
Abstract
Purpose of Review
Direct-acting antiviral regimens for chronic hepatitis C virus (HCV) infection became available in 2014, and these highly curative therapies have the potential to reduce HCV-associated morbidity and mortality, decrease HCV transmission, and eliminate HCV infection as a public health problem. This review summarizes the recommendations by the National Academies of Sciences, Engineering, and Medicine for a US strategy for HCV elimination.
Recent Findings
To achieve proposed targets of reducing HCV incidence by 90% and decreasing HCV-related mortality by 60% by 2030, there is a critical need to improve HCV diagnosis and linkage to care, reduce HCV-related disease by antiviral treatment scale-up, reduce HCV incidence, and strengthen HCV surveillance to determine achievement of HCV elimination targets over time.
Summary
While HCV elimination is feasible, success of this national effort will require ongoing collaboration and critical resource investment by key stakeholders, including medical and public health communities, legislators, community organizers, and patient advocates.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Over 3.2 million people in the USA are chronically infected with hepatitis C virus (HCV) infection [1]. If left untreated, chronic HCV can cause progressive liver fibrosis and cirrhosis, leading to hepatic decompensation and hepatocellular carcinoma [2]. Mortality due to chronic HCV infection has continued to rise in the USA over the last decade, and recent estimates suggest that HCV infection contributes to approximately 20,000 deaths annually [3]. Moreover, death from chronic HCV in this country has now surpassed mortality from more than 60 other nationally notifiable infectious diseases, including human immunodeficiency virus (HIV) infection and tuberculosis [3].
However, all-oral, direct-acting antiviral regimens for the treatment of chronic HCV became available in 2014, resulting in cure of infection in more than 94% of patients with typically no more than 8–12 weeks of treatment and few adverse effects [4•]. The availability of these highly curative therapies offered the potential to reduce the risk of HCV-associated morbidity and mortality, decrease HCV transmission, and eliminate HCV infection as a public health problem [5]. Recognizing the unique opportunity offered by these new antivirals, in June 2016, the World Health Assembly formulated a global action plan to reduce the incidence of HCV infection by 90% and decrease HCV-related mortality by 60% by the year 2030 [6]. Within the US, the Division of Viral Hepatitis of the Centers for Disease Control and Prevention (CDC) sought to establish a formal public health plan that identified specific and measureable HCV elimination goals in the USA that aligned with the global HCV response [7]. To aid in this effort, an independent scientific committee was convened by the National Academies of Sciences, Engineering, and Medicine to identify existing barriers to HCV elimination in the USA, formulate recommendations to overcome these challenges, and propose feasible elimination targets by 2030. An initial report evaluating the feasibility of HCV elimination in the USA and barriers to achieving this goal was released in April 2016 [8••]. A subsequent report formulating recommendations to achieve HCV elimination targets by 2030 was published in March 2017 [9••]. This latter report proposed ways to improve adherence to each step of the HCV care continuum and constitutes the framework for a national strategy to eliminate HCV infection in this country.
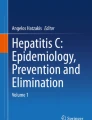
This review summarizes the recommendations to achieve HCV elimination in the USA made by the National Academies committee. These recommendations are grouped into four broad categories corresponding to the key HCV elimination goals: (1) increasing HCV screening, diagnosis, and linkage into care; (2) decreasing HCV-related morbidity and mortality; (3) reducing HCV incidence; and (4) improving national HCV surveillance (see Fig. 1).

Four main categories of national hepatitis C virus elimination goals recommended by the National Academies of Sciences, Engineering, and Medicine and strategies to achieve these goals
Increasing HCV Screening, Diagnosis, and Linkage To Care
Identify Settings for Enhanced HCV Testing Based on Expected Prevalence
To date, the CDC and US Preventive Services Task Force have recommended targeted HCV screening in groups with HCV prevalence higher than that of the general population [10, 11]. However, approximately half of chronic HCV-infected patients in the USA remain unaware of their diagnosis, representing the largest drop-off in the HCV care continuum [12•]. Challenges to HCV diagnosis include the reluctance of patients to report risk behaviors, frequent absence of symptoms associated with chronic infection, and low adherence to HCV screening by providers in clinical practice [8••, 12•]. Diagnosis of HCV infection has been particularly hampered by a lack of prioritization of screening among primary care providers due to competing clinical demands, limited staff time, and discomfort with discussing high-risk behaviors with patients [13, 14]. Recognizing that improving rates of HCV diagnosis will be critical for HCV elimination efforts, the National Academies’ report recommended that the CDC work in conjunction with state and local partners to identify high-risk settings for enhanced HCV testing [9••]. Given that persons with chronic HCV infection may not routinely engage in medical care, HCV screening efforts also will need to be expanded into community-based venues.
Emergency departments may be a potentially high HCV prevalence setting in which to screen for HCV infection. Within 6 months of implementing an HCV testing program at an urban emergency department in the Alameda Health System in Oakland, CA, investigators found a 10% prevalence of HCV antibody-positivity among screened patients [15]. HCV screening did not increase median emergency department length of stay compared to patients undergoing other laboratory testing, supporting the feasibility of integrating HCV screening in this setting [15]. Another study that implemented the CDC’s targeted, risk-based HCV screening guidelines in the Johns Hopkins Hospital Emergency Department in Baltimore, MD found a 13.8% prevalence of HCV antibody-positivity and reported that 31% of identified infections were newly diagnosed [16]. The study also demonstrated that one-quarter of infections would have gone undiagnosed if current CDC birth cohort recommendations were employed, suggesting that in high-risk urban emergency department settings, a practice of universal one-time HCV testing might be effective to diagnose HCV infection [16].
HCV screening initiatives have been implemented in other high HCV prevalence settings. The “Test, Listen, Cure” Hepatitis C Community Awareness Campaign (HepTLC), funded by the CDC, supported HCV testing at sites providing care to people who inject drugs (PWID), including needle/syringe service programs, Ryan White-funded clinics, sexually transmitted infection clinics, and local and state health departments [17]. Between 2012 and 2014, 15,274 PWID were screened, of whom 23% tested positive for HCV antibody, illustrating this program’s successful outreach to a high-risk group. Another effective HCV screening program used a mobile medical unit and patient navigator services to reach patients outside of traditional clinical settings [18]. Participants were recruited by door-to-door outreach and at community events. In the mobile unit, all participants underwent rapid HCV testing and, if positive, confirmatory HCV RNA. Patient navigators provided counseling about test results and facilitated linkage to follow-up HCV care for those found to be HCV RNA-positive. In the first 16 months of this project, 1301 participants were tested, and the prevalence of HCV antibody-positivity was 3.9%. Efforts such as these might be particularly valuable at identifying HCV-infected individuals who do not have frequent contact with the health care system.
Innovative public health-academic partnerships also may be valuable at improving HCV screening and can combine the technical and clinical expertise of an academic institution with the strong local engagement of a community organization to ensure thorough follow-up for newly identified chronic HCV-infected patients. In one such partnership, collaborators at Johns Hopkins University School of Medicine engaged with a community organization in Baltimore, MD called Sisters Together and Reaching (STAR), Inc. to screen PWID at community events, drug treatment centers, and homeless shelters [19]. This effort led to the identification of 49 (15%; n = 325) HCV antibody-positive individuals. Case management personnel worked to confirm chronic HCV infection, obtain health insurance (if not previously acquired), facilitate referral for HCV treatment, and ensure adherence to medical visits [19].
Continued efforts aimed at enhancing HCV screening in settings of expected high prevalence and potentially outside of traditional healthcare venues will be needed to increase the proportion of patients who are diagnosed, linked to care, and treated, which ultimately will be crucial for the success of the US HCV elimination strategy.
Establish Measures to Monitor Adherence to HCV Screening
Attempts to improve adherence to HCV screening guidelines have primarily focused on simplification of screening recommendations and educational interventions but have not been shown to have substantial impact. Recognizing that the complexity of the CDC’s 1998 HCV screening guidelines contributed to low implementation rates [20], simplified guidelines were published in 2012 [10], but HCV screening has remained poor [21, 22]. One study that provided continuous, educational sessions about HCV testing guidelines to primary care clinics over a 15-week period found that adherence to screening actually decreased over time [13].
Given the limitations of existing interventions in improving HCV screening, alternative strategies, such as direct performance evaluation of adherence to viral hepatitis testing and linkage to care, may be effective at improving provider adherence to HCV screening guidelines. The National Committee for Quality Assurance seeks to ensure that recommendations for improving health are implemented in clinical practice and monitors the adherence of these recommendations within health plans. Adding viral hepatitis measures to the Healthcare Effectiveness Data and Information Set may increase the priority of HCV screening by insurers and healthcare providers. Accordingly, the National Academies’ report recommended that the National Committee for Quality Assurance should establish measures to monitor compliance with viral hepatitis screening guidelines [9••].
Increase Support for Hepatitis Case Finding and Linkage to Care
Timely diagnosis of chronic HCV infection and appropriate linkage to care are critical for HCV elimination efforts but have been hampered by inadequate resources within local health departments [23]. The National Academies’ report recommended that the CDC should work with local partners to support standard hepatitis case finding measures and facilitate linkage of all HCV-infected patients into care [9••]. Existing cooperative agreements between each state and the CDC’s Epidemiology and Laboratory Capacity for Infectious Diseases may provide a mechanism for further funding and capacity building around HCV surveillance and follow-up [9••, 24]. This additional funding could be used to support expanded staff resources, build informatics systems, and develop crosswalks between public health systems and electronic health records. The Massachusetts Department of Health and the Harvard Center for Excellence in Public Health Informatics have already collaborated to develop an automated HCV detection and reporting system that extracts relevant data from patients’ electronic health records, applies HCV detection algorithms, and sends potentially new cases of HCV infection to health departments for further investigation [25]. The program is publicly available and compatible with different electronic medical record systems, expanding its utility and reach across clinical practices in the state [9••, 25].
Decreasing HCV-Related Morbidity and Mortality
Expand the Number of HCV Providers
Mathematical modeling analyses within the National Academies’ report estimated that at least 260,000 chronic HCV-infected patients must be treated yearly to achieve elimination of HCV in the USA by 2030 [9••]. As a result, successful HCV treatment scale-up will require expansion of HCV provider capacity. In the interferon era, HCV treatment was primarily coordinated by hepatologists and infectious diseases specialists in office settings with established resources for administering complicated treatment regimens and managing the side effects of antiviral therapy. However, the ease of administering new DAA regimens that are all-oral, well-tolerated, and require short treatment duration has made HCV treatment feasible by non-specialist providers in a variety of settings [26,27,28,29]. In particular, strategies to offer HCV care in the primary care setting may mitigate the drop-offs in linkage to care that occur with subspecialty referral [18]. Consequently, the National Academies’ report proposed that the American Association for the Study of Liver Diseases and the Infectious Diseases Society of America partner with primary care providers and their professional organizations to build capacity to treat chronic HCV infection in the primary care setting [9••]. Capacity building in primary care will require not only one-time training conferences but also standing programs between primary care providers and specialists.
Pilot partnerships have already demonstrated the feasibility of expanding HCV treatment to non-specialist health providers. For example, in the Extension for Community Health Care Outcomes (ECHO) program, the CDC and the University of New Mexico collaborated to build a program that trained primary care physicians in Utah and Arizona, using videoconferencing and case-based learning tools to treat chronic HCV in rural settings with limited access to specialist care [27]. As an additional example, the New York City Department of Health and Mental Hygiene has developed networks to provide educational resources, access to HCV treatment guidelines, and mentoring and consultations for providers managing patients with chronic HCV [28]. Finally, in California, a task-shifting treatment model for HCV was implemented that enabled a trained licensed practical nurse, under the guidance of hepatologists, to treat over 100 HCV-infected patients between 2014 and 2015 [29]. A secure web-based electronic health record enabled the nurse to communicate with hepatologists for medical advice as needed. These reports demonstrate the feasibility of programs aimed at expanding the pool of providers for HCV care and treatment.
Increase HCV Screening and Treatment in Correctional Settings
HCV infection is common in prison and jail settings, with an estimated prevalence of 12–35% [30]. Given that more than 90% of these persons are released and typically have little subsequent contact with the healthcare system, correctional institutions represent valuable settings in which to reduce HCV-related morbidity and mortality. They could offer access to HCV providers—either directly on staff or via telemedicine—to facilitate evaluation and treatment of HCV infection. There is also the opportunity for directly observed therapy in this setting, minimizing the risk of antiviral drug diversion. However, few correctional facilities have formal HCV screening and treatment guidelines [31, 32]. To reduce HCV-associated morbidity, the National Academies’ report recommended that correctional settings should be a focus of HCV screening and treatment efforts [9••]. In support of this recommendation, mathematical model analyses have suggested that strategies for opt-out HCV screening and DAA treatment in the prison setting would be highly cost-effective from a societal perspective [33, 34].
Establish a System to Support Key Populations with Chronic HCV
The high prevalence of chronic HCV infection among marginalized populations, including PWID, homeless, and incarcerated persons, has complicated efforts aimed at HCV diagnosis, linkage to care, and treatment. As a result, the National Academies’ report recommended that the Department of Health and Human Services should work with states to build a comprehensive system of care and support for these key populations with chronic HCV on the scale of the Ryan White system [9••]. The Ryan White HIV/AIDS Program has ensured access to preventive and treatment services for people living with HIV/AIDS in the USA since 1990 [35, 36]. Ryan White programs also offer case management, mental health services, and substance use treatment for their clients, all of which are critical components of care for HCV-infected individuals [35]. Given the overlap in risk factors for HIV and HCV, it might be feasible to expand existing Ryan White programs to offer outreach services for patients with chronic HCV infection, regardless of HIV status. Notably, 29 states have provided HCV treatment for HIV/HCV-coinfected patients through the Ryan White program since 2011 [37]. By providing a safety net for key vulnerable groups who may be underinsured or uninsured, such a comprehensive system of care and support could help to reduce HCV-related morbidity and mortality and greatly aid national HCV elimination efforts.
Remove Restrictions to DAAs and Increase Access to HCV Therapy
The costs of DAAs led public and private insurers in the USA to restrict access to these medications [38]. Insurers established varying criteria for reimbursement of DAAs, such as evidence of advanced liver fibrosis, consultation with a specialist, and/or abstinence from alcohol or illicit drug use [39, 40]. Restrictions for reimbursement of DAAs have been shown to be common across state Medicaid programs [41,42,43]. Criteria for approval of DAAs in Medicare and commercial insurance health plans have not been reported. Analyses conducted shortly after the release of DAAs into the market showed that the downstream effect of these restrictions was to make common the denial of reimbursement of DAA treatment by insurers [44, 45].
The high incidence of denial of DAA therapy by insurers has important implications. From a clinical standpoint, patients denied access to HCV therapy remain at risk for the development of hepatic fibrosis, cirrhosis, liver decompensation, and hepatocellular carcinoma [46••]. Denial of DAA treatment can also lead to ongoing HCV-associated inflammation, which might increase the risk of extra-hepatic complications [47, 48]. Further, failure to treat and cure chronic HCV maintains a reservoir of HCV transmission. From a public health standpoint, the high incidence of denial of DAA treatment represents a major barrier to the goal of HCV elimination. Viral eradication can help to eliminate HCV transmission [49, 50], reduce the risk of liver complications [51], decrease extra-hepatic manifestations [52], and prolong survival [53]. DAA treatment has also been shown to be cost-effective [54,55,56]. The ability to cure chronic HCV in nearly all infected people makes the prospect of eliminating HCV infection in the USA feasible [26]. As a result, the National Academies’ report recommended that public and private insurers should remove restrictions to DAAs that are not medically indicated and offer treatment to all chronic HCV-infected patients [9••]. This recommendation is consistent with guidelines from the American Association for the Study of Liver Diseases/Infectious Diseases Society of America that recommend DAA treatment for all patients with chronic HCV infection [46••].
Given the costs of DAA drugs, alternative means of financing these therapies may need to be considered. The National Academies’ report provided several alternative proposals for financing HCV elimination [9••]. One proposal suggested that the federal government, on behalf of the Department of Health and Human Services, could consider purchasing the rights to a DAA for use in neglected market segments, such as state Medicaid programs, the Indian Health Service, and correctional settings. In such a scenario, the government would acquire the licensing rights to a DAA patent in a voluntary transaction with a pharmaceutical company for use of that drug in these neglected sectors. Such a licensing strategy would allow the government to control costs while negotiating reasonable compensation for drug companies. Although the initial investment for the federal government would be large, the long-term cost savings could be considerable and would allow many patients to be treated [9••]. Alternative strategies to address the costs of DAA treatments might include seeking discounts for bulk or pooled purchases [57, 58] or obtaining DAA regimens through the 340B Drug Discount Program, which provides medications at greatly discounted prices to safety net providers caring for uninsured or low-income patients [59].
Reducing HCV Incidence
Expand Access to Needle/Syringe Services and Opioid Agonist Therapy
Since injection drug use is the predominant mode of HCV transmission in the USA, prevention efforts among PWID must be a priority in order to reduce HCV incidence [60•]. Harm reduction services, which include needle/syringe exchange programs and opioid agonist therapy (OAT), have been shown to have significant impact as HCV prevention strategies. However, their utilization remains low due to restrictive policies and barriers to PWID outreach [60•, 61]. Consequently, the National Academies’ report recommended that states and federal agencies should expand access to needle/syringe exchanges and OAT in accessible venues [9••].
Numerous studies have demonstrated that needle/syringe service programs can lead to long-lasting changes in injecting risk behaviors among PWID, including sharing of needles, syringes, or other injection drug paraphernalia [62,63,64,65]. Several studies have found a lower prevalence and/or incidence of HCV infection among PWID participating in needle/syringe exchange programs compared to those who do not [62, 66, 67]. A cohort study of PWID in the Netherlands found that participants who received full harm reduction services, defined as obtaining all needles/syringes from an exchange program along with daily OAT, had a substantially lower incidence of HCV infection compared to those receiving no harm reduction services (incidence rate ratio, 0.15; 95% CI, 0.06–0.40) [66]. In addition, in one systematic review, needle/syringe service programs were associated with significant decreases in HIV and HCV prevalence [62].
While the number of needle/syringe exchange programs in the USA has grown over time, there remains an insufficient number and disparate distribution of these programs across the country to meet the demands of the PWID population [9••, 68, 69]. Pharmacies, often conveniently located throughout communities and with long hours of operation, represent a viable resource to address the lack of needle/syringe service programs. Pharmacies could provide nonprescription sale of sterile needles/syringes, which has been shown to successfully reduce HIV transmission [70]. While all states permit sale of needles/syringes without prescriptions, there are varying levels of restrictions imposed by states that would need to be re-evaluated to make pharmacies a source of sterile needles/syringes for PWID [70].
In addition to needle/syringe service programs, OAT can have a direct and lasting impact on reducing the overall incidence of HCV infection among PWID. Epidemiological studies show that by enabling PWID to refrain from HCV-related high-risk behaviors, OAT can reduce HCV incidence and prevent HCV transmission [71,72,73,74]. Further, long-term medication management with OAT is associated with retention in treatment, reduction in illicit drug use, and recovery from opioid dependence/abuse [75, 76].
Despite the benefits of OAT, the availability of these services is lagging far behind the growing demand, particularly in rural areas of the USA [77,78,79]. A recent analysis of the geographic distribution of physicians authorized to prescribe buprenorphine as of 2012 found that 42% of all physicians with waivers were psychiatrists who practiced primarily in urban settings, while only 3% were primary care physicians [77]. As a result, it is estimated that more than 30 million Americans are living in counties without access to buprenorphine treatment [77]. Expansion of telehealth services may be a viable approach to increase access to behavioral health and addiction specialists in remote areas that currently lack these resources or the infrastructure to expand addiction treatment services [80]. Given the coexistence of the opioid and HCV epidemics in the USA, leveraging state and federal resources committed to the opioid epidemic toward HCV prevention and treatment will be crucial to halt ongoing HCV transmission.
Improving HCV Surveillance
Support Studies to Measure HCV Incidence/Prevalence in High-Risk Groups
Surveillance of HCV infection is critically important for assessing all steps along the HCV care continuum, including estimating HCV prevalence and new infections, determining the incidence of HCV-associated liver complications, and evaluating linkage to HCV care and DAA treatment. Current estimates of HCV incidence and prevalence are drawn from data collected through household surveys, electronic healthcare databases, and laboratory reporting, often without a focus on the subpopulations disproportionately affected by HCV infection [81]. For example, the most recent National Health and Nutrition Examination Survey (NHANES) report on the prevalence of chronic HCV found that approximately 2.7 million people are chronically infected with HCV in the USA, but this survey excluded homeless, institutionalized, and incarcerated persons, who are at high risk for HCV infection [1]. There are estimated to be an additional 800,000 (range, 300,000–1.5 million) persons with chronic HCV among these high-risk groups based on extrapolations from HCV seroprevalence studies conducted in those populations [81]. The lack of reliable data on HCV prevalence and incidence in these groups limits the ability of public health and medical professionals to establish and advocate for treatment priorities, resource needs, and goals. As a result, the National Academies’ report recommended that the CDC should support cross-sectional and cohort studies in these high-risk populations to measure HCV prevalence and incidence [9••]. Periodic cross-sectional surveys of high-risk populations would provide more accurate estimates of HCV prevalence over time. Cohort studies of similar populations would enhance our understanding of HCV incidence in these groups. Such studies would complement information about HCV infection coming from population-based surveys such as NHANES.
Expand Hepatitis Testing and Case Finding Based on Prevalence
Strengthening HCV surveillance nationally will require a two-pronged approach: (1) allocation of resources to local and state health department to support HCV testing and linkage to care; and (2) expansion of HCV screening and testing in high-risk settings. To meet these needs, the National Academies’ report recommended that the CDC partner with state and local health departments to support standardization of HCV case finding and follow-up [9••].
HCV disease reporting and case follow-up vary across states, which limits the quality of surveillance data available locally and subsequently shared with the CDC. Automated sharing of positive HCV antibody and/or HCV RNA test results from diagnostic laboratories has improved HCV reporting, but may not provide relevant clinical data to support case finding investigations. Investment in informatics infrastructure may take advantage of widespread use of electronic health records to support HCV surveillance systems [9••]. Further, standardization of disease reporting across states could improve efficiency and work flow within local health departments that continually face resource limitations. These improvements could then support infrastructure investment and expansion of enhanced surveillance to other high-risk settings.
Need For a Central HCV Elimination Coordinating Office
All of the HCV elimination efforts discussed above will require cooperation among federal and state agencies, legislators, health care providers, and professional societies. Leadership from a single office would increase logistical efficiency in implementing these recommendations. Prior examples of successful elimination efforts, including polio, measles, and guinea worm, benefitted immensely from strong political engagement and central coordination at the highest levels of government. Therefore, the National Academies’ report proposed that the federal government should oversee a coordinated effort to manage HCV elimination [9••]. Such an effort could take the shape of a central coordinating office dedicated to viral hepatitis elimination that is located in the White House, similar to the White House Office of National AIDS Policy [82]. Alternatively, the coordinating effort could be undertaken by that office, given its proven expertise working with other federal and state agencies to implement national HIV/AIDS policies. The executive authority afforded to a central coordinating office could support HCV elimination efforts in ways not possible at lower levels of government or by public health organizations.
Conclusions
The potential elimination of HCV infection as a public health threat in the USA was not conceivable among scientific, medical, or public health professionals a decade ago. However, advances in HCV treatment, along with rising HCV incidence due to the opioid epidemic in the USA, have created urgency among these communities to address this previously neglected condition. In response, the National Academies of Sciences, Engineering, and Medicine issued two seminal reports in 2016 and 2017 that highlighted the feasibility of HCV elimination in the USA and proposed evidence-based recommendations to overcome existing barriers and achieve HCV elimination as a public health problem by 2030 [8••, 9••]. These recommendations were aimed at increasing HCV diagnosis and linkage to care, decreasing HCV-related disease burden by scaling up DAA-based HCV treatment, reducing HCV transmission among high-risk groups, and building disease surveillance to assess achievement of elimination targets over time. Given the need for collaboration among stakeholders, a central coordinating office would provide logistical efficiency in supporting these recommendations and ensure successful implementation of the US HCV elimination strategy. Only through such coordinated collaboration will the elimination of HCV infection be not only aspirational, but truly attainable.
References
Papers of particular interest, published recently, have been highlighted as: • Of importance •• Of major importance
Denniston MM, Jiles RB, Drobeniuc J, Klevens RM, Ward JW, McQuillan GM, et al. Chronic hepatitis C virus infection in the United States, national health and nutrition examination survey 2003 to 2010. Ann Intern Med. 2014;160(5):293–300. https://doi.org/10.7326/M13-1133.
Westbrook RH, Dusheiko G. Natural history of hepatitis C. J Hepatol. 2014;61(1 Suppl):S58–68. https://doi.org/10.1016/j.jhep.2014.07.012.
Ly KN, Hughes EM, Jiles RB, Holmberg SD. Rising mortality associated with hepatitis C virus in the United States, 2003–2013. Clin Infect Dis. 2016;62(10):1287–8. https://doi.org/10.1093/cid/ciw111.
• Pawlotsky JM. New hepatitis C therapies: the toolbox, strategies, and challenges. Gastroenterology. 2014;146(5):1176–92. https://doi.org/10.1053/j.gastro.2014.03.003. Important initial review summarizing the development of direct-acting antiviral agents and interferon-sparing treatment strategies for chronic HCV infection.
Lok AS, Chung RT, Vargas HE, Kim AY, Naggie S, Powderly WG. Benefits of direct-acting antivirals for hepatitis C. Ann Intern Med. 2017;167:812–3. https://doi.org/10.7326/M17-1876.
World Health Organization. Combating hepatitis B and C to reach elimination by 2030. http://apps.who.int/iris/bitstream/10665/206453/1/WHO_HIV_2016.04_eng.pdf?ua=1. Accessed 24 Oct 2017.
Department of Health and Human Services. The U.S. national viral hepatitis action plan for 2017–2020. https://www.hhs.gov/sites/default/files/National%20Viral%20Hepatitis%20Action%20Plan%202017-2020.pdf. Accessed 24 Oct 2017.
•• National Academies of Sciences Engineering, and Medicine. Eliminating the Public Health Problem of Hepatitis B and C in the United States: Phase one report, Washington (DC): The National Academies Press; 2016. Formative Phase One report published by the National Academies to first evaluate and describe the feasibility of a national strategy for the elimination of HCV in the US.
•• National Academies of Sciences EaM. In: Strom BL, Buckley GJ, editors. A National Strategy for the elimination of hepatitis B and C: phase two report. Washington (DC): The National Academies Press; 2017. Seminal phase two report published by the National Academies that provides clear recommendations for achievement of US HCV elimination targets by 2030.
Smith BD, Morgan RL, Beckett GA, Falck-Ytter Y, Holtzman D, Teo CG, et al. Recommendations for the identification of chronic hepatitis C virus infection among persons born during 1945–1965. MMWR Recomm Rep. 2012;61(RR-4):1–32.
Moyer VA, USPSTF. Screening for hepatitis C virus infection in adults: U.S. preventive services task force (USPSTF) recommendation statement. Ann Intern Med. 2013;159(5):349–57. https://doi.org/10.7326/0003-4819-159-5-201309030-00672.
• Yehia BR, Schranz AJ, Umscheid CA, Lo Re V 3rd. The treatment cascade for chronic hepatitis C virus infection in the United States: a systematic review and meta-analysis. PLoS One. 2014;9(7):e101554. https://doi.org/10.1371/journal.pone.0101554. Important systematic review that depicts the care continuum for HCV infection in the US.
Southern WN, Drainoni ML, Smith BD, Koppelman E, McKee MD, Christiansen CL, et al. Physician nonadherence with a hepatitis C screening program. Qual Manag Health Care. 2014;23(1):1–9. https://doi.org/10.1097/QMH.0000000000000007.
Almario CV, Vega M, Trooskin SB, Navarro VJ. Examining hepatitis C virus testing practices in primary care clinics. J Viral Hepat. 2012;19(2):e163–9. https://doi.org/10.1111/j.1365-2893.2011.01539.x.
White DA, Anderson ES, Pfeil SK, Trivedi TK, Alter HJ. Results of a rapid hepatitis C virus screening and diagnostic testing program in an urban emergency department. Ann Emerg Med. 2016;67(1):119–28. https://doi.org/10.1016/j.annemergmed.2015.06.023.
Hsieh YH, Rothman RE, Laeyendecker OB, Kelen GD, Avornu A, Patel EU, et al. Evaluation of the Centers for Disease Control and Prevention recommendations for hepatitis C virus testing in an urban emergency department. Clin Infect Dis. 2016;62(9):1059–65. https://doi.org/10.1093/cid/ciw074.
Blackburn NA, Patel RC, Zibbell JE. Improving screening methods for hepatitis C among people who inject drugs: findings from the HepTLC initiative, 2012–2014. Public Health Rep. 2016;131(Suppl 2):91–7. https://doi.org/10.1177/00333549161310S214.
Trooskin SB, Poceta J, Towey CM, Yolken A, Rose JS, Luqman NL, et al. Results from a geographically focused, community-based HCV screening, linkage-to-care and patient navigation program. J Gen Intern Med. 2015;30(7):950–7. https://doi.org/10.1007/s11606-015-3209-6.
Irvin R, McAdams-Mahmoud A, Hickman D, Wilson J, Fenwick W, Chen I, et al. Building a community—academic partnership to enhance hepatitis C virus screening. J Community Med Health Educ. 2016;6(3) https://doi.org/10.4172/2161-0711.1000431.
Centers for Disease Control and Prevention. Recommendations for prevention and control of hepatitis C virus (HCV) infection and HCV-related chronic disease. MMWR Recomm Rep. 1998;47(RR-19):1–39.
Jewett A, Garg A, Meyer K, Wagner LD, Krauskopf K, Brown KA, et al. Hepatitis C virus testing perspectives among primary care physicians in four large primary care settings. Health Promot Pract. 2015;16(2):256–63. https://doi.org/10.1177/1524839914532291.
Centers for Disease Control and Prevention. Locations and reasons for initial testing for hepatitis C infection—chronic hepatitis cohort study, United States, 2006–2010. MMWR Morb Mortal Wkly Rep. 2013;62(32):645–8.
Centers for Disease Control and Prevention. Guidelines for viral hepatitis surveillance and case management. Atlanta, GA. 2005. https://www.cdc.gov/hepatitis/pdfs/2005guidlines-surv-casemngmt.pdf. Accessed 31 July 2017.
Centers for Disease Control and Prevention. Epidemiology and laboratory capacity for infectious diseases (ELC) cooperative agreement. https://www.cdc.gov/ncezid/dpei/epidemiology-laboratory-capacity.html. Accessed 22 Oct 2017.
Klompas M, Murphy M, Lankiewicz J, McVetta J, Lazarus R, Eggleston E, et al. Harnessing electronic health records for public health surveillance. Online J Public Health Inform. 2011;3(3) https://doi.org/10.5210/ojphi.v3i3.3794.
Pawlotsky JM, Feld JJ, Zeuzem S, Hoofnagle JH. From non-a, non-B hepatitis to hepatitis C virus cure. J Hepatol. 2015;62(1 Suppl):S87–99. https://doi.org/10.1016/j.jhep.2015.02.006.
Mitruka K, Thornton K, Cusick S, Orme C, Moore A, Manch RA, et al. Expanding primary care capacity to treat hepatitis C virus infection through an evidence-based care model—Arizona and Utah, 2012–2014. MMWR Morb Mortal Wkly Rep. 2014;63(18):393–8.
Laraque F, Varma JK. A public health approach to hepatitis C in an urban setting. Am J Public Health. 2017;107(6):922–6. https://doi.org/10.2105/AJPH.2017.303718.
Yoo ER, Perumpail RB, Cholankeril G, Jayasekera CR, Ahmed A. Expanding treatment access for chronic hepatitis C with task-shifting in the era of direct-acting antivirals. J Clin Transl Hepatol. 2017;5(2):130–3. https://doi.org/10.14218/JCTH.2016.00059.
Weinbaum C, Lyerla R, Margolis HS, Centers for Disease Control and Prevention. Prevention and control of infections with hepatitis viruses in correctional settings. Centers for Disease Control and Prevention. MMWR Recomm Rep. 2003;52(RR-1):1–36. quiz CE1–4
Beckman AL, Bilinski A, Boyko R, Camp GM, Wall AT, Lim JK, et al. New hepatitis C drugs are very costly and unavailable to many state prisoners. Health Aff. 2016;35(10):1893–901. https://doi.org/10.1377/hlthaff.2016.0296.
Maurer KG, Gondles EF. Hepatitis C in correctional settings: challenges and opportunities. Coalition of Correctional Health Authorities and American Correctional Association 2015;2(1):1–15.
Liu S, Watcha D, Holodniy M, Goldhaber-Fiebert JD. Sofosbuvir-based treatment regimens for chronic, genotype 1 hepatitis C virus infection in U.S. incarcerated populations: a cost-effectiveness analysis. Ann Intern Med. 2014;161(8):546–53. https://doi.org/10.7326/M14-0602.
He T, Li K, Roberts MS, Spaulding AC, Ayer T, Grefenstette JJ, et al. Prevention of hepatitis C by screening and treatment in U.S. prisons. Ann Intern Med. 2016;164(2):84–92. https://doi.org/10.7326/M15-0617.
Cahill SR, Mayer KH, Boswell SL. The Ryan white HIV/AIDS program in the age of health care reform. Am J Public Health. 2015;105(6):1078–85. https://doi.org/10.2105/AJPH.2014.302442.
Sood N, Juday T, Vanderpuye-Orgle J, Rosenblatt L, Romley JA, Peneva D, et al. HIV care providers emphasize the importance of the Ryan White Program for access to and quality of care. Health Aff. 2014;33(3):394–400. https://doi.org/10.1377/hlthaff.2013.1297.
Wills T, Friedrich M, Beal J, Somboonwit C, Mcintosh S, Bork A et al. Implementing hepatitis C treatment programs in comprehensive HIV clinics: the Health Resources and Services Administration (HRSA) special projects of national significance hepatitis C treatment exapnsion initiative. ID Week 2014; October 10, 2014; Philadelphia. [Abstract PA2014].
Trooskin SB, Reynolds H, Kostman JR. Access to costly new hepatitis C drugs: medicine, money, and advocacy. Clin Infect Dis. 2015;61(12):1825–30. https://doi.org/10.1093/cid/civ677.
Simon RE, Pearson SD, Hur C, Chung RT. Tackling the hepatitis C cost problem: a test case for tomorrow's cures. Hepatology. 2015;62(5):1334–6. https://doi.org/10.1002/hep.28157.
Grebely J, Haire B, Taylor LE, Macneill P, Litwin AH, Swan T, et al. Excluding people who use drugs or alcohol from access to hepatitis C treatments—is this fair, given the available data? J Hepatol. 2015;63(4):779–82. https://doi.org/10.1016/j.jhep.2015.06.014.
Barua S, Greenwald R, Grebely J, Dore GJ, Swan T, Taylor LE. Restrictions for Medicaid reimbursement of sofosbuvir for the treatment of hepatitis C virus infection in the United States. Ann Intern Med. 2015;163(3):215–23. https://doi.org/10.7326/M15-0406.
Canary LA, Klevens RM, Holmberg SD. Limited access to new hepatitis C virus treatment under state Medicaid programs. Ann Intern Med. 2015;163(3):226–8. https://doi.org/10.7326/M15-0320.
Ooka K, Connolly JJ, Lim JK. Medicaid reimbursement for oral direct antiviral agents for the treatment of chronic hepatitis C. Am J Gastroenterol. 2017;112(6):828–32. https://doi.org/10.1038/ajg.2017.87.
Lo Re V 3rd, Gowda C, Urick PN, Halladay JT, Binkley A, Carbonari DM, et al. Disparities in absolute denial of modern hepatitis C therapy by type of insurance. Clin Gastroenterol Hepatol. 2016;14(7):1035–43. https://doi.org/10.1016/j.cgh.2016.03.040.
Younossi ZM, Bacon BR, Dieterich DT, Flamm SL, Kowdley K, Milligan S, et al. Disparate access to treatment regimens in chronic hepatitis C patients: data from the TRIO network. J Viral Hepat. 2016;23(6):447–54. https://doi.org/10.1111/jvh.12506.
•• American Association for the Study of Liver Diseases/Infectious Diseases Society of America. Recommendations for testing, managing, and treating hepatitis C. http://www.hcvguidelines.org. Accessed 10 Aug 2017. Important evidence-based consensus guidelines issued by major specialty societies providing guidance for clinicians on up-to-date care and management of chronic HCV infection.
Negro F, Forton D, Craxi A, Sulkowski MS, Feld JJ, Manns MP. Extrahepatic morbidity and mortality of chronic hepatitis C. Gastroenterology. 2015;149(6):1345–60. https://doi.org/10.1053/j.gastro.2015.08.035.
Soriano V, Berenguer J. Extrahepatic comorbidities associated with hepatitis C virus in HIV-infected patients. Curr Opin HIV AIDS. 2015;10(5):309–15. https://doi.org/10.1097/COH.0000000000000175.
Harris RJ, Martin NK, Rand E, Mandal S, Mutimer D, Vickerman P, et al. New treatments for hepatitis C virus (HCV): scope for preventing liver disease and HCV transmission in England. J Viral Hepat. 2016;23(8):631–43. https://doi.org/10.1111/jvh.12529.
Martin NK, Thornton A, Hickman M, Sabin C, Nelson M, Cooke GS, et al. Can hepatitis C virus (HCV) direct-acting antiviral treatment as prevention reverse the HCV epidemic among men who have sex with men in the United Kingdom? Epidemiological and modeling insights. Clin Infect Dis. 2016;62(9):1072–80. https://doi.org/10.1093/cid/ciw075.
Backus LI, Belperio PS, Shahoumian TA, Mole LA. Impact of sustained virologic response with direct-acting antiviral treatment on mortality in patients with advanced liver disease. Hepatology. 2017; https://doi.org/10.1002/hep.29408.
Mahale P, Engels EA, Li R, Torres HA, Hwang LY, Brown EL, et al. The effect of sustained virological response on the risk of extrahepatic manifestations of hepatitis C virus infection. Gut. 2017;67:553–61. https://doi.org/10.1136/gutjnl-2017-313983.
van der Meer AJ, Veldt BJ, Feld JJ, Wedemeyer H, Dufour JF, Lammert F, et al. Association between sustained virological response and all-cause mortality among patients with chronic hepatitis C and advanced hepatic fibrosis. JAMA. 2012;308(24):2584–93. https://doi.org/10.1001/jama.2012.144878.
Najafzadeh M, Andersson K, Shrank WH, Krumme AA, Matlin OS, Brennan T, et al. Cost-effectiveness of novel regimens for the treatment of hepatitis C virus. Ann Intern Med. 2015;162(6):407–19. https://doi.org/10.7326/M14-1152.
Rein DB, Wittenborn JS, Smith BD, Liffmann DK, Ward JW. The cost-effectiveness, health benefits, and financial costs of new antiviral treatments for hepatitis C virus. Clin Infect Dis. 2015;61(2):157–68. https://doi.org/10.1093/cid/civ220.
Chahal HS, Marseille EA, Tice JA, Pearson SD, Ollendorf DA, Fox RK, et al. Comparative clinical effectiveness and value of novel interferon-free combination therapy for hepatitis C genotype 1: summary of California technology assessment forum report. JAMA Intern Med. 2015;175(9):1559–60. https://doi.org/10.1001/jamainternmed.2015.3348.
Allison MA, O'Leary ST, Lindley MC, Crane LA, Hurley LP, Beaty BL, et al. Financing of vaccine delivery in primary care practices. Acad Pediatr. 2017;17:770–7. https://doi.org/10.1016/j.acap.2017.06.001.
Huff-Rousselle M. The logical underpinnings and benefits of pooled pharmaceutical procurement: a pragmatic role for our public institutions? Soc Sci Med. 2012;75(9):1572–80. https://doi.org/10.1016/j.socscimed.2012.05.044.
Health Resources and Services Administration (HRSA). 340B drug pricing program http://www.hrsa.gov/opa. Accessed 10 Aug 2017.
• Grebely J, Dore GJ, Morin S, Rockstroh JK, Klein MB. Elimination of HCV as a public health concern among people who inject drugs by 2030—what will it take to get there? J Int AIDS Soc. 2017;20(1):1–8. https://doi.org/10.7448/IAS.20.1.22146. Important review describing specific challenges and proposed solutions to achieve HCV elimination among people who inject drugs (PWID), a group with the highest HCV prevalence.
Perlman DC, Jordan AE, Uuskula A, Huong DT, Masson CL, Schackman BR, et al. An international perspective on using opioid substitution treatment to improve hepatitis C prevention and care for people who inject drugs: structural barriers and public health potential. Int J Drug Policy. 2015;26(11):1056–63. https://doi.org/10.1016/j.drugpo.2015.04.015.
Abdul-Quader AS, Feelemyer J, Modi S, Stein ES, Briceno A, Semaan S, et al. Effectiveness of structural-level needle/syringe programs to reduce HCV and HIV infection among people who inject drugs: a systematic review. AIDS Behav. 2013;17(9):2878–92. https://doi.org/10.1007/s10461-013-0593-y.
Fernandes RM, Cary M, Duarte G, Jesus G, Alarcao J, Torre C, et al. Effectiveness of needle and syringe Programmes in people who inject drugs—an overview of systematic reviews. BMC Public Health. 2017;17(1):309. https://doi.org/10.1186/s12889-017-4210-2.
Holtzman D, Barry V, Ouellet LJ, Des Jarlais DC, Vlahov D, Golub ET, et al. The influence of needle exchange programs on injection risk behaviors and infection with hepatitis C virus among young injection drug users in select cities in the United States, 1994–2004. Prev Med. 2009;49(1):68–73. https://doi.org/10.1016/j.ypmed.2009.04.014.
Huo D, Ouellet LJ. Needle exchange and injection-related risk behaviors in Chicago: a longitudinal study. J Acquir Immune Defic Syndr. 2007;45(1):108–14. https://doi.org/10.1097/QAI.0b013e318050d260.
Van Den Berg C, Smit C, Van Brussel G, Coutinho R, Prins M, Amsterdam C. Full participation in harm reduction programmes is associated with decreased risk for human immunodeficiency virus and hepatitis C virus: evidence from the Amsterdam cohort studies among drug users. Addiction. 2007;102(9):1454–62. https://doi.org/10.1111/j.1360-0443.2007.01912.x.
Jones L, Pickering L, Sumnall H, McVeigh J, Bellis MA. Optimal provision of needle and syringe programmes for injecting drug users: a systematic review. Int J Drug Policy. 2010;21(5):335–42. https://doi.org/10.1016/j.drugpo.2010.02.001.
Centers for Disease Control and Prevention. Syringe exchange programs—United States, 2008. MMWR Morb Mortal Wkly Rep. 2010;59(45):1488–91.
Des Jarlais DC, McKnight C, Goldblatt C, Purchase D. Doing harm reduction better: syringe exchange in the United States. Addiction. 2009;104(9):1441–6. https://doi.org/10.1111/j.1360-0443.2008.02465.x.
Oramasionwu CU, Johnson TL, Zule WA, Carda-Auten J, Golin CE. Using pharmacies in a structural intervention to distribute low dead space syringes to reduce HIV and HCV transmission in people who inject drugs. Am J Public Health. 2015;105(6):1066–71. https://doi.org/10.2105/AJPH.2015.302581.
Islam N, Krajden M, Shoveller J, Gustafson P, Gilbert M, Buxton JA, et al. Incidence, risk factors, and prevention of hepatitis C reinfection: a population-based cohort study. Lancet Gastroenterol Hepatol. 2017;2(3):200–10. https://doi.org/10.1016/S2468-1253(16)30182-0.
Midgard H, Hajarizadeh B, Cunningham EB, Conway B, Backmund M, Bruggmann P, et al. Changes in risk behaviours during and following treatment for hepatitis C virus infection among people who inject drugs: the ACTIVATE study. Int J Drug Policy. 2017;47:230–8. https://doi.org/10.1016/j.drugpo.2017.05.040.
Turner KM, Hutchinson S, Vickerman P, Hope V, Craine N, Palmateer N, et al. The impact of needle and syringe provision and opiate substitution therapy on the incidence of hepatitis C virus in injecting drug users: pooling of UK evidence. Addiction. 2011;106(11):1978–88. https://doi.org/10.1111/j.1360-0443.2011.03515.x.
Palmateer NE, Taylor A, Goldberg DJ, Munro A, Aitken C, Shepherd SJ, et al. Rapid decline in HCV incidence among people who inject drugs associated with national scale-up in coverage of a combination of harm reduction interventions. PLoS One. 2014;9(8):e104515. https://doi.org/10.1371/journal.pone.0104515.
Ayanga D, Shorter D, Kosten TR. Update on pharmacotherapy for treatment of opioid use disorder. Expert Opin Pharmacother. 2016;17(17):2307–18. https://doi.org/10.1080/14656566.2016.1244529.
Bart G. Maintenance medication for opiate addiction: the foundation of recovery. J Addict Dis. 2012;31(3):207–25. https://doi.org/10.1080/10550887.2012.694598.
Rosenblatt RA, Andrilla CH, Catlin M, Larson EH. Geographic and specialty distribution of US physicians trained to treat opioid use disorder. Ann Fam Med. 2015;13(1):23–6. https://doi.org/10.1370/afm.1735.
DeFlavio JR, Rolin SA, Nordstrom BR, Kazal LA Jr. Analysis of barriers to adoption of buprenorphine maintenance therapy by family physicians. Rural Remote Health. 2015;15:3019.
Jones EB. Medication-assisted opioid treatment prescribers in federally qualified health centers: capacity lags in rural areas. J Rural Health. 2017;34:14–22. https://doi.org/10.1111/jrh.12260.
Gonzalez SA, Fierer DS, Talal AH. Medical and behavioral approaches to engage people who inject drugs into care for hepatitis C virus infection. Addict Disord Their Treat. 2017;16(2 Suppl 1):S1–S23. https://doi.org/10.1097/ADT.0000000000000104.
Edlin BR, Eckhardt BJ, Shu MA, Holmberg SD, Swan T. Toward a more accurate estimate of the prevalence of hepatitis C in the United States. Hepatology. 2015;62(5):1353–63. https://doi.org/10.1002/hep.27978.
Office of National AIDS Policy. https://www.whitehouse.gov/onap. Accessed 23 Oct 2017.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
Charitha Gowda declares no conflicts of interest.
Vincent Lo Re reports grants from AstraZeneca and reports having served on the committee convened by the National Academies of Sciences, Engineering, and Medicine to outline a national strategy for HCV elimination, outside the submitted work.
Human and Animal Rights and Informed Consent
This article does not contain any studies with human or animal subjects performed by any of the authors.
Additional information
This article is part of the Topical Collection on Hepatitis C
Rights and permissions
About this article

Cite this article
Gowda, C., Lo Re, V. Strategies for the Elimination of Hepatitis C Virus Infection as a Public Health Threat in the United States. Curr Hepatology Rep 17, 111–120 (2018). https://doi.org/10.1007/s11901-018-0394-x
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11901-018-0394-x