
Abstract
The incidence of both frailty and lower urinary tract symptoms, including urinary incontinence, overactive bladder, underactive bladder, and benign prostatic hyperplasia, increases with age. However, our understanding of the relationship between frailty and lower urinary tract symptoms, both in terms of pathophysiology and in terms of the evaluation and management of such symptoms, is greatly lacking. This brief review will summarize definitions and measurement tools associated with frailty and will also review the existing state of the literature on frailty and lower urinary tract symptoms in older individuals.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Almost half (46%) of all urologic visits and 62% of all urologic procedures are performed in older adults [1]. These numbers will rise dramatically with the rapidly growing older population, which is projected to increase at least 20% by the year 2030 [2]. Among the most common urologic conditions in the older population are lower urinary tract symptoms, which also increase with increasing age.
A particular subset of older individuals has added vulnerabilities such as pre-existing illness, poor functional status, polypharmacy, cognitive deficits, and limited social support, placing them at particular risk for frailty and associated adverse events. While both lower urinary tract symptoms and frailty are common among the older population, the literature is limited in its characterization of these individuals and in their response to various treatments.
Herein, we will review the concept of frailty and the current state of the literature at the intersection of frailty and lower urinary tract symptoms including urinary incontinence, overactive bladder, underactive bladder, and benign prostatic hyperplasia.
Frailty; Definition and Measurement
Frailty is a state of vulnerability that has been conceptualized as a biologic syndrome of decreased reserve or resistance to stressors, resulting in adverse outcomes such as disability, institutionalization, and mortality. Frailty is considered to be potentially reversible and therefore, a target for care strategies to improve outcomes. Depending on the measurement used, frailty exists in anywhere from 36 to 88% of older individuals [3]. A single operational definition of frailty, however, has yet to be defined, and definitions typically follow two main conceptualizations: the frailty phenotype and the accumulation of deficits model.
Fried et al. developed the frailty phenotype using data from the Cardiovascular Health Study. They looked at 5317 men and women ages 65 and older and followed them for up to 7 years. They conceptualized frailty as distinct from disability, comorbidity, and old age and as more of a biologic syndrome spanning across multiple physiologic systems causing vulnerability and adverse outcomes. Their model incorporates age-associated declines in lean body mass, strength, endurance, balance, walking performance, and low activity, where multiple components must be present to define frailty. They further proposed a theoretical cycle of frailty associated with declining energetics and reserve.
They then operationalized this theoretical cycle into five criteria: (1) slow walking speed, (2) weakness (defined as impaired grip strength), (3) low physical activity, (4) self-reported exhaustion, and (5) unintended weight loss (10 lbs in the past year). Individuals with deficits in three or more categories are defined as “frail”, those with deficits in one or two categories are defined as “pre-frail”, and those with no deficits as “robust”. This frailty phenotype is independently predictive of incident falls, worsening mobility, or declines in activities of daily living (ADLs), hospitalization and death over 3 years. Intermediate frailty is associated with intermediate risk of these outcomes and an increased risk of becoming frail over a time period of 3–4 years [4].
The deficit accumulation model of frailty, on the other hand, was popularized by Rockwood et al. and suggests that frailty is represented by discrete failures of redundant physiologic systems. In this model, the more deficits that occur, the more likely it is that adverse outcomes will result. Rockwood’s original model was based on data from the Canadian Study of Health and Aging and includes 96 items comprised of symptoms, signs, functional impairments, and laboratory abnormalities that make up a frailty index [5].
Neither the frailty phenotype nor the deficit accumulation model is all inclusive or ideal for the clinical setting. The frailty phenotype omits items on cognition or mood and is not practical to use in a busy clinical setting [6]. The deficit accumulation model lends itself for use in large databases, such as the American College of Surgeons National Surgical Quality Improvement Project (ACS-NSQIP), [7] making it helpful for research and public health and policy purposes, but also impractical in the clinical setting.
In order to address the need for a usable frailty model in the clinical setting, Robinson et al. developed a frailty assessment specifically for older individuals undergoing surgery. This includes the following measures: (1) Mini-Cog Test (cognition), albumin, having fallen in the past 6 months, hematocrit, Katz score (function), and Charlson index (comorbidity). These criteria were applied to 100 individuals (average age 74) undergoing major operations requiring postoperative intensive care unit admission. Using logistic regression analysis, the authors found that the presence of any functional dependence was the strongest predictor of 6-month mortality and that the presence of four or more of the measured deficits had high sensitivity (81%) and specificity (86%) for 6-month mortality [8].
In a subsequent study looking at 201 patients ages 65 and older undergoing elective colorectal or cardiac surgery, Robinson et al. evaluated seven baseline frailty traits and their relationship to postoperative complications. These traits included the following: (1) Katz score ≤ 5, (2) Timed Up and Go Test ≥ 15 s, (3) Charlson index ≥ 3, (4) Mini-Cog Score ≤ 3, (5) anemia < 35%, (6) albumin < 3.4 g/dL, and (7) one or more falls within 6 months. The presence of four or more traits classified an individual as “frail”. The authors found that preoperative frailty was associated with increased postoperative complication rates after both colorectal (58%) and cardiac (56%) operations that was independent of advancing age. Frail individuals also had longer hospital stays and higher 30-day readmission rates [9]. Next, the authors isolated the Timed Up and Go Test and found that individuals with slower Timed Up and Go Test speeds were associated with increased postoperative complications and increased 1-year mortality, suggesting that this test may be a single parsimonious measure that can be easily executed in the clinical setting as opposed to the more complex risk calculators previously described [10].
Lower Urinary Tract Symptoms
The study of frailty among older individuals with lower urinary tract symptoms (LUTS) is in its infancy. Unfortunately, frail older individuals are often poorly represented in research studies, especially in those that include pharmacotherapy and invasive interventions. In part, this is because frail individuals often suffer from multiple impairments, such as poor mobility, cognitive impairment, and renal failure, in addition to multiple comorbidities such as heart failure and polypharmacy, [11] making their involvement in studies complicated for researchers and for patients alike. Herein, we will discuss what is known about frailty and certain LUTS including urinary incontinence, overactive bladder, underactive bladder, and benign prostatic hyperplasia (BPH).
Urinary Incontinence
Urinary incontinence occurs in 30–40% of individuals over the age of 65 [12, 13] and in up to 60–70% of individuals residing in long-term care facilities. Incontinence is so common among the older population that it is considered to be a geriatric syndrome alongside frailty, delirium, falls, dizziness, syncope, gait abnormalities, sleep disorders, and pressure ulcers [14]. Additionally, incontinence has been shown to be associated with a twofold increased risk of impairment of both personal and instrumental activities of daily living, suggesting that it may represent an early marker of frailty [15•].
Nursing home residents by definition exhibit a frailty phenotype and represent a good cohort for the study of frailty. One study found an increased risk of newly recognized urinary incontinence among nursing home residents following a diagnosis of several other disease conditions including Parkinson’s disease, stroke, depression, and congestive heart failure. They further documented a significantly increased risk of hospitalization and nursing home admissions among women and men with urinary incontinence, independent of age, gender, and multiple comorbid conditions, with a 30 and 50% higher risk of hospitalization and 2.0 and 3.2 times higher adjusted risk of admission to a nursing facility, respectively [16].
Urinary continence in the frail older population is multifactorial and is not just reliant on the genitourinary tract. For example, continence in this population depends on sufficient cognition to recognize and interpret the desire to void and to locate and reach a restroom in adequate time to avoid leakage of urine [17]. Furthermore, interventions in the frail older population often involve behavioral strategies such as prompted voiding, habit retraining, timed voiding, and combined toileting and exercise therapy [15•]. One systematic review of conservative treatment of urinary incontinence in the frail older population found that pelvic muscle exercise, physical training in combination with ADLs, prompted voiding and attention training, and help to toilet are important treatment strategies, albeit, with limited evidence due to the lack of high-quality studies [18].
Resnick found that 40% of institutionalized older individuals were chronically incontinent of urine. He performed detailed urodynamic studies on 94 of these individuals and found that detrusor overactivity was the leading cause of incontinence (61%), with half of these individuals having concomitant impaired detrusor contractility. Other causes of incontinence among women were stress urinary incontinence (21%), detrusor underactivity (8%), and outlet obstruction (4%). Among men, the leading cause of incontinence was outlet obstruction (29%). Overall, at least 35% of men and women had more than one cause for their incontinence, suggesting that the etiology of urinary incontinence in the frail older population is complex [19].
Overactive Bladder
There are several age-related changes that predispose an individual to overactive bladder, or the symptom complex of urinary urgency, usually with frequency and nocturia, in the absence of the pathology such as infection or stones [20]. Among these changes are an age-related decrease in the neural control of continence and changes to the bladder itself. From a neural standpoint, functional magnetic resonance imaging (fMRI) studies indicate a decrease in the neural control of continence represented in the insula, anterior cingulate cortex, and prefrontal cortex. There is also a heightened activation of the anterior cingulate cortex with low bladder volumes, representing an increase in bladder sensitivity or perceived sense of urgency. From a bladder standpoint, there are documented changes in the urothelium, neurotransmitters and receptors, and inflammation that are associated with overactive bladder [21].
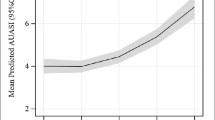
Among individuals ages 65 and older presenting to an outpatient benign urology practice, men and women with a diagnosis of overactive bladder were significantly more frail, defined by the Timed Up and Go Test, compared to individuals with other non-oncologic urologic diagnoses. On average, individuals with an overactive bladder diagnosis had a mean Timed Up and Go Test time of 13.7 ± 7.9 s compared to 10.9 ± 5.2 s among those with other non-oncologic urologic diagnoses (p < 0.0001). Interestingly, in regression analysis, frailty, when adjusted for age, race, sex, and number of medications, was a statistically significant predictor of overactive bladder (OR 3.0, 95% CI 2.0–4.8), while age, adjusted for frailty, race, sex, and number of medications, was not. These are the first data to help distinguish the effects of frailty from age among individuals with overactive bladder, and they underscore the importance of frailty among this population [22].
Data on treatments for overactive bladder among the frail older population are limited, as this population is often excluded from research trials. One systematic review [23•] found that oxybutynin was the only drug studied in the frail population [24,25,26]. All of these studies evaluated the use of oxybutynin versus placebo among nursing home residents and all found a lack of clinical effectiveness of oxybutynin compared to placebo with no differences in adverse events between the two.
More recently, a randomized placebo control trial looked at the efficacy of fesoterodine in vulnerable older men and women. They randomized 562 community dwelling individuals with high rates of comorbidity, polypharmacy, and functional impairment to fesoterodine versus placebo. The treatment group had significantly greater improvement at 12 weeks in urgency urinary incontinence episodes per 24 h (−2.84 versus −2.20, p = 0.002) and adverse events were similar to those typically seen in younger individuals [27•]. Of note, β3-adrenoceptor agonists have not been specifically studied specifically in older or frail older individuals [28].
In order to avoid systemic side effects of pharmacotherapy, third line treatments for overactive bladder such as onabotulinumtoxinA and sacral neuromodulation offer alterative treatment options. One study evaluated the use of 100 units of onabotulinumtoxinA in 166 patients with urodynamic evidence of detrusor overactivity who were medication refractory. They defined frailty in individuals who met at least three of the following criteria: unintentional weight loss, self-reported exhaustion, slow walking speed, weakness, and/or low physical activity. In total, they evaluated the use of onabotulinumtoxinA in 61 frail older individuals, 63 non-frail older individuals, and 42 individuals younger than age 65. While success rates were similar between the three groups at 3 and 6 months after treatment, the success rates at 12 months after treatment were significantly lower in the frail older group compared to the other groups (6.82% compared to 22.3 and 23.1%, in the non-frail older and younger groups, respectively), and the cumulative success rate was significantly lower in the frail older group than in the other two groups (p = 0.009). Frail older individuals had significantly higher rates of elevated post void residuals (defined as >150 ml) compared to the other groups (60.7% compared to 39.7 and 35.7% in non-frail older and younger individuals, respectively; p = 0.018) and urinary retention developed in 11.5% of frail older individuals compared to 6.3 and 2.4% of non-frail older and younger individuals (p = 0.203) [29]. Of note, the use of sacral neuromodulation has not been evaluated specifically in the frail older population.
Underactive Bladder
The study of underactive bladder is still in its early stages, and no direct correlations have been made to frailty; however, there is reason to believe that a relationship may exist. Underactive bladder syndrome is defined by the International Continence Society as the “perception of detrusor underactivity, characterized by symptoms of prolonged voiding, hesitancy, slow and/or intermittent stream, and/or sensation of incomplete emptying” [30]. While the etiology of underactive bladder is still an enigma, it is postulated that it may represent chronic untreated or treatment refractory overactive bladder (due to neurological disease such as diabetes), bladder outlet obstruction, sarcopenia, aging, and frailty. It has been further hypothesized that untreated or severe overactive bladder progresses to detrusor hyperreflexia with impaired contractility (DHIC) and then into overactive bladder [31•]. Furthermore, it would be reasonable to posit that since frailty is associated with overactive bladder and since overactive bladder may lead to or be related to underactive bladder, that frailty and underactive bladder are indeed linked.
Benign Prostatic Hyperplasia
Benign prostatic hyperplasia (BPH) is common among older individuals. Approximately 21% of men ages 70 and older experience nocturia, 22% experience incomplete bladder emptying, and 57% experience a weak urinary stream [32]. The sequelae of BPH can greatly affect quality of life and may include acute urinary retention, urinary tract infections, bladder stone formation, gross hematuria, and even renal failure in extreme cases.
While there is no known documented direct link between frailty and BPH, physicians should proceed with caution and consider frailty when recommending treatment strategies. For example, the use of alpha-blockers as medical therapy should be prescribed with great caution due to the potential for orthostatic hypotension related to this medication. Procedures to treat BPH should also be undertaken with considerable care and thought in the frail older population.
Using data from ACS-NSQIP, frailty was shown to be associated with a statistically significant increased log odds of complications [33] and of discharge to a skilled or assisted living facility [34] among individuals undergoing transurethral resection of the prostate (TURP) after adjustment for multiple factors including year, age, race, type of anesthesia, smoking status, and recent weight loss. Collectively, these findings speak to the importance of preoperative counseling and thoughtful and informed decision-making among frail older men contemplating TURP.
Another study analyzing 2869 nursing home residents undergoing TURP found that procedure failure, measured as the presence of a Foley catheter 1 year after surgery was associated with poor baseline functional status (RR 1.34, 95% CI 1.18–1.52), decline in ADLs in the 6 months prior to surgery (RR 1.10, 95% CI 1.02–1.19), having 1–2 hospitalizations in the year prior to surgery (RR 1.26, 95% CI 1.09–1.46), and having a Foley catheter at baseline (RR 1.39, 95% CI 1.29–1.50). An overwhelming majority (94%) of men who had a Foley at baseline and were alive 1 year later continued to have a Foley catheter, making this an unhelpful and unnecessary procedure in this population [35].
Conclusion
Consideration and evaluation of frailty are extremely important components to caring for the growing number of older individuals with lower urinary tract symptoms. While the study of frailty in relationship to specific lower urinary tract symptoms is in its infancy, there is a growing body of literature to begin to unravel the complexities associated with caring for frail older individuals with urinary incontinence, overactive bladder, underactive bladder, and benign prostatic hyperplasia. Further research is needed to both improve our understanding and our treatment strategies for this particularly vulnerable and at-risk population.
References
Papers of particular interest, published recently, have been highlighted as: • Of importance
Drach GW, Griebling TL. Geriatric urology. J Am Geriatr Soc. 2003;51(7 Suppl):S355–8.
Clayton JL. Special needs of older adults undergoing surgery. AORN J. 2008;87(3):557–70. quiz 571-554
van Iersel MB, Rikkert MG. Frailty criteria give heterogeneous results when applied in clinical practice. J Am Geriatr Soc. 2006;54(4):728–9.
Fried LP, Tangen CM, Walston J, et al. Frailty in older adults: evidence for a phenotype. J Gerontol A Biol Sci Med Sci. 2001;56(3):M146–56.
Mitnitski AB, Mogilner AJ, Rockwood K. Accumulation of deficits as a proxy measure of aging. ScientificWorldJournal. 2001;1:323–36.
Sternberg SA, Wershof Schwartz A, Karunananthan S, Bergman H, Mark Clarfield A. The identification of frailty: a systematic literature review. J Am Geriatr Soc. 2011;59(11):2129–38.
Velanovich V, Antoine H, Swartz A, Peters D, Rubinfeld I. Accumulating deficits model of frailty and postoperative mortality and morbidity: its application to a national database. J Surg Res. 2013;183(1):104–10.
Robinson TN, Eiseman B, Wallace JI, et al. Redefining geriatric preoperative assessment using frailty, disability and co-morbidity. Ann Surg. 2009;250(3):449–55.
Robinson TN, Wu DS, Pointer L, Dunn CL, Cleveland JC Jr, Moss M. Simple frailty score predicts postoperative complications across surgical specialties. Am J Surg. 2013;206(4):544–50.
Robinson TN, Wu DS, Sauaia A, et al. Slower walking speed forecasts increased postoperative morbidity and 1-year mortality across surgical specialties. Ann Surg. 2013;258(4):582–8. discussion 588-590
Rosier PF, Gajewski JB, Sand PK, Szabo L, Capewell A, Hosker GL. Executive summary: the International Consultation on Incontinence 2008—committee on: "dynamic testing"; for urinary incontinence and for fecal incontinence. Part 1: innovations in urodynamic techniques and urodynamic testing for signs and symptoms of urinary incontinence in female patients. Neurourol Urodyn. 2010;29(1):140–5.
Hannestad YS, Rortveit G, Sandvik H, Hunskaar S. A community-based epidemiological survey of female urinary incontinence: the Norwegian EPINCONT study. Epidemiology of incontinence in the county of Nord-Trondelag. J Clin Epidemiol. 2000;53(11):1150–7.
Stenzelius K, Mattiasson A, Hallberg IR, Westergren A. Symptoms of urinary and faecal incontinence among men and women 75+ in relations to health complaints and quality of life. Neurourol Urodyn. 2004;23(3):211–22.
DuBeau CE. Urinary incontinence. In: Medina-Walpole A, Pacala JT, Potter JF, editors. Geriatrics review syllabus: a core curriculum in geriatric medicine. 9th ed. New York: American Geriatrics Society; 2016.
• Wagg A, Gibson W, Ostaszkiewicz J, et al. Urinary incontinence in frail elderly persons: report from the 5th International Consultation on Incontinence. Neurourology and urodynamics. 2015;34(5):398–406. Evidence based guidelines on the management of frail older individuals with urinary incontinence
Thom DH, Haan MN, Van Den Eeden SK. Medically recognized urinary incontinence and risks of hospitalization, nursing home admission and mortality. Age Ageing. 1997;26(5):367–74.
Gibson W, Wagg A. New horizons: urinary incontinence in older people. Age Ageing. 2014;43(2):157–63.
Stenzelius K, Molander U, Odeberg J, et al. The effect of conservative treatment of urinary incontinence among older and frail older people: a systematic review. Age Ageing. 2015;44(5):736–44.
Resnick NM, Yalla SV, Laurino E. The pathophysiology of urinary incontinence among institutionalized elderly persons. N Engl J Med. 1989;320(1):1–7.
Abrams P, Cardozo L, Fall M, et al. The standardisation of terminology in lower urinary tract function: report from the standardisation sub-committee of the International Continence Society. Urology. 2003;61(1):37–49.
Suskind AM. The aging overactive bladder: a review of aging-related changes from the brain to the bladder. Current Bladder Dysfunction 2017.
Suskind AM, Quanstrom K, Zhao S, et al. Overactive bladder is strongly associated with frailty in older individuals. 2017.
• Samuelsson E, Odeberg J, Stenzelius K, et al. Effect of pharmacological treatment for urinary incontinence in the elderly and frail elderly: a systematic review. Geriatrics & gerontology international. 2015;15(5):521–34. Systematic review of 1038 abstracts and 309 texts looking at the efficacy of pharmacological treatment for urinary incontinence in the elderly and frail elderly.
Ouslander JG, Schnelle JF, Uman G, et al. Does oxybutynin add to the effectiveness of prompted voiding for urinary incontinence among nursing home residents? A placebo-controlled trial. J Am Geriatr Soc. 1995;43(6):610–7.
Lackner TE, Wyman JF, McCarthy TC, Monigold M, Davey C. Randomized, placebo-controlled trial of the cognitive effect, safety, and tolerability of oral extended-release oxybutynin in cognitively impaired nursing home residents with urge urinary incontinence. J Am Geriatr Soc. 2008;56(5):862–70.
Lackner TE, Wyman JF, McCarthy TC, Monigold M, Davey C. Efficacy of oral extended-release oxybutynin in cognitively impaired older nursing home residents with urge urinary incontinence: a randomized placebo-controlled trial. J Am Med Dir Assoc. 2011;12(9):639–47.
• Dubeau CE, Kraus SR, Griebling TL, et al. Effect of fesoterodine in vulnerable elderly subjects with urgency incontinence: a double-blind, placebo controlled trial. The Journal of Urology. 2014;191(2):395–404. Randomized, double-blind placebo controlled trial of fesoterodine in medically complex older individuals with urgency incontinence. This study is among the first to evalute the use of medical therapy in frail individuals and found that it was generally well tolerated.
Liao CH, Wang CC, Jiang YH. Intravesical onabotulinumtoxinA injection for overactive bladder patients with frailty, medical comorbidities or prior lower urinary tract surgery. Toxins (Basel). 2016;8(4):91.
Liao CH, Kuo HC. Increased risk of large post-void residual urine and decreased long-term success rate after intravesical onabotulinumtoxinA injection for refractory idiopathic detrusor overactivity. J Urol. 2013;189(5):1804–10.
Smith PP, Birder LA, Abrams P, Wein AJ, Chapple CR. Detrusor underactivity and the underactive bladder: symptoms, function, cause—what do we mean? ICI-RS think tank 2014. Neurourol Urodyn. 2016;35(2):312–7.
• Chancellor MB. The overactive bladder progression to underactive bladder hypothesis. International Urology and Nephrology. 2014;46(Suppl 1):S23–7. An interesting article discussing a theory on the progression of overactive to underactive bladder.
Platz EA, Smit E, Curhan GC, Nyberg LM, Giovannucci E. Prevalence of and racial/ethnic variation in lower urinary tract symptoms and noncancer prostate surgery in U.S. men. Urology. 2002;59(6):877–83.
Suskind AM, Walter LC, Jin C, et al. Impact of frailty on complications in patients undergoing common urological procedures: a study from the American College of Surgeons National Surgical Quality Improvement database. BJU Int. 2016;117(5):836–42.
Suskind AM, Jin C, Cooperberg MR, et al. Preoperative frailty is associated with discharge to skilled or assisted living facilities after urologic procedures of varying complexity. Urology. 2016;97:25–32.
Suskind AM, Walter LC, Zhao S, Finlayson E. Functional outcomes after transurethral resection of the prostate in nursing home residents. J Am Geriatr Soc 2016.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
Anne Suskind declares no potential conflicts of interest.
Human and Animal Rights and Informed Consent
This article does not contain any studies with human or animal subjects performed by any of the authors.
Funding
NIDDK K12 DK83021-07; K12 Urologic Research (KURe) Career Development Program, Pepper Center Research Career Development Core (RCDC) Advanced Scholar Award.
Additional information
This article is part of the Topical Collection on Lower Urinary Tract Symptoms & Voiding Dysfunction
Rights and permissions
About this article

Cite this article
Suskind, A.M. Frailty and Lower Urinary Tract Symptoms. Curr Urol Rep 18, 67 (2017). https://doi.org/10.1007/s11934-017-0720-9
Published:
DOI: https://doi.org/10.1007/s11934-017-0720-9