
Abstract
Low-density lipoproteins (LDL) play a causal role in the development of atherosclerosis, and reduction of LDL cholesterol with a statin is a cornerstone in prevention of cardiovascular disease. However, it remains an unmet need to reduce the residual risk on maximally tolerated statin alone or in combination with other drugs such as ezetimibe. Among the new LDL-lowering therapies, PCSK9 inhibitors appear the most promising class. Genetic studies suggest that triglyceride-rich lipoproteins are associated with cardiovascular risk and several promising triglyceride-lowering therapies are at various stages of development. At the opposite end, high-density lipoprotein (HDL) cholesterol seems to not be causally associated with cardiovascular risk, and thus far, trials designed to reduce cardiovascular risk by mainly raising HDL cholesterol levels have been disappointing. Nevertheless, new drugs targeting HDL are still in development. This review describes the new drugs reducing LDL, apolipoprotein(a), and triglyceride-rich lipoproteins, and the strategies to modulate HDL metabolism.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
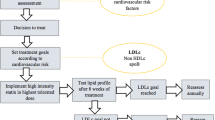
Consistent findings from clinical endpoint trials and from genetic studies have reaffirmed the causal role of low-density lipoprotein cholesterol (LDL-C) concentration in the development of atherosclerotic cardiovascular disease (ASCVD) [1]. Lowering LDL-C with a statin reduces the risk of ASCVD and all-cause mortality [2, 3], and statin therapy is endorsed by international guidelines as first-line therapy for cholesterol-lowering management in patients with ASCVD risk [4, 5].
Despite an increased use of statin therapy, a large proportion of patients with high ASCVD risk fail to achieve optimal LDL-C lowering on statin monotherapy, including those on high-dose statins [6]. Recently, ezetimibe added to statin therapy was found to reduce cardiovascular (CV) events in acute coronary syndrome patients more than statins alone [7]; further reduction of CV events was related to the magnitude of LDL-C lowering as demonstrated for statin therapy. However, there are patient populations either unable to achieve optimal LDL-C levels despite statin and ezetimibe combination therapy, or intolerant to statins, particularly at a high dose [8].
In clinical practice, a substantial number of patients at high and very high risk of ASCVD require LDL-C lowering larger than currently achievable with statins alone or in combination with other available lipid-lowering drugs such as ezetimibe. Moreover, other lipoprotein abnormalities particularly elevated triglyceride-rich lipoprotein levels, with/without low levels of high-density lipoprotein cholesterol (HDL-C), have been linked to the residual cardiovascular risk on statin therapy. Even if the residual risk can also be reduced by a better control of associated CV risk factors such as blood pressure, smoking, or lack of physical activity, it remains an important need for efficacious agents to decrease LDL-C and triglyceride-rich lipoproteins, and to modulate HDL metabolism.
New Drugs Targeting LDL Metabolism
Despite the availability of statins, ezetimibe, and other classes of drugs lowering LDL such as bile acid sequestrants, there remains an intense interest in the development of new LDL-lowering agents (Table 1); some agents have been already approved and others are still in clinical development. Among all the drugs listed in Table 1, the most exciting and promising class is certainly proprotein convertase subtilisin/kexin type 9 (PCSK9) inhibitors.
PCSK9 Inhibitors
Recent comprehensive reviews have described the discovery, genetics, structure, and function of PCSK9 in regulating LDL-C levels [9–12, 13•]. In summary, since the discovery of PCSK9 in 2003 [14, 15], it has been well established that PCSK9 regulates cholesterol metabolism mainly by targeting the LDL receptor for degradation in the liver: Gain-of-function mutations in PCSK9 are one of the genetic causes of autosomal dominant hypercholesterolemia [15]. Conversely, low-of-function mutations are associated with lower concentrations of LDL-C and reduced coronary heart disease [16, 17]. PCSK9, secreted into the plasma by the liver, binds the LDL receptor of the surface of hepatocyte and induces modification of LDL receptor conformation, avoiding normal recycling of LDL receptor, enhancing its degradation in endosomes/lysosomes and resulting in reduced clearance of LDL particles. By consequence, PCSK9 inhibition is a very attractive strategy for lowering LDL-C and enhancing the efficacy of statin treatment.
Several therapeutic approaches to the inhibition of PCSK9 have been proposed [18, 19•], targeting either extracellular PCSK9 by monoclonal antibodies (mAbs) or adnectins, or intracellular PCSK9 by antisense oligonucleotides (ASOs) or small interfering RNA (siRNA). The development of two ASOs was stopped in phase I due to safety concerns. In a phase I trial of ALN-PCS, a siRNA inhibitor of PCSK9 developed by Alnylan Pharmaceuticals, a dose-dependent reduction in LDL-C was observed, with a 40 % reduction with the highest dose, associated with a 70 % reduction in plasma PCSK9 levels [20]. However, in this trial, ALN-PCS was administered intravenously and healthy subjects required premedication with dexamethasone and antihistamines. A new formulation has been developed for subcutaneous (SC) administration, and in recent phase I trial, this new formulation was generally well tolerated, with similar LDL-C reduction to data reported for mAbs in subjects with and without statin coadministration [21]. The durability of the effect on LDL-C and PCSK9 levels supporting a biannual dose regimen needs to be confirmed in larger studies, and this agent will enter in phase II. Inhibition of PCSK9 binding to LDL receptor by adnectins such as BMS-962476 are in phase I [19•]. An alternative approach for PCSK9 inhibition could be a peptide-based anti-PCSK9 vaccine to provide a long-term LDL-C management [22]. Finally, mAbs are the most studied and advanced approach with two mAbs approved in 2015 alirocumab [23•] and evolocumab [24•], and two other with published phase II data, bococizumab [25] and LY3015014 [26].
Efficacy of PCSK9 Inhibition with mAbs
Globally, in combination with a statin or in monotherapy, mAbs induced dramatic significant decreases in LDL-C (from 45 to 70 %) and in all the other atherogenic parameters non-HDL-C, apolipoprotein(apo)B, and also lipoprotein(a) (Lp(a)). Three large phase III programs have been developed with alirocumab, evolocumab, and bococizumab administered as SC injections every 2 weeks or every 4 weeks. So far, in the phase III trials published with alirocumab and evolocumab, the efficacy has been demonstrated:
-
In patients with heterozygous familial hypercholesterolemia (FH) [27••, 28] and with homozygous FH [29••]
-
In high-risk patients not controlled by maximally tolerated statin and other lipid lowering therapies [30••, 31, 32]
-
In combination with statins in patients with high LDL-C [33–36]
-
In patients who could not tolerate statins due to muscle-related side effects [39, 40]
Encouraging findings suggesting that PCSK9 mAbs can decrease CV events have been observed from exploratory or post hoc analysis as part of the longer term safety trials ODYSSEY LONG TERM with alirocumab [30••] and OSLER with evolocumab [41••]. Moreover, meta-analyses of phase II and III trials found reduced total mortality with alirocumab and evolocumab, in trials ranging from 12 to 78 weeks [42, 43], with several limitations in these analyses, particularly due to the limited number of either CV events or deaths. Whether PCSK9 mAbs definitively reduce the incidence of CV events in patients on statin therapy shall be demonstrated with the four ongoing CV outcome trials [44–47] including more than 70,000 high-risk patients (Table 2).
To date, alirocumab and evolocumab SC injections appeared well-tolerated in trials up to 78 weeks in duration. Injection site reactions were relatively rare and mild. Neurocognitive events were reported more frequently with both alirocumab in ODYSSEY LONG TERM (1.2 vs 0.5 %) and evolocumab in OSLER-1 and OSLER-2 (0.9 vs 0.3 %) [30••, 41••]. The possibility that PCSK9 inhibitors may induce neurocognitive disorders is evaluated by the ongoing EBBINGHAUS trial [48], realized in a substudy of FOURIER trial [44]. Concerns regarding the risk of very low LDL-C levels have been addressed in complementary analysis of long-term safety trials over 78 weeks of treatment [30••, 41••]: No excess of adverse events has emerged in patients with LDL-C <25 mg/dL.
PCSK9 inhibition may become a major breakthrough in prevention of ASCVD [49]. Results of ongoing outcomes studies shall be crucial to evaluate the cost-effectiveness of PCSK9 inhibitor treatment [50].
Mipomersen
Mipomersen is an ASO that specifically blocks the messenger RNA (mRNA) translation into apoB and thereby the synthesis of apoB-containing lipoproteins. Mipomersen 200 mg in SC injections once weekly decreases LDL-C, apoB, and Lp(a) by 25–35 % in patients with severe hypercholesterolemia, including heterozygous and homozygous FH [51]. However, side effects are frequently related to either injection site reactions and flu-like symptoms, or hepatic fat accumulation and transaminases elevations. In a long-term evaluation of efficacy and safety, 55 % of the patients discontinued treatment within the first 2 years of treatment [52]. By consequence, the drug was approved by the FDA with a box warning only for homozygous FH. The approval has been refused by EMA due to side-effects. In the specific population of homozygous FH, mipomersen decreased LDL-C, apoB, and Lp(a) by ≈25 % [53].
Lomitapide
Microsomal triglyceride transfer protein (MTP) is essential for assembly and secretion of very-low-density lipoproteins (VLDL) in the liver and of chylomicrons in the intestine. Several MTP inhibitors have been tested in humans, most abandoned due to poor gastrointestinal tolerability, elevations in hepatic transaminases and increase of hepatic steatosis [54]. However, lomitapide, an oral MTP inhibitor, has been approved by both FDA and EMA for patients with homozygous FH. This approval has been based on the results of an open-label study in 29 homozygous FH patients [55]. In this trial, lomitapide started at a dose of 5 mg/day and titrated at 4-week intervals to a maximum of 60 mg daily has reduced LDL-C by 50 % at week 26 and 38 % at week 78. The efficacy was similar for patients with or without apheresis [56]. However, despite the LDL-C lowering effect, the poor tolerability and side effects (increases in liver enzymes and hepatic steatosis) should limit the use of lomitapide to negative-negative LDL receptor homozygous FH patients.
Bempedoic Acid (ETC-1002)
Bempedoic acid (ETC-1002) is an oral agent with a novel dual mechanism of action: By inhibiting ATP citrate lyase, the drug can decrease LDL-C, and by activation of AMP kinase, beneficial effects on glucose, lipids, inflammation, and weight gain could be expected, suggesting a development for patient with hypercholesterolemia and type 2 diabetes [57]. In patients with hypercholesterolemia, ETC-1002 reduced LDL-C levels up to 27 % in a phase II trial [58]. In patients with type 2 diabetes, ETC-1002 120 mg/day significantly lowered LDL-C by 43 % (vs 4 % with placebo) and high-sensitivity C-reactive protein (hsCRP) by 41 % (vs 11 % with placebo) [57]. In patients with or without statin intolerance, ETC-1002 lowered LDL-C and hs-CRP more than ezetimibe and the combination of ETC-1002 and ezetimibe induced an additive effect in terms of LDL-C reduction [59]. Larger phase III trials are required to assess long-term efficacy and safety.
Gemcabene
Gemcabene is an oral drug initially evaluated for a broad use in hypercholesterolemia, but with moderate LDL-C lowering effect (up to 25 %) [60]. The mechanisms of action include an inhibition of acetyl CoA carboxylase and an enhancement of VLDL clearance by decreasing apoCIII. The drug is now planned to be developed for use in homozygous FH based on mechanism of action and preclinical animal data.
CAT-2054
CAT-2054, a conjugate of eicosapentaenoic acid and niacin, is a novel inhibitor of the sterol response element-binding protein (SREBP) transcription factor. CAT-2054 does not activate the GPR109A receptor that causes flushing. In preclinical studies, CAT-2054 reduced plasma LDL-C and PCSK9 in nonhuman primates. A phase I trial has been recently presented [61], and the drug is planned to enter phase II.
New Drugs Targeting Triglyceride-Rich Lipoproteins
The causal relevance of high fasting and non-fasting triglyceride (TG) levels for an increased risk of ASCVD has been largely debated [62]. Indeed in observational studies, the relationship between TG and ASCVD risk is attenuated after adjustment for associated variables, including HDL-C [63]. However, post hoc analyses of statin trials [64, 65] suggest that higher levels of TG-rich lipoproteins correlate with residual risk. The action of lipases on VLDL and chylomicrons results in the formation of remnant particles with increased cholesterol content and potential role for atherogenicity [62, 66]. Moreover, recent genetic studies highly support a causal role for TG-rich lipoproteins in ASCVD risk [67–70] and identify potential targets for TG reduction. Several new drugs specifically aimed at reducing TG are being developed.
New Omega-3 Fatty Acid Preparations
Two new omega-3 fatty acid (FA) formulations have been developed: Vascepa® containing eicosapentaenoic acid (EPA) ethyl esters and Epanova® containing free FA formulations of EPA and docosahexaenoic acid (DHA). These two formulations reduced plasma TG by around 30 % at a 4 g daily dose [71, 72]. These formulations are currently evaluated in long-term outcome trials, REDUCE-IT for Vascepa® [73] and STRENGTH for Epanova® [74] in high cardiovascular risk patients with hypertriglyceridemia on optimal statin therapy.
ApoC3 Antisense Oligonucleotide
Loss-of-function variants in the gene of ApoC3 encoding the protein apoC-III known to inhibit lipoprotein lipase and to enhance intrahepatic production of VLDL are associated with reduced TG levels and decreased ASCVD risk [69, 70], suggesting that ApoC3 inhibitors should be an adequate target.
An ASO targeted to the ApoC3 mRNA in the liver, volanesorsen (formerly ISIS 304801), has been shown to reduce TG levels by 56–86 % in three patients with familial chylomicronemia syndrome [75•]. This effect was confirmed in a phase II trial conducted in hypertriglyceridemic patients with or without fibrate therapy [76•]. Treatment with volanesorsen resulted in dose-dependent decreases in both plasma ApoC3 and triglyceride levels up to 70–80 %. Phase III studies are ongoing.
Angiopoietin-Like Protein Inhibitors
Angiopoietin-like proteins (ANGPTLs) 3 and 4 are other inhibitors of the activity of lipoprotein lipase. Inhibition of ANGPTLs 3 and 4 using neutralizing mAbs (such as REGN 1500) has been reported to reduce TG levels in animal models [77, 78]. Early human clinical trials are ongoing.
New PPAR-α Agonists
Peroxisome proliferator-activated receptor (PPAR)-α agonists are an old class of drugs known to decrease TG and ApoC3 levels. However, clinical outcome trials have not yielded consistent results [72], even if a prespecified subgroup of ACCORD trial highly suggests a beneficial effect of fenofibrate/simvastatin therapy for diabetic patients with high TG and low HDL-C on simvastatin. The development of new PPAR-α agonists more potent and selective such as Pemafibrate (K-877) [79] remains of interest. The clinical efficacy of Pemafibrate shall be evaluated in a landmark trial named PROMINENT recently decided.
Lipoprotein Lipase Gene Therapy
Alipogene tiparvovec gene therapy has been approved by EMA in 2012. Alipogene tiparvovec is administered through intramuscular injections of an adeno-associated virus vector [80]. This strategy is intended to treat rare patients with LPL deficiency and severe or multiple pancreatitis attacks, despite dietary fat restrictions.
New Drugs Targeting HDL Metabolism
Although HDL-C levels are strongly inversely associated with ASCVD risk, the causal role of HDL-C is uncertain and is complicated by the inverse relationship between HDL-C and TG levels. Moreover, human genetic studies have led to major doubts about the causality of HDL-C levels in atherosclerosis [81, 82]. However, HDL-targeted therapies need to be explored as strategies that aim to normalize HDL function [83]. Indeed, recent epidemiological studies have shown that HDL cholesterol efflux capacity predicts ASCVD risk, independently of HDL-C levels [84], and it remains of interest to evaluate new strategies modulating HDL metabolism.
CETP Inhibitors
Cholesteryl ester transfer protein (CETP) transfers cholesteryl esters from HDL to proatherogenic lipoproteins. Even if some human genetic studies have concluded that CETP gene polymorphisms associated with decreased CETP activity are accompanied by a lower ASCVD risk, all the genetic variations at the CETP gene locus are not conclusive in terms of CV risk [85•] and three different CETP inhibitors—torcetrapib, dalcetrapib, and evacetrapib—have failed in large clinical outcome trials. Two other CETP inhibitors are still in development (anacetrapib and TA-8995). These two drugs induce large significant increases in HDL-C and ApoA-I and decreases in LDL-C (up to 45 % with TA-8995) [86, 87]. However, the future of CETP inhibition will depend on the results of the ongoing REVEAL trial in which >30,000 high-risk patients have been randomized to receive anacetrapib or placebo [88].
HDL Infusion Agents
Approaches to promote cholesterol efflux could be the infusion of reconstituted HDL (rHDL) containing ApoA-I and phospholipids. Indeed, in 2003, a small clinical trial has demonstrated that infusions of ApoA-I Milano (ETC-216) induced a modest reduction in atheroma volume [89]. Three rHDL are currently in clinical development MDCO-216 (originally ETC-216), CSL-112, and CER-001 with some published data reporting a positive role on reverse cholesterol transport and carotid atherosclerosis [90–92] and supporting further clinical investigations.
ApoA-I Upregulators
Another approach to promote cholesterol efflux from tissues is an increase of the endogenous production of ApoA-I by stimulating its gene transcription. The oral drug RVX-208 increased Apo-AI and HDL-C levels, and enhanced serum cholesterol efflux capacity [93]. However, in the ASSURE trial, RVX-208 treatment has not been associated with regression of coronary atherosclerosis evaluated by serial intravascular ultrasound imaging [94].
Strategies Targeting Lipoprotein(a)
The consistent association between elevated Lp(a) levels and increased ASCVD risk, together with genetic findings, indicates that elevated Lp(a) is a causal risk factor for ASCVD [95, 96]. By consequence, lowering Lp(a) is a new target in CV prevention [97]. Some new drugs previously described such as PCSK9 inhibitors, mipomersen, lomitapide, and CETP inhibitors also decreased Lp(a) usually by around 25–30 %, but the clinical significance of this effect is unknown. Highly specific and potent Lp(a) lowering strategy would provide the opportunity to demonstrate that lowering Lp(a) leads to a reduction in ASCVD.
Antisense Therapy Targeting Lp(a)
ASO ISIS-Apo(a)RX was designed to reduce the synthesis of apo(a) in the liver and consequently to decrease the plasma levels of Lp(a). In a phase I study, SC injections of ISIS-Apo(a)RX (100–300 mg) resulted in dose-dependent, selective reductions of plasma Lp(a) up to 78 % in the 300-mg group [98••].
Conclusion
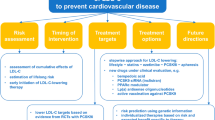
Clinical trials and genetic studies have demonstrated the cause role of LDL in the development of ASCVD. Although statins represent the cornerstone of dyslipidemia management, ezetimibe is also effective to reduce CV risk. However, the need for complementary agents reducting LDL-C remains important, especially for patients unable to achieve optimal LDL-C on current available therapies and for patients unable to tolerate efficacious statins. Among the new LDL-lowering drugs, PCSK9 inhibitors are certainly the most promising class. The ongoing CV endpoint trials using PCSK9 monoclonal antibodies shall be crucial not only in terms of CV prevention but also to appreciate the cost-effectiveness of this approach.
Recent genetic studies also support a causal role of TG-rich lipoproteins in the risk of ASCVD. Consequently, new clinical endpoint trials with either newer generation of omega-3 FA or PPAR-α agonist have been designed to evaluate the CV benefit in patients with elevated triglycerides on maximally tolerated statin therapy. Moreover, genetic studies have identified new strategies targeting TG such as apoC3 inhibitors. The development of new drugs increasing HDL-C has been disappointing, and the future of CETP inhibitors is linked to the results of the ongoing REVEAL trial. Other strategies to modulate HDL metabolism are at the early stage of development. Finally, promising preliminary data to reduce Lp(a) have been published with specific oligonucleotides blocking the synthesis of apo(a).
References
Papers of particular interest, published recently, have been highlighted as: • Of importance •• Of major importance
Catapano AL, Ference BA. IMPROVE-IT and genetics reaffirm the causal role of LDL in cardiovascular disease. Atherosclerosis. 2015;241:498–501.
Cholesterol Treatment Trialists’ (CTT) Collaborators. Efficacy and safety of cholesterol-lowering treatment: prospective meta-analysis of data from 90,056 participants in 14 randomised trials of statins. Lancet. 2005;366:1267–78.
Cholesterol Treatment Trialists’ (CTT) Collaboration. Efficacy and safety of more intensive lowering of LDL cholesterol: a meta-analysis of data from 170,000 participants in 26 randomised trials. Lancet. 2010;376:1670–81.
The Fifth Joint Task Force of the European Society of Cardiology and Other Societies on Cardiovascular Disease Prevention in Clinical Practice (constituted by representatives of nine societies and by invited experts). European guidelines on cardiovascular disease prevention in clinical practice (version 2012). Eur Heart J. 2012;33:1635–701.
Stone NJ, Robinson J, Lichtenstein AH, et al. 2013 ACC/AHA guideline on the treatment of blood cholesterol to reduce atherosclerotic cardiovascular risk in adults. A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation. 2014;129(25 Suppl 2):S1–45.
Boekholdt SM, Hovingh GK, Mora S, et al. Very low levels of atherogenic lipoproteins and the risk for cardiovascular events. J Am Coll Cardiol. 2014;64:485–94.
Cannon CP, Blazing MA, Giugliano RP, for the IMPROVE-IT investigators, et al. Ezetimibe added to statin therapy after acute coronary syndromes. N Engl J Med. 2015;372:2387–97.
Stroes ES, Thompson PD, Corsini A, et al. Statin-associated muscle symptoms: impact on statin therapy - European Atherosclerosis Society Consensus Panel Statement on Assessment, Aetiology and Management. Eur Heart J. 2015;36:1012–22.
Seidah NG, Awan Z, Chrétien M, et al. PCSK9. A key modulator of cardiovascular health. Circ Res. 2014;114:1022–36.
Norata GD, Tibolla G, Catapano AL. PCSK9 inhibition for the treatment of hypercholesterolemia: promises and emerging challenges. Vascul Pharmacol. 2014;62:103–11.
Marais AD, Kim JB, Wasserman SM, et al. PCSK9 inhibition in LDL cholesterol reduction: genetics and therapeutic implications of very low plasma lipoprotein levels. Pharmacol Ther. 2015;145:58–66.
Shimada YJ, Cannon CP. PCSK9 (proprotein convertase subtilisin/kexin type 9) inhibitors: past, present, and the future. Eur Heart J. 2015;36:2415–24.
Bergeron N, Phan BAP, Ding Y, et al. Proprotein convertase subtilisin/kexin type 9 inhibition. A new therapeutic mechanism for reducing cardiovascular disease risk. Circulation. 2015;132:1648–66. A recent comprehensive review on PCSK9 function and PCSK9 inhibition.
Seidah NG, Benjannet S, Wickham L, et al. The secretory proprotein convertase neural apoptosis-regulated convertase 1 (NARC-1): liver regeneration and neuronal differentiation. Proc Natl Acad Sci U S A. 2003;100:928–33.
Abifadel M, Varret M, Rabes JP, et al. Mutations in PCSK9 cause autosomal dominant hypercholesterolemia. Nat Genet. 2003;34:154–6.
Cohen JC, Boerwinkle E, Mosley Jr TH, et al. Sequence variations in PCSK9, low LDL, and protection against coronary heart disease. N Engl J Med. 2006;354:1264–72.
Benn M, Nordestgaard BG, Grande P, et al. PCSK9 R46L, low-density lipoprotein cholesterol levels, and risk of ischemic heart disease: 3 independent studies and meta-analyses. J Am Coll Cardiol. 2010;55:2833–42.
Hedrick JA. Targeting PCSK9 for the treatment of hypercholesterolemia. Curr Opin Invest Drugs. 2009;10:938–46.
Turner T, Stein EA. Non-statin treatments for managing LDL cholesterol and their outcomes. Clin Ther. 2015;37:2751–69. Good review on new treatments targeting LDL metabolism.
Fitzgerald K, Frank-Kamenetsky M, Shulga-Morskaya S, et al. Effect of an RNA interference drug on the synthesis of proprotein convertase subtilisin/kexin type 9 (PCSK9) and the concentration of serum LDL cholesterol in healthy volunteers: a randomised, single-blind, placebo-controlled, phase 1 trial. Lancet. 2014;383:60–8.
Fitzgerald K, Simon A, White S, et al. ALN-PCSsc, an RNAi investigational agent that inhibits PCSK9 synthesis with the potential for effective bi-annual dosing. Presented at AHA scientific session 2015.
Galabova G, Brunner S, Winsauer G, et al. Peptide-based anti-PCSK9 vaccines – An approach for long-term LDLc management. PLoS One. 2014;9:e114469.
Farnier M. An evaluation of alirocumab for the treatment of hypercholesterolemia. Expert Rev Cardiovasc Ther. 2015;13:1307–23. Recent review on alirocumab.
Langslet G, Emery M, Wasserman SM. Evolocumab (AMG 145) for primary hypercholesterolemia. Expert Rev Cardiovasc Ther. 2015;13:477–88. Recent review on evolocumab.
Ballantyne CM, Neutel J, Cropp A, et al. Results of bococizumab, a monoclonal antibody against proprotein convertase subtilisin/kexin type 9, from a randomized, placebo-controlled, dose-ranging, study in statin-treated subjects with hypercholesterolemia. Am J Cardiol. 2015;115:1212–21.
Kastelein JJP, Nissen SE, Rader DJ, et al. Safety and efficacy of LY3015014, a monoclonal antibody to proprotein convertase subtilisin/kexin type 9 (PCSK9): a randomized, placebo-controlled phase 2 study. Eur Heart J. 2016; Jan 12: online.
Kastelein JJP, Ginsberg HN, Langslet G, et al. ODYSSEY FH I and FH II: 78-week results with alirocumab treatment in 735 patients with heterozygous familial hypercholesterolemia. Eur Heart J. 2015;36:2996–3003. Studies evaluating efficacy of alirocumab in two large cohorts of heterozygous FH.
Raal FJ, Stein EA, Dufour R, et al. PCSK9 inhibition with evolocumab (AMG 145) in heterozygous familial hypercholesterolemia (RUTHERFORD-2): a randomized, double-blind, placebo-controlled trial. Lancet. 2015;385:331–40.
Raal FJ, Honarpour N, Blom DJ, et al. Inhibition of PCSK9 with evolocumab in homozygous familial hypercholesterolaemia (TESLA Part B); a randomised, double-blind, placebo-controlled trial. Lancet. 2015;385:341–50. Study showing a significant effect of evolocumab for homozygous FH with residual LDL receptor activity.
Robinson JG, Farnier M, Krempf M, et al. For the ODYSSEY LONG TERM Investigators. Efficacy and safety of Alirocumab in reducing lipids and cardiovascular events. New Engl J Med. 2015;372:1489–99. Important phase III trial evaluating long term efficacy and safety of alirocumab, with a post-hoc analysis suggesting a cardiovascular benefit.
Kereiakes DJ, Robinson JG, Cannon CP, et al. Efficacy and safety of the proprotein convertase subtilisin/kexin type 9 inhibitor alirocumab among high cardiovascular risk patients on maximally tolerated statin therapy: the ODYSSEY COMBO I study. Am Heart J. 2015;169:906–15.
Cannon CP, Cariou B, Blom D, et al. Efficacy and safety of alirocumab in high cardiovascular risk patients with inadequately controlled hypercholesterolaemia on maximally tolerated doses of statins: the ODYSSEY COMBO II randomized controlled trial. Eur Heart J. 2015;36:1186–94.
Robinson JG, Nedergaard BS, Rogers WJ, et al. Effect of evolocumab or ezetimibe added to moderate- or high-intensity statin therapy on LDL-C lowering in patients with hypercholesterolemia. JAMA. 2014;311:1870–82.
Blom DJ, Hala T, Bolognese M, et al. A 52-week placebo-controlled trial of evolocumab in hyperlipidemia. N Engl J Med. 2014;370:1809–19.
Farnier M, Jones P, Severance R, et al. Efficacy and safety of adding alirocumab to rosuvastatin versus adding ezetimibe or doubling the rosuvastatin dose in high cardiovascular-risk patients: the ODYSSEY OPTIONS II randomized trial. Atherosclerosis. 2016;244:138–46.
Bays H, Gaudet D, Weiss R, et al. Alirocumab as add-on to atorvastatin versus other lipid treatment strategies: ODYSSEY OPTIONS I randomized trial. J Clin Endocrinol Metab. 2015;100:3140–8.
Roth EM, Taskinen MR, Ginsberg HN, et al. Monotherapy with the PCSK9 inhibitor alirocumab versus ezetimibe in patients with hypercholesterolemia: results of a 24 week, double-blind, randomized Phase 3 trial. Int J Cardiol. 2014;176:55–61.
Koren MJ, Lundqvist P, Bolognese M, et al. Anti-PCSK9 monotherapy for hypercholesterolemia – the MENDEL-2 randomized, controlled phase 3 clinical trial of evolocumab. J Am Coll Cardiol. 2014;63:2531–40.
Stroes E, Colquhoun D, Sullivan D, et al. Anti-PCSK9 antibody effectively lowers cholesterol in patients with statin intolerance: the GAUSS-2 randomized, placebo-controlled phase 3 clinical trial of evolocumab. J Am Coll Cardiol. 2014;63:2541–8.
Moriarty PM, Thompson PD, Cannon CP, for the ODYSSEY ALTERNATIVE Investigators, et al. Efficacy and safety of alirocumab vs ezetimibe in statin-intolerant patients, with a statin rechallenge arm: the ODYSSEY ALTERNATIVE randomized trial. J Clin Lipidol. 2015;9:758–69.
Sabatine MS, Giugliano RP, Wiviott SD, for the Open-Label Study of Long-Term Evaluation against LDL Cholesterol (OSLER) Investigators, et al. Efficacy and safety of evolocumab in reducing lipids and cardiovascular events. N Engl J Med. 2015;372:1500–9. Important phase III trial suggesting a cardiovascular benefit after one year of evolocumab treatment.
Navarese EP, Kolodziejczak M, Schulze V, et al. Effects of proprotein convertase subtilisin/kexin type 9 antibodies in adults with hypercholesterolemia. A systematic review and meta-analysis. Ann Intern Med. 2015;163:40–51.
Lipinski MJ, Benedetto U, Escarcega RO, et al. The impact of proprotein convertase subtilisin-kexin type 9 serine protease inhibitors on lipid levels and outcomes in patients with primary hypercholesterolaemia: a network meta-analysis. Eur Heart J. 2016;37:536–45.
Sabatine MS, Giugliano RP, Keech A, et al. Rationale and design of the Further cardiovascular OUtcomes Research with PCSK9 Inhibition in subjects with Elevated Risk (FOURIER) trial. Am Heart J. 2016;173:94–101.
Schwartz GG, Bessac L, Berdan LG, et al. Effect of alirocumab, a monoclonal antibody to PCSK9, on long-term cardiovascular outcomes following acute coronary syndromes: rationale and design of the ODYSSEY outcomes trial. Am Heart J. 2014;168:682–9.e1.
SPIRE-1: The evaluation of Bococizumab (PF-04950615; RN316) in reducing the occurrence of major cardiovascular events in high risk subjects. www.clinicaltrials.gov, NCT 01975376, accessed on February 2016.
SPIRE-2: The evaluation of Bococizumab (PF-04950615; RN316) in reducing the occurrence of major cardiovascular events in high risk subjects. www.clinicaltrials.gov, NCT 01975389, accessed on February 2016.
EBBINGHAUS: Evaluating PCSK9 Binding antiBody Influence oN cognitive HeAlth in High cardiovascular Risk Subjects. www.clinicaltrials.gov, NCT02207634, accessed on February 2016.
Giugliano RP, Sabatine MS. Are PCSK9 inhibitors the next breakthrough in the cardiovascular field ? J Am Coll Cardiol. 2015;65:2638–51.
Tice JA, Kazi DS, Pearson SD. Proprotein convertase subtilisin/kexin type 9 (PCSK9) inhibitors for treatment of high cholesterol levels. Effectiveness and value. JAMA Intern Med. 2016;176:107–8.
Agarwala A, Jones P, Nambi V. The role of antisense oligonucleotide therapy in patients with familial hypercholesterolemia: risks, benefits, and management recommendations. Curr Atheroscler Rep. 2015;17:467.
Santos RD, Duell PB, East C, et al. Long-term efficacy and safety of mipomersen in patients with familial hypercholesterolaemia: 2-year interim results of an open-label extension. Eur Heart J. 2015;36:566–75.
Raal FJ, Santos RD, Blom DJ, et al. Mipomersen, an apolipoprotein B synthesis inhibitor, for lowering of LDL cholesterol concentrations in patients with homozygous familial hypercholesterolaemia: a randomised, double-blind, placebo-controlled trial. Lancet. 2010;375:998–1006.
Ahmad Z, Khera A. The role of microsomal triglyceride transfer protein inhibitors in the treatment of patients with familial hypercholesterolemia: risks, benefits, and management. Curr Atheroscler Rep. 2015;17:469.
Cuchel M, Meagher EA, du Toit Theron H, for the phase 3 HoFH Lomitapide Study Investigators, et al. Efficacy and safety of a microsomal triglyceride transfer protein inhibitor in patients with homozygous familial hypercholesterolaemia: a single-arm, open-label, phase 3 study. Lancet. 2013;381:40–6.
Stefanutti C, Blom DJ, Averna MR, for the phase 3 HoFH Lomitapide Study Investigators, et al. The lipid-lowering effects of lomitapide are unaffected by adjunctive apheresis in patients with homozygous familial hypercholesterolaemia – A post-hoc analysis of a Phase 3, single-arm, open-label trial. Atherosclerosis. 2015;240:408–14.
Gutierrez MJ, Rosenberg NL, MacDougall DE, et al. Efficacy and safety of ETC-1002, a novel investigational low-density lipoprotein-cholesterol-lowering therapy for the treatment of patients with hypercholesterolemia and type 2 diabetes mellitus. Arterioscler Thromb Vasc Biol. 2014;34:676–83.
Ballantyne CM, Davidson MH, MacDougall DE, et al. Efficacy and safety of a novel dual modulator of adenosine triphosphate-citrate lyase and adenosine monophosphate-activated protein kinase in patients with hypercholesterolemia. Results of a multicenter, randomized, double-blind, placebo-controlled, parallel-group trial. J Am Coll Cardiol. 2013;62:1154–62.
Thompson P, Ballantyne C, McKenney J, et al. ETC-1002 lowers LDL-C more than ezetimibe in patients with hypercholesterolemia with or without statin intolerance and has a similar safety and tolerability profile. J Am Coll Cardiol. 2015;65:A345.
Bays HE, McKenney JM, Dujovne CA, et al. Effectiveness and tolerance of a new lipid-altering agent, gemcabene, in patients with low levels of high-density lipoprotein cholesterol. Am J Cardiol. 2003;92:538–43.
Donovan JM, Mancini M, Sanabria C, et al. Phase 1 study of CAT-2054, an oral modulator of SREBP. J Clin Lipidol. 2015;9:474–5.
Nordestgaard B, Varbo A. Lipids and cardiovascular disease 3. Triglycerides and cardiovascular disease. Lancet. 2014;384:626–35.
Di Angelantonio E, Sarwar N, Perry P, et al. Major lipids, apolipoproteins, and risk of vascular disease. JAMA. 2009;302:1993–2000.
Miller M, Cannon CP, Murphy SA, for the PROVE-IT-TIMI 22 Investigations, et al. Impact of triglyceride levels beyond low-density lipoprotein cholesterol after acute coronary syndrome in the PROVE-IT TIMI 22 trial. J Am Coll Cardiol. 2008;51:724–30.
Schwartz GG, Abt M, Bao W, et al. Fasting triglycerides predict recurrent ischemic events in patients with acute coronary syndrome treated with statins. J Am Coll Cardiol. 2015;65:2267–75.
Varbo A, Benn M, Tybjærg-Hansen A, et al. Remnant cholesterol as a causal risk factor for ischemic heart disease. J Am Coll Cardiol. 2013;61:427–36.
Holmes MV, Asselbergs FW, Palmer TM, et al. Mendelian randomization of blood lipids for coronary heart disease. Eur Heart J. 2015;36:539–50.
Triglyceride Coronary Disease Genetics Consortium and Emerging Risk Factors Collaboration. Triglyceride-mediated pathways and coronary disease: collaborative analysis of 101 studies. Lancet. 2010;375:1634–39.
Jørgensen AB, Frikke-Schmidt R, Nordestgaard BG, et al. Loss-of-function mutations in APOC3 and risk of ischemic vascular disease. N Engl J Med. 2014;371:32–41.
The TG and HDL Working Group off the Exome Sequencing Project, National Heart, Lung, and Blood Institute. Loss-of-function mutations in APOC3, triglycerides and coronary disease. N Engl J Med. 2014;371:22–31.
Gryn SE, Hegele RA. Novel therapeutics in hypertriglyceridemia. Curr Opin Lipidol. 2015;26:484–91.
Sahebkar A, Chew GT, Watts GF. Recent advances in pharmacotherapy for hypertriglyceridemia. Prog Lipid Res. 2014;56:47–66.
REDUCE-IT: A study of AMR101 to evaluate its ability to reduce cardiovascular events in high risk patients with hypertriglyceridemia and on statin. www.clinicaltrials.gov, NCT 01492361, accessed on February 2016.
STRENGTH: Outcomes study to assess statin residual risk reduction with Epanova in high CV risk patients with hypertriglyceridemia. www.clinicaltrials.gov, NCT 02104817, accessed on February 2016.
Gaudet D, Brisson D, Tremblay K, et al. Targeting APOC3 in the familial chylomicronemia syndrome. N Engl J Med. 2014;371:2200–6. Proof-of-concept trial demonstrating ApoC3 inhibition would be effective to treat hyperchylomicronemia.
Gaudet D, Alexander VJ, Baker BF, et al. Antisense inhibition of apolipoprotein C-III in patients with hypertriglyceridemia. N Engl J Med. 2015;373:438–47. Important trial showing positive effects of ASO apoC3 inhibitor.
Gusarova V, Alexa CA, Wang Y, et al. ANGPTL3 blockade with a human monoclonal antibody reduces plasma lipids in dyslipidemic mice and monkeys. J Lipid Res. 2015;56:1308–17.
Wang Y, Gusarova V, Banfi S, et al. Inactivation if ANGPTL3 reduces hepatic VLDL- triglyceride secretion. J Lipid Res. 2015;56:1296–307.
Liu ZM, Hu M, Chan P, et al. Early investigational drugs targeting PPAR-alpha for the treatment of metabolic disease. Expert Opin Investig Drugs. 2015;24:611–21.
Ferreira W, Twisk J, Kwikkers K, et al. Immune responses to intramuscular administration of alipogene tiparvocec (AAV1-LPL(S447X)) in a phase II clinical trial of lipoprotein lipase deficiency gene therapy. Hum Gene Ther. 2014;25:180–8.
Voight BF, Peloso GM, Orho-Melander M, et al. Plasma HDL cholesterol and risk of myocardial infarction: a mendelian randomisation study. Lancet. 2012;380:572–80.
Nordestgaard BG, Tybjærg-Hansen A. Genetic determinants of LDL, lipoprotein(a), triglyceride-rich lipoproteins and HDL: concordance and discordance with cardiovascular disease risk. Curr Opin Lipidol. 2011;22:113–22.
Kingwell BA, Chapman MJ, Kontush A, et al. HDL-targeted therapies: progress, failures and future. Nat Rev. 2014;13:445–64.
Saleheen D, Scott R, Javad S, et al. Association of HDL cholesterol efflux capacity with incident coronary heart disease events: a prospective case-control study. Lancet Diabetes Endocrinol. 2015;3:507–13.
Gautier T, Masson D, Lagrost L. The potential of cholesteryl ester transfer protein as a therapeutic target. Exper Opin Ther Targets. 2016;20:47–59. Excellent review on the putative role of CETP inhibition.
Kastelein JJP, Besseling J, Shah S, et al. Anacetrapib as lipid-modifying therapy in patients with heterozygous familial hypercholesterolaemia (REALIZE): a randomized, double-blind, placebo controlled, phase 3 study. Lancet. 2015;385:2153–61.
Howingh GK, Kastelein JP, van Deventer SJH, et al. Cholesterol ester transfer protein inhibition by TA-8995 in patients with mild dyslipidaemia (TULIP); a randomised, double-blind, placebo-controlled phase 2 trial. Lancet. 2015;386:452–60.
REVEAL: Randomized EValuation of the Effects of Anacetrapib Through Lipid-modification. www.clinicaltrials.gov, NCT 01252953, accessed on February 2016.
Nissen SE, Tsunoda T, Tuzcu EM, et al. Effect of recombinant ApoA-I Milano on coronary atherosclerosis in patients with acute coronary syndromes: a randomized controlled trial. JAMA. 2003;290:2292–300.
Kootte RS, Smits LP, van der Valk FM, et al. Effect of open-label infusion of an apoA-1-containing particle (CER-001) on RCT and artery wall thickness in patients with FHA. J Lipid Res. 2015;56:703–12.
Hovingh GK, Smits LP, Stefanutti C, et al. The effect of an apolipoprotein A-I-containing high-density lipoprotein-mimetic particle (CER-001) on carotid artery wall thickness in patients with homozygous familial hypercholesterolemia: the Modifying Orphan Disease Evaluation (MODE) study. Am Heart J. 2015;169:736–42.e1.
Gille A, Easton R, D’Andrea D, et al. CSL112 enhances biomarkers of reverse cholesterol transport after single and multiple infusions in healthy subjects. Arterioscler Thromb Vasc Biol. 2014;34:2106–14.
Bailey D, Jahagirdar R, Gordon A, et al. RVX-208: a small molecule that increases apolipoprotein A-I and high-density lipoprotein cholesterol in vitro and in vivo. J Am Coll Cardiol. 2010;55:2580–9.
Nicholls SJ, Puri R, Wolski K, et al. Effect of the BET protein inhibitor, RVX-208, on progression of coronary atherosclerosis: results of the Phase 2b, randomized, double-blind, multicenter, ASSURE trial. Am J Cardiovasc Drugs. 2016;16:55–65.
Jacobson TA. Lipoprotein(a), cardiovascular disease, and contemporary management. Mayo Clin Proc. 2013;88:1294–311.
Nordestgaard BG, Chapman MJ, Ray K, et al. Lipoprotein(a) as a cardiovascular risk factor: current status. Eur Heart J. 2010;31:2844–53.
Van Capelleveen JC, van der Valk FM, Stroes ESG. Current therapies for lowering lipoprotein(a). J Lipid Res. 2015 Dec 4.
Tsimikas S, Viney NJ, Hughes SG, et al. Antisense therapy targeting apolipoprotein(a): a randomised, double-blind, placebo-controlled phase 1 study. Lancet. 2015;386:1472–83. First-trial with an ASO blocking apo(a) synthesis.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
Dr. Farnier reports having received grants, consulting fees, and/or honoraria, and delivering lectures for Abbott/Mylan, Amgen, AstraZeneca, Eli Lilly, Genzyme, Kowa, Merck and Co, Pfizer, Roche, Sanofi/Regeneron, and Servier.
Human and Animal Rights and Informed Consent
This article does not contain any studies with human or animal subjects performed by any of the authors.
Additional information
This article is part of the Topical Collection on Lipid Abnormalities and Cardiovascular Prevention
Rights and permissions
About this article

Cite this article
Farnier, M. Future Lipid-Altering Therapeutic Options Targeting Residual Cardiovascular Risk. Curr Cardiol Rep 18, 65 (2016). https://doi.org/10.1007/s11886-016-0743-8
Published:
DOI: https://doi.org/10.1007/s11886-016-0743-8