
Abstract
Cutaneous metastasis from laryngeal carcinoma is an uncommon occurrence. We reported a man with laryngeal squamous cell carcinoma developed cutaneous metastasis on his neck and anterior chest wall after undergoing treatment. Thus, new skin lesions in laryngeal cancer patients may indicate cutaneous metastasis and it signifies poor prognosis.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Distant metastases from squamous cell carcinoma (SCC) of the head and neck to the skin are uncommon and only 1–2% of the cases have been reported [1]. Laryngeal SCC usually metastasizes to the lungs, followed by the liver, bones and central nervous system [2]. The most common presentation of cutaneous metastases is multiple papulonodular lesions but sporadic cases of solitary or multiple keratoacanthoma-like lesions also have been described [3]. Skin metastasis signifies poor prognosis, thus influencing the treatment planning and how the patients should be counseled [4].
Case Report
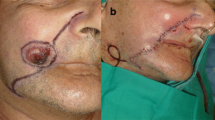
A 64-year-old gentleman presented with generalized weakness and multiple skin nodules over the neck and anterior chest wall for the past 4 months (Fig. 1). The nodules were painless and progressively worsening. Six months prior, he was diagnosed with stage IVb glottic carcinoma and underwent total laryngectomy. The surgery was uneventful and subsequently completed radiotherapy to a total dose of 70 Gy in 35 fractions over 7 weeks. However, he was complicatedly diagnosed with radiation dermatitis 4 months after he completed radiotherapy.

Extensive skin nodules over the neck extending to the anterior chest wall can be seen in anterior view (a) and lateral view (b)
Skin biopsy taken from the nodule revealed there is infiltration of malignant cells arranged in nests and cords surrounded by desmoplastic stroma. The tumour cells exhibit moderate nuclear pleomorphism with round to oval vesicular nucleoli, prominent nucleoli and abundant cytoplasm. The biopsy margin shows presence of tumour and the overlying dermis shows no dysplasia. Immunohistochemical studies were positive for CK 5/6 which is suggestive of metastatic squamous cell carcinoma.
Computed tomography (CT) of neck and thorax revealed diffused skin and soft tissue thickening at the anterior neck extending to the submandibular region to the anterior chest wall. No metastatic nodule was noted in the lungs or abdomen region. Given the deteriorating general condition and poor performance status, supportive and palliative care was offered to the patient. The patient succumbed to the disease three months after the diagnosis was made.
Discussion
The diagnosis of squamous cell carcinoma can be made primarily from the history, physical examination, and ultimately from the biopsy of the lesion. Most common sites of distant metastasis from SCC of head and neck are lungs (70–85%), liver (10–30%), and bone (15–39%) [5]. Cutaneous metastases from the larynx are rare and only fourteen cases have been reported [6]. It is reported that most skin metastases occurred in older males aged 58 to 75, typically within two years of diagnosis [7].
The exact mechanism of how skin metastases can occur from laryngeal carcinoma is unknown. Distant skin metastases are thought to develop through hematogenous spread, whereas local metastases occur by spread via the dermal lymphatics. A few studies have suggested that skin invasion likely spreads along subdermal lymphatics, leaving residual microscopic disease in the lymphatic system [8]. It is suggested that radiotherapy increases the vulnerability of the skin region to other conditions such as cutaneous metastases or opportunistic infections [9]. The most common primary source of cutaneous metastases in females is breast carcinoma while in male patients is from the lung. However, almost any internal cancer can metastasize to the skin [10].
Cutaneous metastases from laryngeal carcinoma may present as multiple painless, firm papulonodular lesions, mimicking an inflammatory process or even keratoacanthoma-like lesions that can occur anywhere on the body. Other presentation of skin metastases from SCC malignancies such as ulcero-proliferative nodules, are also reported [6]. Cutaneous metastases can be found regionally in the skin of the neck/chest, nasal tip, and distant skin sites such as the abdomen, umbilicus, back, and upper limb [4]. In our case, the patient presented with multiple painless nodules over the skin at the neck and chest region, which was the previous radiated site.
Skin metastasis is associated with poor prognosis. The presence of dermal lymphatic tumour spread is a sign of advanced disease with a similar prognosis to distant metastatic tumour spread [2]. The average mean survival is 6 months from the diagnosis of skin metastases [4]. Treatment in these cases is usually palliative and must be individualized. Although the current standard of care for patients with cutaneous metastases includes curative surgical resection with adjuvant chemoradiation, it is unlikely to extend survival rate significantly [8]. As a result of the patient’s deteriorating condition, he chose to receive palliative and comfort care after the diagnosis.
Conclusion
Laryngeal carcinoma with skin metastases is rare. Treatment options currently available are ineffective in addressing skin metastases, posing a challenge in providing adequate care for patients with this condition. Early detection of skin metastasis is very important as it carries poor prognosis and short life expectancies, hence the treatment aims to relieve patients’ symptoms and improve quality of life.
References
Ellis DL, Riahi RR, Murina AT, Cohen PR (2014) Metastatic laryngeal carcinoma mimicking eruptive keratoacanthomas: report of keratoacanthoma-like cutaneous metastases in a radiation port. Dermatol Online J 20(9)
Spector JG, Sessions DG, Haughey BH, Chao KSC, Simpson J, El Mofty S et al (2001) Delayed Regional metastases, distant metastases, and second primary malignancies in squamous cell carcinomas of the larynx and hypopharynx. Laryngoscope 111(6):1079–1087
Riahi RR, Cohen PR (2013) Malignancies with skin lesions mimicking Keratoacanthoma. Dermatol Online J 19(11):20397
Emanuel H, Emanuel P Cutaneous metastasis of head and neck malignancy. Int J Head Neck Surg 6(2):57–63
Takes RP, Rinaldo A, Silver CE, Haigentz M, Woolgar JA, Triantafyllou A et al (2012) Distant metastases from head and neck squamous cell carcinoma. Part I. Basic aspects. Oral Oncol 48(9):775–779
Trehan R, Pandey AK, Khosla D, Dimri K, Punia RS (2015) Apropos of a case of cutaneous metastasis from laryngeal cancer with review of literature. J Cancer Res Ther 11(3):655
Bottoni U, Innocenzi D, Mannooranparampil TJ, Richetta A, Giudice M, Del CS (2001) Inflammatory cutaneous metastasis from laryngeal carcinoma. Eur J Dermatology 11(2):124–126
Diebolt JH, Yu KM, Wood S, Ziegler A, France A, Villwock MR et al (2023) Prognostic implications of skin invasion in locally advanced oral cavity squamous cell carcinoma. Otolaryngol Head Neck Surg 169(1):69
Araghi F, Fatemi A, Rakhshan A, Moravvej H, Tabary M, Dadkhahfar S (2020) Skin metastasis of laryngeal carcinoma presenting as multiple eruptive nodules. Head Neck Pathol 14(4):1154
Alcaraz I, Cerroni L, Rütten A, Kutzner H, Requena L (2012) Cutaneous metastases from internal malignancies: a clinicopathologic and immunohistochemical review. Am J Dermatopathol 34(4):347–393
Author information
Authors and Affiliations
Corresponding author
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Ariffin, N.I.N.M., Dahari, K.A.S.A., Gani, N.A. et al. A Rare Manifestation of Cutaneous Metastasis from Laryngeal Carcinoma. Indian J Otolaryngol Head Neck Surg (2024). https://doi.org/10.1007/s12070-024-04981-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s12070-024-04981-5