
Abstract
Objectives
To analyze the effect of Official Development Aid (ODA) dollars on child mortality over the course of the United Nation’s Millennium Development Goals initiative.
Methods
The relationship between child mortality and Official Development Aid over the duration of the Millennium Development Goals (2000–2015) is examined here using a longitudinal panel of country-level data from the World Bank and the United Nations. An Ordinary Least Squares regression approach was used with country-level fixed effects. Models were estimated for the full sample and by Human Development Index development strata (high, medium, and low developed countries) with clustered standard errors.
Results
ODA appears to be most strongly associated with decreases in child mortality in Medium Developed Countries. Every one dollar per capita increase in ODA is associated with a 0.035 decrease in child deaths per 1000 births.
Conclusions
Significant gains were made in decreasing child mortality over the last 15 years. The need for more progress remains. Allocation of ODA to developing countries can be an effective policy tool in achieving public health goals.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
The year 2015 marked the conclusion of the Millennium Development Goals (MDG), a historic policy initiative lead by the United Nations (UN). The UN, comprised of 189 member nations, as well as other multinational agencies developed the MDG to reduce global poverty and hunger and improve global public health and equality. As we move further into the new millennium, it is critical for scholars and policy makers to evaluate whether the goals of the MDG initiatives were accomplished. This study focuses on the use of Official Development Aid dollars (ODA) as a tool to accomplish gains in child health, specifically by decreasing the mortality rate for children less than 5 years of age.
The MDG focused on eight areas, including education, child and maternal mortality, hunger, poverty, gender equality, infectious disease reduction (especially HIV/AIDS and malaria), environmental sustainability, and global partnerships. One of the most ambitious, critical goals of the MDG initiative was the goal to reduce child mortality (number of deaths prior to age 5 per 1000 live births) by two-thirds (from 1990 levels). Even though child mortality has been cut in half since 1990, 30,000 children were dying every day in 2000 at the inception of the MDG. Today, approximately 16,000 die daily, most from preventable causes (United Nations 2015a, b).
Income disparities and geographic (rural versus urban) health disparities are two of the greatest contributors to child mortality rates (Tacke and Waldmann 2013; Mujica et al. 2014). Other studies have found variables that contribute to infant or child mortality reduction (infant mortality is included in child mortality), including public health care expenditure, health factors (including access to care and vaccinations), educational outcomes, access to sanitation and safe water, female education, maternal mortality, life expectancy, and GDP (Mahy 2003; Sartorius 2014; Goli and Arokiasamy 2014).
To achieve its goals, one of which was to reduce child mortality, the MDG initiative focused on investing Official Development Aid. Official Development Aid (ODA) is defined by the Organization for Economic.
Cooperation and Development (OECD) as:
“Monetary resources and concessions provided by official agencies, including state and local governments…to countries and territories … administered with the promotion of the economic development and welfare of developing countries as its main objective” (OECD 2015).
ODA has long been preferred over private aid flows because it is meant to be a stable, long-term commitment from donor governments (United Nations 2015c). For example, ODA allows recipient governments to make long-term plans to build new infrastructure, or to provide salaries or scholarships for necessary personnel (UNDP 2011).
While ODA has been the preferred funding mechanism for international development over the past 70 years, it is controversial because the funding is not always associated with intended outcomes. Extant literature has cited that confounding variables include a lack of good governance, aid dependence, poor absorptive capacity, poverty traps, conflict, unstable or unpredictable aid flows, aid fungibility, and misalignment of the objectives of a donor with the needs of a recipient (Dietrich 2011; Easterly 2001; Knack 2000; Ovaska 2003; Sen 1999). While the causal mechanism between aid dollars and population health outcomes has been difficult to establish and the use of ODA remains controversial, the UN continues to identify ODA as one of the primary tools used to forward its goals (United Nations 2015d).
Understanding the mechanisms by which child mortality is affected may impact policy makers’ decisions on the allocation of ODA. This study is an empirical evaluation of the effect of ODA on child mortality during the MDG initiative, which spanned from 2000 to 2015. The primary research question is whether ODA is a significant predictor of child (<5 years) mortality. We hypothesize that ODA is a significant predictor of child mortality; specifically, it is expected that as ODA increases, child mortality will decrease. To investigate this relationship, a longitudinal panel of country-level data is used.
Methods
Data for this study are from the World Bank’s World Development Indicators (WDI) dataset (The World Bank 2015). These data include demographic and economic indicators, as well as health, education, and employment indicators. For the purposes of this analysis, the observation period is limited to 2000 through 2015, the duration of the MDG initiative. The study design is a quasi-experimental, longitudinal analysis using country-level panel data from the WDI. The unit of analysis is the country, where each country is observed annually for 16 years. A total of 183 countries are included in the original WDI dataset, but for all analyses countries with an annual change in child mortality of 5% or more (due to a natural disaster or war) are excluded as outliers. The unit of analysis is the country-year—the sample of 183 countries over the 16 year time frame (excluding outliers) yielded a full sample size of 2864. Additional data regarding the Human Development Index and development classification of nations come from the United Nations (United Nations 2014). The panel dataset used in this study is strongly balanced.
Data were stratified based on the UN Human Development Index (HDI) levels from the year 2000. The HDI divides countries into four groups, and defines them as Low, Medium, High, or Very High developed based on GDP, life expectancy, and education variables. Strata were defined by the baseline year (2000 levels) and countries were classified in their year 2000 stratum for the entire observation period. High and Very High developed countries were aggregated into a single stratum due to the limited number of observations—most countries receiving ODA are not in these strata, so the two groups were combined.
Child mortality served as the dependent variable in this analysis, operationalized as the number of child deaths (<5 years of age) per 1000 live births. ODA per capita was the independent variable of interest. It is operationalized in two ways; as current dollars per capita, and as current dollars per capita squared. Squared per capita ODA was also created and included in the models to allow for nonlinearity of the examined relationship.
Control variables selected for the model were those supported by the literature as being significant predictors of infant and child mortality. Each of these variables were also tested and were confirmed for inclusion with a correlation coefficient threshold of |0.45| or more. Controls include adolescent fertility (births per 1000 females aged 15–19), female mortality (deaths per 1000 women in the population), aggregated life expectancy (measured in years), the tuberculosis detection rate, the percent of the population with access to sanitation, the percent of the population with access to safe water, the rate of anemia in both pregnant women and in children under five, the aggregated immunization rate of both measles and diphtheria, the gross domestic product per capita (in 2012 USD), the female rate of primary school enrollment as a percent of male enrollment, and the female rate of primary school completion. In addition, year and country-level fixed effects were used to control for time and time-invariant country-level variation, respectively. The full sample descriptive statistics are included in Table 1.
Models
We hypothesized that ODA was a significant predictor of child mortality; specifically, it was expected that when ODA increased, child mortality decreased. To estimate the relationship between ODA and child mortality, an Ordinary Least Squares multiple regression approach was used. Ordinary Least Squares is the preferred estimation approach as the dependent variable (child mortality) is continuous, as is the independent variable of interest (ODA, measured in dollars per capita). Models were estimated for the full sample of countries, and then disaggregated by HDI strata to capture differences occurring for various levels of development.
Five models were estimated for the full sample and each development stratum to examine the relationship between child mortality and ODA. The first was a simple regression model that included no controls. Each subsequent model added control variables. The fifth model controlled for all selected variables and added a fixed effects term to control for unobservable variation within countries. The last model, which included all controls, year, and country-level fixed effects is the preferred model, as it provides the best fit for the data and includes controls previously found in the literature to be significant predictors of child mortality.
In addition to disaggregating the sample by development level and estimating the models in multiple iterations from simple to complex, additional sensitivity analyses were performed to ensure robustness of results. The functional form of the dependent variable, child mortality, was tested in a number of different ways for goodness of fit. Alternative specifications included yearly change, progress toward goal, and yearly percent change. The direct measurement (deaths per 1000 live births) is preferred, as it controls for the national population and provided the best fit.
To further ensure the robustness of models and results, we conducted a Fisher-type unit root test and were able to reject the null that the panel does contain a unit root. The p value of the unit root analysis was p < 0.001, leading us to reject the null and conclude that the panel is stationary and strongly balanced. In estimating the fixed effects models, we understand that serial-autocorrelation can occur. For this reason, we have now re-estimated all fixed effects models by clustering at the country-level. The resulting standard errors are completely robust to any kind of serial correlation and heteroskedasticity.
The functional form of the independent variable, official development aid received (ODA), was also tested in a number of different ways. Alternative forms included per capita receipt, logged per capita receipt, squared per capita receipt, and percent change in per capita receipt. Per capita receipt is the preferred form, as it controls for population and provided the best fit. Squared per capita receipt is also included in the model to allow for nonlinearity of the relationship between child mortality and ODA. All analyses were performed with STATA v.14.0.
Results
Table 2 shows the variable means and standard deviations divided into three strata: Low Developed Countries (LDC), Medium Developed Countries (MDC), and High Developed Countries (HDC), which is an aggregate of High and Very High Developed countries as classified by the 2000 Human Development Index (HDI). As one might expect, LDCs have a lower GDP, life expectancy, female primary enrollment and completion rates, as well as lower rates of access to sanitation and safe water, lower immunization rates, and lower tuberculosis detection rates when compared to MDCs and HDCs. MDCs have similarly lower rates than HDCs. LDCs also experience the highest rates of adolescent fertility, female mortality, and anemia in both children and pregnant women, while HDC have the lowest.
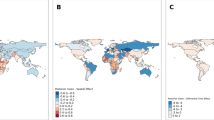
For the full sample, mean child mortality during the study period was approximately 43 deaths per 1000 live births. Over the observation period, child mortality decreased by an average of 3.75 percent annually. Mean ODA per capita over the observation period is $92.93 (2015 US dollars). Over the observation period, ODA per capita increased by approximately 17 percent annually. Results for the first set of OLS models, estimated on the full sample of countries, are reported in Table 3. The fifth and most stringent model shows a significant negative relationship between child mortality and ODA per capita. An ODA increase of one dollar per capita is associated with a child mortality decrease of 0.02 deaths per thousand live births. Both ODA and the ODA squared term are statistically significant (at the p < 0.10 and p < 0.05 levels respectively). Including a quadratic term in the model allows for the expression of non-linear relationship, and with both coefficients we calculated the tipping point of the ODA association with child mortality. The overall tipping point for the full sample is $142.85 per person. This is compared to $92.93, which is the average level of per capita ODA in the full sample.
All other controls were confirmed to have a significant relationship with child mortality except for adolescent fertility. The strongest relationship in the model is observed to be child mortality is life expectancy. As life expectancy increases by 1 year, child mortality decreases by 7.97 deaths per 1000 live births (p < 0.01).
Per capita GDP has a small but significant positive relationship with child mortality (p < 0.01). Female education in the form of primary enrollment rate (compared to the number of male enrollees) is strong and significant (p < 0.01). Every one percent increase in female primary enrollment is associated with a decrease of 0.0054 deaths per 1000 births in child mortality. Access to both sanitation and safe water both have almost as strong a negative relationship with child mortality as female primary enrollment, with each percent increase in access associated with 0.0052 and 0.0044 reductions respectively (p < 0.01).
There is no significant relationship found between ODA and child mortality in the most developed countries. There is a very significant negative relationship with adolescent fertility; every additional woman of 1000 between the ages of 15 and 19 giving birth is associated with a 0.031 decrease in child mortality. Female mortality also has a negative and significant relationship with child mortality. A one unit increase in female mortality is associated with a child mortality decrease of 0.15 deaths per 1000 live births (p < 0.01).
Life expectancy still appears to be the most significant variable in reducing child mortality. Every year increase in life expectancy is associated with a decrease in child mortality of 2.84 deaths per every 1000 live births (p < 0.01). The results for high-developed countries are shown in Table 4 below.
The relationship between ODA and child mortality appears to be quite different for MDCs than the HDCs. For every dollar per capita increase in ODA, there is a 0.035 decrease in child deaths per 1000 births. There is also a significant and positive relationship with the square ODA term, demonstrating a tipping point at $203.48 of per capita spending.
There is not a significant relationship with adolescent mortality, but female mortality is a strong negative predictor; for every additional death per 1000, child mortality decreases by 0.19 deaths. Other significant controls in the Medium Developed Countries include life expectancy, sanitation access, child anemia, water access, pregnant anemia, immunization rate, and the female completion rate. Full results for the medium and low devleoped country models are provided in Tables 5 and 6, respectively.
There is no significant relationship between child mortality and ODA in low developed countries. There is also no demonstrable relationship between child mortality and adolescent fertility or GDP per capita. Negative and significant relationships with child mortality in low developed countries are observed with female mortality, life expectancy, tuberculosis detection rate, sanitation access, safe water access, child anemia, the immunization rate, and the female primary completion rate. A positive and significant relationship is present between child mortality and the rate of anemia in pregnancy.
Discussion
The relationship between ODA and child mortality in MDCs appear to be the most significant finding in our country-level development strata results. There is a negative and significant relationship between ODA and child mortality in MDCs only. The quadratic term is positive and also statistically significant relationship between the square of ODA and child mortality in the MDC model, indicating a tipping point at which we can calculate the maximum return on investment for aid dollars. In MDCs, we find that every additional dollar of ODA per capita is associated with a decrease in child mortality, and that the maximum return on ODA investment occurs at $203.49 per capita.
The global mean of ODA is $92.93 per capita. MDCs receive, on average, $104.40 per capita, LDCs receive $56.16, and HDCs receive $99.12 per capita. Applying the same formula to the full sample, we calculate a maximum benefit point at $181.82 per capita worldwide (with significant findings of the relationships between ODA and the squared term with child mortality rates). According to these estimates, if donor nations were to increase ODA per capita to MDC to just over $200 per capita, we might observe additional decreases in child mortality rates.
Based on these findings, if ODA per capita were increased by $99.09 per capita in MDCs, we would expect to see a commensurate decrease in child mortality of 3.5 deaths per 1000 live births in MDC. The mean birth rate in MDC in 2013 was 24.6 live births per 1000, child mortality was 39.42 deaths per 1000 live births, and the population of MDC was 4.06 billion persons. Therefore, an increase of $99.09 in ODA per capita would cost just over $402 billion, and would result in a child mortality rate of (in theory) 35.92, which translates to approximately 349,560 deaths per year, or 958 deaths per day, at a cost of $1,150,017 per life.
However, this kind of investment increase would be unprecedented, and the decrease in child mortality globally would amount to approximately 6% (or less than 2 years’ progress at current rates). The greatest investment increase seen under the UN MDGs was a promise to double aid to African nations over 5 years (a $40 billion promise). Donor nations may not have the ability to give such an amount, so such a precipitous increase in ODA per capita is likely not feasible. It is, however, important to note that these findings lend support to the hypothesis that ODA is associated with improvements in public health in medium developed countries—in this case, we find a significant decrease in child mortality. Our contribution lies in the disaggregation of countries by development level, so that we can observe the independent effect of ODA on child mortality being most significant for those countries falling in the “medium” developed category.
Many of the controls also have a significant relationship with child mortality, indicating that investments of ODA into programs that improve these factors are also investments that could indirectly contribute to the reduction of child mortality rates. Investments that increase life expectancy, access to safe water, reduce rates of childhood anemia, and increase immunization rates could each contribute to lower rates of child mortality.
Child mortality is negatively associated with pregnant anemia (as pregnant anemia increases, child mortality goes decreases), and as seen with the full sample, as access to sanitation increases, child mortality also increases. Additionally, as female enrollment in primary school rates increase, child mortality increases but child mortality does decrease as primary school completion rates increase, as reported in other studies (Sartorius 2014).
One possible explanation for the relationship with pregnant anemia is the operationalization of child mortality: child mortality is measured as the rate per 1000 live births. Anemia during pregnancy increases the risk of stillbirth (Stephansson et al. 2000). However, there is unclear evidence as to the effects of an anemic pregnancy on the infant post-natally (Allen and Linday 2002). Child anemia is positively correlated with child mortality, so if children are persistently anemic after birth, they are more likely to die prior to their fifth birthday.
Another seemingly paradoxical finding is that between female mortality and child mortality. Evidence on this relationship is inconclusive and merits further research, yet we cautiously discuss one possible explanation that has been posited in the literature here. The inverse relationship between female mortality and child mortality may be an effect of conflation with the documented effect of birth order on child mortality; younger mothers have fewer children, and therefore a higher level of investment in children of lower birth order (or, stated differently, those children that are born first). Higher child mortality is associated with higher birth order and the correlated underinvestment in subsequent children (Ballweg and Pagtolun-An 1992). However, empirical work has only hypothesized on what might be going on and a causal relationship has not yet been established. This is an important area for further inquiry.
There is no significant relationship found between ODA and child mortality rates in LDCs. This may be due to the fact that the rate of reduction in child mortality has been increasing over the past decades, while ODA per capita has actually begun to decrease. Additionally, LDCs have experienced the fastest progress of any strata over that same time period. The implication of this finding is that, while ODA may not be contributing directly to a decrease in child mortality, something is.
Child mortality is the most responsive to external factors in LDC when compared to MDC and HDC; the coefficients indicating the relationships between controls and child mortality are greatest in LDCs. For example, while a 1-year increase in life expectancy in an MDC translates to 5.26 fewer child deaths per 1000 live births, the same increase in life expectancy in an LDC yields more than twice as much benefit: a reduction of 11.5 deaths per 1000 live births.
Limitations
There are several limitations in the current study. This study looked at the effect of overall ODA per capita by recipient’s development level, but did not examine it by donor or by the ODA donation sector. This could be an important predictor (e.g., the majority of United Kingdom ODA goes to LDC and the majority of ODA from the United States goes to MDC). There may be differences in the way ODA is given by different nations that make it more or less effective, rather than recipient differences driving these findings (United Nations 2015d).
The Human Development Index (HDI) that was used as the stratification tool, was only used to stratify the observations by level. Specific HDI scores were not used to control for development level, which may have allowed the models to have greater sensitivity.
While outliers were identified, the majority of fragile or conflict-torn states are LDC; the history of every country included in the study was not examined for the past 15 years, and therefore conflict and fragility were not controlled for in separate strata. Individual country-level studies may be more useful to determine exactly where aid is effective and where it is not, rather than a global overview.
Conclusion
Across the globe there has been a precipitous drop in the child mortality rate over the past 25 years. This decrease is associated with official development aid, at least in part. The relationship between child mortality and official development aid is likely not a direct relationship, as money itself is not an intervention; it is what the money is used to do that is contributing to reductions in child mortality. Therefore, many of the same arguments found in previous studies apply; aid is a useful tool if it is used by the right hands. Good governance and adequate infrastructure are still requirements for aid to be effective.
Child mortality is a moving target, and LDC hard targets to hit. Despite representing just 11% of the global population, LDCs carry 40% of the child mortality rate, but have also contributed to 40% of the reduction in child mortality from 2000 to 2015 (The World Bank 2015). No other strata are so disproportionately burdened.
This study represents a glimpse into the effectiveness of the policy changes spurred by the MDGs. While it currently appears that ODA is ineffective in LDCs, which are surely the countries that most need effective aid implementation, the progress over the past 15 years indicates that ODA has played a significant role in reducing child mortality in Medium Developed countries. Specifically, we find that for every dollar per capita increase in ODA, there is a 0.035 decrease in child deaths per 1000 births. If progress remains consistent, many Low Developed countries could cross the tipping point of development where ODA might be more effective. These findings suggest that progress might be expedited using ODA as a policy tool.
ODA has been controversial in the literature for decades, but changes appear to slowly be transforming ODA from being part of the problem to part of the solution. The findings of this study indicate the need for more detailed research into donor and recipient behavior and how those factors influence child mortality. Doing so could further identify and enumerate sound development strategies that achieve the Sustainable Development Goals, the next United Nations initiative focusing on global improvement in health and wellbeing across the world.
References
Aidoo, Michael, Terlouw, Dianne J, Kolczak, Margarette S, McElroy, Peter D, Kuile, Feiko O ter, Kariuki, Simon, Nahlen, Bernard, Lal, Altaf A, Udhayakuma, Venkatachalam (2002) Protective effects of the sickle cell gene against malaria morbidity and mortality. Lancet 359(9314):1311–1312
Allen, Linday H. (2000) Anemia and iron Deficiency: effects on pregnancy and outcome. Am J Clin Nut 71(5):1280–1284
Ballweg JA, Pagtolun-An Imelda G (1992) Parental underinvestment: a link in the fertility-mortality continuum. Pop Res Pol Rev 11.1: 73–89.
Boone P (1996) Politics and the effectiveness of foreign aid. Eur Econ Rev 40:289–329
Dietrich S (2011) The politics of public health aid: why corrupt governments have incentives to implement aid effectively. World Dev 39(1):55–63
Dunning T (2004) Conditioning the effects of aid: cold war politics, donor credibility, and democracy in Africa. Int Org (No. 02) 58: 409–423.
Easterly W (2001) The Elusive quest for growth. MIT Press, Cambridge
Easterly W (2009) How the millennium development goals are unfair to Africa. World Devel 37(1):26–35
Filmer, Deon, Leon H. Pritchett (1999) The impact of public spending on health: does money matter? Soc Sci Med 49: 1309–1323.
Fleck, Robert K., Kilby, Christopher (2010) Changing aid regimes? U.S. foreign aid from the cold war to the war on terror. J Dev Econ 91(2):185–197
Fretts, Ruth C, Schmittdiel, Julie, McLean, Frances H, Usher, Robert H, Goldman, Marlene B (1995) Increased maternal age and the risk of fetal death. New Eng J Med 333:953–957
Goli S, Arokiasamy P (2014) Maternal and child mortality indicators across 187 countries of the world: converging and diverging. Glob Pub Health (No. 03) 9: 342–360.
Griffin K.(1991) Foreign aid after the cold war. Dev Change 22: 645–685.
Hansen H, Tarp F (2001) Aid and growth regressions. J Dev Econ 64:547–570
Knack S (2000) Aid dependence and the quality of governance: a cross-country empirical analysis. The World Bank, Washington, D.C
Knack S, Keefer P (1997) Does social capital have an economic payoff? a cross-country investigation. Quart J Econ 112(1997):1252–1288
Mahy M (2003) Childhood mortality in the developing world: a review of evidence from the demographic and health surveys. DHS Comparative Reports No. 4. ORC Macro, Calverton, Maryland
Maizels A, Nissanke MK (1984) Motivations for aid to developing countries. World Dev 12(9):879–900
Martin SP (2000) Diverging fertility among U.S. women who delay childbearing past age 30. Demography 37(4):523–533
Moalem S, Prince J (2007) Survival of the sickest: the surprising connections between disease and longevity. Harper Perennial, New York
Moyo D (2009) Dead aid: why aid is not working and how there is a better way for Africa. Farrar, Strauss and Giroux, New York.
Mujica O, Vasquez E, Duarte EC, Cortez-Escalante JJ, Molina J, Silva JB Jr (2014) Socioeconomic inequalities and mortality trends in BRICS, 1990–2010. Bull World Health Organ 92(405):405–412
OECD (2008) The Paris declaration on aid effectiveness and the accra agenda for action. http://www.oecd.org. http://www.oecd.org/dac/effectiveness/34428351.pdf. Accessed 16 Nov 2015.
OECD (2015) Official development assistance: definition and coverage. http://www.oecd.org/dac/stats/officialdevelopmentassistancedefinitionandcoverage.htm. Accessed 20 Nov 2015.
Ovaska T (2003) The failure of development aid. Cato J 23(2):175–188
Millennium Promise (2009) Millennium development timeline. http://mp.convio.net/site/DocServer/MP_Timeline.pdf?docID=1502. Accessed 15 Nov 2015.
Rindfuss RR, Morgan SP, Offutt K (1996) Educating and the changing age pattern of american fertility: 1963–1989. Demography 33(3):277–290
Sartorius BK (2014) Global infant mortality trends and attributable determinants: an ecological study using data from 192 countries for the period 1990–2011. Pop Health Metrics 12:29
Sen A (1999) Development as freedom. Anchor Books, New York
Smith GCS, Pell JP (2001) Teenage pregnancy and risk of adverse perinatal outcomes associated with first and second births: population based retrospective cohort study. Brit Med J 323:476
Stephansson O, Dickman PW, Johansson A, Cnattingius S (2000) Maternal hemoglobin concentration during pregnancy and risk of stillbirth. J Am Med Assoc 284(20):2611–2617
Tacke T, Waldmann RJ (2013) Infant mortality, relative income and public policy. Appl Econ 45:3240–3254.
The World Bank (2015) World development indicators. http://data.worldbank.org/data-catalog/world-development-indicators. Accessed 15 Sep 2015.
Trumbull WN, Wall HJ (1994) Estimating aid-allocation criteria with panel data. Econ J 104(425):876–882
UNDP (2011) Towards human resilience: sustaining MDG progress in and age of economic uncertainty. Bureau for development policy, United Nations development programme. UNDP, New York.
United Nations (2014) Human development report. http://hdr.undp.org/en/content/human-development-index-hdi. Accessed 15 Sep 2015
United Nations (2015a) Goal 3: ensure healthy lives and promote well-being for all at all ages. http://www.un.org/sustainabledevelopment/sustainable-development-goals. Accessed 16 Nov 2015
United Nations (2015b) News on millennium development goals 2015. http://www.un.org/millenniumgoals. Accessed 17 Nov 2015
United Nations (2015c) Sustainable development goals 2015. https://sustainabledevelopment.un.org. Accessed 17 Nov 2015
United Nations (2015d) The millennium development goals report. United Nations. July 2015. http://www.un.org/millenniumgoals/news.shtml. Accessed 10 Nov 2015
WHO (2002) Report of the commission on macroeconomics and health. Regional office for South-East Asia, World Health Organization, Jakarta
Williamson CR (2008) Foreign aid and human development: the impact of foreign aid to the health sector. South Econ J 75(1):188–207
Zanger SC (2000) Good governance and European Aid: the impact of political conditionality. Eur Un Pol 1(3):293–317
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
This study was not funded by any grant.
Ethical approval
This article does not contain any studies with human participants or animals performed by any of the authors.
Additional information
This article is part of the special issue “Development and Public Health”.
Rights and permissions
About this article

Cite this article
Winkleman, T.F., Adams, G.B. An empirical assessment of the relationship between Official Development Aid and child mortality, 2000–2015. Int J Public Health 62, 231–240 (2017). https://doi.org/10.1007/s00038-017-0940-2
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00038-017-0940-2