
Abstract
Purpose of Review
We outline the diverse processes contributing to bone mineralization and bone matrix maturation by describing two mouse models with bone strength defects caused by restricted deletion of the receptor tyrosine kinase ligand EphrinB2.
Recent Findings
Stage-specific EphrinB2 deletion differs in its effects on skeletal strength. Early-stage deletion in osteoblasts leads to osteoblast apoptosis, delayed initiation of mineralization, and increased bone flexibility. Deletion later in the lineage targeted to osteocytes leads to a brittle bone phenotype and increased osteocyte autophagy. In these latter mice, although mineralization is initiated normally, all processes involved in matrix maturation, including mineral accrual, carbonate substitution, and collagen compaction, progress more rapidly.
Summary
Osteoblasts and osteocytes control the many processes involved in bone mineralization; defining the contributing signaling activities may lead to new ways to understand and treat human skeletal fragilities.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Bone strength is determined both by its mass and its mechanical competence governed by relative collagen and mineral levels in the bone matrix. When mineralization is impaired, defects in bone strength are observed; the most extreme examples include osteogenesis imperfecta, hypophosphatasia, and vitamin D–deficient rickets; these are also associated with changes in bone mass and shape, likely secondary to the bone’s poor mechanical competence. There are also less severe defects in bone mineralization where bone shape is retained, but the overall mechanical strength is compromised. One related example is the early use of sodium fluoride therapy for osteoporosis; although it increased bone mass in animal models and increased bone mineral density in patients, it did not improve strength, likely because of changes in mineral structure brought about by incorporation of fluoride into the apatite structure [1]. This review will focus on recent advances describing the processes by which bone matrix matures and the stages in the osteoblast lineage controlling these processes, the latter as identified by mice with fragile skeletons due to stage-specific EphrinB2 deletion in osteoblasts and osteocytes.
Overview of Bone Formation and Mineralization Initiation
At its most basic level, bone formation involves two steps: (1) matrix rich in collagen type I (osteoid) is deposited by osteoblasts, and (2) the matrix becomes mineralized. Osteoblasts produce the organic component of bone matrix, mainly hydrated collagen type I (90%). The osteoblasts synthesize collagen I pro-alpha chains within their rough endoplasmic reticulum (ER) where it is post-translationally modified by ER-specific enzymes [2]. These modifications, including proline hydroxylation, ensure proper procollagen folding and secretion; following this modification, the processed chains are transported to the Golgi apparatus where they are assembled to form a triple helix. After carbohydrate molecules are added to the triple helix, the resulting procollagen structure is released from the Golgi through secretory granules then exported from the cell [3]. In the extracellular space, collagen I pro-peptides are cleaved and assembled into cross-striated microfibrils which merge into mature fibrils through axial and longitudinal growth [4]. Mature collagen fibrils are bundled after inter- and intramolecular covalent cross-linking between single collagen strands by lysyl oxidase [5].
After the bone matrix is deposited, it becomes mineralized. This occurs in two phases: primary and secondary mineralization. During the first days, bone mineral accumulates rapidly, reaching ~ 70% of total mineral levels (primary mineralization) [6]. Further gradual mineralization (secondary mineralization) follows, and can last for years [7], either until that region is resorbed during bone remodeling or until it reaches maximal mineral levels. In undecalcified bone sections, primary mineralization can be detected by fluorochrome labels such as tetracycline or calcein, which bind to calcium in the circulation and are incorporated into the bone as it mineralizes; sharp linear labels indicate rapid primary mineralization in lamellar bone (Fig. 1); slow secondary mineralization does not normally incorporate sufficient label to fluoresce. The distance between the labels indicates how much osteoid is deposited and how quickly it is mineralized (mineral appositional rate). Diffuse and less ordered labeling is seen during woven bone deposition, during embryonic bone development [8], at the growth plate primary spongiosa [9], and in conditions such as hypophosphatasia [10] and vitamin D deficiency [11].

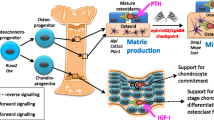
Specific roles of osteoblast lineage cells during their differentiation and some key differentiation markers: from stromal stem cell to osteocyte. Osteoblast differentiation commences when stromal stem cells express the commitment genes Runx2 and Osterix (Osx). The Osx1Cre transgene initiates gene recombination at LoxP sites from this stage of differentiation. Following their commitment, the cells differentiate into mature osteoblasts which migrate to the bone surface, where they produce the collagen-I-containing osteoid matrix, expressing Col1a1 and Col1a2 mRNAs and protein. Further differentiation into the late osteoblast stage that initiates mineralization is limited by the checkpoint between the tyrosine kinase receptor EphB4 and its ligand EphrinB2 which are both expressed throughout osteoblast differentiation. Some osteoblasts become embedded into the bone matrix, where they express Dmp1 and differentiate into osteocytes. The Dmp1Cre transgene initiates gene recombination at this stage of differentiation, and these cells play a role limiting bone matrix maturation
Initiation of Bone Mineralization by Late-Stage Osteoblasts: Blocking Differentiation Delays Initiation
The difference in fluorochrome label patterns between woven and lamellar bone is strong evidence that collagen bundle orientation influences mineral deposition. At a nanoscale level, parallel collagen fiber orientation within bundles is also important: characteristic hole zones between each collagen fiber leave space for mineral crystals to initially deposit and start growing [12]. Osteoblasts on the newly formed bone surface, and osteocytes within the bone matrix, also produce non-collagenous proteins such as osteocalcin, MEPE, PHOSPHO-1, and alkaline phosphatase, which initiate and regulate osteoid matrix mineralization [13,14,15,16]. Once mineralization is initiated, a biological apatite (bioapatite) provides bone matrix stiffness.
Our work on the receptor tyrosine kinase ligand EphrinB2 in osteoblasts has helped identify the osteoblast stage that initiates mineralization. EphrinB2 is a membrane-bound receptor tyrosine kinase ligand, which, with EphB4 (its main receptor), is expressed at all stages of osteoblast differentiation, including osteocytes [17, 18]. EphrinB2 is also expressed by osteoclasts [17, 18], and early studies indicated that EphrinB2 on the osteoclast cell surface interacted with EphB4 in osteoblasts when these cells were cultured together, providing a potential bidirectional communication pathway [17]. While this was an appealing model for intercellular communication, deletion of EphrinB2 in osteoclasts in vivo resulted in no detectable bone phenotype [6]; the rarity of direct contact of mature osteoclasts with osteoblasts was thought to be an explanation for why this interaction is not essential for normal bone mass [19]. The role of EphrinB2 expression and signaling in the osteoclast remains unclear, but is discussed at length elsewhere [19]. In contrast to the osteoclast-specific knockout, genetic deletion of EphrinB2 in osteoblasts and chondrocytes caused significant changes in bone formation and bone development, as well as a change in the way osteoblasts and chondrocytes support osteoclastogenesis [6, 20]. This indicates that the main role of EphrinB2 in bone is held within the osteoblast lineage, and will be discussed below. Those studies arose because EphrinB2 signaling depends on direct cell-to-cell contact, and osteoblasts work in connected teams to form bone matrix [21,22,23], leading us to hypothesize that EphrinB2/EphB4 signaling might regulate osteoblast differentiation and bone formation.
EphrinB2 expression in osteoblasts and osteocytes is rapidly upregulated by parathyroid hormone (PTH) and parathyroid hormone-related protein (PTHrP) [18, 24]. The former is an approved therapy to stimulate bone formation in post-menopausal osteoporosis, and the latter is a local bone formation stimulus secreted by osteoblasts [25] and osteocytes [26]. When cultured osteoblasts were treated with a pharmacological agent to block EphrinB2’s interaction with its receptor EphB4, late stages of osteoblast differentiation and mineralization were inhibited [18, 27, 28]. Non-collagenous proteins produced by both osteoblasts and osteocytes that regulate mineralization (osteocalcin, matrix extracellular phosphoglycoprotein (Mepe), and Dentin matrix acidic phosphoprotein 1 (Dmp1)) were downregulated, but earlier osteoblast markers, including alkaline phosphatase, were not. When EphrinB2:EphB4 inhibition was tested in vivo, early-stage osteoblast numbers were increased, but there were less late-stage osteoblasts [27], suggesting an EphrinB2:EphB4-dependent checkpoint through which osteoblasts must pass to reach late differentiation stages [27]. Functionally, a higher quantity of osteoid was observed, but the rate at which the primary mineralization front moved (measured by mineral appositional rate) did not change. This indicated that the stages of osteoblast differentiation controlling initiation of bone mineralization are beyond the EphrinB2:EphB4 checkpoint (Fig. 1).
A genetic approach confirmed this. Using the OsxCre transgene to target EphrinB2 deletion to the osteoblast lineage from the earliest stage of osteoblast commitment resulted in elevated osteoblast apoptosis. When PCR for stage-specific mRNA markers was used, this revealed EphrinB2-deficient osteoblasts could differentiate normally up to a certain point, but late osteoblast markers were significantly reduced. Functionally, osteoid deposition occurred, but initiation of mineralization was delayed, leading to a thickened osteoid seam [6]. With EphrinB2:EphB4 blockade [27] or with EphrinB2 genetic deletion in the osteoblast lineage [6], the mineralization front, while delayed in its formation, was still observed as two sharp lines. This is similar to osteomalacia in humans [29]. The speed at which mineralization is initiated and the amount of mineral deposited can therefore be regulated independently (Fig. 2). This contrasts with, for example, alkaline phosphatase deficiency (hypophosphatasia), in which mineralization is not only initiated slowly but also progresses slowly, and a diffuse mineralization front is observed (Fig. 2) [30]. In osteoblast-targeted EphrinB2 deficiency, only initiation of mineralization is delayed. Although this leads to very little change in bone shape and structure, it results in a material defect of increased bone flexibility [6]. This all confirmed that blocking late-stage osteoblast differentiation by targeting the EphrinB2:EphB4 checkpoint impaired initiation of mineralization [6, 19].

Changes in the bone matrix during maturation in healthy bone and in 3 types of defects in mouse periosteum (a) and human osteonal bone (b). Indicative regions are indicated by the red boxes in panels a and b. Healthy bone (c) is shown with osteoblasts on the osteoid surface, differentiating into osteocytes that change morphology, becoming more mature as the matrix is mineralized. Calcein labels (green) are recently bound during primary mineralization. As bone matures (deeper regions), the collagen helices become more compact, and mineral content and carbonate substitution within the bioapatite increase. EphrinB2 deletion in the osteoblast lineage from the committed progenitor stage (OsxCre.Efnb2f/f) in mice mimics osteomalacia (d). Osteoblast apoptosis and inhibition of late-stage differentiation leads to delayed initiation of mineralization (thick osteoid and narrow calcein labeling) but normal progression of mineral and collagen maturation. EphrinB2 deletion in osteocytes (Dmp1Cre.Efnb2f/f) has a contrasting effect (e), where mineralization is initiated normally, indicated by the calcein labels, but more mineral is deposited, more carbonate substitution occurs, and the collagen fibers become more compact. This high level of mineralization is also observed in patients with atypical femur fracture. In hypophosphatasia or hypophosphatemic or vitamin D-deficient rickets, and in vitamin receptor (VDR)-deficient and DMP1 null mice, the defect in mineralization is more severe (f). Mineralization initiation is delayed, and the level of mineral deposition is low, as indicated by diffuse labeling and paler shading. Carbonate substitution is reported to be high, but the impact on collagen cross-linking or compaction has not been investigated. Image of human osteonal bone was kindly provided by C.D. Thomas, The University of Melbourne, from the Melbourne Femur Research Collection
During osteoid deposition and primary mineralization, some osteoblasts are embedded within the collagen matrix and differentiate to form mature osteocytes. This concurrent process has a significant impact on mineralization. As these cells differentiate, their expression of mineralization factors increases. This includes Dmp1, Mepe, ectonucleotide pyrophosphatase/phosphodiesterase (Enpp1), and phosphate-regulating neutral endopeptidase (Phex) [31,32,33].
Since EphrinB2 is expressed in osteocytes [18], we sought to determine whether its deletion at this later differentiation stage also delayed bone mineralization initiation. We again used a targeted genetic approach, this time using the Dmp1Cre transgene to target genetic deletion to osteocytes and late osteoblasts (Dmp1Cre.Efnb2f/f mice). Although bone strength was impaired in this new model, the defect was different from that resulting from deletion earlier in the lineage (the Osx1Cre.Efnb2f/f model) [24]. Bones from the new mice exhibited no osteomalacia, and were not more flexible. Instead, Dmp1Cre.Efnb2f/f mice had brittle bones [24]. There were no changes in bone shape, no changes in osteoid deposition or mineral appositional rate, and no changes in mRNA levels for known genes that regulate initiation of mineralization (such as ALP, osteocalcin, Mepe, Dmp1) [24]. Instead, there was a change in later stages of the mineralization process. Understanding this requires a more detailed description of later events during bone mineralization which we will now describe.
Many Changes Occur in the Bone Matrix as Mineralization Progresses
Bone mineralization is a term encompassing many processes, not only mineral accumulation. Both during primary and secondary mineralization, mineral crystal size and shape increase, the bioapatite structure becomes more ordered and carbonate is incorporated into it, the collagen fibers become more condensed and cross-linked, and water content reduces. Although these changes can be observed during bone matrix maturation within lamellar structures such as osteons or mature murine cortical bone distant from the growth plate, there is much variation in the degree of mineralization at the tissue level. This is most readily observed by back-scattered electron microscopy of osteonal bone (see Fig. 2b) [34, 35]. Such heterogeneity results from bone remodeling, and strengthens bone by improving crack resistance [36]. A higher bone remodeling level results in lower total mineralization since secondary mineralization is truncated by bone resorption; rapidly remodeling bone is younger tissue [34, 37]. In contrast, when remodeling is low, for example, when anti-resorptive therapies like bisphosphonates are administered, more bone completes secondary mineralization uninterrupted and reaches the maximal mineralization level [38]. This effect of remodeling on bone mineral levels also explains why trabecular bone is less mature than cortical bone. In the growing cortex (including non-osteonal bone such as murine bone), less mature bone close to the growth plate is also more heterogeneous [39].
Increasing Mineralization
After mineralization is initiated, the amount of mineral compared with collagen continues to increase (mineral:matrix ratio). This has been described in many species, including mouse, rabbit, rat, baboon, and human cortical bone [7, 37, 40,41,42,43•]. High-resolution methods for FTIR, using synchrotron light sources coupled with timed fluorochrome labeling, allowed compositional analysis at specific ages of the bone matrix in mice and rabbits [7, 38, 44, 43•]. In these methods, fluorochrome labels defined the most recent surfaces on which bone is formed, and by measuring regions at increasing distance from the label, bone is measured at regions of greater “bone age” within the same sample. In both species, an initial rapid increase in mineral:matrix ratio was observed, followed by a lower slope in the more mature regions, consistent with initial rapid primary mineralization followed by slower mineral accumulation [7, 38, 44, 43•]. This is observed either while progressing inward from the periosteal or endosteal edges of growing bone [44, 43•] or while progressing outward from the center of an osteon undergoing bone formation [7, 38, 44].
Mineral Becomes More Crystalline
Mineral crystallinity is determined by a crystal’s degree of structural order, or perfection, compared with an ideal crystal lattice. Bone mineral (bioapatite) is a modified hydroxyapatite (Ca10(OH)2(PO4)6) structure which contains additional ions such as carbonate (CO3) and phosphate (HPO4), and is therefore less crystalline than pure hydroxyapatite. Bioapatite formation in bone (and in teeth, chitons, and corals) includes an initial transitory phase in which an amorphous crystal is formed; this disordered mineral is sufficiently flexible to be molded by matrix proteins (such as collagen) into the shape required [45]. As mineral crystals mature within the bone matrix, the structure becomes more crystalline through multiple processes.
The bone crystal surface initially contains a less ordered non-apatitic hydrated layer surrounding the stable, apatitic domain; this contains labile carbonate and phosphate ions. As bone matures, this non-apatitic proportion decreases and the stable, apatitic proportion increases [46]. In solution, amorphous calcium phosphate is unstable and spontaneously forms carbonated hydroxyapatite, after passing through an intermediate unstable octacalcium stage, which is hydrolyzed to form hydroxyapatite [47, 48]. Similar mineral maturation processes occur during initial mineralization in multiple vertebrate species [49]. Raman spectroscopy revealed both amorphous calcium phosphate and octacalcium phosphate are present during suture mineralization in embryonic calvaria organ cultures [50]. These bands became less prominent as bone matured, consistent with very early suggestions that amorphous calcium phosphate precipitates and octacalcium are precursors for mature bioapatite [51, 52]. When crystallinity and crystallite size were assessed with increasing bone age from the growing murine periosteum, these parameters increased during primary and secondary mineralization and, like mineral:matrix ratio, reached a plateau in older bone [43•]. Although increased crystallinity improves material strength, excessive crystallinity is also linked to fragile bones [53], but the mechanisms by which crystallinity contributes to mechanical strength remain unclear [54]. Mineral crystallinity is understood to be at least partially controlled by the collagen matrix, and although factors released by osteoblasts and osteocytes may contribute, these are yet to be fully defined.
Carbonate Substitution
As bioapatite ages, carbonate (CO32−) ions are incorporated into the crystal lattice [55] at three different sites. Carbonate ions incorporated into bioapatite, even in the absence of collagen, enable formation of the characteristic plate-like crystals of bone [56•] which contribute to bone strength at the nanoscale level. Carbonate type A substitutes for monovalent anionic sites (OH−), while carbonate type B substitutes for trivalent anionic sites (PO43−) and a labile carbonate site which diminishes during human osteonal bone maturation [42]. Type B carbonate substitution is the most common in bone [57, 58]. Early studies also showed increased carbonate substitution with increasing maturity of apatite crystals in vitro [59], but this occurs much more slowly and does not reach the same level as observed in vivo [60]. When measured in adult murine bone tissue, the carbonate:phosphate ratio increases with bone age, both from the periosteum in growing mice [43•] and in rabbit bone from the endocortical and osteonal surfaces [44]. This increase correlated very strongly with the increase in mineral:matrix ratio, and reached a plateau in mature bone [43•, 44]. Although carbonate substitution increases with mineralization within normal bone tissue, in the Hyp mouse, a model of hypophosphatemic rickets, carbonate:phosphate levels are elevated even though mineralization is defective [61], indicating that these are not always co-regulated.
The increase in carbonate substitution with matrix maturation is consistent with early observations that carbonate content is higher in bone samples from older animals, noted in chicken [59], rat, and bovine cortical bone [62, 63]. This increase in carbonate level has been postulated to contribute to the weaker strength of aged bone, but mechanisms by which this occurs are elusive.
Collagen Cross-linking and Compression Increase
As bone matrix matures and becomes more mineralized, two changes occur in bone collagen: it becomes more cross-linked and more compact.
Collagen’s intermolecular cross-linking pattern contributes to bone’s tensile strength and elasticity [64]. Collagen cross-linking within the bone matrix can be quantified by two specific cross-links in situ, pyridinoline (Pyr) and dehydro-dihydroxylysino-norleucine (deH-DHLNL), Pyr:deH-DHLNL (1660:1690 ratio by FTIRM) [64]. In both human trabecular bone [65] and murine cortical bone [43•], there is a gradual increase in collagen cross-linking with increasing bone age.
Collagen fiber compaction was detected in murine periosteal and rabbit endocortical bone by a gradual reduction in amide I:II ratio which reached a plateau in the most mature regions of bone [43•, 44]. The amide I peak reflects vibration of C=O bonds running perpendicular to the collagen helical axis, and the amide II peak reflects C–N bond vibration along the collagen fiber axis [66]. The amide I:II ratio therefore reflects the proportional change in perpendicular (amide I) to parallel (amide II) stretch of the collagen triple helix. This suggests collagen fibers are subject to steric hindrance in their perpendicular direction as mineral accumulates, making them narrower at a molecular level. This is likely due to mineral crystals growing and wrapping more tightly around the collagen fibers [67•].
Osteocytes Within the Matrix Change Their Gene Expression Pattern and Morphology
As the bone matrix matures, osteocytes within the matrix also mature. This is reflected in changes in gene expression, a reduction in cell motility, an increase in dendritic length, and a reduction in cell body size (reviewed in [32]). The very many osteocyte dendritic processes within the skeleton (3.7 trillion) are a major component of the bone matrix, and the large surface area of the osteocyte lacunocanalicular network (215 m2) provides ample space for bone mineral exchange and regulation [68•].
It is well known that genes expressed by osteocytes regulate mineralization [32]. And indeed, areas with higher osteocyte canalicular density are more mineralized than regions with less canals [69], supporting the idea that the network contributes to mineralization within the bone matrix itself. Osteocytes also appear to respond to changes in their surrounding matrix as the matrix matures and becomes more mineralized. If mineralization is delayed pharmacologically, osteocyte maturation is also delayed; this has been shown by administration of a modified bisphosphonate which delayed mineralization and osteocytes in the unmineralized matrix retained an early osteoid osteocyte phenotype: they did not express sclerostin and retained a large cytoplasm, with extensive protein-producing Golgi [70]. This suggests osteocytes sense mineralization levels in the surrounding matrix, and these signals may tell the osteocyte when to “switch off” mineral production. The mechanisms by which osteocytes might sense mineral levels remain unknown. It may be sensed by a change in fluid pressure within the canalicular network, or there may be a change in the way the cell body interacts with the lacunar walls or the way the dendrites interact with the canalicular walls.
Water Content Reduces
As the osteoid matrix is mineralized, water content also reduces. Bone contains water within the lacunocanalicular and Haversian systems, but there is also water loosely bound to the bone matrix, and tightly bound within collagen fibers and hydroxyapatite crystals (see [71] for an excellent overview). It has been suggested that, in addition to the actions of collagen and carbonate, water bound to the bioapatite surface may play a role early in mineralization to orient the mineral crystals through an amorphous, presumably labile, calcium phosphate layer [72].
Accelerated Matrix Maturation When EphrinB2 Was Deleted in Osteocytes
Changes in these aspects of matrix maturation were observed in the brittle Dmp1Cre.Efnb2f/f bones. Although there was no change in mineral appositional rate, when the bones of these mice were assessed by sFTIRM, the bone exhibited more rapid matrix maturation, indicated by higher carbonate substitution, greater mineral deposition, and higher collagen compaction [24] (Fig. 2). Very high mineral levels were deposited in the matrix as soon as mineralization was initiated. In addition, carbonate substitution and collagen compaction were also accelerated, further supporting the link between the three processes. These changes in the bone matrix had sufficient impact to change bone strength without changing the skeletal shape or structure; this appears to be the first report in a mouse model of such an event.
Another indicator of accelerated bone matrix maturation in Dmp1Cre.Efnb2f/f bone was a greater osteocyte lacunar density, and reduction in osteocyte cell body size [24]. Dmp1Cre targets late osteoblasts when they become embedded within the newly formed osteoid [73]. This may indicate more rapid osteocyte incorporation into the bone matrix; such activity may promote mineral accumulation and carbonate incorporation in Dmp1Cre.Efnb2f/f bones, but whether this causes or results from the increased mineralization is not known.
The different strength defects between the flexible OsxCre.Efnb2f/f bones with delayed initiation of mineralization and brittle highly mineralized Dmp1Cre.Efnb2f/f bones sheds new light on how specific stages of osteoblast/osteocyte differentiation regulate bone mineralization (Fig. 1). Delayed initiation of mineralization in both OsxCre.Efnb2f/f mice [6] and mice with systemic EphrinB2:EphB4 inhibition [27] indicates that initiation is controlled by osteoblasts differentiated beyond the early stage of OsxCre expression and beyond the EphrinB2:EphB4 checkpoint. In Dmp1Cre.Efnb2f/f mice, osteoblasts survived past the checkpoint, and initiation of mineralization was normal. The osteoblast stage controlling initiation timing is therefore not only after the EphrinB2:EphB4 checkpoint, but is before Dmp1Cre-targeted EphrinB2 deletion. The stage of differentiation targeted for EphrinB2 deletion in the Dmp1Cre.Efnb2f/f mouse therefore controls mineral accumulation (Fig. 2). Although Dmp1Cre expression has been reported by lineage tracing in osteoblasts, when we used DMP1-GFP–based sorting of osteoblasts and matrix-embedded osteocytes from our mouse model, we observed no EphrinB2 deletion in less mature cells [24]. We suggest that matrix-embedded osteocytes are the stage at which EphrinB2 is deleted in Dmp1Cre.Efnb2f/f mice.
Compositional Defects in Human Skeletal Conditions
In humans, major defects in bone compositional strength can result from defective collagen deposition (as in osteogenesis imperfecta) or delayed initiation of mineralization (as in osteomalacia, hypophosphatasia, or rickets) (Fig. 1). Are there conditions in humans similar to the Dmp1Cre.Efnb2f/f mouse, where mineralization is initiated normally, but matrix maturation is accelerated? Although osteogenesis imperfecta is associated with increased brittleness and increased mineralization, these conditions are also associated with changes in bone shape, which we did not observe in the Dmp1Cre.Efnb2f/f mouse. There are at least three human conditions in which bone shape is normal, but mineralization level may be increased.
One possibility is that the Dmp1Cre.Efnb2f/f mouse is similar to patients with fragility fractures who do not have clinically diagnosed osteoporosis on the basis of areal bone mineral density (BMD) scans. Although areal BMD is used as a standard screening tool for osteoporosis, it is becoming clear that it has low sensitivity as a predictor of fracture risk, with recent estimates suggesting most patients with fragility fracture do not have clinically defined osteoporosis (T score < − 2.5 by areal BMD) [74•]. This suggests there may be a diversity of bone fragility phenotypes—some can be detected by areal BMD scans, but others may relate to (for example) high mineral:matrix ratio, low mineral:matrix ratio [75], or high carbonate:mineral ratio [76].
A clinical condition recently associated with high mineral:matrix ratio is atypical femoral fracture (AFF) experienced by a subset of patients undergoing bisphosphonate-based therapies for osteoporosis. It is associated with anti-resorptive therapies but only observed very rarely. Evidence is accumulating that AFF patients may have an intrinsic defect in bone composition: (1) there appears to be underlying genetic susceptibility [77], (2) Asian women have a 6-fold higher risk of AFF [78] and higher tissue mineral density [79] than Caucasian women, and (3) when bone from fracture sites of patients with AFF was assessed by FTIRM it was found to have a higher mineral:matrix ratio than bone from women with typical osteoporotic fractures [80•]. Also contributing to AFF is a decrease in heterogeneity resulting from the reduction in bone turnover caused by bisphosphonate treatment [81]; this too was confirmed in bone from AFF patients [80•]. The more homogenous material was associated with greater crack propagation, consistent with the increased fragility and unusual transverse fracture pattern [80•]. The underlying cellular defect leading to high mineral deposition in AFF has not been defined. If it is similar to the defect in mineral deposition in the Dmp1Cre.Efnb2f/f mice, understanding how this pathway regulates bone mineralization may be helpful for predicting susceptibility to this condition and provide ways to manage it.
It is not clear yet whether the high mineral:matrix ratio observed in patients with AFF exists prior to bisphosphonate treatment. It is becoming widely accepted that anti-resorptive therapies, by suppressing remodeling, extend the period in which secondary mineralization can occur [38]. This leads to an increase in bone mineral density reflecting an increase in mineral content rather than an increase in bone mass [81, 82]. If high mineral:matrix ratio in AFF patients precedes therapy, the bisphosphonate treatment may exacerbate the underlying condition.
Osteocyte-Derived Matrix Vesicles and Autophagic Processes in Mineralization
What is the primary event causing increased matrix maturation in Dmp1Cre.Efnb2f/f mice? It appears to be a defect initiated by EphrinB2-deficient osteocytes which have elevated exocytic matrix vesicle production and elevated autophagy both in vivo and in vitro.
Mineral incorporation within the extracellular matrix remains poorly defined. The longest standing model is that exocytotic vesicles (matrix vesicles) bud from cells facing the matrix (osteoblasts, or in mineralizing cartilage, hypertrophic chondrocytes). These vesicles then accumulate ions outside the cell and rupture, releasing mineral into the surrounding matrix [83, 84]. The amorphous mineral formed is subsequently nucleated (to ordered crystals, see above); the process is driven by contact with collagen, and by secreted nucleators [85, 86]. Matrix vesicles were originally reported to lack mineral and to accumulate poorly crystalline mineral only after budding from the cell and becoming immobilized in the collagen matrix [87]. In contrast, there is a body of data from in vitro studies showing calcium phosphate crystals residing within intracellular vesicles of osteoblast-like cells and their release as mineral-containing matrix vesicles [85, 86, 88]. More recently, calcium phosphate was detected within mitochondrial granules and intracellular vesicles transporting material to the ECM in osteoblasts, suggesting calcium is stored in and transported from the mitochondria during mineralization [89]. To date, all studies of matrix vesicles are limited to studies in cultured osteoblasts, chondrocytes, or mesenchymal cells. This means we do not yet know whether the same processes occur in osteocytes or whether they occur in bone in vivo. Osteocytes are likely to release mineral into the surrounding lacunocanalicular fluid where it is incorporated during secondary mineralization. This is also a possible mechanism by which mineral is deposited after osteocytic osteolysis in lactation [90], including in mildly vitamin D–deficient mice which form very thick osteoid seams during lactation that are rapidly re-mineralized [91]. Our finding that Dmp1Cre.Efnb2f/f osteocytes show increased exocytic budding would be consistent with these osteocytes releasing more matrix vesicles into their surrounding matrix, thereby contributing to the elevated mineralization level independent of initiation rate [24].
Osteoblasts could use autophagosomes as vehicles for apatite crystal secretion into the extracellular space via exocytosis (i.e., secretory autophagy). This suggestion was based on detection of mineral within autophagosomes in cultured osteosarcoma cells [92]. Indeed, when the hypermineralized bones of Dmp1Cre.Efnb2f/f mice were analyzed by RNAseq, although no known mineralization genes were regulated, the top 30 genes dysregulated included 10 genes previously associated with autophagic processes [24]. This suggests another possible mechanism by which mineral release by osteocytes may be controlled.
Autophagy is a group of lysosome-based recycling and secretory processes; these contribute to many cellular functions, including adaptation to starvation, protein secretion, and elimination of intracellular microbes [93]. Autophagy can be categorized into two classes, canonical degradative macro-autophagy, which involves Atg proteins, and micro-autophagy (including mito-phagy and ER-phagy), which can be Atg-independent. Autophagy increases during osteoblast differentiation [92], consistent with a role in mineralization. Atg family member mRNA levels were not changed in Dmp1Cre.Efnb2f/f bones, suggesting EphrinB2 deficiency does not modify canonical degradative macro-autophagy. Rather, the genes dysregulated in EphrinB2-deficient bones are associated with a subset of autophagic processes including mitophagy (degradation of mitochondria) and ER-phagy (micro-autophagic degradation of the ER); in addition, autophagosomes in Dmp1Cre.Efnb2f/f osteocytes contained degraded ER [24]. This is consistent with ER and mitochondria being involved in producing and releasing mineral-containing matrix vesicles [89]. Whether osteocyte-derived matrix vesicles mediating secondary mineralization are distinct from those released by osteoblasts is not known; nor is it known yet whether matrix vesicles from EphrinB2-deficient osteocytes differ from wild type in their mineral content or interaction with the collagen matrix.
Concluding Statements
Bone fragility may include conditions where bone volume is normal, but the strength of the matrix itself is defective; this is highlighted by the two models we have discussed here. Understanding how bone mineralization occurs and how both osteoblasts and osteocytes control the multiple processes involved in bone matrix maturation is a field ripe for exploration.
Ultimately, by identifying how these cells contribute to mineralization and matrix maturation, we may identify ways to increase bone strength “from within” without the need to form new bone tissue. This could be particularly helpful in those with fragility caused, not by low bone mass, but by alterations in bone composition. Could mineral release by osteocytes be manipulated in the adult skeleton? This needs to be explored further, but presents an exciting possibility which could make use of methods currently in development to target therapies specifically to osteocytes. Such methods could regulate matrix vesicle release by osteocytes in conditions where bone mineral content is too low or too high.
References
Papers of particular interest, published recently, have been highlighted as: • Of importance
Everett ET. Fluoride’s effects on the formation of teeth and bones, and the influence of genetics. J Dent Res. 2011;90(5):552–60. https://doi.org/10.1177/0022034510384626.
Myllyharju J. Intracellular post-translational modifications of collagens. In: Brinckmann J, Notbohm H, Müller PK, editors. Collagen: primer in structure, processing and assembly. Berlin, Heidelberg: Springer Berlin Heidelberg; 2005. p. 115–47.
Leblond CP. Synthesis and secretion of collagen by cells of connective tissue, bone, and dentin. Anat Rec. 1989;224(2):123–38. https://doi.org/10.1002/ar.1092240204.
Lamande SR, Bateman JF. Procollagen folding and assembly: the role of endoplasmic reticulum enzymes and molecular chaperones. Semin Cell Dev Biol. 1999;10(5):455–64. https://doi.org/10.1006/scdb.1999.0317.
Mouw JK, Ou G, Weaver VM. Extracellular matrix assembly: a multiscale deconstruction. Nat Rev Mol Cell Biol. 2014;15(12):771–85. https://doi.org/10.1038/nrm3902.
Tonna S, Takyar FM, Vrahnas C, Crimeen-Irwin B, Ho PW, Poulton IJ, et al. EphrinB2 signaling in osteoblasts promotes bone mineralization by preventing apoptosis. FASEB J. 2014;28(10):4482–96. https://doi.org/10.1096/fj.14-254300.
Fuchs RK, Allen MR, Ruppel ME, Diab T, Phipps RJ, Miller LM, et al. In situ examination of the time-course for secondary mineralization of Haversian bone using synchrotron Fourier transform infrared microspectroscopy. Matrix Biol. 2008;27(1):34–41. https://doi.org/10.1016/j.matbio.2007.07.006.
Wu JY, Aarnisalo P, Bastepe M, Sinha P, Fulzele K, Selig MK, et al. Gsalpha enhances commitment of mesenchymal progenitors to the osteoblast lineage but restrains osteoblast differentiation in mice. J Clin Invest. 2011;121(9):3492–504. https://doi.org/10.1172/JCI46406.
Poulton IJ, McGregor NE, Pompolo S, Walker EC, Sims NA. Contrasting roles of leukemia inhibitory factor in murine bone development and remodeling involve region-specific changes in vascularization. J Bone Miner Res. 2012;27(3):586–95. https://doi.org/10.1002/jbmr.1485.
Weinstein RS, Whyte MP. Heterogeneity of adult hypophosphatasia report of severe and mild cases. JAMA Intern Med. 1981;141(6):727–31. https://doi.org/10.1001/archinte.1981.00340060035010.
Amling M, Priemel M, Holzmann T, Chapin K, Rueger JM, Baron R, et al. Rescue of the skeletal phenotype of vitamin D receptor-ablated mice in the setting of normal mineral ion homeostasis: formal histomorphometric and biomechanical analyses1. Endocrinology. 1999;140(11):4982–7. https://doi.org/10.1210/endo.140.11.7110.
Roschger P, Blouin S, Paschalis E, Gamsjaeger S, Klaushofer K, Misof B. Bone Material Quality. In: Pietschmann P. Principles of bone and joint research. Springer International Publishing. 2017;1–15. https://doi.org/10.1007/978-3-319-58955-8_1.
Houston B, Stewart AJ, Farquharson C. PHOSPHO1-a novel phosphatase specifically expressed at sites of mineralisation in bone and cartilage. Bone. 2004;34(4):629–37. https://doi.org/10.1016/j.bone.2003.12.023.
Ling Y, Rios HF, Myers ER, Lu Y, Feng JQ, Boskey AL. DMP1 depletion decreases bone mineralization in vivo: an FTIR imaging analysis. J Bone Miner Res. 2005;20(12):2169–77. https://doi.org/10.1359/JBMR.050815.
Gowen LC, Petersen DN, Mansolf AL, Qi H, Stock JL, Tkalcevic GT, et al. Targeted disruption of the osteoblast/osteocyte factor 45 gene (OF45) results in increased bone formation and bone mass. J Biol Chem. 2003;278(3):1998–2007. https://doi.org/10.1074/jbc.M203250200.
Poole KE, van Bezooijen RL, Loveridge N, Hamersma H, Papapoulos SE, Lowik CW, et al. Sclerostin is a delayed secreted product of osteocytes that inhibits bone formation. FASEB J. 2005;19(13):1842–4.
Zhao C, Irie N, Takada Y, Shimoda K, Miyamoto T, Nishiwaki T, et al. Bidirectional EphrinB2-EphB4 signaling controls bone homeostasis. Cell Metab. 2006;4(2):111–21.
Allan EH, Hausler KD, Wei T, Gooi JH, Quinn JM, Crimeen-Irwin B, et al. EphrinB2 regulation by PTH and PTHrP revealed by molecular profiling in differentiating osteoblasts. J Bone Miner Res. 2008;23(8):1170–81. https://doi.org/10.1359/jbmr.080324.
Vrahnas C, Sims NA. EphrinB2 signalling in osteoblast differentiation, bone formation and endochondral ossification. Curr Mol Biol Rep. 2015;1(4):148–56. https://doi.org/10.1007/s40610-015-0024-0.
Tonna S, Poulton IJ, Taykar F, Ho PW, Tonkin B, Crimeen-Irwin B, et al. Chondrocytic EphrinB2 promotes cartilage destruction by osteoclasts in endochondral ossification. Development. 2016;143(4):648–57. https://doi.org/10.1242/dev.125625.
Ecarot-Charrier B, Glorieux FH, van der Rest M, Pereira G. Osteoblasts isolated from mouse calvaria initiate matrix mineralization in culture. J Cell Biol. 1983;96(3):639–43.
Abe Y, Akamine A, Aida Y, Maeda K. Differentiation and mineralization in osteogenic precursor cells derived from fetal rat mandibular bone. Calcif Tissue Int. 1993;52(5):365–71.
Gerber I, ap Gwynn I. Influence of cell isolation, cell culture density, and cell nutrition on differentiation of rat calvarial osteoblast-like cells in vitro. Eur Cell Mater. 2001;2:10–20.
Vrahnas C, Blank M, Dite TA, Tatarczuch L, Ansari N, Crimeen-Irwin B, et al. Increased autophagy in EphrinB2 deficient osteocytes is associated with hypermineralized, brittle bones. Nat Commun. In Press. https://doi.org/10.1038/s41467-019-11373-9.
Miao D, Li J, Xue Y, Su H, Karaplis AC, Goltzman D. Parathyroid hormone-related peptide is required for increased trabecular bone volume in parathyroid hormone-null mice. Endocrinology. 2004;145(8):3554–62. https://doi.org/10.1210/en.2003-1695.
Ansari N, Ho PW, Crimeen-Irwin B, Poulton IJ, Brunt AR, Forwood MR, et al. Autocrine and paracrine regulation of the murine skeleton by osteocyte-derived parathyroid hormone-related protein. J Bone Miner Res. 2018;33(1):137–53. https://doi.org/10.1002/jbmr.3291.
Takyar FM, Tonna S, Ho PW, Crimeen-Irwin B, Baker EK, Martin TJ, et al. EphrinB2/EphB4 inhibition in the osteoblast lineage modifies the anabolic response to parathyroid hormone. J Bone Miner Res. 2013;28(4):912–25. https://doi.org/10.1002/jbmr.1820.
Martin TJ, Allan EH, Ho PW, Gooi JH, Quinn JM, Gillespie MT, et al. Communication between EphrinB2 and EphB4 within the osteoblast lineage. Adv Exp Med Biol. 2010;658:51–60. https://doi.org/10.1007/978-1-4419-1050-9_6.
Melsen F, Mosekilde L. Trabecular bone mineralization lag time determined by tetracycline double-labeling in normal and certain pathological conditions. Acta Pathol Microbiol Scand A Pathol. 1980;88(2):83–8.
Millán JL, Whyte MP. Alkaline phosphatase and hypophosphatasia. Calcif Tissue Int. 2016;98(4):398–416. https://doi.org/10.1007/s00223-015-0079-1.
Kalajzic I, Braut A, Guo D, Jiang X, Kronenberg MS, Mina M, et al. Dentin matrix protein 1 expression during osteoblastic differentiation, generation of an osteocyte GFP-transgene. Bone. 2004;35(1):74–82. https://doi.org/10.1016/j.bone.2004.03.006.
Dallas SL, Bonewald LF. Dynamics of the transition from osteoblast to osteocyte. Ann N Y Acad Sci. 2010;1192:437–43. https://doi.org/10.1111/j.1749-6632.2009.05246.x.
Paic F, Igwe JC, Nori R, Kronenberg MS, Franceschetti T, Harrington P, et al. Identification of differentially expressed genes between osteoblasts and osteocytes. Bone. 2009;45(4):682–92. https://doi.org/10.1016/j.bone.2009.06.010.
Boivin G, Meunier PJ. Changes in bone remodeling rate influence the degree of mineralization of bone. Connect Tissue Res. 2002;43(2–3):535–7.
Roschger P, Gupta HS, Berzlanovich A, Ittner G, Dempster DW, Fratzl P, et al. Constant mineralization density distribution in cancellous human bone. Bone. 2003;32(3):316–23.
Granke M, Makowski AJ, Uppuganti S, Nyman JS. Prevalent role of porosity and osteonal area over mineralization heterogeneity in the fracture toughness of human cortical bone. J Biomech. 2016;49(13):2748–55. https://doi.org/10.1016/j.jbiomech.2016.06.009.
Paschalis EP, Betts F, DiCarlo E, Mendelsohn R, Boskey AL. FTIR microspectroscopic analysis of normal human cortical and trabecular bone. Calcif Tissue Int. 1997;61(6):480–6.
Fuchs RK, Faillace ME, Allen MR, Phipps RJ, Miller LM, Burr DB. Bisphosphonates do not alter the rate of secondary mineralization. Bone. 2011;49(4):701–5. https://doi.org/10.1016/j.bone.2011.05.009.
Enlow DH. A study of the post-natal growth and remodeling of bone. Am J Anat. 1962;110:79–101. https://doi.org/10.1002/aja.1001100202.
Donnelly E, Boskey AL, Baker SP, van der Meulen MC. Effects of tissue age on bone tissue material composition and nanomechanical properties in the rat cortex. J Biomed Mater Res A. 2010;92(3):1048–56. https://doi.org/10.1002/jbm.a.32442.
Gourion-Arsiquaud S, Burket JC, Havill LM, DiCarlo E, Doty SB, Mendelsohn R, et al. Spatial variation in osteonal bone properties relative to tissue and animal age. J Bone Miner Res. 2009;24(7):1271–81. https://doi.org/10.1359/jbmr.090201.
Paschalis EP, DiCarlo E, Betts F, Sherman P, Mendelsohn R, Boskey AL. FTIR microspectroscopic analysis of human osteonal bone. Calcif Tissue Int. 1996;59(6):480–7.
• Vrahnas C, Pearson TA, Brunt AR, Forwood MR, Bambery KR, Tobin MJ, et al. Anabolic action of parathyroid hormone (PTH) does not compromise bone matrix mineral composition or maturation. Bone. 2016;93:146–54. https://doi.org/10.1016/j.bone.2016.09.022 This work provides a detailed study of the changes in bone matrix that occur with maturation, including accumulation of mineral, carbonate substitution, collagen compaction, and collagen cross-linking, identified by analyzing newly formed periosteal murine bone by synchrotron-based Fourier-transform infrared microspectrosopy.
Vrahnas C, Buenzli PR, Pearson TA, Pennypacker BL, Tobin MJ, Bambery KR, et al. Differing effects of parathyroid hormone, alendronate, and odanacatib on bone formation and on the mineralization process in intracortical and endocortical bone of ovariectomized rabbits. Calcif Tissue Int. 2018;103(6):625–37. https://doi.org/10.1007/s00223-018-0455-8.
Weiner S, Sagi I, Addadi L. Choosing the crystallization path less traveled. Science. 2005;309(5737):1027–8. https://doi.org/10.1126/science.1114920.
Farlay D, Panczer G, Rey C, Delmas PD, Boivin G. Mineral maturity and crystallinity index are distinct characteristics of bone mineral. J Bone Miner Metab. 2010;28(4):433–45. https://doi.org/10.1007/s00774-009-0146-7.
Brown WE, Smith JP, Lehr JR, Frazier AW. Octacalcium phosphate and hydroxyapatite: crystallographic and chemical relations between octacalcium phosphate and hydroxyapatite. Nature. 1962;196(4859):1050–5. https://doi.org/10.1038/1961050a0.
Christoffersen J, Christoffersen MR, Kibalczyc W, Andersen FA. A contribution to the understanding of the formation of calcium phosphates. J Cryst Growth. 1989;94(3):767–77. https://doi.org/10.1016/0022-0248(89)90102-4.
Mahamid J, Aichmayer B, Shimoni E, Ziblat R, Li C, Siegel S, et al. Mapping amorphous calcium phosphate transformation into crystalline mineral from the cell to the bone in zebrafish fin rays. Proc Natl Acad Sci U S A. 2010;107(14):6316–21. https://doi.org/10.1073/pnas.0914218107.
Crane NJ, Popescu V, Morris MD, Steenhuis P, Ignelzi MA Jr. Raman spectroscopic evidence for octacalcium phosphate and other transient mineral species deposited during intramembranous mineralization. Bone. 2006;39(3):434–42. https://doi.org/10.1016/j.bone.2006.02.059.
Eanes ED, Meyer JL. The maturation of crystalline calcium phosphates in aqueous suspensions at physiologic pH. Calcif Tissue Res. 1977;23(1):259–69. https://doi.org/10.1007/BF02012795.
Brown WE. Crystal growth of bone mineral. 1966;44:205–220.
Faibish D, Ott SM, Boskey AL. Mineral changes in osteoporosis: a review. Clin Orthop Relat Res. 2006;443:28–38. https://doi.org/10.1097/01.blo.0000200241.14684.4e.
Unal M, Creecy A, Nyman JS. The role of matrix composition in the mechanical behavior of bone. Curr Osteoporos Rep. 2018;16(3):205–15. https://doi.org/10.1007/s11914-018-0433-0.
Zapanta-Legeros R. Effect of carbonate on the lattice parameters of apatite. Nature. 1965;206(4982):403–4. https://doi.org/10.1038/206403a0.
• Deymier AC, Nair AK, Depalle B, Qin Z, Arcot K, Drouet C, et al. Protein-free formation of bone-like apatite: new insights into the key role of carbonation. Biomaterials. 2017;127:75–88. https://doi.org/10.1016/j.biomaterials.2017.02.029 Evidence that carbonate, independent of collagen, contributes to the characteristic shape of bone mineral crystal formation.
Rey C, Combes C, Drouet C, Glimcher MJ. Bone mineral: update on chemical composition and structure. Osteoporos Int. 2009;20(6):1013–21. https://doi.org/10.1007/s00198-009-0860-y.
Rey C, Collins B, Goehl T, Dickson IR, Glimcher MJ. The carbonate environment in bone mineral: a resolution-enhanced Fourier transform infrared spectroscopy study. Calcif Tissue Int. 1989;45(3):157–64. https://doi.org/10.1007/BF02556059.
Rey C, Renugopalakrishnan V, Collins B, Glimcher MJ. Fourier transform infrared spectroscopic study of the carbonate ions in bone mineral during aging. Calcif Tissue Int. 1991;49(4):251–8.
Rey C, Kim HM, Gerstenfeld L, Glimcher MJ. Structural and chemical characteristics and maturation of the calcium-phosphate crystals formed during the calcification of the organic matrix synthesized by chicken osteoblasts in cell culture. J Bone Miner Res. 1995;10(10):1577–88. https://doi.org/10.1002/jbmr.5650101020.
Macica CM, King HE, Wang M, McEachon CL, Skinner CW, Tommasini SM. Novel anatomic adaptation of cortical bone to meet increased mineral demands of reproduction. Bone. 2016;85:59–69. https://doi.org/10.1016/j.bone.2015.12.056.
Legros R, Balmain N, Bonel G. Age-related changes in mineral of rat and bovine cortical bone. Calcif Tissue Int. 1987;41(3):137–44.
Akkus O, Adar F, Schaffler MB. Age-related changes in physicochemical properties of mineral crystals are related to impaired mechanical function of cortical bone. Bone. 2004;34(3):443–53. https://doi.org/10.1016/j.bone.2003.11.003.
Paschalis EP, Verdelis K, Doty SB, Boskey AL, Mendelsohn R, Yamauchi M. Spectroscopic characterization of collagen cross-links in bone. J Bone Miner Res Off J Am Soc Bone Miner Res. 2001;16(10):1821–8. https://doi.org/10.1359/jbmr.2001.16.10.1821.
Paschalis EP, Shane E, Lyritis G, Skarantavos G, Mendelsohn R, Boskey AL. Bone fragility and collagen cross-links. J Bone Miner Res. 2004;19(12):2000–4. https://doi.org/10.1359/JBMR.040820.
Gadaleta SJ, Landis WJ, Boskey AL, Mendelsohn R. Polarized FT-IR microscopy of calcified turkey leg tendon. Connect Tissue Res. 1996;34(3):203–11.
• Reznikov N, Bilton M, Lari L, Stevens MM, Kroger R. Fractal-like hierarchical organization of bone begins at the nanoscale. Science. 2018;360(6388). https://doi.org/10.1126/science.aao2189 Detailed study of the three-dimensional organization of bone mineral crystals and their configuration around collagen fibers.
• Buenzli PR, Sims NA. Quantifying the osteocyte network in the human skeleton. Bone. 2015;75:144–50. https://doi.org/10.1016/j.bone.2015.02.016 An entertaining study of the magnitude and complexity of the osteocyte network—contains useful data for making comparisons with other organ systems.
Roschger A, Roschger P, Wagermaier W, Chen J, van Tol AF, Repp F, et al. The contribution of the pericanalicular matrix to mineral content in human osteonal bone. Bone. 2019;123:76–85. https://doi.org/10.1016/j.bone.2019.03.018.
Irie K, Ejiri S, Sakakura Y, Shibui T, Yajima T. Matrix mineralization as a trigger for osteocyte maturation. J Histochem Cytochem. 2008;56(6):561–7.
Granke M, Does MD, Nyman JS. The role of water compartments in the material properties of cortical bone. Calcif Tissue Int. 2015;97(3):292–307. https://doi.org/10.1007/s00223-015-9977-5.
Wang Y, Von Euw S, Fernandes FM, Cassaignon S, Selmane M, Laurent G, et al. Water-mediated structuring of bone apatite. Nat Mater. 2013;12(12):1144–53. https://doi.org/10.1038/nmat3787.
Lu Y, Xie Y, Zhang S, Dusevich V, Bonewald LF, Feng JQ. DMP1-targeted Cre expression in odontoblasts and osteocytes. J Dent Res. 2007;86(4):320–5.
• Lespessailles E, Cortet B, Legrand E, Guggenbuhl P, Roux C. Low-trauma fractures without osteoporosis. Osteoporos Int. 2017;28(6):1771–8. https://doi.org/10.1007/s00198-017-3921-7 A helpful clinical study that explains the many fragility fractures that are not predicted by low areal bone mineral density scans.
Roschger P, Misof B, Paschalis E, Fratzl P, Klaushofer K. Changes in the degree of mineralization with osteoporosis and its treatment. Curr Osteoporos Rep. 2014;12(3):338–50. https://doi.org/10.1007/s11914-014-0218-z.
McCreadie BR, Morris MD, Chen TC, Sudhaker Rao D, Finney WF, Widjaja E, et al. Bone tissue compositional differences in women with and without osteoporotic fracture. Bone. 2006;39(6):1190–5. https://doi.org/10.1016/j.bone.2006.06.008.
Nguyen HH, van de Laarschot DM, Verkerk AJ, Milat F, Zillikens MC, Ebeling PR. Genetic risk factors for atypical femoral fractures (AFFs): a systematic review. JBMR Plus. 2018;2(1):1–11. https://doi.org/10.1002/jbm4.10024.
Lo JC, Hui RL, Grimsrud CD, Chandra M, Neugebauer RS, Gonzalez JR, et al. The association of race/ethnicity and risk of atypical femur fracture among older women receiving oral bisphosphonate therapy. Bone. 2016;85:142–7. https://doi.org/10.1016/j.bone.2016.01.002.
Boutroy S, Walker MD, Liu XS, McMahon DJ, Liu G, Guo XE, et al. Lower cortical porosity and higher tissue mineral density in Chinese American versus white women. J Bone Miner Res. 2014;29(3):551–61. https://doi.org/10.1002/jbmr.2057.
• Lloyd AA, Gludovatz B, Riedel C, Luengo EA, Saiyed R, Marty E, et al. Atypical fracture with long-term bisphosphonate therapy is associated with altered cortical composition and reduced fracture resistance. Proc Natl Acad Sci U S A. 2017;114(33):8722–7. https://doi.org/10.1073/pnas.1704460114 An important study of bone biopsies from patients with atypical femur fractures compared with relevant controls, showing their increased mineral:matrix ratio and reduced toughness.
Sims NA, Ng KW. Implications of osteoblast-osteoclast interactions in the management of osteoporosis by antiresorptive agents denosumab and odanacatib. Curr Osteoporos Rep. 2014;12(1):98–106. https://doi.org/10.1007/s11914-014-0196-1.
Seeman E, Martin TJ. Antiresorptive and anabolic agents in the prevention and reversal of bone fragility. Nat Rev Rheumatol. 2019;15(4):225–36. https://doi.org/10.1038/s41584-019-0172-3.
Anderson HC. Electron microscopic studies of induced cartilage development and calcification. J Cell Biol. 1967;35(1):81–101.
Bonucci E. Fine structure of early cartilage calcification. J Ultrastruct Res. 1967;20(1):33–50.
Rohde M, Mayer H. Exocytotic process as a novel model for mineralization by osteoblasts in vitro and in vivo determined by electron microscopic analysis. Calcif Tissue Int. 2007;80(5):323–36. https://doi.org/10.1007/s00223-007-9013-5.
Stanford CM, Jacobson PA, Eanes ED, Lembke LA, Midura RJ. Rapidly forming apatitic mineral in an osteoblastic cell line (UMR 106-01 BSP). J Biol Chem. 1995;270(16):9420–8.
Anderson HC. Molecular biology of matrix vesicles. Clin Orthop Relat Res. 1995;314:266–80.
Azari F, Vali H, Guerquin-Kern JL, Wu TD, Croisy A, Sears SK, et al. Intracellular precipitation of hydroxyapatite mineral and implications for pathologic calcification. J Struct Biol. 2008;162(3):468–79. https://doi.org/10.1016/j.jsb.2008.03.003.
Boonrungsiman S, Gentleman E, Carzaniga R, Evans ND, McComb DW, Porter AE, et al. The role of intracellular calcium phosphate in osteoblast-mediated bone apatite formation. Proc Natl Acad Sci U S A. 2012;109(35):14170–5. https://doi.org/10.1073/pnas.1208916109.
Qing H, Ardeshirpour L, Pajevic PD, Dusevich V, Jahn K, Kato S, et al. Demonstration of osteocytic perilacunar/canalicular remodeling in mice during lactation. J Bone Miner Res. 2012;27(5):1018–29. https://doi.org/10.1002/jbmr.1567.
Gillies BR, Ryan BA, Tonkin BA, Poulton IJ, Ma Y, Kirby BJ, et al. Absence of calcitriol causes increased lactational bone loss and lower milk calcium but does not impair post-lactation bone recovery in Cyp27b1 null mice. J Bone Miner Res. 2018;33(1):16–26. https://doi.org/10.1002/jbmr.3217.
Nollet M, Santucci-Darmanin S, Breuil V, Al-Sahlanee R, Cros C, Topi M, et al. Autophagy in osteoblasts is involved in mineralization and bone homeostasis. Autophagy. 2014;10(11):1965–77. https://doi.org/10.4161/auto.36182.
Ponpuak M, Mandell MA, Kimura T, Chauhan S, Cleyrat C, Deretic V. Secretory autophagy. Curr Opin Cell Biol. 2015;35:106–16. https://doi.org/10.1016/j.ceb.2015.04.016.
Acknowledgments
St. Vincent’s Institute is supported by the Victorian State Government Operational Infrastructure Program.
Funding
NAS is supported by a National Health and Medical Research Council (Australia) Senior Research Fellowship.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
Martha Blank and Natalie A. Sims declare no conflict of interest.
Human and Animal Rights and Informed Consent
This article does not contain any studies with human or animal subjects performed by any of the authors.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
This article is part of the Topical Collection on Skeletal Biology and Regulation
Rights and permissions
About this article

Cite this article
Blank, M., Sims, N.A. Cellular Processes by Which Osteoblasts and Osteocytes Control Bone Mineral Deposition and Maturation Revealed by Stage-Specific EphrinB2 Knockdown. Curr Osteoporos Rep 17, 270–280 (2019). https://doi.org/10.1007/s11914-019-00524-y
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11914-019-00524-y