stage—86%
-
3.
T3 and T4 stage—62% each.
Survival rate for glottic cancer, Mendenhall et al. [47] (Figs. 11, 12).

5 years survival rates for supraglottic malignancies, after radiotherapy [46]

Survival rate for glottic cancer [47]
-
1.
T1 stage—85%
-
2.
T2 stage—80%
-
3.
T3 stage—77%
-
4.
T4 stage—70%
Thyroid Malignancy
The 10 year survival for: Ramsden et al. [48].
-
1.
Intrathyroid papillary carcinoma > 90%
-
2.
Extra thyroid papillary carcinoma falls to 60%
-
3.
Follicular carcinoma—80%
-
4.
Medullary and anaplastic carcinoma has further worse prognosis (Fig. 13).
Fig. 13 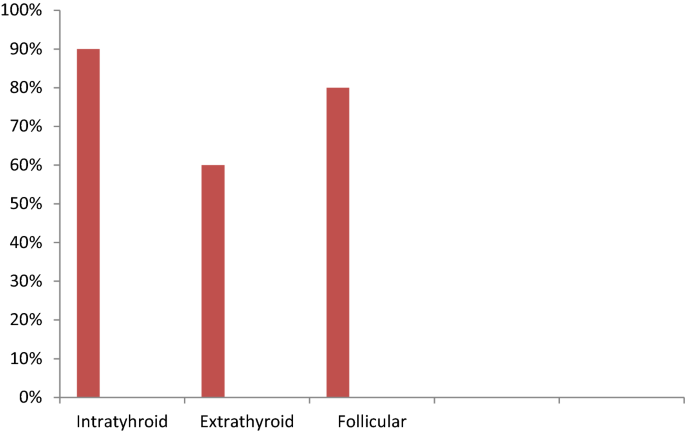
Survival rate for thyroid cancer

Conclusion
Early diagnosis and appropriate therapy in head and neck neoplastic lesions with a regular meticulous follow up has the best surgical outcome.
References
Marur S, Forastiere AA (2008) Head and neck cancer: changing epidemiology, diagnosis, and treatment. Mayo Clin Proc 83:489–501
Posner M (2006) Options in the treatment of head and neck cancer. In: Posner M (ed) CMP medica, The Oncology Group. Manhasset, New York, pp 1–122
Ambrosch P (2007) The role of laser microsurgery in the treatment of laryngeal cancer. Curr Opin Otolaryngol Head Neck Surg. 15:82–88
Myers EN, Wagner RL, Johnson JT (1994) Microlaryngoscopic surgery for T1 glottic lesions: a cost-effective option. Ann Otol Laryngol. 103:28–30
Mendenhall WM, Villaret DB, Amdur RJ et al (2002) Planned neck dissection after radiotherapy for squamous cell carcinoma of the head and neck. Head Neck 24:1012
Watkinson JC, Gaze MN, Wilson JA (2000)Neck dissection. In: Watkinson JC, Gaze MN, Wilson JA(eds) Stell & Maran’s head & neck surgery, 4th edn. Hodder Arnold, London, pp 67–81
Goefert H (1988) Malignant neck disease. In: Watkinson JC, Gaze MN, Wilson JA (eds) Stell & Maran’s head & neck surgery, 4th edn. Hodder Arnold, London, pp 197–213
Bartlett E (2000) Principles of non-surgical treatment. In: Watkinson JC, Gaze MN, Wilson JA (eds) Stell & Maran’s head & neck surgery,4th edn. Hodder Arnold, London, pp 67–81
Bourhis J, Overgaard J, Audry H, Ang KK, Saunders M, Bernier J et al (2006) Hyperfractionated or accelerated radiotherapy in head and neck cancer: a meta-analysis. Lancet 368:843–854
Eisbruch A, Foote RL, O’Sullivan B, Beitler JJ, Vikram B (2002) Intensity-modulated radiation therapy for head and neck cancer: emphasis on the selection and delineation of the targets. Semin Radiat Oncol. 12(3):238–249
Lincoln A (2000) Tumours of the nasopharynx. In: Watkinson JC, Gaze MN, Wilson JA (eds) Stell & Maran’s Head & Neck Surgery, 4th edn. Hodder Arnold, London, pp 397–408
Cohen EE, Lingen MW, Vokes EE (2004) The expanding role of systemic therapy in head and neck cancer. J Clin Oncol 22:1743–1752
Fu KK (1985) Biological basis for the interaction of chemotherapeutic agents and radiation therapy. Cancer 55:2123–2130
Colevas AD (2006) Chemotherapy options for patients with metastasis or recurrent squamous cell carcinoma of the head and neck. J Clin Oncol 24:2644–2652
Stupp R, Weichselbaum RR, Vokes EE (1994) Combined modality therapy of head and neck cancer. Sermin Oncol 21:349–358
De Andres L, Brunet J, Lopez-Pousa A, Burgues J, Vega M, Tabernero JM et al (1995) Randomized trial of neoadjuvant cisplatin and fluorouracil versus carboplatin and fluorouracil in patients with stage IV-M0 head and neck cancer. J Clin Oncol 13:1493–1500
Forastiere AA, Metch B, Schuller DE, Ensley JF, Hutchins LF, Triozzi P et al (1992) Randomized comparison of cisplatin plus fluorouracil and carboplatin plus fluorouracil versus methotrexate in advanced squamous-cell carcinoma of the head and neck: a Southwest Oncology Group study. J Clin Oncol 10:1245–1251
Jeremic B, Shibamoto Y, Stanisavljevic B, Milojevic L, Milicic B, Nikolic N (1997) Radiation therapy alone or with concurrent low-dose daily either cisplatin or carboplatin in locally advanced unresectable squamous cell carcinoma of the head and neck: a prospective randomized trial. Radiother Oncol 43:29–37
Argiris A (2005) Induction chemotherapy for head and neck cancer: will history repeat itself? [published correction appears in J Natl Compr Canc Netw. 2005 Jul;3(4):table of contents]. J Natl Comp Cancer Netw 3(3):393–403
Karamouzis MV, Grandis JR, Argiris A (2007) Therapies directed against epidermal growth factor receptor in aerodigestive in aerodigestive carcinomas. JAMA 298:70–82
Agiris A, Karamouzis MV, Raben D, Ferris RL (2008) Head and neck cancer. Lancet 371:1695–1709
Rosenthal DI, Pistenmaa DA, Glatstein E (1994) A review of neoadjuvant chemotherapy for head and neck cancer: partially shrunken tumours may be both leaner and meaner. Int J Radiat Oncol Biol Phys 28:315–320
Goldie JH, Coldman AJ (1986) Theoretical considerations regarding the early use of adjuvant chemotherapy. In: Ragaz J, Bank PR, Goldie JH (eds) Recent results. Cancer research, preoperative (Neoadjuvant) chemotherapy. Springer, New York, pp 30–35
Weijl NI et al (2004) Supplementation with antioxidant micronutrients and chemotherapy-induced toxicity in cancer patients treated with cisplatin-based chemotherapy: a randomised, double-blind, placebo-controlled study. Eur J Cancer 40(11):1713–1723
Lawenda BD, Kelly KM, Ladas EJ, Sagar SM, Vickers A, Blumberg JB (2008) Should supplemental antioxidant administration be avoided during chemotherapy and radiation therapy? J Natl Cancer Inst 100:773–783
Wu A et al (2011) Innovative DNA Vaccine for Human Papillomavirus (HPV)-Associated Head and Neck Cancer. NIHPA Authors Manuscript. 18(3):304–312
Herbst RS, Kim ES, Harari PM (2001) IMC-C225, an anti-epidermal growth factor receptor monoclonal antibody, for treatment of head and neck cancer. Expert Opin Biol Ther. 1(4):719–732
Takimoto CH, Calvo E (2008) Principles of oncologic pharmacotherapy. In: Pazdur R, Wagman LD, Camphausen KA, Hoskins WJ (eds) Cancer management: a multidisciplinary approach, 11 edn
Mendenhall WM, Werning JW, Pfister DG (2008) Treatment of head and neck cancers. In: Devita et al (eds) cancer principles & practice of oncology, 8th edn. Wolters Kluwer, Philadelphia, pp 811–877
Lund VJ (1990) Tumours of the nose and sinuses. In: Watkinson JC, Gaze MN, Wilson JA (eds) Stell & Maran’s head & neck surgery, 4th edn. Hodder Arnold, London, pp 377–396
Hoille R (2000) Tumours of major salivary glands. In: Watkinson JC, Gaze MN, Wilson JA (eds) Stell & Maran’s head & neck surgery, 4th edn. Hodder Arnold, London, pp 441–456
Jones AS (2008) Malignant tumours of the salivary glands. In. George et al (eds) Scottt-Brown’s otorhinolaryngology, head and neck surgery, 7th edn. Hodder Arnold, London, pp 2493–2521
Jackson CG, FACS MD (2002) Surgery for Benign Tumors of the Temporal Bone. In: Glasscock ME, Gulya AJ (eds) Glasscock-Shambaugh surgery of the ear, 5th edn. Ontario BC Decker Inc, pp 714–742
Galen (2000) Tumours of the lip and oral cavity. In: Watkinson JC, Gaze MN, Wilson JA (eds) Stell & Maran’s head & neck surgery, 4th edn. Hodder Arnold, London, pp 275–317
Maran AGD, Stell PM (2000) Tumours of the hypopharynx. In: Watkinson JC, Gaze MN, Wilson JA (eds) Stell & Maran’s head & neck surgery, 4th edn. Hodder Arnold, London, pp 335–56
Gay J (2000) Tumours of the larynx. In: Watkinson JC, Gaze MN, Wilson JA (eds) Stell & maran’s head & neck surgery, 4th edn. Hodder Arnold, London, pp 233–274
Howard RJ (2000) Tumours of the thyroid and parathyroid glands. In: Watkinson JC, Gaze MN, Wilson JA (eds) Stell & Maran’s head & neck surgery, 4th edn. Hodder Arnold, London, pp 459–485
Dulguerov P, Jacobson MS, Allal AS, Lehmann W, Calcatera T (2001) nasal and paranasal carcinoma: are we making progress? Cancer 92:3012–3029
Katz TS, Mendenhall WM, Morris CG, Amdur RJ, Hinerman RW, Villaret DB (2001) Malignant tumours of the nasal cavity and paranasal sinuses. Head Neck 24:821–829
Lee AW (1999) Complications of radiation therapy. In: van Hasselt CA, Gibb AG (eds) Nasopharyngeal carcinoma, 2nd edn. The Chinese University Press, Hong Kong, pp 255–275
Gonzalez-Moles MA, Esteban F, Rodriguez-Archilla A, Ruiz-Avila I, Gonzalez-Moles S (2002) Importance of tumour thickness measurement in prognosis of tongue cancer. Oral Oncol 38:394–397
Woods CI, Strasnick B, Jackson CG (1993) Surgery for glomus tumors: the Otology Group experience. Laryngoscope 103:65
Hull MC, Morris CG, Tannehill SP et al (2003) Definitive radiotherapy alone or combination with a planned neck dissection for squamous cell carcinoma of the pharyngeal wall. Cancer 98:2224
Amdur RJ, Mendenhall WM, Stringer SP et al (2001) Organ preservation with radiotherapy for T1–T2 carcinoma of the pyriform sinus. Head Neck 23:353
Shah JP, Patel SG (2003) Larynx and trachea. In: Head and neck surgery and oncology, 3rd edn. Mosby, London
Hinerman RW, Mendenhall WM, Amdur RJ et al (2002) carcinoma of the supraglottis larynx: treatment results with radiotherapy alone or with planned neck dissection. Head Neck 24:456
Mendenhall WM, Amdur RJ, Morris CG et al (2001) T1-T2N0 squamous cell carcinoma of the glottic larynx treated with radiation therapy. J Clin Oncol 19:4029
Ramsden J, Watkinson JC (2008) Thyroid cancer. In: George et al (eds) Scottt-Brown’s otorhinolaryngology, head and neck surgery, 7th edn. Hodder Arnold, London, pp 2711–2749
Author information
Authors and Affiliations
Corresponding author
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Munjal, M., Kaur, R., Kaur, R. et al. Therapeutic Modalities in Head–Neck Neoplasia and Prognostication: A Review. Indian J Otolaryngol Head Neck Surg 74 (Suppl 2), 2445–2457 (2022). https://doi.org/10.1007/s12070-020-02200-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12070-020-02200-5