
Abstract
Cadmium is a heavy metal that has been suggested to be a carcinogen by evidence. A number of published studies have investigated the association between cadmium levels and prostate cancer, but the results were inconsistent. Thus, we conducted a meta-analysis to get a precise estimate of this subject. After a careful searching and screening, a total of 11 publications containing 14 separated studies were included. Based on a random-effect model, the pooled data showed that cadmium levels of prostate tissues (standard mean difference (SMD) = 3.17, 95 % confidence interval (CI) = 0.60–5.74, P < 0.05) and plasma (SMD = 4.07, 95 % CI = 2.01–6.13, P < 0.05) were significantly higher in prostate cancer patients than those in the healthy controls. No difference of hair and nail cadmium levels between the prostate cancer cases and the controls was found. The data suggested that cadmium exposure might exert an influence on the tumorigenesis of prostate tissues. Future investigations with large sample sizes are needed to verify the results.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Prostate cancer is the most common cancer that is the sixth cause of cancer death in men in the world [1]. However, its risk factors remain unclear. Previously, epidemic factors such as smoking and alcohol consumption are believed to be risk factors for prostate cancer [2]. Besides, sexually transmitted infections [1], genetic variations [3], and even excess fatness [4] might also confer prostate cancer risk. Recently, dietary factors have been suggested to play a role in the genesis of prostate carcinoma [5]. For example, low-carbohydrate intake, soy protein, omega-3 (w-3) fat, green teas, tomatoes and tomato products, and zyflamend might reduce prostate cancer risk, and conversely, a higher saturated fat intake or a higher β-carotene status might increase carcinoma risk [6]. As we know, the dietary factors may influence the levels of trace elements such as selenium, zinc, arsenic, cadmium, and nickel in tissues or serums, which might exert an effect on cancer risk [7].
For prostate cancer, recent meta-analyses revealed that decreased zinc levels in prostate tissue may have an association with increased cancer risk [8]. Besides, increasing plasma/serum selenium may be related to a decreased prostate cancer risk [9]. Nevertheless, few meta-analyses on the association between other element levels and prostate carcinoma have been published.
Cadmium is a human neoplastic heavy metal that is usually taken up from vegetables and grains developed in contaminated soil. Once absorbed, it can bind to metallothionein and is stored in the tissues of solid organs such as kidney because the mechanisms for the excretion of this heavy metal from the body are absent [10]. The long biological half-life of cadmium in humans could lead to malignant transformation of tissues via multiple pathways [11]. Thus, cadmium accumulation in the body is thought to have a correlation with risk of a variety of cancers, such as bladder cancer [12], pancreatic cancer [13], and lung cancer [14].
A number of studies have been devoted to the cadmium levels and prostate cancer risk. However, the results were inconsistent and conflicting. To our knowledge, few meta-analyses on this topic have been published to date. Thus, in the present study, we aimed to conduct a quantitative meta-analysis containing published data up to Sep. 2015 that increased statistical power to obtain a conclusive estimation.
Materials and Methods
Literature Search Strategy
A systematic search was carried out in multiple bibliographic databases such as Medline, EMBASE, and China National Knowledge Infrastructure (CNKI) without a language limitation, including all papers published up to Sep. 2015. In the initial search, a combination of the following keywords was used: cadmium, trace element, neoplasm, tumor, cancer, prostate, and urinary system. Other possible publications were screened by checking the references of the retrieved papers.
Inclusion Criteria
The following criteria were used for the literature selection: first, studies focused on the levels of cadmium in the bodies of patients with prostate carcinoma; second, papers must offer both exposed group and control group; and third, studies must offer the size of sample, the mean, and standard deviation (SD) of cadmium level or necessary information that readers can infer the results. Accordingly, the exclusion criteria were used as follows: first, papers showed insufficient information about cadmium levels; second, studies only concerned animal experiments or cell line cultures; and third, reviews or duplicate publications. After rigorous searching, we reviewed all papers according to the criteria mentioned above for further analysis.
Data Extraction and Quality Assessment
Eligible publications were independently reviewed by two of the authors according to the inclusion criteria. Data were extracted and illustrated in a database. For discrepancies of the data, a discussion was made in order to reach an agreement. On the basis of this situation, if a conflicting evaluation still existed, another author was consulted to resolve the dispute and then a final decision was made by the majority of the votes.
The Newcastle-Ottawa Scale (NOS) was used to assess the quality of the studies, which ranges from 0 to 9 stars [15]. Studies with less than 4 stars were excluded.
Statistical Analysis
The SMDs and the corresponding 95 % CIs were used to compare the cadmium levels between patients with prostate carcinoma and controls. Heterogeneity testing was evaluated with a chi-square-based Q statistic test. If a P value for a given Q test was found to be more than 0.1, ORs were pooled according to a fixed-effect model (Mantel-Haenszel) [16]. Otherwise, a random-effect model (DerSimonian and Laird) was selected [17]. A funnel plot was constructed to assess the publication bias via visual inspection of the plot [18]. An asymmetrical plot indicated possible publication bias. Then, Egger’s linear regression test was used to further evaluate symmetry of the funnel plot [19]. Statistical analysis was carried out using the program STATA 11.0 software (Stata Corporation, TX, USA).
Results
Study Characteristics
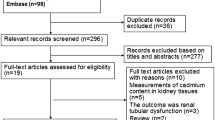
Possible publications relevant to the keywords were retrieved and screened. A total of 241 publications were primarily obtained, of which 212 irrelevant papers were excluded. Thus, 29 publications were eligible. After a careful review of the paper contents, three review articles [20–22] and four studies without healthy control group [23–26] were excluded. Then, 11 publications providing insufficient information [27–37] were further excluded. Lastly, 11 publications including 14 separated studies were selected for data extraction [38–47] (Fig. 1).

The flow diagram of included/excluded studies
The NOS scores of all studies were greater than four, and thus, they were all included. Among the selected publications, only two was written in Chinese [38, 48], while the remaining nine were in English. The relevant information was listed in Table 1. As shown in this table, the first author and the number of cases and controls for each study were presented. The mean levels of cadmium and their standard deviations as well as other necessary information such as detection method and countries were also included. There were six studies that focused on prostate tissue, four on plasma, two on hair, and two on nail. A total of three methods for detecting cadmium levels were used, namely, flame atomic absorption spectrophotometry (AAS), flameless AAS, and graphite furnace AAS.
Meta-Analysis Results
Main results of the meta-analysis were shown in Table 2. The overall data from 14 studies were pooled in a random-effect model because significant heterogeneity was found among the studies (Q = 619.71, P < 0.05). The comparison of cadmium levels between prostate cancer cases and healthy controls showed that cadmium levels in prostate cancer patients were markedly higher than those in the controls (SMD = 3.19, 95 % CI = 1.94–4.45, P < 0.05).
When the data were stratified by sample types, significant differences were observed in the subgroups regarding prostate tissue (SMD = 3.17, 95 % CI = 0.60–5.74, P < 0.05) and plasma (SMD = 4.07, 95 % CI = 2.01–6.13, P < 0.05), demonstrating that levels of cadmium in prostate tissue and plasma are higher in prostate cancer cases than those in the controls, respectively. No difference could be found in the subgroups regarding hair (SMD = 2.38, 95 % CI = −2.18–6.95, P > 0.05) and nail (SMD = 3.16, 95 % CI = −3.09–9.40, P > 0.05), respectively (Fig. 2).

The association of prostate cancer risk with cadmium levels (prostate cancer cases versus controls; stratified by sample type). Forest plots showed that cadmium levels of prostate tissues and plasma in prostate cancer cases were higher than those in the controls. No differences were found in the comparisons regarding hair and nail
In the subgroup analysis about geographical location, significant differences were also shown in all groups except the Africa group (SMD = 30.19, 95 % CI = −4.02–64.40, P > 0.05). As shown in Table 1, there were a total of ten studies that provided information about the mean age for the cases and controls, and thus, these studies were stratified by age. Since the mean ages of the cases ranged from 55.18 to 73.0 years, the studies were divided into two subgroups, namely, less than 65 years (<65) group and equal to or greater than 65 years (≧65) group, respectively. The results showed that the significance of the two subgroups (≧65 SMD = 4.42, 95 % CI = 2.29–6.55, P < 0.05; <65 SMD = 4.00, 95 % CI = 2.34–5.65, P < 0.05) were in accordance with the overall data, respectively, as presented in Table 2 and Fig. 3.

The association of prostate cancer risk with cadmium levels (prostate cancer cases versus controls; stratified by age). Forest plots showed that cadmium levels in prostate cancer cases of were not higher or lower than those in the controls for the two subgroups
Sensitivity analysis was used to evaluate the effect of a single study on the overall effect estimate by deleting any one study each time during repeated analysis. The results showed that the statistical significance of the results was not altered when any single study was omitted (data not shown), indicating the robustness of the results.
Bias Diagnostics
A funnel plot was created to detect possible publication bias. Then, Egger’s linear regression tests were performed to assess the symmetry of the plot. A potential publication bias might exist because Egger’s test suggested that the funnel plot was not symmetrical (t = 2.47, P = 0.03).
Discussion
In the present study, we compared the levels of cadmium in the bodies between prostate cancer patients and healthy controls by performing a meta-analysis and found that cadmium levels in prostate tissues and plasma of prostate cancer patients were significantly higher than those of healthy controls, respectively, indicating that cadmium accumulation in prostate tissue and plasma might be involved in the neoplastic process of prostate tissues.
As a heavy metal, cadmium has been suggested to be a pathogenic factor or a carcinogen for humans by several published meta-analyses. For instance, cadmium accumulation is responsible for hypertension, atherosclerosis, and acute coronary events [49]. Also, cadmium might influence the neurodevelopment and behavioral disorders in children [50]. Only a few meta-analyses reported the association of cadmium and cancer risk. In 2000, a meta-analysis showed that high exposure to cadmium may increase risk of pancreatic cancer [51]. Also, elevated levels of cadmium were found in breast cancer patients compared with those in the controls [52]. Nevertheless, environmental cadmium exposure at a low-level might be a risk factor for lung carcinoma [53]. Moreover, Larsson et al. suggested that cadmium, even at a low concentration, could increase mortality caused by cancer or non-cancer diseases [54]. The evidence supported the notion that cadmium exposure might be a pathogenic factor in a number of malignant disorders.
The underlying mechanisms by which cadmium initiates or assists cancerigenesis are not fully understood. Reports showed that exposure to cadmium at a low concentration could lead to DNA fragmentation [55] and microsatellite instability [56] in cells. Moreover, cadmium exposure could induce the secretion of tumor necrosis factor-alpha [57] that is a cytokine associated with a number of cancer risk [58]. Additionally, cadmium induces increase in reactive oxygen species formation, which in turn interferes with cell signaling and lastly induce DNA damage [59]. Thus, cancerigenesis of prostate tissues might be initiated. Notably, the cadmium levels in hair and nail between prostate cancer patients and controls are not significantly different. The data indicated a tendency that cadmium accumulated in organs and blood rather than skin appendages, consistent with a study by Bibi et al. [60] in which cadmium levels in hair and nail were low, though those in blood were high. Therefore, the skin appendages should be cautiously used to predict internal cadmium concentration [61].
As we know, cadmium might have a long half-life in the body owing to the absence of the mechanisms by which cadmium would be excreted out. Thus, the age and the cadmium concentration might be positively correlated. To address this topic, we conducted subgroup analysis on age. The data suggested that the age might not exert a marked influence on the overall results. However, in the present meta-analysis, all cancer cases with available mean ages were late-middle and aged men, while the controls were not well matched to the cases. Moreover, the mean ages of the cases and the controls were provided only in 10 out of 14 studies. Thus, the results should be interpreted with care. Future primary investigations covering wide age ranges are warranted to address this subject.
Significant heterogeneity was seen for the overall data, and thus, a random-effect model was used. We tried to stratify the data according to sample types and geographical locations, and however, heterogeneity still existed in each comparison, indicating that multiple factors such as study design, sample size, and lifestyle factors might lead to the heterogeneity. Nevertheless, sensitivity analysis suggested the robustness of the results. In the present study, evident publication bias was also shown for the overall data. However, it is worth noting that the number of the included studies was limited, which might result in the inaccuracy of the bias tests. On the basis of this situation, future well-designed studies comprising larger sample sizes are required to derive a precise estimate.
Several limitations might be included in this study. First, this study only involved data from articles published in Chinese and English. Thus, papers written in other languages were inevitably missed, and any selection bias must exist. Second, confounding factors, such as gender, smoking, and drinking, were not assessed in most of the included studies. Hence, it is difficult for us to conduct subgroup analyses on these factors, and the estimate for the comparison might deviate from the exactness. Third, the stages of prostate cancer were not considered and evaluated in most of the selected studies. Future investigations on this issue might help clarify the effect of cadmium on prostate cancer development.
In conclusion, the data of the present meta-analysis showed that cadmium levels in prostate tissues and plasma of prostate cancer patients were significantly higher than those of healthy controls, suggesting that cadmium exposure might exert an influence on the tumorigenesis of prostate tissues. Future investigations with large sample sizes are needed to verify the results.
References
Caini S, Gandini S, Dudas M, Bremer V, Severi E, Gherasim A (2014) Sexually transmitted infections and prostate cancer risk: a systematic review and meta-analysis. Cancer Epidemiol 38(4):329–338. doi:10.1016/j.canep.2014.06.002
Sawada N, Inoue M, Iwasaki M, Sasazuki S, Yamaji T, Shimazu T, Tsugane S (2014) Alcohol and smoking and subsequent risk of prostate cancer in Japanese men: the Japan Public Health Center-based prospective study. Int J Cancer 134(4):971–978. doi:10.1002/ijc.28423
Attard G, Parker C, Eeles RA, Schroder F, Tomlins SA, Tannock I, Drake CG, de Bono JS (2015) Prostate cancer. Lancet. doi:10.1016/S0140-6736(14)61947-4
Byers T, Sedjo RL (2015) Body fatness as a cause of cancer: epidemiologic clues to biologic mechanisms. Endocr Relat Cancer 22(3):R125–R134. doi:10.1530/ERC-14-0580
Labbe DP, Zadra G, Ebot EM, Mucci LA, Kantoff PW, Loda M, Brown M (2014) Role of diet in prostate cancer: the epigenetic link. Oncogene. doi:10.1038/onc.2014.422
Lin PH, Aronson W, Freedland SJ (2015) Nutrition, dietary interventions and prostate cancer: the latest evidence. BMC Med 13:3. doi:10.1186/s12916-014-0234-y
Navarro Silvera SA, Rohan TE (2007) Trace elements and cancer risk: a review of the epidemiologic evidence. Cancer Causes Control 18(1):7–27. doi:10.1007/s10552-006-0057-z
Gumulec J, Masarik M, Adam V, Eckschlager T, Provaznik I, Kizek R (2014) Serum and tissue zinc in epithelial malignancies: a meta-analysis. PLoS One 9(6), e99790. doi:10.1371/journal.pone.0099790
Hurst R, Hooper L, Norat T, Lau R, Aune D, Greenwood DC, Vieira R, Collings R, Harvey LJ, Sterne JA, Beynon R, Savovic J, Fairweather-Tait SJ (2012) Selenium and prostate cancer: systematic review and meta-analysis. Am J Clin Nutr 96(1):111–122. doi:10.3945/ajcn.111.033373
Fujishiro H, Yano Y, Takada Y, Tanihara M, Himeno S (2012) Roles of ZIP8, ZIP14, and DMT1 in transport of cadmium and manganese in mouse kidney proximal tubule cells. Metallomics Integr Biometal Sci 4(7):700–708. doi:10.1039/c2mt20024d
Koedrith P, Kim H, Weon JI, Seo YR (2013) Toxicogenomic approaches for understanding molecular mechanisms of heavy metal mutagenicity and carcinogenicity. Int J Hyg Environ Health 216(5):587–598. doi:10.1016/j.ijheh.2013.02.010
Feki-Tounsi M, Hamza-Chaffai A (2014) Cadmium as a possible cause of bladder cancer: a review of accumulated evidence. Environ Sci Pollut Res Int 21(18):10561–10573. doi:10.1007/s11356-014-2970-0
Luckett BG, Su LJ, Rood JC, Fontham ET (2012) Cadmium exposure and pancreatic cancer in south Louisiana. J Environ Public Health 2012:180186. doi:10.1155/2012/180186
Demir N, Turksoy VA, Kayaalti Z, Soylemezoglu T, Savas I (2014) The evaluation of arsenic and cadmium levels in biological samples of cases with lung cancer. Tuberkuloz ve toraks 62(3):191–198
Stang A (2010) Critical evaluation of the Newcastle-Ottawa Scale for the assessment of the quality of nonrandomized studies in meta-analyses. Eur J Epidemiol 25(9):603–605. doi:10.1007/s10654-010-9491-z
Mantel N, Haenszel W (1959) Statistical aspects of the analysis of data from retrospective studies of disease. J Natl Cancer Inst 22(4):719–748
DerSimonian R, Laird N (1986) Meta-analysis in clinical trials. Control Clin Trials 7(3):177–188
Munafo MR, Clark TG, Flint J (2004) Assessing publication bias in genetic association studies: evidence from a recent meta-analysis. Psychiatry Res 129(1):39–44. doi:10.1016/j.psychres.2004.06.011
Egger M, Davey Smith G, Schneider M, Minder C (1997) Bias in meta-analysis detected by a simple, graphical test. BMJ 315(7109):629–634
Luevano J, Damodaran C (2014) A review of molecular events of cadmium-induced carcinogenesis. J Environ Pathol Toxicol Oncol 33(3):183–194
Sahmoun AE, Case LD, Jackson SA, Schwartz GG (2005) Cadmium and prostate cancer: a critical epidemiologic analysis. Cancer Investig 23(3):256–263
Verougstraete V, Lison D, Hotz P (2003) Cadmium, lung and prostate cancer: a systematic review of recent epidemiological data. J Toxicol Environ Health B Crit Rev 6(3):227–255. doi:10.1080/10937400306465
Guzel S, Kiziler L, Aydemir B, Alici B, Ataus S, Aksu A, Durak H (2012) Association of Pb, Cd, and Se concentrations and oxidative damage-related markers in different grades of prostate carcinoma. Biol Trace Elem Res 145(1):23–32. doi:10.1007/s12011-011-9162-2
Lee JD, Wu SM, Lu LY, Yang YT, Jeng SY (2009) Cadmium concentration and metallothionein expression in prostate cancer and benign prostatic hyperplasia of humans. J Formos Med Assoc 108(7):554–559. doi:10.1016/s0929-6646(09)60373-9
Anetor JI, Ajose F, Anetor GO, Iyanda AA, Babalola OO, Adeniyi FA (2008) High cadmium/zinc ratio in cigarette smokers: potential implications as a biomarker of risk of prostate cancer. Niger J Phys Sci 23(1–2):41–49
Gray MA, Centeno JA, Slaney DP, Ejnik JW, Todorov T, Nacey JN (2005) Environmental exposure to trace elements and prostate cancer in three New Zealand ethnic groups. Int J Environ Res Public Health 2(3–4):374–384
Armstrong BG, Kazantzis G (1985) Prostatic cancer and chronic respiratory and renal disease in British cadmium workers: a case control study. Br J Ind Med 42(8):540–545
Bako G, Smith ES, Hanson J, Dewar R, Hill GB (1981) Cadmium and prostatic cancer in Alberta. Can Med Assoc J 124(2):121
Chen YC, Pu YS, Wu HC, Wu TT, Lai MK, Yang CY, Sung FC (2009) Cadmium burden and the risk and phenotype of prostate cancer. BMC Cancer 9:429. doi:10.1186/1471-2407-9-429
Elghany NA, Schumacher MC, Slattery ML, West DW, Lee JS (1990) Occupation, cadmium exposure, and prostate cancer. Epidemiology (Cambridge, Mass) 1(2):107–115
Eriksen KT, Halkjaer J, Meliker JR, McElroy JA, Sorensen M, Tjonneland A, Raaschou-Nielsen O (2015) Dietary cadmium intake and risk of prostate cancer: a Danish prospective cohort study. BMC Cancer 15:177. doi:10.1186/s12885-015-1153-9
Julin B, Wolk A, Johansson JE, Andersson SO, Andren O, Akesson A (2012) Dietary cadmium exposure and prostate cancer incidence: a population-based prospective cohort study. Br J Cancer 107(5):895–900. doi:10.1038/bjc.2012.311
Neslund-Dudas C, Mitra B, Kandegedara A, Chen D, Schmitt S, Shen M, Cui Q, Rybicki BA, Dou QP (2012) Association of metals and proteasome activity in erythrocytes of prostate cancer patients and controls. Biol Trace Elem Res 149(1):5–9. doi:10.1007/s12011-012-9391-z
Sarafanov AG, Todorov TI, Centeno JA, Macias V, Gao W, Liang WM, Beam C, Gray MA, Kajdacsy-Balla AA (2011) Prostate cancer outcome and tissue levels of metal ions. Prostate 71(11):1231–1238. doi:10.1002/pros.21339
Vinceti M, Venturelli M, Sighinolfi C, Trerotoli P, Bonvicini F, Ferrari A, Bianchi G, Serio G, Bergomi M, Vivoli G (2007) Case–control study of toenail cadmium and prostate cancer risk in Italy. Sci Total Environ 373(1):77–81. doi:10.1016/j.scitotenv.2006.11.005
West DW, Slattery ML, Robison LM, French TK, Mahoney AW (1991) Adult dietary intake and prostate cancer risk in Utah: a case–control study with special emphasis on aggressive tumors. Cancer Causes Control 2(2):85–94
van der Gulden JW, Kolk JJ, Verbeek AL (1995) Work environment and prostate cancer risk. Prostate 27(5):250–257
Ouyang S, Li S (2000) Investigation of trace elements in hair of patients with prostate carcinoma, benign prostatic hypertrophy, and normal controls. Bull Hunan Med Univ 25 (3)
Qayyum MA, Shah MH (2014) Comparative study of trace elements in blood, scalp hair and nails of prostate cancer patients in relation to healthy donors. Biol Trace Elem Res 162(1–3):46–57. doi:10.1007/s12011-014-0123-4
Platz EA, Helzlsouer KJ, Hoffman SC, Morris JS, Baskett CK, Comstock GW (2002) Prediagnostic toenail cadmium and zinc and subsequent prostate cancer risk. Prostate 52(4):288–296. doi:10.1002/pros.10115
Brys M, Nawrocka AD, Miekos E, Zydek C, Foksinski M, Barecki A, Krajewska WM (1997) Zinc and cadmium analysis in human prostate neoplasms. Biol Trace Elem Res 59(1–3):145–152
Feustel A, Wennrich R, Steiniger D, Klauss P (1982) Zinc and cadmium concentration in prostatic carcinoma of different histological grading in comparison to normal prostate tissue and adenofibromyomatosis (BPH). Urol Res 10(6):301–303
Feustel A, Wennrich R, Dittrich H (1987) Zinc, cadmium and selenium concentrations in separated epithelium and stroma from prostatic tissues of different histology. Urol Res 15(3):161–163
Lahtonen R (1985) Zinc and cadmium concentrations in whole tissue and in separated epithelium and stroma from human benign prostatic hypertrophic glands. Prostate 6(2):177–183
Ogunlewe JO, Osegbe DN (1989) Zinc and cadmium concentrations in indigenous blacks with normal, hypertrophic, and malignant prostate. Cancer 63(7):1388–1392
Feustel A, Wennrich R (1986) Zinc and cadmium plasma and erythrocyte levels in prostatic carcinoma, BPH, urological malignancies, and inflammations. Prostate 8(1):75–79
Habib FK, Hammond GL, Lee IR, Dawson JB, Mason MK, Smith PH, Stitch SR (1976) Metal-androgen interrelationships in carcinoma and hyperplasia of the human prostate. J Endocrinol 71(1):133–141
Chen G, Wu L, Wu Y, Zhu J (2015) Content change of zinc and cadmium in serum of patients with prostate cancer and its clinical significance. J Clin Urol (China) 30(5):439–441
Caciari T, Sancini A, Fioravanti M, Capozzella A, Casale T, Montuori L, Fiaschetti M, Schifano MP, Andreozzi G, Nardone N, Tomei G, Ciarrocca M, Rosati MV, Tomei F (2013) Cadmium and hypertension in exposed workers: a meta-analysis. Int J Occup Med Environ Health 26(3):440–456. doi:10.2478/s13382-013-0111-5
Rodriguez-Barranco M, Lacasana M, Aguilar-Garduno C, Alguacil J, Gil F, Gonzalez-Alzaga B, Rojas-Garcia A (2013) Association of arsenic, cadmium and manganese exposure with neurodevelopment and behavioural disorders in children: a systematic review and meta-analysis. Sci Total Environ 454–455:562–577. doi:10.1016/j.scitotenv.2013.03.047
Schwartz GG, Reis IM (2000) Is cadmium a cause of human pancreatic cancer? Cancer Epidemiol Biomarkers Prev 9(2):139–145
Rahim F, Jalali A, Tangestani R (2013) Breast cancer frequency and exposure to cadmium: a meta-analysis and systematic review. Asian Pac J Cancer Prev 14(7):4283–4287
Nawrot TS, Martens DS, Hara A, Plusquin M, Vangronsveld J, Roels HA, Staessen JA (2015) Association of total cancer and lung cancer with environmental exposure to cadmium: the meta-analytical evidence. Cancer Causes Control. doi:10.1007/s10552-015-0621-5
Larsson SC, Wolk A (2015) Urinary cadmium and mortality from all causes, cancer and cardiovascular disease in the general population: systematic review and meta-analysis of cohort studies. Int J Epidemiol. doi:10.1093/ije/dyv086
Oliveira H, Monteiro C, Pinho F, Pinho S, Ferreira de Oliveira JM, Santos C (2014) Cadmium-induced genotoxicity in human osteoblast-like cells. Mutat Res Genet Toxicol Environ Mutagen 775–776:38–47. doi:10.1016/j.mrgentox.2014.10.002
Du X, Lan T, Yuan B, Chen J, Hu J, Ren W, Chen Z (2015) Cadmium-induced microsatellite instability in the kidneys and leukocytes of C57BL/6J mice. Environ Toxicol 30(6):683–692. doi:10.1002/tox.21946
Haase H, Ober-Blobaum JL, Engelhardt G, Hebel S, Rink L (2010) Cadmium ions induce monocytic production of tumor necrosis factor-alpha by inhibiting mitogen activated protein kinase dephosphorylation. Toxicol Lett 198(2):152–158. doi:10.1016/j.toxlet.2010.06.010
Yang Z, Lv Y, Wang Y (2012) Meta-analysis shows strong positive association of the TNF-alpha gene with tumor stage in bladder cancer. Urol Int 89(3):337–341. doi:10.1159/000341701
Filipic M (2012) Mechanisms of cadmium induced genomic instability. Mutat Res 733(1–2):69–77. doi:10.1016/j.mrfmmm.2011.09.002
Bibi M, Hashmi MZ, Malik RN (2015) The level and distribution of heavy metals and changes in oxidative stress indices in humans from Lahore district. Pak Hum Exp Toxicol. doi:10.1177/0960327115578063
Tete N, Afonso E, Crini N, Drouhot S, Prudent AS, Scheifler R (2014) Hair as a noninvasive tool for risk assessment: do the concentrations of cadmium and lead in the hair of wood mice (Apodemus sylvaticus) reflect internal concentrations? Ecotoxicol Environ Saf 108:233–241. doi:10.1016/j.ecoenv.2014.07.010
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing Interests
The authors declared that they have no competing interests.
Additional information
Statement: This study is an original work
Rights and permissions
About this article

Cite this article
Zhang, L., Zhu, Y., Hao, R. et al. Cadmium Levels in Tissue and Plasma as a Risk Factor for Prostate Carcinoma: a Meta-Analysis. Biol Trace Elem Res 172, 86–92 (2016). https://doi.org/10.1007/s12011-015-0576-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12011-015-0576-0