
Abstract
Tumor necrosis factor-related apoptosis-inducing ligand is a potential therapeutic anti-cancer drug with selective cytotoxicity in cancer cells. However, in multiple clinical trials, the therapeutic effect of TRAIL is limited owing to tumor resistance. The combination of small molecules or other drugs may represent a suitable strategy to overcome TRAIL resistance. This study found that 20(s)-ginsenoside Rh2 sensitized non-sensitive human hepatocellular carcinoma cells to TRAIL-induced apoptosis. The combination of TRAIL and Rh2 decreased cell viability and increased caspase cascade-induced apoptosis in several liver cancer cell lines. Moreover, we found that Rh2 reduced the apoptosis-related protein XIAP and Survivin, a negative regulator of the apoptosis pathway. At the same time, Rh2 can further enhance TRAIL-induced apoptosis by upregulating the death receptor 5, thereby significantly enhancing its anti-tumor effect. Furthermore, Rh2 enhanced the therapeutic efficacy of TRAIL in mouse xenograft models, suggesting that Rh2 also sensitizes TRAIL in vivo. Taken together, our study indicates that Rh2 may act as a sensitizer in combination with TRAIL to increase the efficacy of its anti-tumor activity.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Hepatocellular carcinoma (HCC) is the seventh most common cancer presenting with solid tumors and the fourth leading cause of cancer-related deaths worldwide [1]. At present, classical chemotherapy is still the main treatment for HCC. Procedures such as surgical resection, ablation, transarterial chemoembolization, and stereotactic body radiation therapy for HCC are current therapeutic strategies [2]. A multidisciplinary approach is associated with improved survival of hepatocellular carcinoma patients, but selecting an appropriate therapeutic strategy is also important for patients [3].
TRAIL, a tumor necrosis factor-related apoptosis-inducing ligand, is an attractive agent for cancer therapy because it induces apoptosis in cancer cells but not in normal cells [4,5,6]. TRAIL interacts with TRAIL-R1/death receptor 4 (DR4) and TRAIL-R2/death receptor 5 (DR5) expressed by tumor cells, thereby inducing the apoptotic pathways in cells [7]. There are two principal signaling pathways involved in apoptosis: the extrinsic and intrinsic pathways. The extrinsic pathway is activated when TRAIL binds to death receptors, such as DR4 and DR5, and triggers the caspase cascade. The binding of TRAIL to DR4 and DR5 results in the death-inducing signaling complex (DISC) assembly, which incorporates the adaptor protein Fas-associated death domain (FADD). Through FADD, activation of pro-caspases 8 and 10 leads to the release of active caspase molecules, which activate the effector caspase-3 [8,9,10]. The intrinsic pathway includes the interplay between members of the Bcl-2 family, leading to the activation of caspase-9 and the effector caspase from mitochondria to the cytoplasm [11,12,13]. However, not all malignancies are sensitive and responsive to TRAIL. For TRAIL-insensitive tumor cells, a broader approach is to combine other drugs for treatment [14, 15]. Importantly, such combinations increase the sensitivity to TRAIL, which makes TRAIL play a critical role in cancer therapy.
Ginsenoside Rh2, a purified ginseng saponin, exhibits anti-tumor effects in various cancer cell types, such as human breast cancer MCF-7 cells [16], human AML THP-1 cells [17], and SK-Hep-1 human hepatoma cells [18]. However, the molecular mechanism of Rh2 anti-tumor activity has not been explained fully, and it is mainly related to tumor cell proliferation or apoptosis [19]. For example, Rh2 effectively inhibited IL-6-induced signal transducer and activator of transcription 3 (STAT3) phosphorylation and the expression of matrix metalloproteinases (MMPs), resulting in the inhibition of human colorectal cancer cell invasion [20]. In HepG2 cells, Rh2 could suppress proliferation, promote apoptosis, and inhibit metastasis by downregulating β-catenin through activating GSK-3β [21]. In addition, Rh2 was used in combination with other drugs for synergistic treatment. Rh2 and sodium selenite combination have a synergistic effect on HCT116 human colorectal carcinoma cells [22]. In a previous study, the ginsenoside metabolite Rg3 was combined with TRAIL in treating hepatocellular carcinoma, thus, providing a basis for combining TRAIL and Rh2 [23].
This study found that the combination of TRAIL and Rh2 produced significant anti-tumor effects both in vitro and in vivo. Some cancer cells, including HCC cells, are resistant to TRAIL. However, Rh2-induced TRAIL was more sensitive to the HepG2 cells. Then, we demonstrated that the combined mechanism of TRAIL and Rh2 is to upregulate tumor cells DR5 expression and decrease expression of the apoptosis inhibitory proteins XIAP and Survivin, thereby causing a stronger apoptotic activity of TRAIL, and also verified this hypothesis in vivo. This study will improve the efficiency of treating TRAIL-insensitive cell lines and avoid high-dose drug toxicity while achieving better therapeutic outcomes.
Materials and methods
Materials
Ginsenoside Rh2 (≥ 98% purity, #MB6871) was purchased from Dalian Meilun Biotechnology Co., Ltd. (Dalian, China). Dulbecco's modified Eagle's medium (DMEM), RPMI 1640, fetal bovine serum (FBS), penicillin, streptomycin, and trypsin were purchased from Gibco (Gaithersburg, MD, USA). Antibodies against caspase-3 (#9662), cleaved caspase-3 (#9661), and Survivin (#2808) were obtained from Cell Signaling Technology (Danvers, MA, USA). Caspase-8 (#551244), XIAP (#610716), and Bcl-2 (#610538) were purchased from BD Biosciences (San Jose, CA, USA). Antibodies against DR4 (#ab216662) and DR5 (#ab199357) were purchased from Abcam (Cambridge, UK). PARP (#11040-MM04) was purchased from Sino Biological (Beijing, China). Tubulin (#abs137976) and β-actin (#abs132001) were purchased from Absin (Shanghai, China). The pan-caspase inhibitor zVAD (#HY-16658B) was purchased from MedChem Express (NJ, US).
Cell viability assay
Human hepatocellular carcinoma cells HepG2, SMMC-7701, LM-3, and human liver cells HL7702 were purchased from the American Type Culture Collection (ATCC, Manassas, VA, USA), and the identity of the line was re-confirmed after expansion and passaging. Cells were cultured with 10% FBS in DMEM or RPMI 1640 plus 100U/mL penicillin and 100 mg/mL streptomycin at 37 °C in a humidified 5% CO2 atmosphere. Experimental cells (1 × 104/100 μL) were grown in a 96-well plate, incubated for 24 h and then treated with TRAIL and Rh2 at the indicated concentrations. Cell viability was assessed using the MTT assay, according to previously described procedures.
Annexin V-FITC/PI flow cytometry assay
Cells were seeded at a concentration of 2 × 105 cells/well in a 6-well plate and incubated with TRAIL and Rh2 for 24 h. Importantly, Rh2 was pretreated for 30 min followed by TRAIL in the combination group. Apoptotic cells were detected using an Annexin V-FITC/PI Apoptosis Detection Kit (#KGA1014, KeyGEN BioTECH, Jiangsu, China). Following digestion, the cells were washed twice in ice-cold phosphate-buffered saline (PBS) by centrifugation at 300 × g for 5 min and resuspended in 500 μL binding buffer. Cells were then stained with 5 μL Annexin V-FITC and 5 μL propidium iodide (PI) for 15 min in the dark at room temperature and analyzed by two-color flow cytometry (Becton Dickinson, Franklin Lakes, NJ, USA). Annexin V-FITC fluorescence was detected in FL-1, and PI was detected in FL-3.
Western blotting
The harvested cells were mixed with radio immunoprecipitation assay (RIPA) buffer (#P0013, Beyotime, Jiangsu, China) for 10 min. The proteins were separated by SDS-PAGE and transferred onto a nitrocellulose membrane (Millipore, Billerica, MA, USA) after electrophoresis. Then, the membranes were incubated for 1 h at room temperature in blocking buffer, followed by overnight incubation at 4 °C with primary antibodies overnight. The next day, the membranes were washed with PBS containing 0.2% Tween20 (PBST) and incubated with secondary antibodies for 1 h. After washing three times with PBST, the signal was detected using an automatic chemiluminescence image analysis system (Tanon, Shanghai, China).
Caspase-3, -8, and -9 activity analysis
Caspase activity was measured using a caspase activity kit (#C1115, #C1152, #C1157, Beyotime, Jiangsu, China) according to the manufacturer's instructions. The detailed method was described previously. Briefly, cells were incubated with TRAIL and Rh2 for 4 h, 8 h, 16 h, and 24 h, respectively. Rh2 was pretreated for 30 min, followed by TRAIL in the combination group. The cells were resuspended in lysis buffer and incubated on ice for 15 min. The lysate was centrifuged at 12,000 rpm at 4 °C for 15 min. Activities of caspase-3, -8, and -9 were measured using the substrate peptides Ac-DEVD-pNA, Ac-IETD-pNA, and Ac-LEHD-pNA, respectively. The release of pNA was determined by measuring the absorbance at a wavelength of 405 nm.
Human apoptosis protein array
We used an apoptosis array (#ARY009) purchased from R&D Systems (Minneapolis, MN, USA) to detect different apoptotic proteins according to the manufacturer's instructions. Briefly, HepG2 cells were treated with 25 μM Rh2 for 24 h. Cells were collected, washed, and then were lysed by lysis buffer, and total proteins were extracted. Protein concentrations were approximately 200 μg of lysate, and each array antibody membrane was blocked and then incubated with protein overnight at 4 °C. The membrane incubated with HRP linked Streptavidin conjugated for 1 h at room temperature. Apoptotic proteins were visualized using enhanced chemiluminescence (ECL).
Reverse transcription PCR
HepG2 cells were treated with TRAIL (50 ng/mL), Rh2 (25 μM), and Rh2 pretreated for 30 min, followed by TRAIL in the combination group. The TransZol Up Plus RNA Kit (#ER501-01, Transgen, Beijing, China) was used to extract total RNA from treated cells according to the manufacturer's instructions. cDNA was obtained using the PrimeScript RT Reagent Kit with gDNA Eraser (#RR047A, Takara, Otsu, Japan). Using cDNA as the template, a quantitative real-time PCR assay was performed with TB Green Premix Ex Taq (#RR820Q, Takara) and a CFX96 real-time PCR system (Bio-Rad, CA, USA). β-actin was used as the reference gene.
PCR amplification was conducted using the following primers: DR4: Forward 5′-CAGAACGTCCTGGAGCCTGTAAC-3′ Reverse 5′-ATGTCCATTGCCTGATTCTTTGTG-3′; DR5: Forward 5′ -TGCAGCCGTAGTCTTGATTG-3′ Reverse 5′-GCACCAAGTCTGCAAAGTCA-3′; Bcl-2: Forward 5′-GGAGAGCGTCAACAGGGAGA-3′ Reverse 5′-CAGCCAGGAGAAATCAAACAGAG; XIAP: Forward 5′-ACTTCGGGTTTCACGACTCC-3′ Reverse 5′-TACACAAGCTGTACCCACCG-3′; β-actin: Forward 5′- CAGGTCATCACCATTGGCAATGAGC-3′ Reverse 5′-GATGTCCACGTCACACTTCATGA-3′.
Flow cytometry analysis
For the HepG2 cells stained for DR4 and DR5, the cells were suspended in PBS after Rh2 treatment for 12 h. Cells were then incubated with PE anti-human CD261 (#307206, DR4, TRAIL-R1) antibody (BioLegend, CA, USA) and APC anti-human CD262 (#307408, DR5, TRAIL-R2) antibody (BioLegend, CA, USA) for 20 min in the dark. Subsequently, the cells were washed with PBS and analyzed using flow cytometry (Becton Dickinson, Franklin Lakes, NJ, USA).
Tumor tissues were collected in RPMI 1640 and cut into several pieces. The cells were then ground into individual cells in a plate after 1 h of collagenase treatment at 37 °C. The cells were centrifuged at 300 × g for 5 min, washed with PBS, and resuspended in staining buffer. Mouse intratumoral cells were stained with the following antibodies: FITC anti-human CD45 (#982316), PE anti-human CD261 (DR4, TRAIL-R1), APC anti-human CD262 (DR5, TRAIL-R2), and isotype control FITC Mouse IgG1 (#406605, BioLegend, CA, USA) for 20 min in the dark. The stained cells were analyzed using flow cytometry.
Xenograft mouse models
Female BALB/c nu/nu mice (5 weeks old) were obtained from Vital River Laboratories (VRL, Beijing, China). Human hepatocellular carcinoma cells HepG2 (5 × 105) in the log phase were implanted subcutaneously (s.c.) in the flanks of mice. The mice were randomized into four groups (PBS, TRAIL, Rh2, and TRAIL + Rh2, n = 10/group). When the tumor reached a volume of approximately 100–150 mm3, mice were intraperitoneally administered a dose of 1 mg/kg Rh2, 1 nM TRAIL, or PBS (100 μL) for eight consecutive days. Tumor growth was monitored daily for 20 days, and the tumor volume (mm3) was calculated as (length × width2)/2. When the total tumor volume reached 1500 mm3, the animals were euthanized. At the end of treatment, three mice from each group were sacrificed randomly. The liver, kidney, and tumor tissues were fixed with 4% paraformaldehyde, and paraffin sections were obtained for H&E staining and immunohistochemistry.
Statistical analysis
Values are expressed as the mean ± SEM. Statistical analysis was performed using a one-way analysis of variance or an unpaired t-test followed by the Newman-Keuls test. Statistical significance was set at P < 0.05. Statistical analysis was performed using GraphPad Prism 8. All experiments were repeated at least three times.
Results
Rh2 sensitizes human hepatocellular carcinoma cells to TRAIL-induced cell death
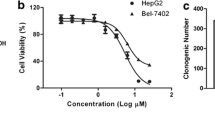
TRAIL may have produced anti-tumor effects in various tumor cells in earlier studies by inducing apoptosis. The cytotoxic activity of TRAIL and Rh2 in human hepatocellular carcinoma cells was assessed using the MTT assay. The results showed that a concentration of 200 ng/mL of TRAIL alone was required for cytotoxicity. When the TRAIL concentration was 200 ng/mL, the cell viability of SMMC-7701 was 42.8%, but that of HepG2 and LM-3 cells was approximately 80% (Fig. 1a). Rh2 concentrations greater than 25 μM were required for substantial cytotoxicity in all three cell lines (Fig. 1b). However, when cells were pretreated with Rh2 for 30 min followed by low concentrations of TRAIL (25 ng/mL) for 16 h, the SMMC-7701, and LM-3 cells were underwent cell death as evidenced by MTT assay (Fig. 1c). With the same treatment, the cell viability in the combination of TRAIL and 50 μM Rh2 was 11%, which was remarkably suppressed compared with cells treated with Rh2 and TRAIL alone (Fig. 1d). The inhibitory effect of the combination group was significantly higher than that of the individual group. Moreover, the combined group cells showed changes in cell morphology, and cell shrinkage and death occurred (Fig. 1e). However, human normal liver cells (HL7702) were insensitive to TRAIL and Rh2, indicating that sensitization may be limited to cancer cells (Fig. 1f).

Combined TRAIL and Rh2 treatment in HepG2. a and b HepG2 cells treated as indicated with TRAIL (a) or Rh2 (b) for 16 h and viability analyzed using the MTT assay. c and d SMMC-7701 and LM-3 (c) and HepG2 cells (d) pretreated with Rh2 30 min followed by treatment with TRAIL (25 ng/mL) for 16 h, and viability analyzed by the MTT assay. e Representative phase-contrast microscopic images. HepG2 cells treated with Rh2 (25 μM), TRAIL (25 ng/mL), or Rh2 plus TRAIL for 16 h. The scale bar = 100 μm. f. Human normal liver cells (HL7702) treated with Rh2 (25 μM), TRAIL (25 ng/mL), or Rh2 plus TRAIL for 16 h, and cell viability analyzed by the MTT assay. All results shown are averages ± SEM (*P < 0.05; **P < 0.01; ***P < 0.001)
Rh2 promotes TRAIL-induced caspase-dependent apoptotic cell death
To evaluate the effect of TRAIL and Rh2 on apoptosis in HepG2 cells, we performed an experiment to detect the apoptotic pathway. We found that TRAIL and Rh2 themselves have the ability to induce apoptosis over time, even if very limited. However, the combination of TRAIL and Rh2 can significantly increase the apoptosis of HepG2 cells, and at the same time, it is enhanced with the prolongation of the effect time (Fig. 2a). At 12 h, the combination group could significantly induce the apoptosis of HepG2 cells compared with the TRAIL alone. At 24 h, the total number of apoptotic cells in the combined group was significantly higher than that in the TRAIL and Rh2 alone groups (Fig. 2b). TRAIL-induced apoptosis is executed by the extrinsic cell death pathway, with caspase-3 as the executioner caspase. Rh2 alone did not affect caspase-3 cleavage in HepG2 cells, but Rh2 pretreatment significantly augmented TRAIL-induced cleavage of caspase-3 and PARP cleavage. Meanwhile, caspase-8 was also activated in the combined TRAIL and Rh2 treatment group (Fig. 2c and d). Moreover, to validate that cell death was via the apoptotic pathway, we used a pan-caspase inhibitor zVAD to inhibit caspase signaling. The results showed that the activities of caspase-3, PARP, and caspase-8 were inhibited by zVAD inhibition, indicating that the combined effect of TRAIL and Rh2 is indeed through the caspase pathway (Fig. 2e and f). To further illustrate the effect of the caspase pathway, we detected caspase-8, -9, and -3 enzyme activity at different time points. The results showed that caspase-8 and -3 enzyme activity peaked at 24 h after combined TRAIL and Rh2 treatment, and caspase activity was significantly stronger than Rh2 alone (Fig. 2g). However, TRAIL or Rh2 alone or in combination had no significant effect on caspase-9 activity. The results indicated that the synergistic effect of TRAIL and Rh2 on apoptosis may be mediated through a caspase-dependent pathway.

Rh2 enhances the caspase activity induced by TRAIL. a HepG2 cells were pretreated with Rh2 (12.5 μM) for 30 min followed by treatment with TRAIL (25 ng/mL) for 4 h, 8 h, 12 h, 16 h, and 24 h, and cell apoptosis was analyzed by FACS using Annexin V-FITC/PI staining. b The quantification of apoptosis in HepG2 cells subjected to different treatments as indicated. c Western blot analysis of caspase-3, PARP, cleaved PARP, and caspase-8 after treatment 24 h. d The related density of caspase-3 and caspase-8 expression. e 25 ng/mL TRAIL, 25 μM Rh2, and 50 μM zVAD were treated HepG2 cells for 24 h, Western blot analysis of caspase-3, PARP, and caspase-8. f The related density of caspase-3 and caspase-8 expression after zVAD treatment. g The activity of caspase-8, caspase-9, and caspase-3 was examined using the colorimetric caspase assay kit in 25 ng/mL TRAIL and 25 μM Rh2
Rh2 downregulates inhibitor of apoptosis proteins
Based on the above results, Rh2 alone can also induce apoptosis in liver cancer cells. To confirm the mechanism of Rh2 apoptosis, we used a human apoptosis protein array as shown in Fig. 3a and b, which demonstrated the upregulation of Bad, cleaved caspase-3, DR5, Fas, and SMAC/Diablo. Moreover, the detection of apoptosis proteins revealed that Survivin expression was suppressed. We detected the mRNA expression of HepG2 cells incubated by 25 μM Rh2 at 0 h, 4 h, 16 h and 24 h. The results showed that the mRNA expressions of bcl-2 and XIAP were significantly reduced when Rh2 was treated for 24 h (Fig. 3c). Next, we analyzed the expression of apoptosis inhibition-associated proteins using immunoblotting to confirm the effect of Rh2 on the apoptotic pathway. As shown in Fig. 3d, Rh2 decreased XIAP and Bcl-2 protein levels, indicating that Rh2 promotes apoptosis by downregulating apoptosis-inhibiting proteins such as XIAP. In addition, when TRAIL and Rh2 were combined, the protein expression of XIAP and Survivin decreased as the Rh2 concentration increased and the combination of TRAIL and Rh2 did not affect the down-regulation (Fig. 3e). Taken together, our results demonstrate that Rh2 can induce apoptosis of liver cancer cells by downregulating the expression of XIAP and Survivin, and TRAIL does not affect this process.

Rh2 downregulates the inhibitor of apoptosis proteins expression. a HepG2 cells were treated with 25 μM Rh2 for 24 h. Human apoptosis protein array was utilized to analyze the effect of Rh2 on expression of apoptosis-related proteins in HepG2 cells. Images of the nitrocellulose proteome profiler membrane show differences in apoptotic protein expression in the control and treated samples. b Relative normalized optional density of apoptosis-related proteins. c The mRNA expression of Bcl-2 and XIAP after 25 μM Rh2 treatment for 0 h, 4 h, 16 h, and 24 h. d Western blotting of lysates from HepG2 cells treated with Rh2 (25 μM) for indicated times. e Western blot analysis of HepG2 cells pretreated with Rh2 (12.5 and 25 μM) for 30 min followed by treatment with TRAIL (50 ng/mL) for 12 h
Rh2 sensitizes TRAIL-induced apoptosis via DR5 upregulation
DR4 and DR5 expression directly affect the TRAIL-induced apoptosis pathway. Quantitative real-time PCR was used to measure DR4 and DR5 mRNA expression (Fig. 4a). After Rh2 treatment, increased DR5 mRNA levels were observed, and DR4 mRNA levels remained unchanged. The mRNA expression of DR5 was significantly higher than that of the control group after Rh2 treatment for 4 h, and the mRNA expression of DR5 also increased with the increase of time. Consistent with the mRNA changes, Rh2 markedly induced the expression of DR5 from 2 h onwards, whereas DR4 expression did not change significantly (Fig. 4b). Furthermore, we examined the expression of DR4 and DR5 after Rh2 treatment in HepG2 cells using flow cytometry analysis, as shown in Fig. 4c. The flow cytometry results also showed that DR5 was significantly upregulated compared with the control, but DR4 expression was unchanged. The relative mean optical density of DR5 in the Rh2-treated group increased significantly (Fig. 4d), indicating that Rh2 may promote TRAIL-induced apoptosis of liver cancer cells by upregulating DR5.

Rh2 upregulates the expression of DR5. a HepG2 cells were pretreated with Rh2 (25 μM) for 4 h, 12 h, and 16 h, and the mRNA expression of DR4 and DR5 was analyzed by qRT-PCR. b Western blotting of lysates from HepG2 cells treated with Rh2 (25 μM) for the indicated times. c HepG2 cells were pretreated with Rh2 for 12 h and analyzed by FASC. d The relative MFI of DR4 and DR5
Combination treatment with Rh2 and TRAIL potentiates in vivo anti-hepatocellular carcinoma activity
The anti-tumor effects of Rh2 and TRAIL against HCC were further investigated in xenograft mice. HepG2 cells were inoculated into the flanks of nude mice, and when tumors were measurable, mice were matched for tumor volumes and assigned to TRAIL, Rh2, or a combination of TRAIL and Rh2. Tumor volumes in the TRAIL, Rh2, and Rh2-TRAIL combination groups were approximately 98%, 86%, and 36%, respectively, compared with the control group (Fig. 5a). It is worth noting that the combination of Rh2 and TRAIL inhibited tumor growth compared with the control group and inhibited tumor growth compared to Rh2 or TRAIL alone. To further explore whether the tumor-suppressive effect in vivo is due to DR5 upregulation in tumor cells by Rh2, we evaluated the intratumoral expression of DR5. The upregulation of DR5 in mice treated with Rh2 or the combination of TRAIL and Rh2 (Fig. 5b) suggests that Rh2 upregulates DR5, which causes TRAIL to induce tumor cell apoptosis and inhibit tumor growth. Next, we investigated the effect of the treatments on in vivo apoptosis by examining cleaved caspase-3 immunohistochemistry staining and H&E staining of xenografted tumors. Caspase-3 cleavage was more pronounced in tumor sections from mice treated with TRAIL plus Rh2 than in tumors from mice treated with either TRAIL or Rh2 alone (Fig. 5c). Quantitation of cleaved caspase-3 staining in tumor sections indicated a significant increase in cell death in the tumors of the mice on combination treatment compared with either treatment alone (Fig. 5d). Importantly, no significant changes were observed during therapy in the livers and kidneys of mice of any treatment group (Fig. 5e), indicating that TRAIL or Rh2 is generally well tolerated in vivo.

The combination of Rh2 with TRAIL inhibits HepG2 growth in mouse xenografts. a HepG2 tumors established subcutaneously in athymic BalB/c nude mice were treated with Rh2 (1 mg/kg), TRAIL (1 nM), or the combination for 20 days. Tumor growth was monitored. Results shown are averages ± SEM (*P < 0.05; **P < 0.01; ***P < 0.001). b The expression of DR5 in tumor tissue was detected by flow cytometry. c In situ detection of cell death in xenografted HCC tumors from A was carried out by using cleaved caspase-3 staining. Scale bar = 200 μm. The scale bar of enlarged images was 50 μm. d The quantification of cleaved caspase-3 positive cells in tissue sections. e H&E staining of the liver and kidney. Scale bar = 50 μm
Discussion
As a novel and promising anti-cancer drug, TRAIL is becoming a very useful strategy for treating cancer [24]. However, TRAIL-based therapy still needs to overcome some obstacles due to acquired or intrinsic drug resistance. In this study, we suggest that Rh2 could act as a sensitizer to TRAIL in HepG2 cells. We found that Rh2-mediated DR5, Bcl-2, XIAP, and Survivin regulation in TRAIL sensitization. Rh2 increased DR5 expression at the mRNA level and downregulated XIAP and Survivin expression. Furthermore, we verified that Rh2 upregulates the expression of DR5 and that combination therapy has a stronger anti-tumor effect than Rh2 alone in mouse xenograft models (Scheme 1).

Schematic diagram of the combined treatment mechanism of TRAIL and Rh2 in HepG2 cells
We show that Rh2 can enhance TRAIL-induced tumor apoptosis in insensitive HepG2 cells by upregulating DR5 expression. Although most cancer cells express DR4 and DR5, the expression level of receptors plays a critical role in determining cell fate in response to TRAIL. Numerous studies have shown convincing evidence that DR5 upregulation can enhance the sensitivity of TRAIL-induced apoptosis [25, 26]. The apoptotic activity of TRAIL is regulated by controlling the expression of DR5. Previous studies have demonstrated that telmisartan can sensitize TRAIL and enhance NSCLC tumor cell death [27]. The molecular mechanism includes the generation of ROS, leading to DR5 upregulation. Wu et al. reported enhanced sensitivity to TRAIL therapy following luteolin treatment in NSCLC cells, which may be associated with increased DR5 expression and upregulation of Drp1-mediated mitochondrial fission [28]. We found that Rh2 directly increased DR5 mRNA and protein expression and caused subsequent activation of the caspase cascade following TRAIL treatment. The combination of TRAIL and Rh2 mainly activated the caspase-3 and caspase-8 pathways. Yesi et al. showed that NanoTRAIL generated ROS-triggered JNK activation and induced subsequent autophagy-assisted DR5 upregulation, resulting in a significantly enhanced anti-tumor efficacy of TRAIL [29]. Therefore, regardless of which compound is combined with TRAIL, it is likely that DR5 plays a major role in the downstream signaling pathway. Meanwhile, we further evaluated the expression of DR5 in the tumor microenvironment in mouse xenograft models. The expression of DR5 in tumor cells was upregulated due to the effect of Rh2, indicating that the regulatory effect of Rh2 in vivo is consistent with the in vitro results. We definitively demonstrated that Rh2 acts as an activator to upregulate DR5 to sensitize tumor cells to TRAIL. However, the molecular mechanism of Rh2 leading to the upregulation of DR5 expression requires further study.
Although upregulating DR5 expression is the key to activating TRAIL activity, regulating downstream signals can maximize TRAIL function. The anti-tumor mechanism underlying the effects of Rh2 is not fully understood, but there are similar mechanisms in different tumor cells. Previously, Wang et al. reported that GRh2 significantly decreased the anti-apoptotic protein Bcl-2 in leukemia cells [30]. We also confirmed that Rh2 treatment reduced the protein expression of Bcl-2 in HepG2 cells, increased the expression of pro-apoptotic proteins Bad and Bax, and reduced levels of XIAP and Survivin. Raedeh et al. showed that XIAP might also play a role in inducing resistance to TRAIL-induced cell death in leukemia [31]. Indeed, XIAP, as a key central component, functions in the crosstalk between the intrinsic and extrinsic pathways. The combination of XIAP inhibitors and TRAIL receptor agonists sensitized TRAIL-resistant cells to hematological neoplasms. Consequently, inhibiting XIAP expression may make tumor cells more sensitive to TRAIL through the combination of Rh2.
Collectively, we showed that Rh2 sensitized HepG2 cells to TRAIL-induced apoptosis through DR5 upregulation both in vivo and in vitro and simultaneously regulated apoptosis-related proteins. Our study indicates that the combination of Rh2 and TRAIL can be used as a promising treatment strategy for liver cancer.
References
Yang JD, Heimbach JK. New advances in the diagnosis and management of hepatocellular carcinoma. BMJ. 2020. https://doi.org/10.1136/bmj.m3544.
Couri T, Pillai A. Goals and targets for personalized therapy for HCC. Hep Intl. 2019;13(2):125–37.
Debes J, et al. Serum biomarkers for the prediction of hepatocellular carcinoma. Cancers. 2021;13(7):1681.
Wiley SR, Schooley K, Smolak PJ, Din WS, Huang CP, Nicholl JK, et al. Identification and characterization of a new member of the TNF family that induces apoptosis. Immunity. 1995;3:673–82.
Walczak H, Miller RE, Ariail K, Gliniak B, Griffith TS, Kubin M, et al. Tumoricidal activity of tumor necrosis factor-related apoptosis-inducing ligand in vivo. Nat Med. 1995;5:157–63.
Ashkenazi A, Pai SF, Fong S, Leung S, Lawrence DA, Marsters SA, et al. Safety and antitumor activity of recombinant soluble Apo2 ligand. J Clin Invest. 1999;104:155–62.
Wong SHM, et al. The TRAIL to cancer therapy: Hindrances and potential solutions. Crit Rev Oncol Hematol. 2019;143:81–94.
de Miguel D, et al. Onto better TRAILs for cancer treatment. Cell Death Differ. 2016;23(5):733–47.
Stuckey DW, Shah K. TRAIL on trial: preclinical advances in cancer therapy. Trends Mol Med. 2013;19(11):685–94.
O’Leary L, et al. Decoy receptors block TRAIL sensitivity at a supracellular level: the role of stromal cells in controlling tumour TRAIL sensitivity. Oncogene. 2015;35(10):1261–70.
Zhang L, Fang B. Mechanisms of resistance to TRAIL-induced apoptosis in cancer. Cancer Gene Ther. 2004;12(3):228–37.
Fulda S, Debatin KM. Extrinsic versus intrinsic apoptosis pathways in anticancer chemotherapy. Oncogene. 2006;25(34):4798–811.
Czabotar PE, et al. Control of apoptosis by the BCL-2 protein family: implications for physiology and therapy. Nat Rev Mol Cell Biol. 2013;15(1):49–63.
Han L, et al. Combination of the natural compound Periplocin and TRAIL induce esophageal squamous cell carcinoma apoptosis in vitro and in vivo: Implication in anticancer therapy. J Expt Clin Cancer Res. 2019. https://doi.org/10.1186/s13046-019-1498-z.
Jo EB, et al. Combination therapy with c-met inhibitor and TRAIL enhances apoptosis in dedifferentiated liposarcoma patient-derived cells. BMC Cancer. 2019. https://doi.org/10.1186/s12885-019-5713-2.
Lee H, et al. Ginsenoside Rh2 epigenetically regulates cell-mediated immune pathway to inhibit proliferation of MCF-7 breast cancer cells. J Ginseng Res. 2018;42(4):455–62.
Wang Z, et al. Enhancing the antitumor activity of an engineered TRAIL-coated oncolytic adenovirus for treating acute myeloid leukemia. Sig Transduct Targeted Ther. 2020. https://doi.org/10.1038/s41392-020-0135-9.
Oh J, et al. Caspase-3-dependent protein kinase C delta activity is required for the progression of Ginsenoside-Rh2-induced apoptosis in SK-HEP-1 cells. Cancer Lett. 2005;230(2):228–38.
Nag SA. Ginsenosides as anticancer agents: In vitro and in vivo activities, structure–activity relationships, and molecular mechanisms of action. Front Pharmacol. 2012. https://doi.org/10.3389/fphar.2012.00025.
Songhee H, et al. Ginsenoside 20(S)-Rh2 exerts anti-cancer activity through targeting IL-6-induced JAK2/STAT3 pathway in human colorectal cancer cells. J Ethnopharmacol. 2016;194:83–90.
Shi Q, et al. Anticancer effect of 20(S)-ginsenoside Rh2 on HepG2 liver carcinoma cells: activating GSK-3β and degrading β-catenin. Oncol Rep. 2016;36(4):2059–70.
Zhu C, Qian W, Zhang T, Li F. Combined Effect of Sodium Selenite and Ginsenoside Rh2 on HCT116 Human Colorectal Carcinoma Cells. Arch Iran Med. 2016;19(1):23–9.
Lee J-Y, et al. Sensitization of TRAIL-Induced Cell Death by 20(S)-Ginsenoside Rg3 via CHOP-Mediated DR5 Upregulation in Human Hepatocellular Carcinoma Cells. Mol Cancer Ther. 2013;12(3):274–85.
Kelley S. Targeting death receptors in cancer with Apo2L/TRAIL. Curr Opin Pharmacol. 2004;4(4):333–9.
Jeon M-Y, et al. Dexamethasone Inhibits TRAIL-Induced Apoptosis through c-FLIP(L) Upregulation and DR5 Downregulation by GSK3β Activation in Cancer Cells. Cancers. 2020;12(10):2901.
Woo SM, Min K-J, Kwon TK. Magnolol Enhances the Therapeutic Effects of TRAIL through DR5 Upregulation and Downregulation of c-FLIP and Mcl-1 Proteins in Cancer Cells. Molecules. 2020;25(19):4591.
Rasheduzzaman M, et al. Telmisartan generates ROS-dependent upregulation of death receptor 5 to sensitize TRAIL in lung cancer via inhibition of autophagy flux. Int J Biochem Cell Biol. 2018;102:20–30.
Wu B, et al. Luteolin enhances TRAIL sensitivity in non-small cell lung cancer cells through increasing DR5 expression and Drp1-mediated mitochondrial fission. Arch Biochem Biophys. 2020;692:108539.
Shi Y, et al. Oxidative stress-driven DR5 upregulation restores TRAIL/Apo2L sensitivity induced by iron oxide nanoparticles in colorectal cancer. Biomaterials. 2020;233:119753.
Wang X, Wang Y. Ginsenoside Rh2 Mitigates Pediatric Leukemia Through Suppression of Bcl-2 in Leukemia Cells. Cell Physiol Biochem. 2015;37(2):641–50.
Saraei R, et al. The role of XIAP in resistance to TNF-related apoptosis-inducing ligand (TRAIL) in Leukemia. Biomed Pharmacother. 2018;107:1010–9.
Acknowledgements
This work was supported by the National Natural Science Foundation of China [Grant Number 32071466]; the Project in the Science & Technology Development Plan of Jilin Province [Grant Number 20190304034YY]; the State Key Laboratory of Cell Biology [Grant Number SKLCB2018KF007]; and Fundamental Research Funds for Central Universities.
Author information
Authors and Affiliations
Corresponding authors
Ethics declarations
Conflict of interest
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Liu, W., Wang, S., Yang, Q. et al. 20(s)-ginsenoside Rh2 promotes TRAIL-induced apoptosis by upregulating DR5 in human hepatocellular carcinoma cells. Med Oncol 39, 70 (2022). https://doi.org/10.1007/s12032-022-01663-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s12032-022-01663-6