
Abstract
Background
Mild hypothermia is an effective neuroprotective strategy for a variety of acute brain injuries. Cooling the nasopharynx may offer the capability to cool the brain selectively due to anatomic proximity of the internal carotid artery to the cavernous sinus. This study investigated the feasibility and efficiency of nasopharyngeal brain cooling by continuously blowing room temperature or cold air at different flow rates into the nostrils of normal newborn piglets.
Methods
Experiments were conducted on thirty piglets (n = 30, weight = 2.7 ± 1.5 kg). Piglets were anesthetized with 1–2 % isoflurane and were randomized to receive one of four different nasopharyngeal cooling treatments: I. Room temperature at a flow rate of 3–4 L min−1 (n = 6); II. −1 ± 2 °C at a flow rate of 3–4 L min−1 (n = 6); III. Room temperature at a flow rate of 14–15 L min−1 (n = 6); IV. −8 ± 2 °C at a flow rate of 14–15 L min−1 (n = 6). To control for the normal thermal regulatory response of piglets without nasopharyngeal cooling, a control group of piglets (n = 6) had their brain temperature monitored without nasopharyngeal cooling. The duration of treatment was 60 min, with additional 30 min of observation.
Results
In group I, median cooling rate was 1.7 ± 0.9 °C/h by setting the flow rate of room temperature air to 3–4 L min−1. Results of comparing different temperatures and flow rates in the nasopharyngeal cooling approach reveal that the brain temperature could be reduced rapidly at a rate of 5.5 ± 1.1 °C/h by blowing −8 ± 2 °C air at a flow rate of 14–15 L min−1.
Conclusions
Nasopharyngeal cooling via cooled insufflated air can lower the brain temperature, with higher flows and lower temperatures of insufflated air being more effective.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Clinical investigators have reported that mild and moderate hypothermia can be neuroprotective to reduce brain injury and decrease death and disability for a variety of acute brain injuries following cardiac arrest, and neonatal asphyxia [1–3]. The neuroprotective benefits of hypothermia have been linked to the time to initiate cooling after injury, depth of cooling and rewarming rate [4, 5]. Clinical studies indicate that the temperature range associated with better outcomes appears to be 32–35 °C [6, 7]. The optimal timing of induction of therapeutic hypothermia is still uncertain. However, laboratory data have suggested that there is significantly decreased neurological injury if cooling is initiated as soon as possible after resuscitation [8–10]. Cooling the whole body below 34 °C can cause complications including, shivering, skin erythema, renal failure, coagulopathy, pulmonary hypertension, and increased mortality [11, 12]. Moreover, it may decrease perfusion and oxygenation by impairing myocardial contractility, reducing cardiac output and making the heart more prone to arrhythmia [13, 14]. Such complications along with other ones offset the benefits accrued from the neuroprotective effects of hypothermia. Therefore, in order to avoid the complications associated with systemic hypothermia, it is very important to develop a selective brain cooling (SBC) approach that can be initiated as early as possible to reduce the temperature of the brain tissue uniformly.
Based on anatomical features, blowing cold air into the nasopharynx may offer the capability to cool the brain selectively by cooling blood in both internal carotid arteries via counter-current heat exchange mechanism with the neighboring cavernous sinuses which collect cold venous blood from the mucosal linings of the nasal cavities. Furthermore, cerebrospinal fluid (CSF) chilled at the basal cistern cools the whole brain through the CSF circulation. In the present study, we evaluate the feasibility and efficiency of nasopharyngeal SBC by blowing room temperature or cold air (medical air) into the nostrils at two different flow rates in normal newborn piglets with developed thermal regulation.
Materials and Methods
Animals Preparation and Experimental Procedure
Experiments were conducted on thirty piglets (17 females and 13 males) with an average age of 47 ± 14 h and an average weight of 2.7 ± 1.5 kg. All animal experiments were approved by the Animal Use Subcommittee of the Canadian Council on Animal Care at the University of Western Ontario. Newborn Duroc cross piglets were obtained from a local supplier on the morning of the experiment. Piglets were induced with 4 % isoflurane and then maintained on 2–3 % for preparatory surgery. The 4 % isoflurane provided a rapid induction of anesthesia within 15–30 s while the 2–3 % isoflurane maintained surgical anesthesia, allowing surgical procedures to be performed without any physiological signs of pain or changes of hemodynamic parameters. A tracheotomy was performed and the piglet was ventilated with a volume-controlled mechanical ventilator to deliver oxygen/medical air mixture (2:1). A femoral artery was catheterized to monitor heart rate (HR) and mean arterial blood pressure (MAP) and to intermittently collect arterial blood samples for gas (p a CO2, p a O2), pH and glucose analyses. Arterial CO2 tension (p a CO2) was monitored throughout the experiment, either directly by blood gas measurements or by the end-tidal CO2 tension, and maintained at normocapnia between 37 and 42 mmHg by adjusting the breathing rate and volume. Arterial oxygen tension (p aO2) was maintained at a level between 90 and 130 mmHg by adjusting the ratio of oxygen to medical air. Blood glucose was monitored intermittently and if it fell below 4.5 mmol/L, a 1–2 mL infusion of 25 % glucose solution was administered intravenously. Rectal temperature was recorded from a rectal probe inserted to 3–4 cm from the anal margin. Brain temperature was also measured continuously with a thermocouple probe (Thermometer/Data Logger, HH309A, Type K Thermocouple Inputs, Omega Engineering, Stamford CT; resolution 0.1 °C/0.1 °F). A burr hole 1.5 cm posterior to the bregma along the mid-line was made in the skull with a Dremel tool. The needle thermocouple probe was inserted through the burr hole into the brain to a depth of 2 cm from the brain surface to measure brain temperature.
After surgery, piglets were wrapped with a heated water blanket that was used to maintain the piglets normothermic at 38 ± 0.5 °C for 60 min prior to the initiation of cooling. The temperature control was then discontinued, and the piglets were randomized to receive one of four different nasopharyngeal cooling treatments which involved blowing either room or cold air at either one of two flow rates as were measured and regulated by a flow meter (Timeter Instrument, St Louis, Missouri) into both nostrils of piglets:
-
I.
Room temperature (21 ± 1 °C) at a flow rate of 3–4 L min−1 (n = 6);
-
II.
−1 ± 2 °C at a flow rate of 3–4 L min−1 (n = 6);
-
III.
Room temperature (21 ± 1 °C) at a flow rate of 14–15 L min−1 (n = 6);
-
IV.
−8 ± 2 °C at a flow rate of 14–15 L min−1 (n = 6).
To control for the normal thermal regulatory response of piglets without nasopharyngeal cooling, a control group of piglets (n = 6) had their brain temperature monitored without nasopharyngeal cooling.
Method of Nasopharyngeal Brain Cooling
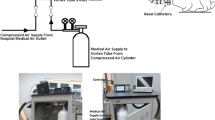
Nasopharyngeal brain cooling was achieved by directing room temperature or cooled air via a catheter in each nostril into the nasal cavities. The nasal catheter comprises a tubular body defining a lumen and an open end in continuous fluid communication with the compressed air hose, and first and second tubular nasal prongs extend from the tubular body (Fig. 1). Each catheter was lubricated with 2 % lidocaine gel for anesthesia and inserted 4–5 cm into each nostril. Air was delivered into the nasal catheters from a pressurized tank through a flow regulator, a pump and a cooling unit (Polyscience refrigerated/heated circulating bath with performance digital temperature controller, model PD07R-40, Polyscience International Inc, Illinois, USA). The circuit was customized by replacing the pump tube with a double-walled tube with circulating cooling liquid (Ethylene glycol, VWR International Inc) in the outer tube and directing medical air (supplied by L’Air Liquide Ltd with the capacity of 232 ft [3] at fill-pressure of 2265 psig) through the inner tube (Fig. 1). Before starting the cooling process, the cooling unit was set to −25 °C with a temperature stability of ±0.05 °C over 30–45 min; the same settings were kept during the entire experiment. Induction of hypothermia was initiated by directing air at the required temperature, either −1 ± 2 °C or −8 ± 2 °C measured at the tip of the nasal catheter and flow rate, either 3–4 or 14–15 L min−1, into the nasal catheters. Once the brain temperature stabilized, the flow rate was decreased to 1 ± 0.5 L min−1 to maintain the lower temperature reached at after an hour of cooling for 30 min.

Schematic representation of the cooling circuit used for nasal cooling. The 7 L container was filled with a cryogenic cooling liquid (Ethylene glycol)
H&E Histopathological Examination
The piglets were sacrificed at the end of the experiment by intravenous injection of potassium chloride (1–2 mL/kg, 2 mEq/mL) while on 5 % inhaled isoflurane. For each piglet, the brain and the snout were excised. Coronal sections of the brain (cut into the 4–5 mm-thick sections) and the snout (at the region of the premolar tooth) were obtained. The tissue sections were fixed in 10 % neutral buffered formalin for 24–48 h, and then transferred into a phosphate buffer saline solution for preservation. These tissue fragments were then paraffin-embedded, cut into 5 µm-thick sections and stained with Hematoxylin and Eosin (H&E) for histopathological examination.
Statistical Analysis
SPSS 17.0.0 (SPSS, Inc, Chicago, IL) was used for all statistical analyses. Normality of the distribution of the measurements was verified using Kolmogorov–Smirnov test. Comparisons of vital signs were analyzed by two-way analysis of variance with group and time as the two factors followed by post hoc test with Bonferroni correction to determine statistical differences at different times within a group and between groups at different times. Statistical significance was based on p value <0.05. All data are presented as mean ± standard deviation unless otherwise noted.
Results
Table 1 displays a summary for the averaged physiologic parameters (MAP, HR, S a O2, pH, tHb, p a O2, and p a CO2) in Group I–IV and control, prior to and during cooling. There was no significant difference in any physiological parameter between the groups at baseline. No significant p a CO2, SaO2, tHb or pH differences were found among different time points. All monitored physiological parameters dropped slowly through the cooling but only HR and MAP decreased significantly (p < 0.05) at the higher flow rate of 14–15 L min−1 or lower temperature of −8 ± 2 °C. However, since the maximum decrease in both HR and MAP at the end of cooling was less than 20 %, no remedy was instituted to correct for these decreases. Arrhythmias were not observed during cooling.
Figure 2 displays the average cooling rates achieved with different nasopharyngeal cooling methods. At the low flow rate of 3–4 L min−1 mean brain cooling rate was significantly greater (p < 0.05) with −1 ± 2 °C than room temperature air. Using either room temperature or chilled air (−1 ± 2 °C or −8 ± 2 °C), there was statistically significant (p < 0.05) greater brain cooling rate with high (14–15 L min−1) than low (3–4 L min−1) flow rate. In the control group, both rectal and brain temperature did not drop more than 0.5 °C (brain: 0.35 ± 0.3 °C; rectal: 0.35 ± 0.3 °C).

Mean brain cooling rate with different nasopharyngeal cooling methods. Asterisk signifies a statistically significant (p < 0.05) difference between high flow rate and low flow rate at both cold and room temperature; hash signifies a statistically significant (p < 0.05) difference between cold temp and room temp at low flow rate (3–4 L min−1)
Following 60 min of baseline to demonstrate relatively constant brain (38.8 ± 0.2 °C) and rectal (38.4 ± 0.2 °C) temperature over this period, brain temperature started falling immediately after the initiation of nasopharyngeal cooling with room temperature air at a flow rate of 3–4 L min−1. One hour post cooling, the brain and rectal temperatures were 37.1 ± 0.9 °C and 37.2 ± 0.5 °C which resulted in mean cooling rates of 1.7 ± 0.9 °C/h and 1.2 ± 0.5 °C/h, respectively, as displayed in Fig. 3(a). With the air flow rate at 3–4 L min−1, the brain and rectal cooling rates were increased by decreasing the air temperature to −1 ± 2 °C by circulating cryogenic cooling liquids in the outer tube of the double-walled pump tube. Figure 3(b) shows both brain and rectal temperature decreased from 38.5 ± 0.7 °C and 38.4 ± 0.7 °C to 34.8 ± 1.7 °C and 35.3 ± 1.7 °C which corresponded to cooling rates of 3.7 ± 1.1 °C/h and 3.1 ± 0.6 °C/h, respectively. Figure 3 shows that it was possible to maintain brain at the temperature arrived at after an hour of cooling with a variation of 0.35 ± 0.45 °C by decreasing the air flow rate to 1 ± 0.5 L min−1. No significant differences were found between brain and rectal cooling rates for either air temperature at the flow rate of 3–4 L min−1. During the baseline monitoring period, brain and rectal temperatures variations were the same (brain: 0.4 ± 0.4 °C; rectal: 0.4 ± 0.5 °C).

Brain and rectal temperature over time for nasopharyngeal cooling method with a room temperature at a flow rate of 3–4 L min−1, b −1 ± 2 °C air at a flow rate of 3–4 L min−1, c room temperature at a flow rate of 14–15 L min−1, and d −8 ± 2 °C air at a flow rate of 14–15 L min−1. Asterisk signifies a statistically significant (p < 0.05) difference between brain and rectal temperature
By increasing flow rate to 14–15 L min−1 at room temperature, Fig. 3(c) demonstrates that brain and rectal temperature could be reduced more rapidly at mean rates of 4.6 ± 1.2 °C/h and 3.1 ± 1.2 °C/h, respectively. Mean brain temperature decreased to 33.9 ± 1.7 °C within approximately 60 min of cooling from baseline (38.5 ± 1.1 °C). Figure 3(d) shows even greater cooling rate using −8 ± 2 °C air at the same flow rate. Both brain and rectal temperature decreased from 38.4 ± 0.8 °C and 38.1 ± 0.8 °C to 32.9 ± 1.1 °C and 35.2 ± 0.7 °C which corresponded to a 5.5 ± 1.1 °C/h and 2.9 ± 0.7 °C/h, respectively. At this higher air flow rate of 14–15 L min−1, there were significant differences between brain and rectal temperature during cooling for either room temperature or −8 ± 2 °C air. After cooling with room temperature or −8 ± 2 °C air at a flow rate of 14–15 L min−1 (but not with 3–4 L min−1), the rectal temperature continued to decrease during the following 30 min when the air flow rate was decreased to 1 ± 0.5 L min−1 to maintain the brain temperature (Fig. 3 (a, b) vs Fig. 3 (c, d)).
Brain–body temperature gradient, calculated as the difference between brain and rectal temperature, for room temperature or −8 ± 2 °C air at the flow rate of 14–15 L min−1 over the baseline and the cooling period is shown in Fig. 4(a). The temperature gradient reached −1.8 ± 0.7 °C after 20 min of cooling and remained significant (p < 0.05) during the rest of cooling period (Fig. 4(b)).

Brain-rectal temperature gradient over time for intranasal cooling method with setting the air flow rate to 14–15 L min−1 at a room temperature and b cold temperature. Asterisk a statistically significant (p < 0.05) difference compared to the baseline
Figure 5(a)–(c) show H&E histopathological examination results of the frontal lobe of the brain and nasal conchae (turbinates) from the nasal cavity of a piglet. There were no pathological findings of bleeding, erythema and blister in the turbinates and of necrosis in the frontal lobe of brains in both gross and H&E histopathological examinations.

Representative H&E histology shows a normal brain cells in gray and white matter of the frontal lobe and b and c intact pseudostratified cilia and conchae (turbinates) cells in the nasal cavity after the nasal cooling process using the air temperature of −8 ± 2 °C air at a flow rate of 14–15 L min−1
Discussion
When the nasal cavity is cooled down, SBC is achieved via heat exchange at the cavernous sinus between cold venous blood from nasal mucosa and warm arterial blood in the carotid rete mirabile on route to the brain [15]. Based on this heat exchange method, we showed that rapid temperature changes in the brain can be achieved by blowing −8 ± 2 °C air at a flow rate of 14–15 L min−1 into the nasal cavity: the brain temperature dropped from 38.4 ± 0.8 °C to 32.9 ± 1.1 °C in 60 min or a cooling rate of 5.5 ± 1.1 °C/h while the body temperature as measured by the rectal temperature probe was >35 °C during cooling. Similarly, Covaciu et al., demonstrated the method of selectively cooling the brain (≈3 °C/h) with cold saline (8–10 °C) circulating in balloon catheters placed into the nasal cavities of large pigs [16]. Likewise, Wolfson et al, employs transnasal evaporative cooling system by spraying of perfluorocarbon liquid (perfluorohexane, PFH; F2 Chemicals) at room temperature which was driven by compressed oxygen into the nasal cavities to achieve average intranasal brain cooling rate of ≈4 °C/h in sheeps [17]. The influence of nasopharyngeal cooling on brain temperature under different range of circulatory states such as untreated cardiac arrest (“no-flow”) or during normal circulation (“normal-flow”) and cardiopulmonary arrest (CPR) situation (“low-flow”) was also shown in a porcine model in a study by Boller et al. [18]. Nasopharyngeal cooling device, RhinoChill (BeneChill, Inc, SanDiego, CA, USA), shows that the brain can be preferentially cooled compared with the other compartments of the body with an average cerebral temperature decrease of −4.7 °C for normal flow, −4.3 °C for no flow and −3.4 °C for low flow after 60 min [18]. Intranasal cooling was beneficial even after prolonged cardiac arrest in a porcine model, where it significantly improved the return of spontaneous resuscitation rate and reduced CPR duration [19, 20]. The administration of cold nasal air flow and intranasal cooling were both tested in human studies [21–24]. These methods proved to be feasible and improved the neurological outcome. However, evaluating the effect of selective cooling methods on the human brain is challenging because direct measurements of the brain temperature cannot be made without the need for surgery. Furthermore, invasive temperature measurements do not inform on the intra-cerebral distribution of temperature changes induced by these methods. The RhinoChill device vaporizes perfluorocarbon along by oxygen at flow rate of 60–80 L min−1 with a catheter system into the nasal cavity leading to a fast induction of hypothermia initially in brain as the main target organ, resulting in delayed systemic hypothermia [21]. However, Perfluorocarbons raise environmental and health issues. They are powerful greenhouse gases and deplete the ozone layer and are listed as toxic substances under the Canadian Environmental Protection Act [25]. Another safety concern is the risk of coolant aspiration which might cause lung damage over prolonged periods since neural protection therapy may involve mild hypothermia being maintained for a period of 72 h [26]. Therefore, new cooling methods should be effective in terms of safety, fast cooling rates and easy to apply in the pre-clinical setting.
We explored a method of nasopharyngeal cooling by continuously blowing room temperature or cold air into the nostrils at different conditions on normal newborn piglets with developed thermal regulation. Piglets were studied because they are commonly used animal model of newborn human neurology [27]. The newborn piglets in the present study had an average body temperature of 38.2 ± 0.6 °C (range 37.5–38.8 °C), which was within the normal temperature range of piglets. Thermoregulatory response in newborn piglets were progressively achieved after 48 h of birth [28]. In our study, brain temperature decreased with a mean cooling rate of 1.7 ± 0.9 °C after the start of cooling procedure, by setting the air flow rate to 3–4 L min−1. The rate of brain cooling can be improved by increasing the air flow rate and/or decreasing the temperature of circulating cryogenic cooling liquids in outer tube of heat exchanger. Brain temperature reduced more rapidly at a rate of 5.5 ± 1.1 °C/h with increasing air flow to 14–15 L min−1 at cold temperature (−8 ± 2 °C air). Rectal temperature continued to decrease till it equilibrated to the brain temperature during the maintenance period. Since 25 % of the cardiac output goes to the brain, the decline in rectal temperature was due to whole body cooling subsequent to cooling of the blood supplying the brain. In this study, the body of the piglets was only covered with linen sheets and no external heating sources were utilized. In future experiments, the drop in core temperature can be controlled using recirculating heated water blanket and packing hot water gloves around the body of the piglets. Finally, newborn piglets are known to have less established heat regulation than more mature piglets [29]. The temperature of cooled air achieved at tip of the catheter at high flow rate (14–15 L min−1) is lower than the case of low air flow rate (3–4 L min−1) i.e., −8 ± 2 °C and –1 ± 2 °C, respectively. This is due to the increase in the rate of convective heat transfer between cryogenic cooling liquid (Ethylene glycol) in the outer tube and directing medical air through the inner tube. The temperature of −8 ± 2 °C and a flow rate of 14–15 L min−1 were chosen from the results of a small series of titration experiments in n = 6 pigs in which both temperature and flow rate were adjusted with the target of cooling the brain to 32–34 °C within 30–45 min. Although it is unlikely that air at subzero temperature will induce freezing damage to the mucosa and embedded blood vessels and nerves of the nasal cavity, we monitored temperature inside the nasal cavity to avoid subzero temperature. A thermistor was placed at the tip of one of the two nasal catheters to measure temperature inside the nasal cavity throughout the experiments. Even at a flow rate of 14–15 L min−1 and a temperature of −8 ± 2 °C air was warmed rapidly along the nasal catheters before reaching the nasopharyngeal tissue. An average temperature of about 7–8 °C was consistently measured with the catheter tip thermistor. Regardless of cooling conditions, HR and MAP decreased with cooling. The level of gaseous carbon dioxide, or P aCO2, in arterial blood depends on the solubility coefficient of this gas, which is dependent on temperature and decreases as temperature decreases [30]. The CO2 gas crosses the blood–brain barrier and transmits the induced modifications (e.g., alkalosis in hypothermia [31]) to the extracellular environment, which regulates the state of arteriolar vascular tone. This explains why hypothermia-induced hypocapnia may cause arteriolar vasoconstriction and a decrease in intracranial pressure [32]. Moreover, hypothermia may induce metabolic disturbances and electrolyte abnormalities [33]. Such electrolyte disorders can lead to the potentially lethal arrhythmias and other harmful complications [34]. Therefore, in the next set of experiments, frequent measurement of electrolytes during hypothermia will be instituted to prevent critically change in electrolytes levels and guide the appropriate amount of replenishment.
There are some limitations/concerns with our approach that need to be addressed prior to clinical implementation. Firstly, there are anatomical and physiological differences between newborn piglets and humans that are important in this context. The baseline temperature in newborn piglets and humans is different. Pigs differ considerably to humans in their ratio between the size of their nasal cavity and their brain. Importantly, the newborn piglet, in contrast to humans, has a carotid rete that may be a SBC system specific for the pig. Based on the relatively rapid cooling rate achieved in this study by setting the air flow rate to 14–15 L min−1, we suggest that nasopharyngeal cooling with this technique still has great potential for inducing hypothermia on large animal or human by increasing air flow rate up to 30–40 L min−1. Additionally, the higher heat production of large animal model or human comparing to newborn piglet would lead to a better brain-core temperature gradient and consequently better SBC. Secondly, in all of the experimental studies anesthesia was maintained with 1–2 % isoflurane until the end of the experiment without more than 20 % decreases in blood pressure, heart rate, or oxygen saturation. Isoflurane was used as the main anesthetic in the present study, as its administration is easy to apply and quick to control the level of anesthesia. This avoids problems associated with injectable anesthetics, such as a lack of agents to reverse their activity rapidly in case of overdose or possible side-effects. Isoflurane has been shown to minimally influence systemic arterial blood pressure and cardiac output over several hours of anesthesia [35]. However, isoflurane inhibits thermoregulatory responses [36, 37], typically reducing the thresholds for vasoconstriction and shivering by approximately 3 °C and increasing the thresholds for sweating and vasodilation by approximately 1 °C, thus limiting the stress response to cold exposure. Additionally, cooling of the piglet’s brain resulted in hypotension (32 ± 4 mmHg after 1 h of cooling) which is likely a combined effect of temperature reduction, the age of the animal and general anesthesia. Therefore, cerebral perfusion, an important mechanism for the cooling kinetics with nasopharyngeal cooling, will be decreased at that degree of hypotension and might confound the cooling efficiency. Another limitation of this study is that the brain temperature was measured only at one position, and therefore no information was obtained about homogeneity of regional brain temperature. However, two preliminary experiments had examined the temperature gradient within a piglet’s brain, calculated as the difference between frontal and parietal lobes by inserting one probe in each region, and this was found to be no more than 0.1 °C. A final concern with this study is that core body temperature was measured by the rectal temperature probe which may correlate less well with core temperature than esophageal temperature. However, the temperature difference between rectal and esophageal was examined in one experiment and was not more than 0.3 °C.
In conclusion, we have demonstrated that nasopharyngeal cooling by spraying and cooled air into nasal cavities is an effective, feasible, and simple method to selectively reduce brain temperature of newborn piglets. Although the results from this study were encouraging; more experiments with larger animal models for longer periods of cooling time are required to evaluate the efficiency and reliability of the cooling system and reproducibility of the results. Also, to evaluate the efficiency of the method and reproducibility of the cooling, we will switch to a large animal model, juvenile pigs in our next set of experiments, and explore maintenance of the brain–body temperature gradient during 6–7 h cooling and gradual rewarming. We will measure physiological parameters, particularly HR and MAP, as in the current series of experiments and additionally electrolytes during cooling, maintenance, and rewarming phase’s experiments. If HR and MAP decrease more than 20 % from baseline, inotrope, and pressor agents will be administered to return both parameters closer to baseline levels.
References
Sadaka F, Veremakis C. Therapeutic hypothermia for the management of intracranial hypertension in severe traumatic brain injury: a systematic review. Brain Inj. 2012;26:899–908.
Quinn MW, Munyard PF. Treatment of asphyxiated newborns with moderate hypothermia in routine clinical practice: how cooling is managed in the UK outside a clinical trial. Arch Dis Child Fetal Neonatal Ed. 2010;95:F152.
Uray T, Haugk M, Sterz F, Arrich J, Richling N, Janata A, Holzer M, Behringer W. Surface cooling for rapid induction of mild hypothermia after cardiac arrest: design determines efficacy. Acad Emerg Med. 2010;17:360–7.
Moore EM, Nichol AD, Bernard SA, Bellomo R. Therapeutic hypothermia: benefits, mechanisms and potential clinical applications in neurological, cardiac and kidney injury. Injury. 2011;42:843–54.
Povlishock JT, Wei EP. Posthypothermic rewarming considerations following traumatic brain injury. J Neurotrauma. 2009;26:333–40.
Bullock MR, Povlishock JT. Guidelines for the management of severe traumatic brain injury. J Neurotrauma. 2007;24(Suppl 1):S1–106.
Mathur NB, Krishnamurthy S, Mishra TK. Evaluation of who classification of hypothermia in sick extramural neonates as predictor of fatality. J Trop Pediatr. 2005;51:341–5.
Sterz F, Safar P, Tisherman S, Radovsky A, Kuboyama K, Oku K. Mild hypothermic cardiopulmonary resuscitation improves outcome after prolonged cardiac arrest in dogs. Crit Care Med. 1991;19:379–89.
Jia X, Koenig MA, Shin HC, Zhen G, Pardo CA, Hanley DF, Thakor NV, Geocadin RG. Improving neurological outcomes post-cardiac arrest in a rat model: immediate hypothermia and quantitative eeg monitoring. Resuscitation. 2008;76:431–42.
Zhao D, Abella BS, Beiser DG, Alvarado JP, Wang H, Hamann KJ, Hoek TL, Becker LB. Intra-arrest cooling with delayed reperfusion yields higher survival than earlier normothermic resuscitation in a mouse model of cardiac arrest. Resuscitation. 2008;77:242–9.
Eun D, Bhandari A, Boris R, Lyall K, Bhandari M, Menon M, Rogers CG. A novel technique for creating solid renal pseudotumors and renal vein-inferior vena caval pseudothrombus in a porcine and cadaveric model. J Urol. 2008;180:1510–4.
Culic S. Cold injury syndrome and neurodevelopmental changes in survivors. Arch Med Res. 2005;36:532–8.
Dudgeon DL, Randall PA, Hill RB, McAfee JG. Mild hypothermia: its effect on cardiac output and regional perfusion in the neonatal piglet. J Pediatr Surg. 1980;15:805–10.
Sanae T, Kazama S, Nie M, Miyoshi Y, Machii M, Ohara K, Yoshimura H. Free-floating left atrial ball thrombus early after mitral valve replacement. Ann Thorac Cardiovasc Surg. 2000;6:408–10.
Gillan LA. Blood supply to brains of ungulates with and without a rete mirabile caroticum. J Comp Neurol. 1974;153:275–90.
Covaciu L, Allers M, Enblad P, Lunderquist A, Wieloch T, Rubertsson S. Intranasal selective brain cooling in pigs. Resuscitation. 2008;76:83–8.
Wolfson MR, Malone DJ, Wu J, Hoffman J, Rozenberg A, Shaffer TH, Barbut D. Intranasal perfluorochemical spray for preferential brain cooling in sheep. Neurocrit Care. 2008;8:437–47.
Boller M, Lampe JW, Katz JM, Barbut D, Becker LB. Feasibility of intra-arrest hypothermia induction: a novel nasopharyngeal approach achieves preferential brain cooling. Resuscitation. 2010;81:1025–30.
Tsai MS, Barbut D, Wang H, Guan J, Sun S, Inderbitzen B, Weil MH, Tang W. Intra-arrest rapid head cooling improves postresuscitation myocardial function in comparison with delayed postresuscitation surface cooling. Crit Care Med. 2008;36:S434–9.
Wang H, Barbut D, Tsai MS, Sun S, Weil MH, Tang W. Intra-arrest selective brain cooling improves success of resuscitation in a porcine model of prolonged cardiac arrest. Resuscitation. 2010;81:617–21.
Thoresen M, Hobbs CE, Wood T, Chakkarapani E, Dingley J. Cooling combined with immediate or delayed xenon inhalation provides equivalent long-term neuroprotection after neonatal hypoxia-ischemia. J Cereb Blood Flow Metab. 2009;29:707–14.
Harris BA, Andrews PJ, Murray GD. Enhanced upper respiratory tract airflow and head fanning reduce brain temperature in brain-injured, mechanically ventilated patients: a randomized, crossover, factorial trial. Br J Anaesth. 2007;98:93–9.
Mariak Z, White MD, Lewko J, Lyson T, Piekarski P. Direct cooling of the human brain by heat loss from the upper respiratory tract. J Appl Physiol. 1985;1999(87):1609–13.
Dohi K, Jimbo H, Abe T, Aruga T. Positive selective brain cooling method: a novel, simple, and selective nasopharyngeal brain cooling method. Acta Neurochir Suppl. 2006;96:409–12.
Enviroment Canada (http://www.Ec.Gc.Ca/toxiques-toxics/default.Asp?Lang=en&n=98e80cc6-1&xml=aa329670-c3c7-4ad5-a7ab-5fd8a05439f1) [accessed 29 August, 2012].
Azzopardi D, Strohm B, Edwards AD, Halliday H, Juszczak E, Levene M, Thoresen M, Whitelaw A, Brocklehurst P, Steering G, Participants TCR. Treatment of asphyxiated newborns with moderate hypothermia in routine clinical practice: How cooling is managed in the UK outside a clinical trial. Arch Dis Child Fetal Neonatal Ed. 2009;94:F260–4.
Roohey T, Raju TN, Moustogiannis AN. Animal models for the study of perinatal hypoxic-ischemic encephalopathy: a critical analysis. Early Hum Dev. 1997;47:115–46.
Herpin P. Development of thermoregulation and neonatal survival in pigs. Livest Prod Sci. 2002;78:25–45.
Bakhsheshi MF, Stewart EE, Morrison L, Lee TY. Comparison of selective brain cooling in juvenile and newborn piglets using a nasopharyngeal method. The 8th International Conference on Brain Monitoring and Neuroprotection in the newborn. 2014.
Bratton SL, Chestnut RM, Ghajar J, McConnell Hammond FF, Harris OA, Hartl R, Manley GT, Nemecek A, Newell DW, Rosenthal G, Schouten J, Shutter L, Timmons SD, Ullman JS, Videtta W, Wilberger JE, Wright DW. Guidelines for the management of severe traumatic brain injury. X. Brain oxygen monitoring and thresholds. J Neurotrauma. 2007;24(Suppl 1):S65–70.
Bratton SL, Chestnut RM, Ghajar J, McConnell Hammond FF, Harris OA, Hartl R, Manley GT, Nemecek A, Newell DW, Rosenthal G, Schouten J, Shutter L, Timmons SD, Ullman JS, Videtta W, Wilberger JE, Wright DW. Guidelines for the management of severe traumatic brain injury. Ix. Cerebral perfusion thresholds. J Neurotrauma. 2007;24(Suppl 1):S59–64.
Chen RY, Chien S. Hemodynamic functions and blood viscosity in surface hypothermia. Am J Physiol. 1978;235:H136–43.
Polderman KH, Peerdeman SM, Girbes AR. Hypophosphatemia and hypomagnesemia induced by cooling in patients with severe head injury. J Neurosurg. 2001;94:697–705.
Koht A, Cane R, Cerullo LJ. Serum potassium levels during prolonged hypothermia. Intensive Care Med. 1983;9:275–7.
Szczesny G, Veihelmann A, Massberg S, Nolte D, Messmer K. Long-term anaesthesia using inhalatory isoflurane in different strains of mice-the haemodynamic effects. Lab Anim. 2004;38:64–9.
Sessler DI. Mild perioperative hypothermia. N Engl J Med. 1997;336:1730–7.
Xiong J, Kurz A, Sessler DI, Plattner O, Christensen R, Dechert M, Ikeda T. Isoflurane produces marked and nonlinear decreases in the vasoconstriction and shivering thresholds. Anesthesiology. 1996;85:240–5.
Bhatti MT. Orbital syndromes. Semin Neurol. 2007;27:269–87.
Acknowledgments
The authors would also like to thank Laura Morrison and Jennifer Hadway for their help in conducting the animal experiments. All work was performed in Lawson Health Research Institute.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflicts of Interest
None.
Funding
Lawson Health Research Institute.
Rights and permissions
About this article

Cite this article
Fazel Bakhsheshi, M., Stewart, E.E., Tai, J.H. et al. Efficacy of Selective Brain Cooling Using a Nasopharyngeal Method in Piglets. Neurocrit Care 24, 140–149 (2016). https://doi.org/10.1007/s12028-015-0195-9
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12028-015-0195-9