
Abstract
Iodine is essential for normal thyroid function, supporting healthy fetal and child development. The relevance between maternal iodine nutrition status and pregnancy outcomes remains controversial. The aim was to explore whether urinary iodine concentrations (UIC)/urinary creatinine (UCr) was associated with thyroid function and adverse pregnancy outcomes. This study was performed in the Department of Endocrinology and Metabolism of the First Affiliated Hospital of Nanjing Medical University. A total of 212 pregnant women were enrolled from May 2018 to November 2021, from the first visit until postpartum. Maternal serum samples were obtained in the second half of pregnancy, and then thyroid-stimulating hormone (TSH), free thyroxine (FT4), free triiodothyronine (FT3), UIC, and UCr were tested. The correlation of UIC/UCr, which represented maternal iodine nutrition status, with TSH, FT4, and FT3 was studied using linear regression. And we assessed associations between UIC/UCr and pregnancy outcomes. Notably, we explored consistency between UIC/UCr and the incidence of low birth weight (LBW) by application of logistic regression analysis. A total of 212 women were divided into 3 groups according to the upper and lower quartiles of UIC/UCr. There were 53 women in group 1 (UIC/UCr < 106.96 ug/g), 106 women in group 2 (UIC/UCr 106.96–259.08 ug/g), and 53 women in group 3 (UIC/UCr > 259.08 ug/g). The level of UIC/UCr had a negative correlation with FT4 (r = − 0.139, p = 0.043) but a positive correlation with TSH (r = 0.096, p = 0.162 > 0.05). There was a significant difference in the incidence of LBW among the 3 groups (p = 0.007). Logistic regression analysis found that the level of UIC/UCr was an independent factor for LBW (p = 0.048, OR = 0.991, 95%CI (0.982, 0.999)). The receiver operating characteristic (ROC) curve showed that the area under the curve (AUC) for UIC/UCr predicting the incidence of low birth weight was 0.687 (p = 0.013, 95%CI 0.575, 0.799). Lower UIC/UCr during pregnancy was associated with higher FT4 and lower TSH. And iodine deficiency during pregnancy is a risk factor for low birth weight. Our findings indicated that more attention should be paid to the appropriate iodine nutrition status in pregnant women, which can help prevent suffering from adverse pregnancy outcomes.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Iodine is essential for synthesizing triiodothyronine (T3) and thyroxine (T4). During pregnancy, there is an increased demand for maternal thyroid hormone because of the placental transport of thyroid hormone to the fetus, an increase in thyroxine-binding globulin concentrations, increased renal clearance, and a higher degradation of thyroid hormone due to placental type III iodothyronine deiodinase [1]. Therefore, pregnant women were recommended to consume approximately 250 µg per day of iodine by the World Health Organization (WHO) in order to avoid iodine deficiency and detrimental consequences [1]. WHO proposed UIC as an essential reference index, and a median UIC of less than 150 ug/L in pregnant women was defined as iodine deficiency. Nevertheless, as an indicator of iodine nutrition status during pregnancy, UIC varies under the influence of multiple factors, including hydration and urine volume; the latest study figured out that UIC/UCr (ug/g) was superior to UIC (ug/L) [2].
Too low or too high iodine intake may negatively influence thyroid function, though the conjunction between iodine condition and thyroid function remains contentious. Some studies found that a higher level of UIC was correlated with higher thyroid stimulating hormone (TSH) and lower free thyroxine (FT4) [3,4,5]. In a study in Swedish [4], UIC and thyroid function have a negative correlation at a median gestational age of 10 weeks, and the UIC/UCr was below 150 μg/g in 80.1% of women. A similar finding was made in Israeli in early pregnancy; it was found that 85% of pregnant women had UIC levels below the adequacy range, with a median of 61 µg/L. However, it was reported that iodine status does not impact thyroid function [6]. The inconsistency is related partly to iodine status in each country, reflecting on maternal iodine reserve, nutrition iodine consumption, and compliance with iodine supplementation.
Whether iodine nutrition status itself could lead to adverse pregnancy outcomes was still controversial. Some research observed that iodine deficiency in pregnant women significantly increased the risk of preterm birth, fetal growth restriction (FGR) or low birthweight (LBW), and so on [7,8,9,10]. However, others reported that iodine nutrition status had little effect on adverse pregnancy outcomes [11,12,13]. All these studies did not consider thyroid hormones, neglecting the potential role of thyroid hormones in the effect of iodine nutrition status on pregnancy outcomes.
Most studies have focused on thyroid function and UIC in early pregnancy. We describe the relationship between iodine nutrition status and thyroid function in the second half of pregnancy and further describe its effect on pregnancy outcome. The main aims of this article were to explore whether iodine nutrition status is correlated to thyroid function in the second half of pregnancy and further analyze the relationship between iodine nutrition status and pregnancy outcome.
Methods
Participants
A total of 298 pregnant women were recruited in the second half of the pregnancy (mainly between 18 and 32 gestational weeks), some of whom were excluded due to thyroid dysfunction (43 subhypothyroidisms, 3 hypothyroidisms, 20 hyperthyroidisms, 6 hyperthyroidisms, and 14 isolated hypothyroinemias). A total of 212 pregnant women were enrolled. All women involved were admitted and gave birth in the First Affiliated Hospital of Nanjing Medical University from May 2018 to November 2021. Inclusion criteria were singleton pregnancy, age of at least 18 years, and normal thyroid function. Exclusion criteria included tumors, autoimmune diseases (such as systemic lupus erythematosus, sicca syndrome, or antiphospholipid antibody syndrome), and heart, liver, and kidney diseases known to affect iodine nutrition status. At baseline, participants’ height, weight, gestational age, and parity were recorded. The oral glucose tolerance test (OGTT) was conducted between 24 and 28 weeks, covering fasting blood glucose (FBG), 1-h post-load blood glucose (PBG-1 h), and 2-h post-load blood glucose (PBG-2 h). Thyroid function parameters, including TSH, FT4, thyroid peroxidase antibody (TPOAb), and iodine nutrition parameters, including urinary iodine and urinary creatinine concentration, were tested at recruitment. All the participants were followed up until delivery. Obstetric outcomes include the mode of birth, preterm birth, low birth weight (LBW), gestational diabetes mellitus (GDM), preeclampsia, and low Apgar scores at 1 and 5 min. We matched each pregnant woman with adverse pregnancy outcomes to two women with non-adverse outcomes based on age (± 2 years) and BMI (± 0.3 kg/m^2).
Sample Collection
Venous blood and urine samples were collected after 8 h fast to measure maternal thyroid function, UIC, and UCr at baseline.
Laboratory Measurements
TSH, free triiodothyronine (FT3), FT4, and TPOAb were measured by chemiluminescence immunoassay (Roche Cobas 6000, ZB/GEM1815-2010, Mannheim, Switzerland). Urinary iodine was determined by using arsenic-cerium-catalyzed spectrophotometry. Urinary creatinine concentration was determined by spectrophotometry.
Reference Scope and Definition of Some Pregnancy-Related Disorders
According to Guidelines for the Diagnosis and Management of Thyroid Diseases in Pregnancy and Postpartum issued by the American Thyroid Association (ATA) in 2017 and Guidelines for Diagnosis and Treatment of Thyroid Diseases in Pregnancy and Postpartum in China, the reference intervals of thyroid function during pregnancy are as follows: 0.45–4.32 mU/L for TSH, 9.77–18.89 pmol/L for FT4 at the second trimester and 0.30–4.98 mU/L for TSH, 9.04–15.22 pmol/L for FT4 at third trimester [14]. The titer of TPOAb > 34 IU/mL was considered to be positive. UIC/UCr was used to evaluate the iodine nutrition status of pregnant women, and pregnant women were divided into 3 groups based on the 25th percentile and 75th percentile of UIC/UCr. There were 53 women in group1 (UIC/UCr < 106.96 ug/g), 106 women in group 2 (106.96 ≤ UIC/UCr < 259.08 ug/g), and 53 women in group 3 (UIC/UCr ≥ 259.08 ug/g). We also used UIC as a grouping criterion according to the WHO criteria of deficiency (less than 150 μg/L), adequate (150–249 μg/L), more than adequate (250–449 μg/L), and excessive (more than 500 μg/L) in pregnant women.
Premature rupture of membranes (PROM) is defined as the rupture of the amniotic sac before the onset of labor. Preterm birth was defined as the birth of a baby at fewer than 37 weeks gestation, excluding iatrogenic preterm birth caused by preeclampsia, placenta previa, fetal growth restriction, and other factors. Low birth weight was defined as a live birth smaller than 2500 g. The definition of fetal macrosomia was birth weight greater than 4000 g, irrespective of gestational age.
Statistical Analysis
Statistical analyses were performed using R. The median and interquartile range (IQR) were used for the statistical analysis of the baseline characteristics with a non-normal distribution, Kruskal–Wallis H statistical method was used for comparison between multiple groups, and chi‐square for categorical variables. Spearman correlation analysis was used to determine the correlation between UIC, UIC/UCr, and thyroid function. The correlation heat map is presented using Origin. The linear model between UIC/UCr and thyroid function was analyzed by R language visualization (ggplot2). We matched each pregnant woman with LBW to two women without LBW based on age (± 2 years) and BMI (± 0.3 kg/m^2). The multivariate logistic regression model was used to evaluate the relationship between different iodine nutrition statuses and adverse pregnancy outcomes. Single-factor analysis of the forest map was performed using GraphPad Prism 8. Covariates (for example, TSH, FT4, FT3, FBG, PBG-1 h, and PBG-2 h) were controlled in the adjusting model. A P‐value of < 0.05 was considered statistically significant. The performance of UIC/UCr in LBW was analyzed by the ROC curve.
Results
Characteristics of Pregnant Women in Different Groups
Tables 1 and 2 show participants’ characteristics among three groups, including but not limited to maternal age, height, weight, BMI, SBP, and DBP. Data were available for 212 participants after exclusions. The mean maternal age at recruitment was 29 years. UIC/UCr had an overall mean of 208.22 µg/g and a median of 180.36 µg/g. The mean of UIC was 186.95 µg/L, and the median was 200 µg/L.
Correlation Between Blood Glucose, Thyroid Function, and UIC/UCr
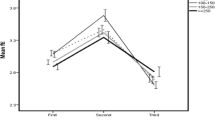
There was a trend toward an association of a lower UIC/UCr with a higher FT4 (P = 0.043), FT3 (P = 0.319), and a lower TSH (P = 0.162) (Figs. 1 and 2). There was no association of UIC with FT4 (P = 0.685), FT3 (P = 0.928), and TSH (P = 0.660).

Pearman’s correlation matrix of serum thyroid function, blood glucose and iodine nutrition status

The correlation between UIC/UCr and TSH, FT3, and FT4
UIC/UCr has a positive trend but did not reach statistical significance with TSH (r = 0.096, p = 0.162) and negatively with FT3 (r = − 0.069, p = 0.319) and FT4 (r = − 0.139, p = 0.043).
Pregnancy Outcomes in Different Iodine Nutrition Status Groups
Except for LBW (p = 0.007) and PROM (p = 0.03), we observed no statistical difference among UIC/Ucr groups in other pregnancy-related complications and adverse outcomes (Table 3). We found that the low UIC/UCr may increase the incidence of LBW. In addition to this, when grouped by UIC, the incidence of pregnancy-related adverse outcomes did not differ significantly among groups (Table 4).
Univariate Analysis and Multivariate Regression Analysis of LBW
Consequently, we further investigated the associations between LBW and UIC/UCr. In order to better control the impact of confounders, we matched each pregnant woman with LBW to two women without LBW based on age (± 2 years) and BMI (± 0.3). Logistic regression analysis was performed in Fig. 3 and found that higher UIC/UCr (p = 0.028) as well as TSH (p = 0.022) could significantly reduce the occurrence of LBW. After adjusting covariates, including blood glucose, FT4, and FT3, the ORs were still significant. It was found that UIC/UCr was an independent factor for LBW (p = 0.033, OR = 0.991, 95%CI (0.983, 0.999)) (Table 5). The ROC curve showed that the AUC for UIC/UCr predicting the incidence of LBW was 0.687 (p = 0.013, 95%CI 0.575, 0.799) (Fig. 4). The optimal cut-off point of UIC/Ucr for the risk of LBW was 200.645 ug/g. The risk of low birth weight was higher when the maternal UIC/UCr was less than the cut-off point.

Univariate analysis of LBW

ROC curves for UIC/UCr in predicting LBW
Discussion
Iodine nutrition status has aroused broad public concern, especially in vulnerable populations such as pregnant women. Maternal iodine nutrition status affects maternal thyroid function and plays a vital role in fetal development and adult health. In our study population, UIC/UCr had an overall mean of 208.22 µg/g and a median of 180.36 µg/g. The mean of UIC was 186.95 µg/L, and a median of 180.36 µg/g. and the median was 200 µg/L. The population with UIC/UCr in the first quantile accounted for 25% of the total population, while the population with UIC < 150 ug accounted for 39%. Interestingly, pregnancy outcomes in the UIC group according to WHO criteria were not statistically significant, whereas the association between UIC/UCr and the incidence of low birth weight infants was statistically significant.
It was found in this study that lower UIC/UCr was associated with higher FT4 and lower TSH. As is well known, severe iodine deficiency can lead to hypothyroidism, but mild-to-moderate iodine deficiency does not. In fact, an elevated TSH is rarely observed in populations that have mild-to-moderate iodine deficiency [3]. One of the autoregulatory responses of a normal thyroid gland to low iodine concentrations is a preferential secretion of T3 over T4. As a consequence, the pregnant women were hypothyroxinemic, corresponding to iodine deficiency, but they were clinically and biochemically euthyroid before their circulating T3 concentration was decreased. In addition, lower UIC/UCr might be associated with an increased risk of autonomous production of thyroid hormone by nodules/multinodular goiters, which resulted in lower TSH [15]. In the current study, UIC/UCr was negatively correlated with FT4, which might be due to a rapid short-term increase in iodine intake during pregnancy via the Wolff–Chaikoff effect. Just as Abel [5] et al. suggested that pregnant women with increased iodine intake due to mild to moderate iodine deficiency were more prone to having lower FT4 concentrations and higher TSH concentrations. Moreover, a cross-sectional study investigated that excessive iodine intake during pregnancy may lead to thyroid hypofunction [16]. Maria Andersson et al. also investigated that both iodine intake levels below or above the recommended interval would lead to an increased risk of thyroid disease in the population; the optimal interval of iodine intake was narrow [17].
Maternal iodine deficiency has a long-term adverse impact on fetal growth and development, especially in the nervous system [18]. However, its short-term effect on pregnancy outcomes remains controversial. We found that low UIC/UCr during pregnancy is a risk factor for low birth weight. Some previous studies documented that iodine insufficiency might negatively influence birth weight and fetal growth, thus making it more likely to develop FGR and SGA. Just as Chen et al. [19] in China found maternal iodine deficiency can affect fetal growth and development, which was assessed by head circumference, femur length, and body weight, on the contrary, a birth cohort[11]in three cities of Britain revealed that the UIC/UCr or UIC was irrelevant to fetal birth weight. These conflicting results might be attributed to populations with various degrees of iodine deficiency and the different stages of UIC/UCr detection during pregnancy. Despite that how maternal iodine nutrition status regulated fetal growth remained unsolved, the role of impaired placental function, which was closely related to the fetus’s development, was thoroughly emphasized [20, 21]. A study on iodine status, thyroid function, and birth weight indicated that iodine concentration in amniotic fluid was negatively correlated with UIC and birth weight [22], suggesting that maternal iodine deficiency disturbs the intrauterine environment, which in turn indirectly affects fetal growth and development. Moreover, maternal iodine nutrition status affected the production of thyroid hormones, which provides the thyroid hormones required by the fetus in the first trimester, regarded as an essential window of narrow variations in maternal thyroid parameters [23]. However, iodine nutrition status is also critical in latter pregnancy, as it affects thyroid hormone synthesis in both maternal and fetal. The optimal cut-off point of UIC/Ucr for the risk of LBW was 200.645 ug/g, which means the risk of low birth weight was higher when the maternal UIC/UCr was less than the cut-off point. So, we recommend that attention should be paid to iodine supplementation during pregnancy. Evidence about the effects of iodine deficiency on other pregnancy outcomes like preterm birth (PTB), preeclampsia, etc. and the potential mechanism involved was still limited and fixed. In our study, premature rupture of membranes was found to be seem related to iodine nutrition status, which was rarely mentioned in other studies. We think that the influence of iodine nutrition status on the intrauterine environment may lead to this outcome. The specific mechanism may need to be confirmed by further animal experiments, and we will pay more attention to this outcome in the following studies.
Few studies have analyzed thyroid function when discussing the effects of UIC or UIC/UCr on pregnancy outcomes. In this study, all the participants revealed relatively normal thyroid function. After adjusting for covariates, TSH as well as UIC/UCr was found to be negatively associated with the incidence of LBW. A Chinese cohort study [24] proposed that compared with normal subjects (0.1 ≤ TSH < 2.5 mIU/L), those with TSH concentrations of 2.5–4.0 mIU/L had a 0.65-fold lower risk of LBW, consistent with our findings that lower TSH within the normal range may be a risk factor for LBW. A previous study had shown low FT4 levels during early pregnancy that remained low in late pregnancy were associated with higher birth weight and a 40% elevated probability of LGA [25]. Our study shows a trend toward an association of higher FT4 with increasing LBW, but this association did not reach statistical significance. The possible mechanisms for this are that a shortage of maternal thyroid hormones can greatly affect fetal growth because they are an essential supplier of fetal thyroid hormones, and thyroid hormone concentrations play a critical role in the catabolic and anabolic processes of glucose, protein, and fat. Additionally, thyroid hormones might directly regulate the secretion and sensitivity of insulin.
We consider that the iodine nutrition status of pregnant women may affect the health of the mother and fetus to some extent, so this exploration has great significance for the development of human health. We were able to study the association of iodine nutrition status with thyroid function and pregnancy outcomes and adjust a large number of potential confounding variables. We use UIC/UCr, which has been shown to be more accurate than UIC, to assess iodine nutrition status. Limitations for interpreting the results of the current study include that we do not quantitative analysis of autoimmune antibodies, which may affect thyroid function and pregnancy outcomes, and we are refining the data in future work. And we will expand the study population in future surveys. Moreover, the cross-sectional design of this study limits causal inference, and we will plan a longitudinal design to explore further. It is hoped that in future studies, more people will pay attention to the effects of iodine nutrition status during pregnancy on neonatal thyroid function and subsequent neurological development, which will have great guiding significance for perinatal health care.
Conclusions
In conclusion, lower UIC/UCr during pregnancy was associated with higher FT4, lower TSH, and a higher risk for LBW. In clinical practice, we need to recognize that iodine deficiency can affect thyroid function in normal pregnant women. More attention should be paid to the association between iodine deficiency and adverse pregnancy outcomes.
Data Availability
The data of this study are available from the corresponding author upon request.
References
Alexander EK, Pearce EN, Brent GA, Brown RS, Chen H, Dosiou C, Grobman WA, Laurberg P, Lazarus JH, Mandel SJ et al (2017) 2017 Guidelines of the American Thyroid Association for the Diagnosis and Management of Thyroid Disease During Pregnancy and the Postpartum. Thyroid 27(3):315–389
Li C, Peng S, Zhang X, Xie X, Wang D, Mao J, Teng X, Shan Z, Teng W (2016) The urine iodine to creatinine as an optimal index of iodine during pregnancy in an iodine adequate area in China. J Clin Endocrinol Metab 101(3):1290–1298
Næss S, Markhus MW, Strand TA, Kjellevold M, Dahl L, Stokland AM, Nedrebø BG, Aakre I (2021) Iodine nutrition and iodine supplement initiation in association with thyroid function in mildly-to-moderately iodine-deficient pregnant and postpartum women. J Nutr 151(10):3187–3196
Levie D, Derakhshan A, Shu H, Broeren M, de Poortere RA, Peeters RP, Bornehag CG, Demeneix B, Korevaar T (2019) The association of maternal iodine status in early pregnancy with thyroid function in the Swedish Environmental Longitudinal, Mother and Child Asthma and Allergy Study. Thyroid 29(11):1660–1668
Abel MH, Korevaar T, Erlund I, Villanger GD, Caspersen IH, Arohonka P, Alexander J, Meltzer HM, Brantsæter AL (2018) Iodine intake is associated with thyroid function in mild to moderately iodine deficient pregnant women. Thyroid 28(10):1359–1371
Schiller T, Agmon A, Ostrovsky V, Shefer G, Knobler H, Zornitzki T (2020) Moderate iodine deficiency is common in pregnancy but does not alter maternal and neonatal thyroid function tests. Front Endocrinol (Lausanne) 11:523319
Charoenratana C, Leelapat P, Traisrisilp K, Tongsong T (2016) Maternal iodine insufficiency and adverse pregnancy outcomes. Matern Child Nutr 12(4):680–687
Snart C, Threapleton DE, Keeble C, Taylor E, Waiblinger D, Reid S, Alwan NA, Mason D, Azad R, Cade JE et al (2020) Maternal iodine status, intrauterine growth, birth outcomes and congenital anomalies in a UK birth cohort. BMC Med 18(1):132
Nazarpour S, Ramezani TF, Amiri M, Simbar M, Tohidi M, Bidhendi YR, Azizi F (2020) Maternal urinary iodine concentration and pregnancy outcomes: Tehran thyroid and pregnancy study. Biol Trace Elem Res 194(2):348–359
Abel MH, Caspersen IH, Sengpiel V, Jacobsson B, Meltzer HM, Magnus P, Alexander J, Brantsæter AL (2020) Insufficient maternal iodine intake is associated with subfecundity, reduced foetal growth, and adverse pregnancy outcomes in the Norwegian mother, father and child cohort study. BMC Med 18(1):211
Snart C, Keeble C, Taylor E, Cade JE, Stewart PM, Zimmermann M, Reid S, Threapleton DE, Poston L, Myers JE et al (2019) Maternal iodine status and associations with birth outcomes in three major cities in the United Kingdom. Nutrients 11(2)
León G, Murcia M, Rebagliato M, Álvarez-Pedrerol M, Castilla AM, Basterrechea M, Iñiguez C, Fernández-Somoano A, Blarduni E, Foradada CM et al (2015) Maternal thyroid dysfunction during gestation, preterm delivery, and birthweight. The Infancia y Medio Ambiente Cohort, Spain. Paediatr Perinat Epidemiol 29(2):113–122
Torlinska B, Bath SC, Janjua A, Boelaert K, Chan SY (2018) Iodine status during pregnancy in a region of mild-to-moderate iodine deficiency is not associated with adverse obstetric outcomes; results from the Avon Longitudinal Study of Parents and Children (ALSPAC). Nutrients 10(3)
Liu J, Yu X, Xia M, Cai H, Cheng G, Wu L, Li Q, Zhang Y, Sheng M, Liu Y et al (2017) Development of gestation-specific reference intervals for thyroid hormones in normal pregnant Northeast Chinese women: what is the rational division of gestation stages for establishing reference intervals for pregnancy women? Clin Biochem 50(6):309–317
Carlé A, Krejbjerg A, Laurberg P (2014) Epidemiology of nodular goitre. Influence of iodine intake. Best Pract Res Clin Endocrinol Metab 28(4):465–479
Shi X, Han C, Li C, Mao J, Wang W, Xie X, Li C, Xu B, Meng T, Du J et al (2015) Optimal and safe upper limits of iodine intake for early pregnancy in iodine-sufficient regions: a cross-sectional study of 7190 pregnant women in China. J Clin Endocrinol Metab 100(4):1630–1638
Andersson M, Braegger CP (2022) The role of iodine for thyroid function in lactating women and infants. Endocr Rev 43(3):469–506
Mulder TA, Korevaar T, Peeters RP, van Herwaarden AE, de Rijke YB, White T, Tiemeier H (2021) Urinary iodine concentrations in pregnant women and offspring brain morphology. Thyroid 31(6):964–972
Chen R, Li Q, Cui W, Wang X, Gao Q, Zhong C, Sun G, Chen X, Xiong G, Yang X et al (2018) Maternal iodine insufficiency and excess are associated with adverse effects on fetal growth: a prospective cohort study in Wuhan, China. J Nutr 148(11):1814–1820
Sun Y, Han Y, Qian M, Li Y, Ye Y, Lin L, Liu Y (2021) Defending effects of iodide transfer in placental barrier against maternal iodine deficiency. Thyroid 31(3):509–518
Habibi N, Grieger JA, Bianco-Miotto T (2020) A review of the potential interaction of selenium and iodine on placental and child health. Nutrients 12(9)
Velasco I, Sánchez-Gila M, Manzanares S, Taylor P, García-Fuentes E (2020) Iodine status, thyroid function, and birthweight: a complex relationship in high-risk pregnancies. J Clin Med 9(1)
Eastman CJ, Ma G, Li M (2019) Optimal assessment and quantification of iodine nutrition in pregnancy and lactation: laboratory and clinical methods, controversies and future directions. Nutrients 11(10)
Chen GD, Pang TT, Lu XF, Li PS, Zhou ZX, Ye SX, Yang J, Shen XY, Lin DX, Fan DZ et al (2020) Associations between maternal thyroid function and birth outcomes in Chinese mother-child dyads: a retrospective cohort study. Front Endocrinol (Lausanne) 11:611071
Zhang C, Yang X, Zhang Y, Guo F, Yang S, Peeters RP, Korevaar T, Fan J, Huang HF (2019) Association between maternal thyroid hormones and birth weight at early and late pregnancy. J Clin Endocrinol Metab 104(12):5853–5863
Author information
Authors and Affiliations
Contributions
All authors contributed to the study conception and design. Material preparation, data collection and analysis were performed by Hongying Zha, Lin Yu, Yi Tang and Lu Sun. The first draft of the manuscript was written by Hongying Zha and Lin Yu, and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Competing Interests
The authors declare no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Hongying Zha and Lin Yu are contributed equally to this work.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Zha, H., Yu, L., Tang, Y. et al. Effect of Iodine Nutrition Status on Thyroid Function and Pregnancy Outcomes. Biol Trace Elem Res 201, 5143–5151 (2023). https://doi.org/10.1007/s12011-023-03600-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12011-023-03600-8