
Abstract
Objective
Skin metastases from gastric cancer are rare and usually occur very late in the course of the disease. The most common metastatic sites liver, the peritoneal surfaces, and the non regional or distant lymph nodes.
Case report
In this case we report the short-term survival of a 67-year-old man complined of multiple nodular lesions in various part of his skin. Histology showed a metastatic signet ring cell adenocarsinoma. Esophagogastroduodenoscopy was performed and a crater- like ulcer, about 3 cm in diameter, was observed on the anterior part of the stomach corpus distal. A biopsy specimen was obtained, and histopathological findings were consistent with gastric signet-ring cell carcinoma. XELOX chemotherapy regimen was initiated for the patient.
Conclusion
Skin metastasis of gastric adenocarcinoma is a rare condition with a poor prognosis. It may be the first manifestation of a clinically silent visceral cancer or may represent a recurrence of an internal malignancy.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Gastric cancer continues to be a major cancer worldwide and is responsible for over 1,000,000 new cases in 2018 and an estimated 783,000 deaths, making it the fifth most frequently diagnosed cancer and the third leading cause of cancer related death in the world [1]. Gastric signet-ring cell carcinoma (GSRC), a different type of gastric cancer, is consistently increasing in Asia, Europe, and the USA, and accounted for 35–45% of new adenocarcinoma cases [2, 3]. Mostly, metastatic spread from gastric cancer occurs in the liver, the peritoneal surfaces, and the non-regional, or distant lymph nodes; less commonly, in the ovary, central nervous system (brain or leptomeningeal), bone, intrathoracic (pleural or parenchymal), or soft tissue [4]. Cutaneous metastasis is rarely the initial manifestation of gastric cancer [5]. Metastatic involvement of the skin income in less than 10% of patients with malignancy. The primary tumors that most commonly metastasize to the skin are breast carcinoma, lung carcinoma, and melanoma [6]. In fact, skin metastasis from stomach cancer is extremely rare; its incidence has been reported to be 0.8–1.1% [7, 8]. The occurrence of skin metastases in patients with cancer usually reflects a late stage in the course of the disease [6]. Signet-ring cell gastric cancer is a subtype of gastric adenocarcinoma according to the 2010 WHO histological classification. We report a case of a signet ring cell carcinoma of the gastric cardia in which multiple nodular metastatic lesions of the skin were the initial symptom.
Case
A 67-year-old male patient presented to the dermatology clinic with nodular lesions on his eyelid, cheeks, scalp, and back for 20 days (Fig. 1). His previous history is unremarkable. He presented with a weight loss of 8 kg within 1 month.

Appearance of nodular lesions on the face and neck
On his physical examination, there were located swollen, red, painless, solid nodular lesions on his eyelid, cheeks, scalp, right shoulder posterior, near the right inferior scapula, right anterior pelvis, right femur anterolateral, and anterior. These lesions were of various sizes, the largest of which was 5 × 4 mm. Chest auscultation demonstrated bilaterally normal breath sounds, and there were no pathological sounds. No pathological findings were present on cardiac and abdominal examination. There were no palpable axillary, laterocervical, supraclavicular, or inguinal lymph nodes.
Laboratory examination results were as follows: Hgb: 12.1 g/dL (13.7–17.5), Hct: 35.1% (40.1–51), MCV: 85.1 (79–92.2), Plt: 186 10 ^ 3/uL (150–400), BUN: 16 mg/dL (7.9–21), creatinine: 0.8 mg/dL (0.84–1.25), Na: 136 mmol/L (136–146), K: 3.8 (3.5–5.1), ALT: 11 U/L (0–45), AST: 16 U/L (0–35), ALP: 261 U/L (30–120), GGT: 22 U/L (0–55), albumin: 2.9 g/dL (3.5–5.2), Ca: 8.1 mg/dL (8.8– 10.6), P: 3.4 mg/dL (2.5– 4.5), Mg: 2.1 mg/dL (1.8– 2.6). Other biochemical tests including CRP and viral serology tests were performed and resulted within normal limits.
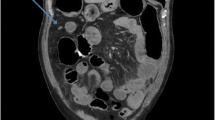
The histomorphologic examination of the posterior right shoulder nodule revealed round cell malignant infiltration, consistent with signet-ring cell carcinoma. Considering the presence of signet ring-like malignant cells containing PAS ( +) intracytoplasmic secret in focal areas within the infiltration, metastatic signet-ring cell carcinoma is considered (Fig. 2). Esophagogastroduodenoscopy was performed, and a crater-like ulcer, about 3 cm in diameter, was observed on the anterior part of the stomach corpus distal. A biopsy specimen was obtained, and histopathological findings were consistent with gastric signet-ring cell carcinoma. This morphologic pattern is associated with adenocarsinoma. Her2 amplification was negative in the molecular analysis of the biopsy material. PET-CT imaging was performed with the intent of tumor staging. The abdominal examination revealed hypermetabolic FDG uptake (SUVmax 6.67) in the gastric corpus. No pathological FDG uptake was detected in the liver, spleen, kidneys, gastrointestinal system, and both in the abdominal and pelvic lymph node groups. Low intensity / mild hypermetabolic involvements (SUVmax 1.68- 3.04) were observed on the skin of right shoulder posterior, near the right inferior scapula, right anterior pelvis, right femur anterolateral, and anterior. On the other hand, multiple pathological lymph nodes at the level of the gastric minor curvature and pathological lymph nodes at the para-aortocaval and interaorthocaval levels were observed in the whole body contrast-enhanced CT imaging. In the thorax, a filling defect with thrombus was observed in the right lung upper lobe pulmonary artery branches. There was no finding in favor of metastasis in the cranial MRI performed on the patient.

Signet-ring morphology with eccentric nuclei, clear cytoplasm, and neutral mucin droplets in the center is observed in some cells in the reticular dermis and tumor cells with atypical pleomorphic nuclei were also evident in skin biopsy
XELOX chemotherapy regimen was initiated for the patient, and low molecular weight heparin (LMWH) was started at a treatment dose for pulmonary embolism. The patient passed away after the third cycle of chemotherapy.
Discussion
The prevalence of skin metastases of visceral tumors amounts to 2% of all skin tumors [9]. Skin metastases are usually detected late in the disease course but may be the initial sign [10]. The occurrence of skin metastases is well defined. Metastatic cutaneous carcinomas typically following characteristics: the painless nodule within the dermis and subcutaneous tissue, the intact and uninvolved elevated epidermis and primarily located in the abdominal wall [11]. The average life expectancy from the appearance of skin nodules to death is 3 months [11]. In our case, the time from the appearance of the skin lesions to the death of the patient was approximately 3 months. Metastatic spread of cancer may occur through the lymphatic system or blood vessels. It may also reach elongated serosal surfaces or perineurium by extending or surgical implantation [12]. The process of metastasis leads histopathologic patterns of metastases namely, intravascular, interstitial, nodular, and intra-epidermal (epidermotropic) [13]. This case supports the concept that metastatic disease is not only a localized process that occurs clinically when a critical size is reached, but also represents a systemic circulatory process.
Conclusion
Gastric signet-ring cell carcinoma is a subtype of gastric adenocarcinoma. Skin metastasis of gastric adenocarcinoma is a rare condition with a poor prognosis. It may be the first manifestation of a clinically silent visceral cancer or may represent a recurrence of an internal malignancy.
References
Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018 Nov;68(6):394–424. https://doi.org/10.3322/caac.21492. Epub 2018 Sep 12. Erratum in: CA Cancer J Clin. 2020;70(4):313.
Taghavi S, Jayarajan SN, Davey A, Willis AI. Prognostic significance of signet ring gastric cancer. J Clin Oncol. 2012;30(28):3493–8. https://doi.org/10.1200/JCO.2012.42.6635 (Epub 2012 Aug 27).
Pernot S, Voron T, Perkins G, Lagorce-Pages C, Berger A, Taieb J. Signet-ring cell carcinoma of the stomach: impact on prognosis and specific therapeutic challenge. World J Gastroenterol. 2015;21(40):11428–38.
Clinical features, diagnosis, and staging of gastric cancer, UpToDate, Author: Paul F Mansfield MD.
Sigon R, Canzonieri V, Rossi C. Early gastric cancer: a single-institution experience on 60 cases. Suppl Tumori. 2003;2:S23–6.
Ruiz SJ, Al Salihi S, Prieto VG, Nagarajan P, Tetzlaff MT, Curry JL, Ivan D, Torres-Cabala CA, Aung PP. Unusual cutaneous metastatic carcinoma. Ann Diagn Pathol. 2019;43:151399.
Hu SC, Chen GS, Wu CS, Chai CY, Chen WT, Lan CC. Rates of cutaneous metastases from different internal malignancies: experience from a Taiwanese medical center. J Am Acad Dermatol. 2009;60:379–87.
Lookingbill DP, Spangler N, Helm KF. Cutaneous metastases in patients with metastatic carcinoma: a retrospective study of 4020 patients. J Am Acad Dermatol 1993;29:228–36.
Nashan D, Müller ML, Braun-Falco M, Reichenberger S, Szeimies RM, Bruckner-Tuderman L. Cutaneous metastases of visceral tumours: a review. J Cancer Res Clin Oncol. 2009;135(1):1–14.
Frey L, Vetter-Kauczok C, Gesierich A, Bröcker EB, Ugurel S. Cutaneous metastases as the first clinical sign of metastatic gastric carcinoma. J Dtsch Dermatol Ges. 2009;7:893–5.
Reingold IM. Cutaneous metastases from internal carcinoma. Cancer. 1966;19(2):162–8.
Resnik KS, DiLeonardo M, Gibbons G. Clinically occult cutaneous metastases. J Am Acad Dermatol. 2006;55(6):1044–7.
Resnik KS. Patterns versus mechanisms of cutaneous metas-tases. Am J Dermatopathol. 1998;20:314.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Ethics Committee Approval
N/A.
Informed Consent
Verbal informed consent was obtained from the patient.
Conflict of Interest
The authors declare no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Bulut, E., Taştekin, E., Topuz, C. et al. Exceptional Variant with Distant Cutaneous Metastasis as the First Clinical Sign in Gastric Signet-Ring Carcinoma. J Gastrointest Canc 53, 1135–1137 (2022). https://doi.org/10.1007/s12029-021-00747-2
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12029-021-00747-2