
Abstract
Reserpine administration results in a predictable animal model of orofacial dyskinesia (OD) that has been largely used to access movement disturbances related to extrapyramidal oxidative damage. Here, OD was acutely induced by reserpine (two doses of 0.7 mg/kg subcutaneous (s.c.)), every other day for 3 days), which was administered after (experiment 1) and before (experiment 2) magnesium (Mg) supplementation (40 mg/kg/mL, peroral (p.o.)). In experiment 1, Mg was administered for 28 days before reserpine treatment, while in experiment 2, it was initiated 24 h after the last reserpine administration and was maintained for 10 consecutive days. Experiment 1 (prevention) showed that Mg supplementation was able to prevent reserpine-induced OD and catalepsy development. Mg was also able to prevent reactive species (RS) generation, thus preventing increase of protein carbonyl (PC) levels in both cortex and substantia nigra, but not in striatum. Experiment 2 (reversion) showed that Mg was able to decrease OD and catalepsy at all times assessed. In addition, Mg was able to decrease RS generation, with lower levels of PC in both cortex and striatum, but not in substantia nigra. These outcomes indicate that Mg is an important metal that should be present in the diet, since its intake is able to prevent and minimize the development of movement disorders closely related to oxidative damage in the extrapyramidal brain areas, such as OD.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Chronic use of typical antipsychotic drugs to treat psychotic symptoms has been related to development of movement disorders, which are manifested by repetitive involuntary movements, parkinsonism, and tremors [1, 2]. Often, these extrapyramidal symptoms can be incapacitating, while their prevention or reversion remains limited.
Reserpine-induced orofacial dyskinesia (OD) is a well-known experimental animal model [3–11], which may be quantified by orofacial movements and catalepsy [7, 12–14]. It has been shown that reserpine is able to deplete catecholamines such as dopamine (DA) by exerting a blockade in the vesicular monoamine transporter (VMAT), thus affecting neuronal transmission or storage. The consequent increase of DA in the cytosol promotes its auto-oxidation and catabolism by monoamine oxidase (MAO) [15], events that are closely related to development of oxidative stress (OS) [16, 17]. Therefore, extrapyramidal symptoms have been linked to reactive species generation and oxidative damage in the basal ganglia of the central nervous system (CNS) [18, 19].
While most studies have focused on antioxidant compounds [3, 20, 21], metals such as magnesium (Mg) are present in vegetables, bread and cold cereals, and milk [22], and their therapeutic potential has been applied clinically to treat asthma [23], fibromyalgia [24], pain [25], eclampsia [26], and cardiac arrhythmias [27]. In fact, Mg is the fourth most abundant divalent cation and the second most abundant intracellular cation of the body. This metal exerts critical regulation of cellular and enzymatic functions, thus affecting ion channels, metabolic cycles, and signaling pathways [28–30].
Increasing evidence indicates that neuronal death may be closely related to both acute and chronic degenerative disorders; Mg levels have been found to be decreased in some of these disorders [31, 32]. As a result, considerable research efforts have been directed toward establishing the mechanisms of such decline and the potential neuroprotective role for Mg [33, 34]. In addition, changes in Mg homeostasis and oxidative damage are closely correlated, suggesting a common mechanism involved in the pathogenesis of different disorders. Some studies have reported that Mg deficiencies may be related to increased susceptibility to in vivo and in vitro oxidative stress such as lipid peroxidation (LP), thus promoting immune-inflammatory response and reduced antioxidant defense systems such as glutathione (GSH), superoxide dismutase (SOD), and ascorbate [35–39].
Considering that acute reserpine is an extensively used animal model of movement disorder, here we propose to evaluate if Mg is able to prevent or minimize the development of reserpine-induced OD, as well as its beneficial effects on the oxidative damage in different brain areas such as cortex, striatum, and substantia nigra.
Material and Methods
Animals
Male Wistar rats weighing 250–320 g (about 3 months old) were used. Groups of three (±1) animals were kept in Plexiglas cages with free access to food (standard chow) and water in a room with controlled temperature (22–23 °C) and on a 12-h light/dark cycle with lights on at 7:00 a.m. Animals were fed with standard chow ad libitum (PuroTrato®, RS, Brazil), which contains adequate levels of Mg following recommendations from the National Research Council (NRC, 1995), during both experiment 1 and experiment 2. The experimental protocol was approved by the Animal Ethics Committee (Universidade Federal de Santa Maria – UFSM 064/2013), which is affiliated to the Council of Animal Experiments (CONCEA), following international norms of animal care and maintenance.
Drugs
Reserpine (methyl reserpate 3,4,5-trimethoxybenzoic acid ester; Sigma Chemical, St. Louis, MO) was dissolved in glacial acetic acid and then diluted to a final concentration of 0.1 % acetic acid with distilled water. The vehicle consisted of a 0.1 % acetic acid solution. Magnesium aspartate (Fragon do Brasil Farmacêutica Ltda) was dissolved in deionized water.
Experimental Procedure
Experiment 1: Preventive Effects of Magnesium Supplementation on the Development of Acute Orofacial Dyskinesia Induced by Reserpine
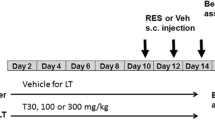
Twenty-eight rats were randomly divided in two groups of 14 animals each and orally supplemented (by gastric probe) with magnesium aspartate solution (40 mg/kg of body weight in 1 mL deionized water/kg body weight [40] or deionized water. After 28 days of oral supplementation, one half of each experimental group was treated with reserpine solution (0.7 mg/kg of body weight in 1 mL vehicle/kg body weight, subcutaneous (s.c.); R and Mg + R groups) or vehicle (0.1 % acetic acid solution; C and Mg groups) for 3 days (every other day). One day (24 h) after the last administration of reserpine/vehicle, all animals were submitted to behavioral evaluations as described in the “Behavioral Testing” section.
Experiment 2: Effects of Supplementation with Magnesium Aspartate on the Reversal of Acute Orofacial Dyskinesia Induced by Reserpine
Twenty-eight rats were randomly divided in two groups of 14 animals each and treated with reserpine solution (two doses of 0.7 mg/kg of body weight in 1 mL vehicle/kg body weight, s.c.; reserpine groups) or vehicle (0.1 % acetic acid solution; C and Mg groups) for 3 days (every other day). Twenty-four hours after the last administration of reserpine/vehicle, the development of orofacial dyskinesia was quantified. One half of each experimental group was immediately supplemented once a day (by gavage) with magnesium aspartate (40 mg/kg of body weight in 1 mL deionized water/kg body weight) (groups Mg and reserpine + Mg) or deionized water (groups C and R). Orofacial dyskinesia was quantified during the subsequent days (each 48 h). Mg supplementation was maintained throughout the behavioral assessment period (10 consecutive days).
Behavioral Testing
Orofacial Dyskinesia
Rats were placed individually in cages (20 × 20 × 19 cm) containing one mirror under the floor and one behind the back wall of the cage to allow behavioral quantification when the animal was facing away from the observer. To quantify the occurrence of OD, the frequency (number) of vacuous chewing movements (VCMs) was recorded for three sets of 6 min with 5-min intervals, totaling to 18 min of observation. VCMs were referred to as single mouth opening in the vertical plane not directed toward physical material [5]. Observers were blind to the drug treatment. In a preliminary study (using 5 control and 10 reserpine-treated rats ) of inter-rater reliability, we found that the use of this method of observation and parameter definition usually results in >91 % agreement between the three different observers. All the calculated p values were significant for p < 0.05.
Catalepsy Time
Catalepsy was measured immediately after OD observation in rats submitted to experiments 1 and 2 using a wire grid (25 × 30 cm2) inclined 45° relative to the bench top. Each rat was placed with its forepaws near the edge of the grid, and the amount of time spent in this atypical position (motionless) was recorded for three times, with a 5-min interval between them. All of the rats treated with reserpine (R and Mg + R of both experiments) were individually placed on the inclined grid and observed for 60 s. At the end of the three replications, the mean time spent by the rat without moving was calculated for each test. This behavioral test was adapted from Rocha [41].
Biochemical Assays
After behavioral evaluations, all animals were anesthetized with sodium thiopental (50 mg/kg body weight, i.p.) and euthanized by exsanguinations. Brains were immediately removed and cut coronally at the caudal border of the olfactory tubercle. Cortex, striatum, and substantia nigra were dissected according to Paxinos and Watson [42] and homogenized in 10 volumes (w/v) of 10 mM Tris-HCl buffer (pH 7.4) for determination of reactive species (RS) generation and protein carbonyl (PC).
Reactive Species Generation with Dichlorofluorescein-Reactive Species (DCH–RS)
RS levels were measured using the oxidant sensing fluorescent probe, 2′,7′-dichlorofluorescein diacetate (DCHF-DA) [43]. Dihydrofluorescein diacetate is superior for detecting intracellular oxidants: comparison with 2′,7′-dichloro dihydrofluorescein diacetate, 5 (and 6)-carboxy-2′,7′-dichloro dihydrofluorescein diacetate, and dihydrorhodamine. Theoxidation (DCHF-DA) to fluorescent dichlorofluorescein (DCF) was determined at 488 nm for excitation and 525 nm for emission. After homogenization of different brain areas (cortex, striatum, and substantia nigra) in 10 volumes (w/v) of 10 mM Tris-HCl buffer, pH 7.4, and centrifuged (15 min, 3500 rpm), 3 mL of the same buffer was added. After 10 s, 10 μM (DCHF-DA) (prepared in ethanol) was added to the mixture, and the fluorescence intensity from DCF was measured for 300 s and expressed as a percentage of the untreated control group. The protein content was normalized by quantification according to Lowry [44].
Protein Carbonyl Quantification
PC was quantified by the method of Levine [45], with some modifications. Soluble protein was mixed with 2,4-dinitrophenylhydrazine (DNPH; 10 Mm in 2 M HCl) or HCl (2 M) and incubated at room temperature for 1 h. Denaturing buffer (150 mM sodium phosphate buffer, pH 6.8, with 3 % sodium dodecyl sulfate), ethanol (99.8 %), and hexane (99.5 %) were added, mixed by shaking, and centrifuged. The protein isolated from the interface was washed two times with ethyl acetate/ethanol 1:1 (v/v) and suspended in denaturing buffer. Each DNPH sample was read at 370 nm in a spectrophotometer against the corresponding HCl sample (blank). The results were expressed as nmol carbonyl/g tissue.
Lipid Peroxidation Estimation
Lipid peroxidation of erythrocytes was determined by measuring the generation of thiobarbituric acid reactive substances (TBARSs) as described by Ohkawa [46], and expressed as nmol MDA/mL.
Statistical Analysis
In experiment 1, while orofacial dyskinesia (OD) was analyzed by two-way ANOVA 2 (control/Mg) × 2 (control/reserpine), catalepsy time was analyzed by the Student’s t test, because this behavior was observed only in the reserpine-treated groups (R and R plus Mg groups). In experiment 2, the Student’s t test was used in the first assessment of OD (C and R groups), which was quantified 24 h after the last reserpine administration. From the second day on (when Mg supplementation was initiated), three-way ANOVA was applied (2 (control/reserpine) × 2 (control/Mg) × 5 behavioral quantifications). This last factor was considered as a repeated measure followed by pairwise comparisons. Catalepsy time was analyzed by two-way ANOVA (2 (control/Mg) × 5 behavioral quantifications) and by pairwise test, considering the behavioral quantification as a repeated measure. Biochemical data from both experiments 1 and 2 were analyzed by two-way ANOVA 2 (control/Mg or reserpine) × (control/reserpine or Mg) for each analyzed tissue (cortex, striatum, substantia nigra, erythrocytes). All the comparisons were followed by Duncan’s multiple range test when appropriate (software Statistica 8.0 for Windows was used). Values of p < 0.05 were considered as statistically significant for all comparisons made.
Results
Experiment 1: Preventive Effects of Magnesium Supplementation on the Development of Acute Orofacial Dyskinesia and Oxidative Damage Induced by Reserpine
Preventive Effects of Mg on Orofacial Dyskinesia (OD) Development and Catalepsy Time
While Mg supplementation did not change orofacial parameters, reserpine treatment was related to OD development, which was partially prevented by Mg (Fig. 1a). Similarly, reserpine-treated rats presented catalepsy, while previous Mg supplementation was able to reduce the time of this behavior (Fig. 1b).

Influence of magnesium supplementation (Mg, 40 mg/kg of body weight in 1 mL deionized water/kg body weight, peroral (p.o.), for 28 days) on the prevention of orofacial dyskinesia (a) and catalepsy time (b) of rats subsequently injected with reserpine (two doses of 0.7 mg/kg of body weight in 1 mL vehicle/kg body weight, s.c., every other day). Animals were maintained with the standard chow during all experimental procedures. Data are expressed as mean ± SEM. Asterisk in (a) indicates significant difference from control group; cross indicates significant difference from Mg group; number sign indicates significant difference from reserpine group, determined by Duncan’s test (P < 0.05). Two-way ANOVA of VCM frequency revealed a significant main effect of supplementation and drug, and a significant supplementation × drug interaction (F(1,24) = 40.09, 67.22, and 26.31, P < 0.001, respectively). Number sign in (b) indicates significant difference from reserpine group, determined by Student’s t test (P < 0.05)
Preventive Effects of Mg on Oxidative Status in Cortex, Striatum, and Substantia Nigra
While Mg decreased RS generation and PC level per se in both cortex (Fig. 2a, d) and substantia nigra (Fig. 2c, f), reserpine treatment was able to increase these oxidative parameters in all evaluated brain areas (Fig. 2a–c). Reserpine administration increased RS generation in all evaluated brain areas (Fig. 2a–c), also increasing PC levels in both striatum (Fig. 2e) and substantia nigra (Fig. 2f). Previous supplementation of Mg was able to prevent reserpine-induced RS generation in both cortex (Fig. 2a) and substantia nigra (Fig. 2c), while the increase of PC levels was prevented in cortex (Fig. 2d) and attenuated in substantia nigra (Fig. 2f). In fact, Mg did not exert protective influence on RS generation and PC levels in striatum (Fig. 2b, e), whose values were comparable to those of the reserpine-treated group.

Influence of magnesium supplementation (Mg, 40 mg/kg of body weight in 1 mL deionized water/kg body weight, p.o., for 28 days) on the prevention of reactive species (RS) generation (a–c) and protein carbonyl (PC) levels (d–f) in cortex, striatum, and substantia nigra, respectively, of rats subsequently injected with reserpine (two doses of 0.7 mg/kg of body weight in 1 mL vehicle/kg body weight, s.c., every other day). Animals were maintained with the standard chow during all experimental procedure. Data are expressed as mean ± SEM. Asterisk indicates significant difference from control group; cross indicates significant difference from Mg group; number sign indicates significant difference from reserpine group, determined by Duncan’s test (P < 0.05). Two-way ANOVA revealed, for RS generation, a significant main effect of supplementation in cortex (a) and substantia nigra (c) (F(1,24) = 44.28 and 90.52, P < 0.001, respectively) and a significant main effect of drug in cortex (a), striatum (b), and substantia nigra (c) (F(1,24) = 5.37, P < 0.05; 45.65, P < 0.001; and 6.24, P < 0.05, respectively), while for PC levels, main effect of supplementation in cortex (d) and substantia nigra (f) (F(1,24) = 9.23, P < 0.05, and 49.42, P < 0.001, respectively) and a significant main effect of drug in striatum (e) and substantia nigra (f) (F(1,24) = 17.47, P < 0.001, and 27.79, P < 0.001, respectively)
Influence of Mg Supplementation Prior to Reserpine Administration on Lipid Peroxidation in Erythrocytes
Mg did not affect LP per se in erythrocytes, but this supplementation was able to prevent reserpine-induced increase of this oxidative marker. In fact, reserpine-treated rats that did not receive Mg previously showed a significant increase of LP in erythrocytes (Table 1).
Experiment 2: Effects of Magnesium Supplementation on the Development of Acute Orofacial Dyskinesia and Oxidative Damage Previously Induced by Reserpine
Reversion of Reserpine-Induced Orofacial Dyskinesia and Catalepsy Time
Animals presented increased VCM frequency 24 h after the last reserpine administration (Fig. 3a). After Mg supplementation was initiated, paired test comparisons indicated that while VCM frequency remained increased in all assessments in the R group, the R + Mg group showed a significant and progressive decrease of VCM frequency from day 2 until day 10. As expected, control and Mg-treated groups showed unchanged VCM number at all times observed (Fig. 3b). Reserpine-treated group showed increased VCM frequency, which was higher than in R + Mg in all assessments. In fact, this last experimental group (R + Mg) was able to reverse the higher frequency of VCM induced by reserpine at days 6 and 10, minimizing this behavior at days 2, 4, and 8, as at these times Mg and R + Mg showed significant differences from each other (Fig. 3b).

Influence of reserpine (two doses of 0.7 mg/kg of body weight in 1 mL vehicle/kg body weight, s.c., every other day) injection on development of orofacial dyskinesia (OD). Animals were maintained with the standard chow during all experimental procedure. Data are expressed as means ± SEM. a Influence of magnesium (Mg, 40 mg/kg of body weight in 1 mL deionized water/kg body weight, p.o.) supplementation or vehicle on OD development in rats previously treated with reserpine. Daily Mg supplementation was initiated immediately after the first behavioral assessment (basal), and maintained at day 10. Asterisk indicates significant difference from control group, determined by Student’s t test (P < 0.05). Asterisk in (b) indicates a significant difference from control group; cross indicates a significant difference from Mg group; number sign indicates a significant difference from reserpine group, determined by Duncan’s test (P < 0.05). Three-way ANOVA of VCM frequency revealed a significant main effect of drug (F(1,24) = 72.50; P < 0.001)),supplementation (F(1,24) = 5.69; P < 0.05)), repeated measure (F(4,108) = 5.10; P < 0.001), a significant drug × supplementation (F(4,108 = 12.83; P < 0.001)), a significant repeated measure × drug (F(4,108) = 11.89; P < 0.001)), and a significant repeated measure× supplementation (F(4,108) = 2.86; P < 0.05)) interaction
Reserpine-treated group was related to increased catalepsy time 24 h after the last drug administration (Fig. 4). After Mg supplementation was initiated, paired test comparisons indicated that while catalepsy time remained increased in all assessments in the R group, the R + Mg group showed decreased cataleptic behavior from day 6 to day 10. Mg supplementation (R + Mg group) decreased catalepsy time at days 2, 8, and 10 after the last reserpine injection. In fact, at days 4 and 6, both experimental groups (R and R + Mg) showed similar catalepsy time (Fig. 4).

Influence of magnesium supplementation (Mg, 40 mg/kg of body weight in 1 mL deionized water/kg body weight, p.o.) or vehicle on reserpine-induced catalepsy time (two doses of 0.7 mg/kg of body weight in 1 mL vehicle/kg body weight, s.c., every other day), observed every 2 days during its administration. Animals were maintained with the standard chow during all experimental procedure. Data are expressed as means ± SEM. Asterisk indicates a significant difference from control group; number sign indicates a significant difference from baseline, determined by Duncan’s test (P < 0.05). Two-way ANOVA of catalepsy time revealed a significant main effect of supplementation (F(1,24) = 33.07; P < 0.001)), repeated measure (F(4,108) = 14.71; P < 0.001), and a significant repeated measure × supplementation (F(4,108) = 4.35; P < 0.001)) interaction
The Effect of Mg Supplementation on Oxidative Status in Cortex, Striatum, and Substantia Nigra
While reserpine increased RS generation in all evaluated brain areas (Fig. 5a–c), this treatment increased PC levels in both cortex (Fig. 5d) and striatum (Fig. 5e), but not in substantia nigra (Fig. 5f). Mg supplementation was able to decrease RS generation in both cortex (Fig. 5a) and striatum (Fig. 5b), but not in substantia nigra (Fig. 5c). PC levels were also reduced by Mg supplementation in cortex (Fig. 5d) and striatum (Fig. 5e), whose values were similar to those of control and Mg-treated groups. In fact, Mg did not reduce PC levels in the substantia nigra (Fig. 5f), for in this brain area, reserpine did not increase the levels of this oxidative marker.

Influence of magnesium supplementation (Mg, 40 mg/kg of body weight in 1 mL deionized water/kg body weight, p.o.) or vehicle on reactive species (RS) generation (a–c) and protein carbonyl (PC) levels (d–f) in cortex, striatum, and substantia nigra, respectively, of rats previously injected with reserpine solution (two doses of 0.7 mg/kg of body weight in 1 mL vehicle/kg body weight, s.c., every other day). Animals were maintained with the standard chow during all experimental procedure. Data are expressed as mean ± SEM. Asterisk indicates significant difference from control group; cross indicates significant difference from Mg group; number sign indicates significant difference from Reserpine group, determined by Duncan’s test (P < 0.05). Two-way ANOVA revealed, for RS generation, a significant main effect of supplementation in striatum (b) (F(1,24) = 18.42, P < 0.001) and drug in cortex (a), striatum (b), and substantia nigra (c) (F(1,24) = 10.06, P < 0.05; 5.93, P < 0.05; and 94.43, P < 0.001, respectively) and a significant drug × supplementation interaction in all evaluated brain areas (a–c) (F(1,24) = 23.69, P < 0.001; 18.93, P < 0.001; and 6.76, P < 0.05, respectively), while for PC levels, a significant main effect of drug in striatum (e) (F(1,24) = 4.74, P < 0.05) and a significant main effect of supplementation and a significant drug × supplementation interaction in cortex (d) (F(1,24) = 30.12, P < 0.001; 4.57, P < 0.05, respectively)
Influence of Mg Supplementation After Reserpine Administration on Lipid Peroxidation in Erythrocytes
Reserpine administration was able to increase LP per se in erythrocytes, whose levels were decreased by Mg supplementation. Mg per se did not change the levels of this oxidative marker, whose value was comparable to that of the control group (Table 1).
Discussion
The current findings showed that (i) Mg supplementation before reserpine administration was sufficient to prevent movement disturbances, as quantified by VCM frequency and catalepsy time; (ii) Mg supplementation was able to prevent RS generation and PC levels in both cortex and substantia nigra, also preventing LP development in erythrocytes; (iii) Mg supplementation following reserpine treatment was able to minimize reserpine-induced VCM frequency and catalepsy time; and (iv) Mg supplementation was able to reduce RS generation and PC levels in both cortex and striatum, thus reverting the increased level of LP in erythrocytes, which were increased in the reserpine-treated group.
Reserpine administration results in a predictable animal model of orofacial dyskinesia (OD) that has been largely used to access movement disturbances related to extrapyramidal oxidative damage, whose mechanism of action is related to dopamine metabolism, excitotoxicity, and neurodegeneration [15]. In fact, reserpine depletes monoamine storage, mainly by blocking their vesicular transporter, thus favoring an excess of the neurotransmitter in the cytosol and consequently in the synaptic cleft. In such dopaminergic structures as cortex, striatum, and substantia nigra, DA itself can be a major contributor for oxidative damage, especially due to dopamine-quinones and hydrogen peroxide generation, as described elsewhere [47–49]. Experimentally, OD has been related to increased oxidative damage in extrapyramidal brain areas [5, 19, 50–54], as also observed here. In the current study, experiment 1 showed that extrapyramidal disorder occurred together with an increased generation of reactive species and a consequent oxidation of proteins in dopaminergic brain areas. Interestingly, magnesium supplementation was able to prevent and partially reverse both movement disturbance and oxidative events, which were quantified in brain areas and erythrocytes. In fact, increased VCM and catalepsy time were observed 24 h after reserpine treatment, which were decreased at days 2 and 6, respectively, of magnesium supplementation. It should be noted that the beneficial properties of magnesium supplementation were more robust when it was initiated prior to reserpine treatment, as in the reversion assay, reserpine-induced behavioral and oxidative damage was more subtly declined. Such evidence was somewhat expected, as it is more difficult to reverse damage already done. Nevertheless, this study confirmed the beneficial effects of magnesium, which were also observed after the development of such damage.
Of particular importance for our findings, current eating habits in Western countries include processed foods, whose chronic consumption has been related to an inadequate supply of micronutrients like vitamins, essential fatty acids, and minerals, including Mg. In fact, a decreased dietary provision of Mg was experimentally related to cataleptic behavior in rodents, while antiparkinson drugs were able to inhibit this extrapyramidal disturbance, indicating that this metal exerts a pivotal role in movement disorders [55]. More exactly, these authors suggested a relationship between dopaminergic hypofunction and cataleptic behavior as a consequence of a low Mg and calcium intake. Additionally, neurodegeneration of nigroestriatal dopaminergic brain area was linked to longer catalepsy [56]. Our attention on Mg was fueled by its important physiological role in regulating cellular and enzymatic functions pertaining to ion channels, metabolic cycles, and signaling pathways. In fact, abnormalities in Mg homeostasis may lead to biochemical dysregulation and thus contribute to the development of neurological disorders, such as Parkinson’s disease [57], among others. Of particular importance, Mg may influence glutathione levels, especially in erythrocytes [58], where this metal is an essential cofactor for synthesis of this antioxidant agent [59]. In this sense, rats submitted to a low Mg intake showed an increased susceptibility to oxidative damage [58, 60], while its supplementation showed a cytoprotective effect [61]. So, Mg supplementation is able to modulate the oxidative/antioxidant status [36, 38] and contribute to different pharmacotherapies for disorders involving oxidative damage. The use of antioxidant substances seems to be effective to reduce experimentally induced movement disorders, as previously reported by our group [3, 4, 67] and other research groups [53, 62–66].
In the current study, when supplemented before reserpine, Mg seems to have exerted a protective action against the generation of reactive species and protein oxidation in the cortex and substantia nigra, preventing as well lipid peroxidation in erythrocytes. Our findings are therefore consistent with previous studies showing that reserpine is able to negatively affect the oxidative status in brain areas involved in movement control [4, 19, 21, 67]. At this time, we cannot explain the differences in oxidative status, which were observed in the different brain structures when Mg was supplemented before and after reserpine administration. In fact, while the substantia nigra sends dopaminergic projections to the striatum as a target, this latter connects to other components of the basal ganglia via multiple projections involving, besides dopaminergic, GABAergic, cholinergic, and glutamatergic systems [68], making somewhat complex the understanding of these findings in each of these brain areas, singly. Moreover, besides dopamine metabolism, a negative relationship between glutamate transporter and OD manifestation in rats exposed to reserpine or haloperidol was reported [5], strengthening relationships between oxidative stress, excitotoxicity, and movement disorders. Concerning the aim of the current study, Mg exerts neuroprotective effects on the central nervous system (CNS). Its action mechanism has been related to a decreased presynaptic release of glutamate, an important excitatory neurotransmitter of the CNS [69]. Moreover, a blockade of glutamatergic N-methyl-D-aspartate (NMDA) receptor has also been associated with Mg [70–72]. In fact, Mg is able to block NMDA glutamate receptor ion channels, preventing ionic flow at typical neuronal resting potentials, thus decreasing activation of voltage-gated channels and reducing neuronal excitability. Of particular importance for our findings, continuous stimulation of NMDA receptor could induce a massive influx of Ca2+ into the cells, promoting cytotoxicity and mitochondrial dysfunction together with a subsequent release of apoptotic factors, which are precursors of cell death [73–76]. In this sense, Ca2+ dysregulation is decisive for neural death and degeneration following ischemic stroke, Parkinson’s disease [77], and Huntington’s disease [78]. In addition, experimental research on spinal cord injuries have shown that Mg was able to inhibit apoptosis, decreasing reactive species generation, lipid peroxidation, and caspase activation by blocking NMDA receptors [79, 80]. Based on all these evidences, it is possible to propose that Mg supplementation may act as an antioxidant modulator, whose action mechanism is mediated by NMDA receptor blockade, thus reducing excitotoxicity from glutamate. However, molecular studies involving the NMDA receptor and glutamate cascade should be conducted.
The present study indicates the beneficial influence of Mg supplementation, as observed by both prevention and reversion of reserpine-induced orofacial dyskinesia and catalepsy. These experimental protocols may contribute to increase our understanding of the pathophysiology of movement disorders and possibly to a preventive treatment.
In conclusion, our study showed that movement disorders may be prevented or attenuated by dietary Mg or by its supplementation. These findings reinforce the validity of this animal model as a fundamental tool to study motor diseases, including parkinsonism, dystonias, and akathisia related to antipsychotic treatment, whose pathophysiology has also been related to oxidative damage and neurotoxicity.
References
Novick D, Haro JM, Bertsch J, Haddad PM (2010) Incidence of extrapyramidal symptoms and tardive dyskinesia in schizophrenia: thirty-six-month results from the European schizophrenia outpatient health outcomes study. J ClinPsychopharmacol 30:531–40. doi:10.1097/JCP.0b013e3181f14098
Bakker PR, de Groot IW, van Os J, van Harten PN (2011) Long-Stay psychiatric patients: a prospective study revealing persistent antipsychotic-induced movement disorder. PLoS One 6:1–6. doi:10.1371/journal.pone.0025588
Trevizol F, Benvegnú DM, Barcelos RCS et al (2011) Comparative study between two animal models of extrapyramidal movement disorders: prevention and reversion by pecan nut shell aqueous extract. Behav Brain Res 221:13–18. doi:10.1016/j.bbr.2011.02.026
Barcelos RCS, Benvegnu DM, Boufleur N et al (2011) Short term dietary fish oil supplementation improves motor deficiencies related to reserpine-induced Parkinsonism in rats. Lipids 46:143–149. doi:10.1007/s11745-010-3514-0
Bürger ME, Fachinetto R, Zeni G, Rocha JBT (2005) Ebselen attenuates haloperidol-induced orofacial dyskinesia and oxidative stress in rat brain. Pharmacol Biochem Behav 81:608–615. doi:10.1016/j.pbb.2005.05.002
Abílio VC, Araújo V, Bergamo M et al (2003) Vitamin E attenuates reserpine-induced Oral dyskinesia and striatal oxidized glutathione/reduced glutathione Ratio (GSSG/GSH) enhancement in rats. Prog Neuro Psychopharmacol 2:7109–7114. doi:10.1016/S0278-5846(02)00340-8
Bergamo M, Abílio VC, Queiroz CMT et al (1997) Effects of age on a new model of Tardive dyskinesia. Neurobiol Aging 18:623–629. doi:10.1016/S0197-4580(97)00152-8
Dutra RC, Andreazza AP, Andreatini ST, Vital MABF (2002) Behavioral effects of MK-801 on reserpine-treated mice. Prog Neuropsychopharmacol Biol Psychiatry 26:487–495. doi:10.1016/S0278-5846(01)00295-0
Raghavendra V, Naidu PS, Kulkarni SK (2001) Reversal of reserpine-induced vacuous chewing movements in rats by melatonin: involvement of peripheral benzodiazepine receptors. Brain Res 904:149–152. doi:10.1016/S0006-8993(01)02455-6
Silva RH, Abilio VC, Torres-Leite D et al (2002) Concomitant development of oral dyskinesia and memory deficits in reserpine-treated male and female mice. Behav Brain Res 132:171–177. doi:10.1016/S0166-4328(01)00409-0
Sussman AN, Trannguyen LTL, Neisewander JL (1997) Acute reserpine administration elicits long-term spontaneous oral dyskinesia. Eur J Pharmacol 337:157–160. doi:10.1016/S0014-2999(97)01271-5
Bürger ME, Alves A, Callegari L, Athayde FAR, Nogueira CW, Rocha JBT (2003) Ebselen attenuates reserpine-induced orofacial dyskinesia and oxidative stress in rat striatum. Prog Neuro Psychopharmacol 27:135–140. doi:10.1016/S0278-5846(02)00344-5
Neisewander JL, Castañeda E, Davisv DA (1994) Dose-dependent Differences in the development of reserpine-induced oral-dyskinesia in rats: support for a model of tardive dyskinesia. Psychopharmacology 116:79–84. doi:10.1007/BF02244874
Queiróz CMT, Frussa-Filho R (1999) Effects of buspirone on na animal model of tardive dyskinesia. Prog Neuro Psychopharmacol 23:1405–1418. doi:10.1016/S0278-5846(99)00074-3
Fuentes P, Paris I, Nassif M, Caviedes P, Segura-Aguilar J (2007) Inhibition of VMAT-2 and DT-diaphorase induce cell death in a substantia nigra-derived cell Line - An experimental cell model for dopamine toxicity studies. Chem Res Toxicol 20:776–783. doi:10.1021/tx600325u
Bilska A, Dubiela M, Sokołowska-Jez˙ewicz M et al (2007) Alpha-lipoic acid differently affects the reserpine-induced oxidative stress in the striatum and prefrontal cortex of rat brain. Neuroscience 146:1758–71. doi:10.1016/j.neuroscience.2007.04.002
Naidu PS, Singh A, Kulkarni SK (2004) Reversal of reserpine-induced orofacial dyskinesia and cognitive dysfunction by quercetin. Pharmacology 70:59–67. doi:10.1159/000074669
Lohr JB, Kuczenski R, Niculescu AB (2003) Oxidative mechanisms and tardive dyskinesia. CNS Drugs 17:47–62. doi:10.2165/00023210-200317010-00004
Teixeira AM, Reckziegel P, Müller L et al (2009) Intense exercise potentiates oxidative stress in striatum of reserpine-treated animals. Pharmacol Biochem Behav 92:231–235. doi:10.1016/j.pbb.2008.11.015
Fachinetto R, Villarinho JG, Wagner C et al (2007) Valerianaofficinalis does not alter the orofacial dyskinesia induced by haloperidol in rats: role of dopamine transporter. Prog Neuropsychopharmacol Biol Psychiatry 31:1478–86. doi:10.1016/j.pnpbp.2007.06.028
Reckziegel P, Dias VT, Benvegnú DM et al (2011) Locomotor damage and brain oxidative stress induced by lead exposure are attenuated by gallic acid treatment. Toxicol Lett 203:74–81. doi:10.1016/j.toxlet.2011.03.006
Ford ES, Mokdad AH (2003) Dietary magnesium intake in a national sample of US adults. J Nutr 133:2879–82
Kowal A, Panaszek B, Barg W, Obojski A (2007) The use of magnesium in bronchial asthma: a new approach to an old problem. Arch Immunol Ther Ex 55:35–9. doi:10.1007/s00005-007-0008-8
Porter NS, Jason LA, Boulton A, Bothne N, Coleman B (2010) Alternative medical interventions used in the treatment and management of myalgic encephalomyelitis/chronic fatigue syndrome and fibromyalgia. J Altern Complement Med 16:235–49. doi:10.1089/acm.2008.0376
Soave PM, Conti G, Costa R, Arcangeli A (2009) Magnesium and anaesthesia. Curr Drug Targets 10:734–43. doi:10.2174/138945009788982487
Euser AG, Cipolla MJ (2009) Magnesium sulfate for the treatment of eclampsia. Stroke 40:1169–75. doi:10.1161/STROKEAHA.108.527788
Manrique AM, Arroyo M, Lin Y et al (2010) Magnesium supplementation during cardiopulmonary bypass to prevent junctional ectopic tachycardia after pediatric cardiac surgery: a randomized controlled study. J Thorac Cardiovasc Surg 139:162–9. doi:10.1016/j.jtcvs.2009.07.064
Saris NE, Mervaala E, Karppanen H et al (2000) Magnesium: an update on physiological, clinical and analytical aspects. Clin Chim Acta 294:1–26. doi:10.1016/S0009-8981(99)00258-2
Sabatier M, Arnaud MJ, Kastenmayer P, Rytz A, Barclay DV (2002) Meal effect on magnesium bioavailability from mineral water in healthy women. Am J Clin Nutr 75:65–71
Wolf FI, Cittadini A (2003) Chemistry and biochemistry of magnesium. Mol Asp Med 24:3–9. doi:10.1016/S0098-2997(02)00087-0
Barra A, Camardese G, Tonioni F et al (2007) Plasma magnesium level and psychomotor retardation in major depressed patients. Magnes Res 20:245–249. doi:10.1684/mrh.2007.0115
Vink R, Cook NL, van den Heuvel C (2009) Magnesium in acute and chronic brain injury: an update. Magnes Res 22:158–162. doi:10.1684/mrh.2009.0175
Hoane MR (2007) Assessment of cognitive function following magnesium therapy in the traumatically injured brain. Magnes Res 20:229–36. doi:10.1684/mrh.2007.0113
Hoane MR, Gilbert DR, Barbre AB, Harrison SA (2008) Magnesium dietary manipulation and recovery of function following controlled cortical damage in the rat. Magnes Res 21:29–37. doi:10.1684/mrh.2008.0128
Regan RF, Jasper E, Guo Y, Panter SS (1998) Effect of magnesium on oxidative neuronal injury in vitro. J Neurochem 70:77–85. doi:10.1046/j.1471-4159.1998.70010077.x
Ariza AC, Bobadilla N, Fernandez C et al (2005) Effects of magnesium sulfate on lipid peroxidation and blood pressure regulators in pre-eclampsia. Clin Biochem 38:128–33. doi:10.1016/j.clinbiochem.2004.09.018
Wolf FI, Trapani V, Simonacci M, Ferre S, Maier JAM (2008) Magnesium deficiency and endothelial dysfunction: is oxidative stress involved? Magnes Res 21:58–64. doi:10.1684/mrh.2008.0129
Turkoglu OF, Eroglu H, Okutan O et al (2008) A comparative study of treatment for brain edema Magnesium sulphate versus dexamethasone sodium phosphate. J Clin Neurosci 15:60–65. doi:10.1016/j.jocn.2007.03.005
Altura BM, Shah NC, Jiang X et al (2009) Short-term magnesium deficiency results in decreased levels of serum sphingomyelin, lipid peroxidation and apoptosis in cardiovascular tissues. Am J Physiol Heart C 297:86–92. doi:10.1152/ajpheart.01154.2008
Safar MM, Abdallah DM, Arafa NM, Abdel-Aziz MT (2010) Magnesium supplementation enhances the anticonvulsant potential of valproate in pentylenetetrazol-treated rats. Brain Res 1334:58–64. doi:10.1016/j.brainres.2010.03.076
Rocha JBT, Santos JET, Rocha LK, Kleinpaul ER (1997) Undernutrition during suckling changes the sensivity to haloperidol and chlorpromazine in two behavioural measures in weaning rats. Pharmacol Toxicol 80:114–123. doi:10.1111/j.1600-0773.1997.tb00040.x
Paxinos G, Watson C (2007) The rat brain in stereotaxic coordinates. Elsevier, Amsterdam
Hempel SL, Buettner GRO, Malley YQ, Wessels DA, Flaherty DM (1999) Dihydrofluo-resceindiacetate is superior for detecting intracellular oxidants: comparisonwith 2′, 7′-dichloro dihydrofluoresceindiacetate, 5 (and 6)- carboxy-2′, 7′-dichloro dihydrofluoresceindiacetate, and dihydrorhodamine. Free Radical Biol Med 27:146–59. doi:10.1016/S0891-5849(99)00061-1
Lowry OH, Rosebrough NJ, Farr AL, Randall RJ (1951) Protein measurement with the Folin–Phenol reagents. J Biol Chem 193:265–275
Levine RL, Williams JA, Stadtman ER, Shacter E (1994) Carbonyl assays for determination of oxidatively modified proteins. Method Enzymol 233:346–357. doi:10.1016/S0076-6879(94)33040-9
Ohkawa H, Ohishi N, Yagi K (1979) Assay for lipid peroxides in animal tissues by thiobarbituric acid reaction. Anal Biochem 95:351–358. doi:10.1016/0003-2697(79)90738-3
Lohr JB (1991) Oxygen radicals and neuropsychiatric illness: some speculations. Arch Gen Psychiatry 48:1097–1106. doi:10.1001/archpsyc.1991.01810360061009
Asanuma M, Miyazaki I, Ogawa N (2003) Dopamine- or L-DOPA-induced neurotoxicity: the role of dopamine quinone formation and tyrosinase in a model of Parkinson’s disease. Neurotox Res 5:165–176. doi:10.1016/j.febslet.2004.12.091
Asanuma M, Miyazaki I, Diaz-Corrales FJ, Ogawa N (2004) Quinone formation as dopaminergic neuron-specific oxidative stress in pathogenesis of sporadic Parkinson’s disease and neurotoxina-induced parkinsonismo. Acta Med Okayama 58:221–233
Naidu PS, Singh A, Kulkarni SK (2003) Quercetin, a bioflavonoid, attenuates haloperidol-induced orofacial dyskinesia. Neuropharmacology 44:1100–1106. doi:10.1016/S0028-3908(03)00101-1
Andreassen OA, Jorgensen HA (2000) Neurotoxicity associated with neuroleptic-induced oral dyskinesi as in rats. Implications for tardive dyskinesia. Prog Neurobiol 61:525–541. doi:10.1016/S0301-0082(99)00064-7
Faria RR, Abílio VC, Grassl C et al (2005) Beneficial effects of vitamin C and vitamin E on reserpine-induced oral dyskinesia in rats: critical role of striatal catalase activity. Neuropharmacology 48:993–1001. doi:10.1016/S0301-0082(99)00064-7
Peroza LR, Busanello A, Leal CQ et al (2013) Bauhinia forficata prevents vacuous chewing movements induced by haloperidol in rats and has antioxidant potential in vitro. Neurochem Res 38:789–796. doi:10.1007/s11064-013-0981-8
Reckziegel P, Peroza LR, Schaeffer LF et al (2013) Gallic acid decreases vacuous chewing movements induced by reserpine in rats. Pharmacol Biochem Be 104:132–137. doi:10.1016/j.pbb.2013.01.001
Taniguchi R, Nakagawasai O, Tan-no K et al (2013) Combined low calcium and lack magnesium is a risk fator for motor déficit in mice. Biosci Biotech Biochem 77:266–270. doi:10.1271/bbb.120671
Schmidt WJ, Kretschmer BD (1997) Behavioural pharmacology of glutamate receptors in the basal ganglia. Neurosci Biobehav Rev 21:381–392. doi:10.1016/S0149-7634(96)00044-9
Oyanagi K, Ka-wakami E, Kikuchi-Horie K et al (2006) Magnesium deficiency over generations in rats with special references to the pathogenesis of the Parkinsonism-dementia complex and amyotrophic lateral sclerosis of Guam. Neuropathology 26:115–128. doi:10.1111/j.1440-1789.2006.00672.x
Kuzniar A, Mitura P, Kurys P et al (2003) The influence of hypomagnesemia on erythrocyte antioxidant enzyme defence system in mice. Biometals 16:349–357. doi:10.1023/A:1020632505289
Minnnich et al (1971) Glutathione biosynthesis in human erythrocytes. 1. Identification of the enzymes of glutathione synthesis in hemolysates. J Clin Invest 50:507–513. doi:10.1172/JCI106519
Boparai RK, Kiran R, Bansal DD (2007) Insinuation of exacerbated oxidative stress in sucrose-fed rats with a low dietary intake of magnesium: evidence of oxidative damage to proteins. Free Radic Res 41:981–989. doi:10.1080/10715760701447892
Regan RF, Guo Y (2001) Magnesium deprivation decreases cellular reduced glutathione and causes oxidative neuronal death in murine cortical cultures. Brain Res 890:177–183. doi:10.1016/S0006-8993(00)03156-5
Colpo G, Trevizol F, Teixeira AM et al (2007) Ilex paraguariensis has antioxidant and attenuates haloperidol-induced orofacial dyskinesia and memory dysfunction in rats. Neurotox Res 12:171–180. doi:10.1007/BF03033914
Nade VS, Kawale LA, Yadav AV (2010) Protective effect of Morusalba leaves on haloperidol-induced orofacial dyskinesia and oxidative stress. Pharm Biol 48:17–22. doi:10.3109/13880200903029357
Daya RP, Tan ML, Sookram CD, Skoblenick K, Mishra RK (2011) Alpha-phenyl-N-tert-butylnitrone prevents oxidative stress in a haloperidol-induced animal model of tardive dyskinesia: investigating the behavioural and biochemical changes. Brain Res 1412:28–36. doi:10.1016/j.brainres.2011.07.014
Macêdo DS, de Oliveira GV, Gomes PXL et al (2011) B vitamins attenuate haloperidol-induced orofacial dyskinesia in rats: possible involvement of antioxidant mechanisms. Behav Pharmacol 22:674–680. doi:10.1097/FBP.0b013e32834aff6d
Patil R, Hiray Y, Shinde S, Langade P (2012) Reversal of haloperidol induced orofacial dyskinesia by Murrayakoenigii leaves in experimental animals. Pharm Biol 50:691–697. doi:10.3109/13880209.2011.618841
Teixeira A, Müller LG, Reckziegel P et al (2011) Beneficial effects of an innovative exercise model on motor and oxidative disorders induced by haloperidol in rats. Neuropharmacology 60:432–438. doi:10.1016/j.neuropharm.2010.10.017
Fix JD (2008) Basal Ganglia and the Striatal Motor System. Neuroanatomy (Board Review Series) (4th ed). Baltimore: Wulters Kluwer & Lippincott Wiliams& Wilkins. pp. 274–281. ISBN 0-7817-7245-1
Lin JY, Chung SY, Lin MC, Cheng FC (2002) Effects of magnesium sulfate on energy metabolites and glutamate in the cortex during focal cerebral ischemia and reperfusion in the gerbil monitored by a dural probe microdialysis technique. Life Sci 71:803–811. doi:10.1016/S0024-3205(02)01738-1
Mayer ML, Westbrook GL, Guthrie PB (1984) Voltage-dependent block by Mg2+ of NMDA responses in spinal cord neurones. Nature 309:261–263. doi:10.1038/309261a0
Bekkers JM, Stevens CF (1993) NMDA receptors at excitatory synapses in the hippocampus: test of a theory of magnesium block. Neurosci Lett 156:73–7. doi:10.1016/0304-3940(93)90443-O
Dingledine R, Borges K, Bowie D, Traynelis SF (1999) The glutamate receptor ion channels. Pharmacol Rev 51:7–61
Trump BF, Berezesky IK (1995) Calcium-mediated cell injury and cell death. FASEB J 9:219–28
Norberg E, Gogvadze V, Ott M et al (2008) An increase in intracellular Ca2+ is required for the activation of mitochondrial calpain to release AIF during cell death. Cell Death Differ 15:1857–1864. doi:10.1038/cdd.2008.123
Lemasters JJ, Theruvath TP, Zhong Z, Nieminen AL (2009) Mitochondrial calcium and the permeability transition in cell death. Biochim Biophys Acta Bioenerg 1787:1395–1401. doi:10.1016/j.bbabio.2009.06.009
Seo JH, Fox JG, Peek RM, Hagen SJ (2012) N-methyl-D-aspartate (NMDA) Channels regulate apoptosis in helicobacter pylori infection by ammonia-induced calcium permeation mechanisms. FASEB J 26:1156.1. doi:10.1053/j.gastro.2011.08.048
Surmeier DJ, Guzman JN, Sanchez-Padilla J (2010) Calcium, cellular aging, and selective neuronal vulnerability in Parkinson’s disease. Cell Calcium 47:175–182. doi:10.1016/j.ceca.2009.12.003
Tang TS, Slow E, Lupu V et al (2005) Disturbed Ca2+ signaling and apoptosis of medium spiny neurons in Hungtingon’s disease. P Natl Acad Sci USA 102:2602–2607. doi:10.1073/pnas.0409402102
Solaroglu I, Kaptanoglu E, Okutan O, Beskonakli E, Attar A, Kilinc K (2005) Magnesium sulfate treatment decreases caspase-3 activity after experimental spinal cord injury in rats. Surg Neurol 64:17–21. doi:10.1016/j.surneu.2005.07.058
Sencer A, Aydoseli A, Aras Y et al (2013) Effects of combined and individual use of N-methyl-D aspartate receptor antagonist magnesium sulphate and caspase-9 inhibitor z-LEDH-fmk in experimental spinal cord injury. Ulus Travma Acil Cer 19:313–319. doi:10.5505/tjtes.2013.45804
Acknowledgments
The authors are grateful to CAPES (M.K., H.J.S., C.T.D.A., K.R., and C.S.P.) and CNPq (Kr.R.) for the fellowships, as well to CNPq (M.E.B.) for the research grants. Authors report no conflicts of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Kronbauer, M., Segat, H.J., De David Antoniazzi, C.T. et al. Magnesium Supplementation Prevents and Reverses Experimentally Induced Movement Disturbances in Rats: Biochemical and Behavioral Parameters. Biol Trace Elem Res 166, 163–172 (2015). https://doi.org/10.1007/s12011-015-0268-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12011-015-0268-9