
Abstract
Child mortality has been declining globally in the last decades but some African countries are still lagging behind in the pace of reduction. This study examined the spatio-temporal patterns in the level and variability of child mortality in 41 Africa countries between 1980 and 2018, and assesses the form of relationship between individual countries’ gross domestic product (GDP) and child mortality using country-level data from World Bank development indicators. Model estimation was based on Bayesian approach. Findings show that child mortality levels are reducing consistently in Africa and that over the 39 years study period, South Africa, Botswana, Namibia, Malawi, Zimbabwe, Mozambique and Zambia all in southern Africa with Egypt, Tunisia and Rwanda experienced the highest variability in child mortality. Also, countries like Nigeria, Mauritania, Chad and Central African Republic are among those with the highest risks of child mortality between 2015-2018 even though the risks were lower relative to other places in the 1980s. Child mortality and GDP always follow each other in reverse order but this is not often the case for all the countries considered.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Unarguably, child mortality is one of the best measures of x-raying the socioeconomic and health conditions of a nation. Globally, infant and child mortality rates have been declining in the past six and a half decades, due to the consequential effects of improved socioeconomic conditions and increased investment in public health and education. Statistics have shown that under-five mortality rate crashed by 58% between 1990-1995 and 2010-2019, with a sharp reduction from 93 deaths per 1,000 live births to 38 deaths per 1,000 live births (UN-IGME 2019). This drastic reduction pioneered an ambitious target of attaining at most 25 deaths per 1000 live births by 2030 in all countries as contained in the Sustainable Development Goals (SDGs) targets (SDG 3.2) (United Nations 2015), the ambition that would require critical understanding of places where the gaps are still huge. The reality, however, is that the chances of dying between birth and age 5 in least developed countries, Land-locked Developing Countries (LLDC) and Small Highland Developing States (SHDS) are not fewer than 40 deaths per 1,000 live births, which is about ten times the chances in Australia with 4 deaths per 1,000 live births and seven times those of mortality in Europe and North America with 6 deaths per 1,000 between 2010 and 2019 (UN-IGME 2019). The widespread regional disparity in child survival ensures that sub-Saharan Africa records the highest rate of under-five mortality estimated at 78 deaths per 1000 live births in 2018; translating to 1 in 13 children dying before their fifth birthday compared with 1 in 199 in developed world (UN-IGME 2019). Even within Africa, a child born in sub-Saharan Africa is three times as likely to die before his or her fifth birthday as a child born in Northern Africa (United-Nations, 2015a; United-Nations 2015b; United-Nations2019).
Over the years, studies on survival chances of under-five children in African countries had made abundance of findings. A majority of the studies have examined the socioeconomic and demographic determinants of child survival in single or multiple countries (Caldwell and McDonald 1982; Yaya et al. 2018) while some others have investigated the role of space (Kazembe et al. 2012; Gayawan et al. 2016; Golding et al. 2017; Li 2006; Balk et al. 2004; Ayoade 2018). Specifically, the recent studies by Golding et al. (2017) and Li et al. (2019) pooled several surveys and censuses data from multiple African countries and examined trend and spatial heterogeneity at subnational and national levels and, indeed, the studies identified spatial heterogeneity at all the levels, indicating that the variability often cross administrative/political boundaries, including national borders, and thus, suggesting that local conditions are important components of the risk of dying before age 5 years.
Higher income at individual and country levels often closely correlates with better health outcome for the country’s population including enhancement of child survival chances (Preston 1975). Thus, macroeconomic indicators and child mortality have been studied but there are instances of divergence outcomes regarding the relationships (Tejada et al. 2019; Pérez-Morenoa et al. 2016; Hojman 1996). O’Hare et al. (2013) substantiated the relationship between Gross Domestic Product (GDP) and mortality in under-five children through a random effects meta-analysis on previous studies and concluded that developing nations witness negative relationship between national income and under-five mortality. Van-Malderen et al. (2019) did a decomposition regression-analysis on measures of Gini-index to explore variability in under-five mortality among 32 sub-Saharan African countries with respect to child sex, place of residence, wealth index and mother’s level of education. Other research efforts shifted a bit, to deduce the effect of health-care accessibility, as O’Donnell (2007) and Hanmer et al. (2003) analytically confirmed that majority of death occurrences in the world are attributed to underutilization of existing and effective health-care interventions, as there was positive relationship between level of income and child immunization, which is a reliable way of increasing survival among young children.
There are several other individual- and macro-level indicators that have direct bearing with the survival chances of young children particularly in resource poor settings. For instance, individuals and households in most developing countries have disproportionate access to education as well as water and sanitation, and there exist inequality in effective coverage of essential health interventions within and between countries. Increasing urbanization in many African countries often lead to informal and sprawling settlements, and this further confound the poor sanitation conditions thereby increasing the risks of morbidity and mortality for young children (Angoua et al. 2018; Appiah-Effah et al. 2019). Further, food price inflation and trade openness particularly as they affect agricultural products have been shown to directly impact on the prevalence of underweight and stunting amongst young children due to the effects on the purchasing power of the caregivers especially those at the lower wealth stratum. These nutritional indicators are critical factors that inhibit the survival chances of young children. The level of government assistance to tradable agriculture improves child nutritional status especially for those children whose parent earn wages from agriculture (Arndt et al. (2016); Adjaye-Gbewonyo et al. 2019). While it would then be worthwhile to explore the effects of these and other similar variables on the dynamics of child mortality in the entire Africa, data that allow for long term exploration of temporal variations are often non-existence or where they exist, they are often characterised by wide spread missing observations.
Considering the substantial disparities in under-five mortality in Africa with respect to time, space and economic growth, a geo-spatial approach is essential to enhance interventions that would tackle the prominent challenges of improving survival among this sub-group of the population in the entire continent, as noted by various researchers. However, previous studies cited above have not adequately assessed trends in mortality over time, while those that explored both spatial and temporal variations, have been limited to the analysis of the levels of mortality (average mortality) without measuring how dispersed the variations could be over time across different locations. We undertake a national level estimates, which are critical for comparing performances across nations and the findings could be useful to international audience and donors. The study was structured to investigate trend in GDP level, a measure of a country’s economic growth and its relationship with child mortality in each of 41 African countries, and to fit a flexible spatio-temporal structured additive distributional log-normal model to mortality rates of the African countries covering 1980-2018. We settled for GDP ahead of other individual- or macro-level indicators as earlier mentioned due to availability of data for most of the countries and importantly, because it is the primary indicator for measuring the rate of growth of a country’s economy, and thus it can be used to determine the overall standard of living and health conditions of individuals in any economy. The modelling approach allows the two parameters of the log-normal model, mean and variance, to be linked with space, time and other possible covariates and thus, enabling the simultaneous assessment of the level and dispersion of under-five mortality across locations of the countries (Rigby and Stasinopoulos 2005; Klein et al. 2015; Somo-Aina and Gayawan2019).
Methods
Data
The motivating data for the study were sourced from the World Development Indicators managed by The World Bank and openly available at https://data.worldbank.org. The database contains top-quality international statistics on worldwide development and poverty alleviation indexes for over 200 countries of the world starting from 1960. We extracted data on under-five mortality rates from 1980 to 2018 because most of the countries do not have the data prior to 1980. Also, because the spatial technique requires that each spatial unit must share boundary with at least one other, countries which have the data but do not share international boundary with another e.g. Lesotho were excluded. In all, we pulled time series data on under-five mortality rate (death per 1000 live births) for 41 African countries (Fig. 1). Regarding GDP, some of the countries do not have the record beginning from 1980 and so, we collected those available and only used a descriptive method to study its relationship with child mortality. The credibility of data from the World Development Indicator is improved through the collaborative effort of statistical experts from national authorities, international development agencies and The World Bank. Specifically, the source of the mortality rate data are registration schemes captured by age-groups from censuses and sample survey data, which are commonly the case in low- and middle- income countries, where comprehensive registration systems are not attained. The United Nations Educational, Scientific, and Cultural Organization (UNESCO) Institute for Statistics works with statistical institutions in individual countries to compile the indicators.

Map of Africa showing the countries included in the study. Excluded countries are shaded
The Lognormal Distributional Regression Model
We assumed that the mortality rates follow a lognormal distribution. This distribution is considered suitable in a situation where the outcome variable grows multiplicatively, and it duly fits into heavily tailed right-skewed data having strictly positive values. If \( Y \sim {\text {lognormal} (\mu , \sigma ^{2})} \) then the probability density function (pdf) is given as:
where y is the response variable that depicts, in this case study, under-five mortality rates (deaths per 1,000 life births), with mean μ ∈R and variance σ2 > 0.
Considering the influence of an array of covariates, and the desire is to explore the influence of the covariates on the different parameters of the response distribution, 𝜗k, where 𝜗1 = μ and 𝜗2 = σ2, the distributional regression framework (Klein et al. 2015) gives accessibility to explore temporal and spatial correlations, unit or cluster definite heterogeneity simultaneously on all the parameters within a framework. Therefore, for a set of observations yi, i = 1,...,n, the distributional additive regression model for the kth parameter 𝜗k is expressed as:
where ηi is an appropriately chosen link function for the different parameters such as the log link for the mean (μ) and logit for the variance (or standard deviation, which is considered here), to ensure positivity; \(S^{\vartheta _{k}}_{(str)}\) corresponds to the spatial structured component for the kth parameter, \(S^{\vartheta _{k}}_{(unstr)}\) is unstructured random term, \(T^{\vartheta _{k}}\) is the temporal term, and \({(ST)}^{\vartheta _{k}}\) accounts for the spatio-temporal variations. For implementations, the complete model was explicitly specified as follows:
Note that only the structured spatial and temporal effects were considered for the sigma parameter.
A Bayesian approach is considered appropriate for estimating the parameters of the model in order to ensure favourable properties such as smoothness for the temporal and spatial terms and shrinkage in the case of the unstructured random effect. The Bayesian inference assumes that all parameters are random variables upon which appropriate prior distributions must be assigned. Bayesian version of the penalized splines (P-splines) was adopted for the temporal effect (Eilers and Marx 1996; Lang and Brezger 2004). This allows for the non-parametric estimation of the temporal term, T as a linear combination of B-splines (basis splines). We considered cubic B-splines based on 20 equidistant knots, which typically induce enough flexibility to capture severe non-linearity. The prior for this was based on second-order random walk.
For the structured spatial and spaio-temporal components, we considered the countries as discrete set of spatial locations si,s ∈ (1,....,S), and used a Markov random field prior that considers the neighbourhood structure of the countries through a binary structure, whereby neighbouring locations that share common boundary are assigned a weight of 1 while 0 is allocated to non-neighbouring ones, and separate regression coefficient is estimated for each region, based on the interaction with time in the case of spatio-temporal. To enforce spatial smoothness, we consider a Gaussian Markov random field prior that induces a penalty where differences between spatially adjacent regions were penalised. The unstructured random component was assigned an exchangeable independent and identically distributed normal prior. More detail about the model components and possible prior distributions are extensively discussed in Fahmeir et al. (2013).
The posterior inference was based on a generic Markov chain Monte Carlo (MCMC) simulation approach as developed by Klein et al. (2015), where proposal densities for blocks of regression coefficients are obtained from a locally quadratic approximation of the log full conditionals.
To implement the model, six models of different specifications were considered by sub-setting the various components of the model for the mean parameter while keeping the temporal and structured spatial components for the sigma parameter because it measures variability. To goal was to explore various components of the spatio-temporal model based on model performance. Model diagnostic was based on deviance information criterion (DIC). The complete models considered and values of the DIC are presented in Table 1. For all the models, we performed 33,000 iterations, discarded the first 3,000 as burn-in and selected every 30th observation for parameter estimation. The Markov chains generated through these processes were investigated through trace plots to ascertain mixing and convergence.
Results
Before proceeding to the results of the spatio-temporal analysis, Fig. 2 presents the box plot of the mortality data from which two things are immediately obvious. First, the plot does not present evidence of outliers in the data set which implies that for the 39 years period under consideration (1980-2018), none of the 41 African countries performed extremely badly or extremely well in child mortality record, relative to the others, to have stood out as outlier. Second, there is evidence that overall, under-five mortality rates are declining steadily in Africa particularly from year 2000, which was around the period that the Millennium Development Goals (MGD) came on board and thus, the decline could be attributed to the efforts. Figure 3 shows the density plots of the mortality rates; presenting the curves for the complete data and for the periods 1980-1989, 1990-1999, and 2000-2018. The intention was to examine how mortality rates fared over the different decades in the continent. The Figure shows that the distribution for all the data is right-skewed, which further justifies the use of lognornal model. The vertical line in the Figure is the median for all years and thus, the median for years 2000-2018 is to the left, lower than the the overall median but those for the other years are to the right thus, greater.

Box plot showing the statistics of under-five mortality rates in African countries from 1980 to 2018

Density plot of under-five mortality rates in African countries from 1980 to 2018
The relationships between GDP and child mortality rates for the African countries are presented in Fig. 4. The red line shows the trends in the mortality rates while the blue line presents those for the GDP. As evident, child mortality rates and GDP mostly follow each other in inverse relation but not for every country. Countries that experience clear-cut inverse relationship include Algeria, Botswana, Burkina Faso, Cameroon, Egypt, Kenya, Morocco, Namibia, Rwanda, Senegal, Tunisia, Uganda, and South Africa though for a number of them, the relationship became obvious after year 2000. Countries without clear-cut inverse relationship or where the downward trend in mortality cannot be viewed to have correspond with growth in GDP are: Angola, Benin, Chad, DR Congo, Gabon, Gambia, Guinea, Mali, Mauritians, Niger, Nigeria, Sierra Leone, and Sudan.

Relationship between GDP and child mortality based on individual African country (blue indicates GDP, red indicates child mortality)
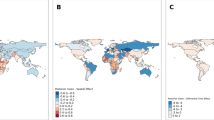
Results of the spatio-temporal analysis as presented in Figs. 5, 6, 7 and 8 are based on those for model 6, which provides the least DIC value as specified in Table 1 and thus, considered the best. The results for the temporal pattern show the posterior mean (black lines) and 95% credible interval (blue lines) for the mean (Fig. 5a) and standard deviation (Fig. 5b) components. The findings reveal that indeed, over the years, there has been a rapid downward trend in levels of child mortality in Africa. However, the standard deviation component shows a consistent zigzag pattern over the years reaching its lowest value in 2017, which imply the year in which variation in child mortality rates was at its minimum across the African countries. Figure 6 shows changes in the levels of mortality rates over time across the countries. During the period 1980-1984, child mortality rates were highest mostly in the northern African countries of Algeria, Morocco, Tunisia, Libya, Egypt, and Ethiopia, in the eastern part of the continent but lower for most countries in the western, central and southern parts. However, for every five-year interval of time, there were considerable changes in the spatial patterns such that at the close of the study period (2015-2018), there was about complete reversal of the pattern that saw some of the countries with lower estimates at the onset of the study period having higher rates. During the years 2015-2018, countries such as Nigeria, Chad, Sudan, Central Africa Republic, Benin, Guinea, and Mauritiana have the highest estimates of level of mortality rates and, interestingly, all these countries were among those with the lowest estimates during the 1980-1984, the starting period. The mortality rate estimates were however lowest during 2015-2018 for countries such as Senegal, Liberia, Niger, Libya, Egypt, Kenya, Uganda, Angola, and Zambia.

Estimates trend in child mortality for a the mean component and b sigma component

Spatio-temporal distribution of child mortality in Africa

Structured and unstructured spatial variations for the mean component

Structured spatial effects on the sigma parameter
Findings from the posterior estimates of the structured and unstructured spatial components of the model presented in Fig. 7 reveal that the structured effects does not present notable differences in the levels of child morality rates as does the unstructured component. The implication is that, when the neighbourhood structures of the countries are considered in estimating the rates, the estimates are not notably different. However, the unstructured random component show lower estimates in mostly countries in the northern and southern parts of the continent namely: Algeria, Morocco, Tunisia, Libya, Egypt, Namibia, Botswana, Zimbabwe, Gabon and Ghana. Estimates for the standard deviation component presented in Fig. 8 show, for each of the countries, the amount of variation in the rates for the 39 years study period. It should be noted that higher estimates indicate locations that experienced huge changes in level of mortality rates over the years while lower estimates show that the changes were minimal. The findings show a clear divide in the pattern of variations with countries in the southern part of the continent, two in the northern part and Rwanda experiencing the highest variations in mortality rates over the 39 years period whereas, a cluster of countries in the western coast had only minimal variability.
Discussions
A sequence of Bayesian spatio-temporal models and the predictive influence of GDP were highlighted to explore under-five mortality rates in 41 African countries using country-level data sourced from the World Development Indicators managed by The World Bank from 1980 to 2018. The relationship between the mortality rates and the individual country’s macroeconomic indicator measure through GDP was descriptively accessed due to unavailability of GDP data for some of the countries beginning from 1980. Following the concept of distributional regression, the two-parameter lognormal model allows us to examine not only the level of mortality but also the measure of variability over time and across space in the continent.
We found substantial variations in mortality rates across the 41 countries over the period of 1980 − 2018 with patterns of clustering formed among neighbouring countries. For instance, between the year 1980 − 1984 under-five mortality rates were highest in the northern region, featuring countries like Algeria, Morocco, Tunisia, Libya, and Egypt, while countries like Niger, Nigeria, and Chad in the west, Cameroon, Congo and Angola in the central, and Namibia, Bostwana and South Africa had the least mortality rates, except for the Eastern region, where some traces of heterogeneity was observed. Geographical homogeneity is further witnessed between the year 2000 − 2004, as countries in the northern region commonly attained reduction in under-five mortality while those in the southern region experienced slight increment. This regional spatial correlation persisted till the year 2015 − 2018, as most countries in West and Central Africa like Nigeria, Benin, Guinea, Mauritania, Cameroon, Central African Republic and Chad had the highest mortality rate, while countries like Kenya, Uganda Namibia, Botswana and Zambia and South Africa were characterized with lower under-five mortality rates. This similar pattern of variation among countries with common boundaries could be attributed to comparable child survival intervention policies and programmes among neighbouring countries, matching climatic conditions, public responses to intervention programmes, governmental support, community participation and ownership for intervention sustainability, societal norms and cultural beliefs, civil war, maternal and child healthcare accessibility and utilization as well as possible uniformity in influence of childhood diseases such as malaria, diarrhoea and pneumonia (UN-IGME 2019; Yaya et al. 2018; Wagner et al. 2018; Burke et al. 2016; Kazembe et al. 2012; Hojman 1996; Rutherford et al. 2010; Caldwell 1990). Similarities in socioeconomic factors as they affect mothers and caregivers, and similarities in fertility levels are other possible factors that could have lead to spatially correlated child mortality rates within the African continent (Gayawan et al. 2016; Pezzulo et al. 2016; Gayawan and Turra 2015; Balk et al. 2004; Caldwell and McDonald 1982).
Findings from the temporal analysis generally reveal a sharp and consistent decline in under-five mortality in Africa. However, a close look at individual countries based on the plots in Fig. 4 and the spatio-temporal maps reveals that the decline is not uniform across board as some countries experienced much more decline than others. Notably, all northern African countries have witnessed more reduction over the years than other countries in the continent (Iqbal and Kiendrebeogo 2014). Such determinants as income growth, education stock, large scale public spending on health, urbanization and food sufficiency that ensure the elimination of wide spread under-nutrition have been identified as the drivers of lower child mortality in North Africa and the Middle East (Iqbal and Kiendrebeogo 2014; Bjegovic-Mikanovic et al. 2019; Boutayeb and Helmert 2011). Universal immunization coverage and appropriate care seeking for sick children are also factors that help shape mortality in northern Africa (Ministry of Health and Population Egypt 2014). Countries in the eastern part of the continent especially Ethiopia witnessed some highly impactful interventions in water supply, sanitation and hygiene (WASH) and in public health policies that improved maternal and child health leading to enhanced survival chances of children (Doherty et al. 2016; Kipp et al. 2016). Southern African countries have also witness reduction in child death over the years however, the progress in the region has been hampered by the persistent high scourge of HIV, which has continued to be the largest cause of fatalities among young children (Tlou et al. 2017). On the other hand, the reduction in the case of West and Central African countries has been minimal with some, e.g. Nigeria still among the countries with highest rates in the world. Some of the traceable causes of this are the high incidence of childhood contagious diseases, such as diarrhoea, pneumonia, malaria, measles and meningitis as well as wide spread malnutrition and low use of maternal and child healthcare services (UN-IGME2019; Yaya et al. 2018; Gayawan and Omolofe 2016). Overall, given the current tempo of reduction, a number of countries have the potentials of attaining the targets of the SDGs while others would require additional interventions.
The findings from the analysis of trends in economic growth of the individual countries and mortality rates confirm the possible divergence relationship between macroeconomic indicators and child survival. The possible varied relationship could occur because, normally, economic growth implies multi-sectoral progress though it cannot alone yield sufficient reduction except when used to purchase physical, social and environmental changes that lower mortality (Bishai et al. 2016; Subramanian and Corsi 2014). However, GDP per capital was found to account for 12% reduction in child mortality in low and medium income countries between 1990 and 2010 (Kuruvilla et al. 2014; Bishai et al. 2016). Improvement in GDP together with progress across health and other sectors contributed largely to the downward trend of child mortality in Egypt (Ministry of Health and Population Egypt 2014). Countries like China, Bangladesh, and Rwanda followed diverse economic strategies and attained huge progress in the indicators while countries like India, Nigeria and others as also revealed by this study experienced fast economic growth which however, do not make commensurate progress in maternal and child health indicators (Kuruvilla et al. 2014).
The study suffers from some limitations. Health, and nutrition related outcomes as well as other socio-demographic determinants of child mortality were not accounted for in the spatio-temporal model and thus, their effects on the residual variations could not be ascertained. Also, the analysis was based on aggregated country-level data which would have concealed within country variations. These limitations notwithstanding, the study provides some glean insight into levels and measure of variability of geographical and temporal patterns of mortality across the continent.
Conclusion
This study establishes the fact that over the years, child mortality experienced by Africa countries are comparable as no country stood out as outlier whether for better or for worst. The space time framework adopted offers the opportunities of examining the variations in child mortality in Africa from different perspective rather than only concentrating on the mean level of mortality or aggregate spatial-only or temporal-only analysis. The key findings from the study are that child mortality levels are generally falling in the continent, but the reduction are faster in some countries than in others, and the relationship with GDP are not always inverse. There were countries particularly on the western coast of the continent who had lower mortality levels relative to others in the 1980s but these countries turned out to record the highest rates during the 2015-2018. Also, variability in child mortality over the study period were higher among countries in the southern part of the continent as well as in three others: Rwanda, Tunisia and Egypt but lowest among most countries in the western coast. Countries with minimal changes in mortality levels over time need to adopt effective local strategies that could cut down on their current number or borrow a leaf from those whose approaches are considered effective. For instance, as identified to have been effective in places like Egypt, it would be necessary to ensure universal immunization coverage and timely healthcare provided for sick children to mitigate the impact of childhood illnesses that are rampart in some African countries. Improvement in WASH and public health policies capable of improving maternal and child healthcare-seeking behaviour could also enhance the survival chances of children across Africa.
Data Availability
The data set used is openly available
Code Availability
The code used for the study can be made available upon request
References
Adjaye-Gbewonyo, K., Vollmer, S., Avendano, M., & Harttgen, K. (2019). Agricultural trade policies and child nutrition in low- and middle-income countries: a cross-national analysis. Globalization and Health, 21.
Angoua, E.L.E., Dongo, K., Templeton, M.R., Zinsstag, J., & Bonfoh, B. (2018). Barriers to access improved water and sanitation in poor peri-urban settlements of Abidjan, Cote d’Ivoire. PloS One, 13, e0202928.
Appiah-Effah, E., Duku, G.A., Azangbego, N.Y., Aggrey, R.K.A., Gyapong-Korsah, B., & Nyarko, K.B. (2019). Ghana’s post-MDGs sanitation situation: an overview. Journal of Water Sanitation and Hygiene for Development, 9, 397–415.
Arndt, C., Hussain, M.A., Salvucci, V., & Osterdal, L.P. (2016). Effects of food price shocks on child malnutrition: The Mozambican experience 2008/2009. Economics and Human Biology, 22, 1–13.
Ayoade, M.A. (2018). Spatio-temporal patterns of under 5 mortality in Nigeria. SSM Population Health, 6, 116–124.
Balk, D., Pullum, T., Storeygard, A., Greenwell, F., & Neuman, M. (2004). A spatial analysis of childhood mortality in West Africa. Population, Space and Place, 10, 175–216.
Bishai, D.M., Cohen, R., Alfonso, Y.N., Adam, T., Kuruvilla, S., & Schweitzer, J. (2016). Factors contributing to maternal and child mortality reductions in 146 low- and middle-income countries between 1990 and 2010. PLoS ONE, 11, e0144908.
Bjegovic-Mikanovic, V., Abousbie, Z.A.S., Breckenkamp, J., Wenzel, H., Broniatowski, R., Nelson, C., Vukovic, D., & Laaser, U. (2019). Social inequalities, regional disparities and healthinequity in North African countries. International Journal for Equity in Health, 14, 1–9.
Boutayeb, A., & Helmert, U. (2011). Social inequalities, regional disparities and healthinequity in North African countries. International Journal for Equity in Health, 10.
Burke, M., Heft-Neal, S., & Bendavid, E. (2016). Sources of variation in under-5 mortality across sub-Saharan Africa: a spatial analysis. Lancet Glob Health, 4, 12.
Caldwell, J. (1990). Cultural and social factors influencing mortality levels in developing countries. The ANNALS of the American Academy of Political and Social Science, 510(1), 44–59.
Caldwell, J., & McDonald, P. (1982). Influence of maternal education on infant and child mortality: Levels and causes. Health Policy and Education, 2, 251–267.
Doherty, T., Rohde, S., Besada, D., Kerber, K., Manda, S., Loveday, M., Nsibande, D., Daviaud, E., Kinney, M., Zembe, W., Leon, N., Rudan, I., Degefie, T., & Sanders, D. (2016). Reduction in child mortality in ethiopia: Analysis of data from demographic and health surveys. Journal of Global Health, 6(2).
Eilers, P., & Marx, B. (1996). Flexible smoothing with b-splines and penalties. Statistical Science, 11, 89–121.
Fahmeir, L., Kneib, T., Lang, S., & Marx, B. (2013). Regression methods, models and application. Springer: Berlin.
Gayawan, E., Adarabioyo, M., Okewole, D., Fashoto, S., & Ukaegbu, J. (2016). Geographical variations in infant and child mortality in West Africa: a geo-additive discrete-time survival modelling. Genus, 72(1), 1–20.
Gayawan, E., & Omolofe, T. (2016). Analyzing Spatial Distribution of Antenatal Care Utilization in West Africa Geo-additive Zero-Inflated Count Model. Spatial Demography, 4, 245–262.
Gayawan, E., & Turra, C. (2015). Mapping the determinants of child mortality in Nigeria estimates from mortality index. African Geographical Review, 34, 1–25.
Golding, N., Burstein, R., Longbottom, J., Browne, A.J., Fullman, N., Osgood-Zimmerman, A., Earl, L., Bhatt, S., Cameron, E., Casey, D.C., Dwyer-Lindgren, L., Farag, T.H., Flaxman, A.D., Fraser, M., Gething, P.W., Gibson, H.S., Graetz, N., Krause, L.K., Kulikoff, X.R., Lim, S.S., Mappin, B., Morozoff, C., Reiner-Jr, R.C., Sligar, A., Smith, D.L., Wang, H., Weiss, D.J., Murray, C., Moyes, C.L., & Hay, S.I. (2017). Mapping under-5 and neonatal mortality in Africa, 2000-15: a baseline analysis for the Sustainable Development Goals. Lancet, 390(10108), 2171–2182.
Hanmer, L., Lensink, R., & White, H. (2003). Infant and child mortality in developing countries: Analysing the data for robust determinants. The Journal of Development Studies, 40(1), 101–118.
Hojman, D.E. (1996). Economic and other determinants of infant and child mortality in small developing countries: the case of Central America and the Caribbean. Applied Econoics, 28, 281–290.
Iqbal, F., & Kiendrebeogo, Y. (2014). The reduction of child mortality in the Middle East and North Africa.
Kazembe, L., Clarke, A., & Kandala, N. (2012). Childhood Mortality in sub-Saharan Africa: cross-sectional insight into small-scale geographical inequalities from census data. BMJ Open, 2(5).
Kipp, A., Blevins, M., Haley, C., Mwinga, K., Habimana, P., Shepherd, B., Aliyu, M., Ketsela, T., & Vermund, S. (2016). Factors associated with declining under-five mortality rates from 2000 to 2013: an ecological analysis of 46 African. British Medical Journal Publishing Group, 6(1).
Klein, N., Kneib, T., Lang, S., & Sohn, A. (2015). Bayesian structured additive distributional regression with an application to regional income inequality in German. The Annals of Applied Statistics, 9(2), 1024–1052.
Kuruvilla, S., Schweitzer, J., Bishai, D., Chowdhury, S., Caramani, D., Frost, L., Cortez, R., Daelmans, B., Francisco, A., Adam, T., Cohen, R., Alfonso, Y.N., Franz-Vasdeki, J., Saadat, S., Pratt, B.A., Eugster, B., Bandali, S., Venkatachalam, P., Hinton, R., Murray, J., Arscott-Mills, S., Axelson, H., Maliqi, B., Sarker, I., Lakshminarayanan, R., Jacobs, T., Jacks, S., Mason, E., Ghaffar, A., Mays, N., Presern, C., Bustreo, F., & on behalf of the Success Factors for Women’s and Children’s Health study groups. (2014). Success factors for reducing maternal and child mortality. Bulletin of the World Health Organization, 92, 533–544.
Lang, S., & Brezger, A. (2004). Bayesian p-splines. Journal of Computational and Graphical Statistics, 13, 183–221.
Li, H. (2006). Bayesian hierarchical models for spatial count data with application to fire frequency in British Columbia. University of Victoria.
Li, Z., Hsiao, Y., Godwin, J., Martin, B., Wakefield, J., & Clark, S. (2019). Changes in the spatial distribution of the under-five mortality rate: small-area analysis of 122 DHS surveys in 262 subregions of 35 countries in Africa. PLoS ONE, 14(1), e0210645.
Ministry of Health and Population Egypt, Partnership for Maternal, Newborn & Child Health. (2014). Success factors for women’s and children’s health: Egypt.
O’Donnell, O. (2007). Access to health care in developing countries: Breaking down demand side barriers. Cadernos de Saude Pú,blicá, 23, 2820–2834.
O’Hare, B., Makuta, I., Chiwaula, L., & Bar-Zeev, N. (2013). Income and child mortality in developing countries: a systematic review and Meta-Analysis. Journal of the Royal Society of Medicine, 106(10), 408–14.
Pérez-Morenoa, S., Blanco-Arana, M., & Bárcena-Martín, E. (2016). Economic cycles and child mortality: a cross-national study of the least developed countries. Economics & Human Biology, 22, 14–23.
Pezzulo, C., Bird, T., Utazi, E., Sorichetta, A., Tatem, A., Yourkavitch, J., & Burgert-Brucker, C. (2016). Geospatial modeling of child mortality across 27 countries in Sub-Saharan Africa. DHS Spatial Analysis Report No. 13. National Population Commission, Federal Republic of Nigeria, Abuja, and ICF International, Rockville, Maryland USA.
Preston, S. (1975). The changing relation between mortality and level of economic development. Population Studies, 29, 231–248.
Rigby, R., & Stasinopoulos, D. (2005). Generalized additive models for location, scale and shape. Applied Statistics, 54, 507–554.
Rutherford, M., Mulholl, K., & Hill, P. (2010). How access to health care relates to under-five mortality in sub-saharan africa: systematic review. Tropical Medicine and International Health, 15(5), 508–519.
Somo-Aina, O., & Gayawan, E. (2019). Structured additive distributional hurdle Poisson modelling of individual fertility levels in Nigeria. Genus, 75, 20.
Subramanian, S.V., & Corsi, D.J. (2014). Association among economic growth, coverage of maternal and child health interventions, and under-five mortality: A repeated cross-sectional analysis of 36 sub-Saharan African countries.
Tejada, C.A.O., Triaca, L.M., Liermann, N.H., Ewerling, F., & Costa, J.C. (2019). Economic crises, child mortality and the protective role of public health expenditure. Ciencia & Saú,de Coletivâ, 24, 4395–4404.
Tlou, B., Sartorius, B., & Tanser, F. (2017). Space-time variations in child mortality in a rural South African population with high HIV prevalence (2000–2014). PLoS ONE, 12, e0182478.
UN-IGME. (2019). Levels and Trends in Child Mortality: Report 2019.
United Nations. (2015). Transforming our world: the 2030 agenda for sustainable development.
United-Nations. (2015a). World Mortality Report, 2015. Department Of economic and social affairs, Population Division, New York.
United-Nations. (2015b). World Population Prospect The 2015 Revision: Key Findings and advance tables. Department of economic and social affairs, Population Division, New York.
United-Nations. (2019). World Population Prospect 2019: Highlight (ST/ESA/SER.a/423) department of economic and social affairs, Population Division, New York.
Van-Malderen, C., Amouzou, A., Barros, A., Masquelier, B., Van-Oyen, H., & Speybroeck, N. (2019). Socioeconomic factors contributing to under-five mortality in sub-Saharan Africa: a decomposition analysis. BMC Public Health, 19(2019), 760.
Wagner, Z., HeftNeal, S., Bhutta, Z., Black, R., Burke, M., & Bendavid, E. (2018). Armed conflict and child mortality in Africa. Lancet, 392 (10150), 857–865.
Yaya, S., Bishwajit, G., Okonofua, F., & Uthman, O. (2018). Under five mortality patterns and associated maternal risk factors in sub-Saharan Africa: A multi-country analysis. PLos One, 13(10), e0205977.
Funding
Not applicable
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interests
None to declare (Not applicable)
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Gayawan, E., Somo-Aina, O. & Awe, O. Spatio-Temporal Dynamics of Child Mortality and Relationship With a Macroeconomic Indicator in Africa. Appl. Spatial Analysis 15, 143–159 (2022). https://doi.org/10.1007/s12061-021-09393-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12061-021-09393-4