
Abstract
The health impacts associated with exposure to elevated concentrations of fine particulate matter (PM2.5) are well recognised. There is a substantial number of studies characterising PM2.5 concentrations outdoors, as well as in homes within low- and middle-income countries. In high-income countries (HICs), there is a sizeable literature on indoor PM2.5 relating to smoking, but the evidence on exposure to PM2.5 generated from non-tobacco sources in homes is sparse. This is especially relevant as people living in HICs spend the majority of their time at home, and in the northern hemisphere households often have low air exchange rates for energy efficiency. This review identified 49 studies that described indoor PM2.5 concentrations generated from a variety of common household sources in real-life home settings in HICs. These included wood/solid fuel burning appliances, cooking, candles, incense, cleaning and humidifiers. The reported concentrations varied widely, both between sources and within groups of the same source. The burning of solid fuels was found to generate the highest indoor PM2.5 concentrations. On occasion, other sources were also reported to be responsible for high PM2.5 concentrations; however, this was only in a few select examples. This review also highlights the many inconsistencies in the ways data are collected and reported. The variable methods of measurement and reporting make comparison and interpretation of data difficult. There is a need for standardisation of methods and agreed contextual data to make household PM2.5 data more useful in epidemiological studies and aid comparison of the impact of different interventions and policies.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
Introduction
Air pollution is a major hazard to public health globally, with nine out of ten people exposed to concentrations that exceed the World Health Organization (WHO) guidance limits. Poor outdoor air quality claims 4.2 million lives every year, and indoor air pollution accounts for 3.8 million annual deaths (World Health Organization 2021a). Particulate matter (PM) is one of the most common air pollutants that is associated with human health harms when it exceeds regulatory levels (Centers for Disease Control and Prevention 2021). PM2.5, PM less than 2.5 μm in diameter, is one of the most harmful pollutants to inhale due to its effects on health (Kelly and Fussell 2015; Schraufnagel et al. 2019).
The adverse health effects associated with exposure to PM2.5 are now well recognised in public health research. Studies have shown that exposure to elevated concentrations of PM2.5 is associated with an increased risk of hospitalisation for cardiopulmonary illnesses such as asthma, ischemic heart disease and cardiac failure (Du et al. 2016; Xing et al. 2016; Hayes et al. 2020). In addition to being linked to morbidity, chronic exposure to PM2.5 can also lead to a higher mortality risk for lung cancer and cardiovascular diseases (Arden Pope et al. 2011, 2020). The health effects of PM2.5 extend beyond the cardiopulmonary system. Recent studies have found associations between PM2.5 and the incidence of chronic kidney disease, type 2 diabetes and cerebrovascular disease (Li et al. 2017; Carey et al. 2018; Bowe et al. 2019; Ghazi et al. 2021). There is also emerging evidence to suggest that dementia, autism, depression and other mental health disorders may be related to long-term exposure (Lam et al. 2016; Braithwaite et al. 2019; Shi et al. 2020). Given the detrimental impact that PM2.5 has on health, there is a need to better understand how human exposure takes place. Characterising and investigating personal exposure to PM2.5 will help tackle emission sources and/or change behaviour to reduce exposure, which should, in turn, reduce the burden of air pollution-related illnesses.
PM2.5 is a ubiquitous pollutant coming from an array of emission sources. Although air pollution is most commonly associated with outdoor environments, PM2.5 generated from indoor sources and breathed in within the home setting is likely to make up a considerable proportion of total population inhaled dose. Even in the twenty-first century, 2.8 billion people still rely on burning solid fuels for heating, cooking and lighting (Bonjour et al. 2013). Indoor PM2.5 concentrations in low- and middle-income countries (LMICs) vary widely and are dependent on the type of combustion device and fuel used. Indoor concentrations of PM2.5 in LMICs often far exceed the WHO air quality guideline (AQG), which currently stand at 15 μg/m3 in 24 h and 5 μg/m3 annually (World Health Organization 2021b). For example, in homes with traditional solid fuel burning stoves in India (Arif and Parveen 2021), Mongolia (Lim et al. 2018) and Honduras (Young et al. 2019), mean 24-h indoor PM2.5 concentrations have been shown to exceed 200 μg/m3. Indoor air quality in LMICs has been extensively studied in recent decades owing to its associated adverse health impacts and implied socioeconomic inequalities. Investigation into indoor PM2.5 in LMICs continues, especially as interventions aimed at tackling the problem have had varied success (Budya and Yasir Arofat 2011; Hanna et al. 2012; Mortimer et al. 2017).
In contrast to LMICs, literature on indoor PM2.5 concentrations in high-income countries (HICs) is comparatively scarce despite it also being a relevant and substantial global problem. Some studies have characterised indoor PM2.5 concentrations in non-residential places within HICs, including offices (Jones et al. 2021), schools (Carrion-Matta et al. 2019), prisons (Semple et al. 2017), restaurants (El‐Sharkawy and Javed 2018) and other microenvironments. However, there are only a small number of studies that have characterised PM2.5 generated from sources in residential settings within HICs. It is important that the health impacts of household indoor PM2.5 levels in HICs are not overlooked, especially as people in HICs spend 90% of their time indoors, with almost 70% of that being at home (Klepeis et al. 2001; Delgado-Saborit et al. 2011), with even higher proportions of time spent at home during the COVID-19 pandemic (O’Donnell et al. 2021). By far, the most investigated source of PM2.5 within home settings in HICs is second-hand tobacco smoke. Studies consistently show that the concentration of indoor PM2.5 is significantly higher in smoking homes than non-smoking homes and often exceeds the WHO AQG (Semple et al. 2015; Zhang et al. 2020). The burning of solid or biomass fuels for the purpose of heating is one of the few non-tobacco household sources that has been investigated in HICs (Schluger 2014; Fleisch et al. 2020; Chakraborty et al. 2020). Other indoor PM2.5 sources have received little attention, despite their commonality within residential settings. These include cooking, cleaning and the combustion of material other than biomass fuel such as candles and incense.
The characterisation of PM2.5 in outdoor environments has been studied extensively in HICs. Databases have been compiled to show the longitudinal changes in outdoor PM2.5 concentrations, as well as indicating the real-time PM2.5 at local levels (Air Quality in Scotland 2022; Department for Environment Food & Rural Affairs 2022). There are also emerging citizen networks, such as PurpleAir that report both outdoor and indoor PM2.5 (PurpleAir 2022). Despite increasing awareness of the need to characterise indoor PM2.5, research into concentrations within home settings in HICs is relatively uncommon. In addition, most studies that report residential PM2.5 concentrations in HICs focus primarily on health outcomes (Habre et al. 2014; Karottki et al. 2014). It is often not obvious from the title of the articles that the studies involve measuring indoor PM2.5 thus making it difficult for those interested in the field to readily access or identify what has already been achieved. This systematic review, therefore, intends to identify, collate and appraise all relevant studies that investigate the indoor PM2.5 concentrations generated from common household sources in HICs and provide a comprehensive overview. The following research questions will be addressed in this systematic review:
-
1.
What are the indoor concentrations of PM2.5 generated from common sources (excluding tobacco or e-cigarettes) in homes within HICs?
-
2.
How do indoor concentrations of PM2.5 in homes within HICs compare to the WHO air quality guideline 2021?
-
3.
What are the methods used in existing studies to measure and report concentrations of PM2.5 in homes within HICs?
By reviewing the current literature and drawing comparisons between various sources of PM2.5, this review aims to highlight the direction in which future research in the field should focus, and ultimately benefit the health of people living in HICs who are at risk of exposure to elevated concentrations of PM2.5 at home.
Materials and methods
This systematic review was performed following the best practices outlined by the Centre for Reviews and Dissemination (Centre for Reviews and Dissemination 2009) and the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) (Page et al. 2021).
Search methods
A literature search was conducted using the PubMed database. The search strategy consisted of key terms covering three topic areas; air quality, emission source and setting. Search terms used to describe air quality included; indoor, home, residential, household, particulate matter and PM2.5. Exact names of household products or activities that generate indoor PM2.5 in home settings were used to search for emission source. Examples of these sources are woodstove, cooking fume, candle and humidifier. As for the setting, due to there being very few relevant studies conducted in HICs, the Boolean Logic “NOT” function was employed to exclude LMICs where studies concerning levels of indoor PM2.5 are most commonly conducted. Details of the search strings are provided in Supplementary Information 1. On the account of the envisaged scarcity of studies in the area of interest, there was no restriction on publication date and the search included all studies through to January 2022.
Eligibility criteria
Studies were included if they met the following eligibility criteria: (1) conducted in HICs as defined by the World Bank in 2021 as having a gross national income per capita above 12,695 USD (The World Bank 2021); (2) PM2.5 concentrations measured and reported in µg/m3; (3) PM2.5 concentrations measured in real-life indoor residential settings (i.e. not laboratory settings, or home settings with highly controlled variables); and (4) the exposure to PM2.5 was objectively measured and was not a subjective assessment or self-reported proxy for exposure. Studies were excluded if they were not published in English, or reported PM2.5 concentrations generated from tobacco combustion (e.g. cigarette or pipe smoking) or e-cigarette sources (vaping). A post hoc decision was made during full-text screening stage about studies that sampled in both smoking and non-smoking homes; studies were excluded if the reported data could not be separated from smoking and non-smoking households.
Selection process
The information from retrieved articles was imported into an Excel spreadsheet. After duplicates were removed, one researcher [SW] screened the titles and, where applicable, abstracts to identify relevant studies according to the eligibility criteria. Full-text articles were assessed if the relevance of a study was not obvious from its title or abstract. The second researcher [SS] randomly selected 10% of all retrieved articles and independently assessed the studies’ relevance to the research questions and whether they met the inclusion criteria. The random selection of the 10% sample was performed in R using Dplyr with the slice_sample function. The initial agreement on studies’ eligibility was 98% between the two researchers; discrepancies were resolved after discussion. Reference checking for additional relevant articles was carried out to maximise the capture of related studies; references were cited by the included studies as well as those citing the included studies.
Data extraction
A data extraction form was designed and piloted before its application to all included studies. The extracted data was organised into two categories, one being study characteristics such as sample size, enrolment period and country where the study was conducted and the other category being methods of exposure assessment in which the following data were recorded: PM2.5 source, sampling duration, measurement device, location of measurement, type of measurement (static or personal) and main findings. The data extraction was completed by one researcher [SW] with the second [SS] cross-checking approximately 10% (n = 7) of studies to identify and minimise errors. The sampling of studies for cross-checking was conducted through selection of the 4th row and then every subsequent 10th row thereafter on the data extraction spreadsheet.
Quality appraisal
The exposure assessment methods in included studies were appraised for their risk of bias. The appraisal was carried out using three criteria from the National Institutes of Health’s quality assessment tool for observational cohort and cross-sectional studies (National Institutes of Health 2021). The criteria were as follows:
-
1.
For exposures that can vary in amount or level, did the study examine different levels of the exposure as related to the outcome (e.g., categories of exposure, or exposure measured as continuous variable)?
-
2.
Were the exposure measures (independent variables) clearly defined, valid, reliable and implemented consistently across all study participants?
-
3.
Was the exposure(s) assessed more than once over time?
Studies that answered “yes” to all three criteria were rated as low risk of bias, one “no” as being medium risk and two “no’s” as having high risk. All studies were included in data synthesis despite their levels of risk of bias.
Results
Study selection
A total of 5553 articles were retrieved from the literature search on PubMed and by reference-checking. After removing 2167 duplicates, 2564 studies were excluded based on their titles and a further 677 on their abstracts. The remaining 145 articles proceeded onto the full-text screening stage in which 96 were excluded due to the following reasons: did not measure and report PM2.5 concentrations; measured PM2.5 concentrations in outdoor, non-residential locations, laboratories or home settings with highly controlled variables; did not objectively measure exposure to PM2.5; and could not separate data from smoking and non-smoking homes. Thus, 49 studies were included in this systematic review (Fig. 1).

Flow diagram of the study selection process
Study characteristics
Supplementary Information 2 details the main characteristics of included studies. There were 22 studies conducted in Europe; five in the UK (Wigzell et al. 2000; Nasir and Colbeck 2013; O’Leary et al. 2018; Chakraborty et al. 2020; Shehab et al. 2021); three in Portugal (Alves et al. 2020; Madureira et al. 2020; Marques and Pitarma 2020); two each in Sweden (Molnar et al. 2005; Omelekhina et al. 2022), Italy (Frasca et al. 2018; Pietrogrande et al. 2021) and Greece (Sarigiannis et al. 2014; Assimakopoulos et al. 2018); one each in Finland (Siponen et al. 2019), Norway (Wyss et al. 2016), Denmark (Karottki et al. 2014), Germany (Salthammer et al. 2014), Poland (Jedrychowski et al. 2006), Switzerland (Monn et al. 1997) and Belgium (Stranger et al. 2009); and one study was multicentric (UK and the Republic of Ireland) (Semple et al. 2012). There was only one study each from Asia (Japan) (Ohura et al. 2005), the Middle East (Kuwait) (Yassin et al. 2012), Oceania (Australia) (Mazaheri et al. 2018) and South America (Chile) (Rojas-Bracho et al. 2002). North America had the most studies, with 18 conducted in the USA (Abt et al. 2000; Brugge et al. 2003; Wallace et al. 2003; Rojas-Bracho et al. 2004; Allen et al. 2004, 2008; Olson and Burke 2006; Baxter et al. 2007; Brown et al. 2009; Hart et al. 2011; Ward et al. 2011; Noonan et al. 2012; Paulin et al. 2013; McNamara et al. 2013; Semmens et al. 2015; Fleisch et al. 2020; Zhao et al. 2020; Hadeed et al. 2021) and five in Canada (Allen et al. 2009; MacNeill et al. 2014; Wheeler et al. 2014; Jeong et al. 2019; Mendell et al. 2022). Included studies were published between 1997 and 2021 with 32 of 49 published since 2011 (Fig. 2).

Number of included studies published in each year
The two most common types of measurement methods used to quantity PM2.5 concentrations were utilised in equal proportion across the studies; optical and gravimetric devices were each employed in 24 studies, with one study using both optical and gravimetric methods. Static sampling was adopted in 37 studies, four placed devices on participants and eight studies used both static and personal placements. Table 1 provides details of placement methods within each type of device.
Out of 49 studies, 40 reported methods in measuring concurrent outdoor PM2.5 concentrations. Data on indoor and outdoor PM2.5 concentrations was available for 31of these studies (Supplementary Information 3) and was extracted. Indoor-to-outdoor (I/O) ratios for each of the studies with complete extractable datasets are presented in Fig. 3. Values > 1 indicate a higher indoor PM2.5 concentration than that measured outdoors.

Calculated I/O ratios of included studies
*I/O ratios are calculated based on measures of central tendency provided in individual original articles.
Of all included studies, 32 were rated as having a low risk of bias for their exposure assessment methods, 15 studies had medium risk, and only two were assessed as having high risk of bias. Most studies that were rated as medium risk were so, due to short sampling durations that would be insufficient in capturing behavioural variabilities; in this systematic review, insufficient sampling period was defined as being ≤ 72 h. The remaining medium risk studies failed to specify the location of sampling device placement, potentially resulting in measurement errors within individual included studies. Studies deemed as being at high risk of bias failed on both sampling duration and specificity of device placement.
Sources of exposure
Although many studies investigated exposure sources other than those listed in Supplementary Information 1, only original studies that reported concentration in μg/m3 were included in this systematic review. Studies that did not report actual measurements relating to a particular source, but instead provided general values of static or personal PM2.5 concentrations, are included in the analysis as having “no specific source”.
Woodstoves
Indoor PM2.5 generated from woodstoves was measured in a total of 15 studies. The reported PM2.5 concentrations varied widely between studies, with 24-h mean or median ranging from as high as 45.0 μg/m3 (Noonan et al. 2012) down to 4.1 μg/m3 (Siponen et al. 2019). Figure 4 illustrates the varied concentration in the ten studies that report PM2.5 in woodstove using homes in a 24-h period and how they compare with the WHO AQG level. Not all studies reported their PM2.5 concentrations over 24 h. Two studies reported 48-h average PM2.5 concentrations of 28.8 (Semmens et al. 2015) and 32.3 (McNamara et al. 2013) μg/m3. A further two gave PM2.5 concentrations as hourly means of 12.2 (Chakraborty et al. 2020) and 26.4 (Wyss et al. 2016) μg/m3. Only one study (Fleisch et al. 2020) reported a weekly median PM2.5 value as being 6.65 μg/m3.

Studies that reported woodstove related PM2.5 concentration in a 24-h period
Solid fuel burning
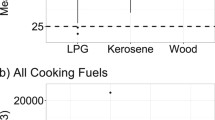
Six studies investigated PM2.5 concentrations associated with solid fuel appliances other than just wood combustion. Two studies examined biomass-burning fireplaces, with one reported the daily mean being 31.1 μg/m3 (Marques and Pitarma 2020), and the other estimated the 24-h mean PM2.5 concentration at 50 μg/m3 during a cold period whilst fireplaces were operating (Sarigiannis et al. 2014). One study investigated two types of solid fuel combustion, coal and peat burning, with 24-h mean PM2.5 concentrations measured at 7.4 and 10.9 μg/m3, respectively (Semple et al. 2012). Coal/wood burning stoves were examined by two studies; one reported the average PM2.5 concentration in August as being 22.9 μg/m3 and in December as 15.0 μg/m3 (Paulin et al. 2013), whilst the other gave mean personal exposure to PM2.5 when coal/wood stoves were in operation as 48.2 μg/m3 (Jedrychowski et al. 2006). The 24-h mean PM2.5 concentration associated with solid fuel burning in general was reported by one study, giving 12.5 μg/m3 in the non-heating season and 33.9 μg/m3 during the heating season (Hadeed et al. 2021).
Cooking
A total of 16 studies examined PM2.5 concentrations related to cooking. Like the previous two sources of exposure, there is a great deal of variation between studies in terms of time periods in which the measurements were reported and in the concentration values themselves. Three studies reported the peak PM2.5 concentration during cooking. Omelekhina et al. (2022) reported a single peak value as high as 3050 μg/m3, whereas the other two studies provided averaged peak values. Zhao’s et al. demonstrated 5-min median peak PM2.5 concentration of 37 μg/m3 (Zhao et al. 2020), whilst Noonan’s study reported a median peak value an order of magnitude higher at 305 μg/m3 (Noonan et al. 2012). Four studies reported their PM2.5 concentrations in 24-h periods, with the values from the three studies (Semple et al. 2012; Siponen et al. 2019; Pietrogrande et al. 2021) conducted in Europe being relatively similar to one another, ranging from 3.1 to 18.7 μg/m3, whilst a 24-h mean value of 54.7 μg/m3 reported from a study in Kuwait is significantly higher (Yassin et al. 2012). One study reported its PM2.5 concentration as an hourly mean (Wyss et al. 2016), and another two studies as 48-h means (Wigzell et al. 2000; Jedrychowski et al. 2006). The remaining six studies (Olson and Burke 2006; Baxter et al. 2007; O’Leary et al. 2018; Mazaheri et al. 2018; Alves et al. 2020; Shehab et al. 2021) (Table 2) reported their cooking related PM2.5 concentrations over various sampling durations, thus making them difficult to group and directly compare.
Candle and incense
Five studies characterised indoor PM2.5 associated with the use of candles and with a further one study investigating the burning of incense. The burning of incense was reported to increase indoor PM2.5 concentration by an average of 6 μg/m3 (Wallace et al. 2003). Two studies reported PM2.5 concentrations of 70 (Noonan et al. 2012) and 36 (Assimakopoulos et al. 2018) μg/m3 during candle burning, while the remaining three reported values over various time frame. For example, a mean hourly concentration of 20.3 μg/m3 was reported by Wyss et al. (2016); Jedrychowski et al. measured the 48-h mean personal exposure to PM2.5 during the burning of candles as being 45.6 μg/m3 (Jedrychowski et al. 2006); and the indoor daily median concentration in Siponen’s study was 4.2 μg/m3 (Siponen et al. 2019).
Cleaning
Two studies examined PM2.5 emission associated with household cleaning. One study reported the median peak PM2.5 during cleaning was 28 μg/m3 (Noonan et al. 2012), whereas the other found house cleaning activities led to a daily median indoor PM2.5 concentration of 4.5 μg/m3 (Siponen et al. 2019).
Humidifier
Only one study characterised PM2.5 associated with the use of a humidifier in a real-life setting; this is perhaps due to humidifiers not being common household items. Nevertheless, the use of a humidifier was shown to lead to an approximate five-fold increase when compared to ambient PM2.5 concentrations. From Brown’s study, the mean exposure was calculated to be 49.5 and 59.0 μg/m3 in winter and summer, respectively (Brown et al. 2009).
No specific source
As previously mentioned, not all studies related indoor PM2.5 concentrations to a specific emission source as 15 of the 49 studies measured general indoor PM2.5 levels at home. Despite the generality of these studies, they also show considerable variation in measurement and reporting methods. Abt used 12-h mean PM2.5 concentration across homes, reporting a value of 13.9 μg/m3 (Abt et al. 2000), whilst both Allen (Allen et al. 2004) and Jeong (Jeong et al. 2019) gave hourly mean concentrations between 5.9 to 8.7 μg/m3. Five studies reported means or medians over 24-h periods. Two of these studies had very similar values, with MacNeil reporting 6.78 μg/m3 in winter and 10.10 μg/m3 in summer (MacNeill et al. 2014), whilst Nasir’s saw PM2.5 concentrations of 6 and 9 μg/m3 in respective seasons (Nasir and Colbeck 2013). Stranger and Ohura also reported similar results, with Stranger reporting a mean PM2.5 concentration of 29.5 μg/m3 (Stranger et al. 2009), whilst Ohura found mean personal exposure in a living room during winter to be 35.3 μg/m3 and 16.5 μg/m3 in summer (Ohura et al. 2005). The one study conducted in Chile found 24-h mean personal exposure to be 69.5 μg/m3 and indoor static measurement to be 68.5 μg/m3 (Rojas-Bracho et al. 2002), which are significantly higher than the four studies conducted in Europe and North America. The remaining seven studies (Monn et al. 1997; Brugge et al. 2003; Rojas-Bracho et al. 2004; Allen et al. 2008; Karottki et al. 2014; Madureira et al. 2020; Mendell et al. 2022) investigating residential PM2.5 concentrations, not related to a particular source, all used a variety of measurement methods and reported their findings over time periods specified in the original articles (Table 3).
Discussion
This review identifies only 49 studies, spanning a period of nearly 25 years, that have measured and quantified concentrations of PM2.5 in non-smoking homes in HICs. Many countries appear to have no published data on typical household concentrations. In the small number of studies identified, there is considerable variability that is often difficult to interpret due to the lack of qualitative or contextual data on the sources and individual behaviours of household residents. The burning of wood and other solid fuels, cooking, the burning of candles and incense, house cleaning and the use of humidifiers have all been studied to varying extent and shown to lead to household indoor PM2.5 concentrations in HICs that exceed the WHO AQG. Despite the many differences in study design and methodology making direct comparison between studies and the extraction of meaningful conclusions difficult, wood/solid fuel burning appliances appear to be the most likely to produce high concentrations of PM2.5 with almost half of the included studies concerning this source reporting values above the WHO AQG 24-h level. Very few studies concerning other sources of exposure report such high PM2.5 concentrations, although there are examples for each source that stand out as having the ability to generate high concentrations.
Although this review has identified that household sources within HICs can lead to indoor PM2.5 concentrations that exceed the WHO AQG; however, they tend to be much lower than those reported in LMICs. For example, the mean indoor PM2.5 concentrations in kitchens with traditional biomass or solid fuel burning stoves in LMICs can be between 530 and 990 μg/m3 (Pope et al. 2017), whereas in this review, the highest reported concentrations associated with similar sources are in the region of 50 μg/m3 in a 24-h period. This echoes similar findings in Lim’s review that concludes the personal exposure to PM2.5 in HICs is much lower than countries in other classifications by income levels (Lim et al. 2022). The difference in indoor PM2.5 concentrations between smoking and non-smoking homes in HICs is another avenue for comparison. From the included studies within this review where samples were obtained from both smoking and non-smoking homes,Footnote 1 smoking, either from active smoking or second-hand smoke, led to indoor PM2.5 concentrations to increase by 5.7 to 37 μg/m3. It is important to be mindful of these values when comparing data and that there are many factors to consider when drawing conclusions from these results.
It is apparent from the review of literature that there are limited data on household indoor PM2.5 related to non-tobacco sources within HICs. These studies in HICs only started to emerge in the late 1990s with just two to three publications per year thereafter, culminating in a total of 49 studies. Despite the inherent difficulties of carrying out exposure assessment studies in LMICS, there is considerably more research in these settings. Due to the focus on indoor combustion in homes within LMICs, a systematic review conducted in 2017 identified 55 studies in LMICs that characterised indoor PM2.5 associated with the use of cookstoves (Quansah et al. 2017).
Within the literature on PM2.5 concentrations in homes within HICs, biomass and solid fuel burning for heating, followed by cooking fume, are the focus in most of the identified studies, whilst only a handful of studies investigated PM2.5 generated from house cleaning, the burning of candles and incense, and other PM-generating activities. There is also a geographical skew in the location of conducted studies, with the majority of studies carried out in North America and Europe. Other HICs, especially those in Asia, the Middle East, Oceania and South America, are seldom mentioned, creating significant gaps within the literature.
Within the limited literature on the indoor PM2.5 generated from household sources, there are two predominant methods utilised in the quantification of PM2.5; these are optical and gravimetric. Despite their widespread use within the field, there remain considerable differences, not only between measurement methods, but also within the two groups of devices, with variation arising between different models and brands based on the same measurement technology (Lanki et al. 2002; Wallace et al. 2011). At present, there appears to be no recognised standard procedure or calibration technique to correct for many of these differences. This problem in measurement is further complicated by the implementation of the measurement technique by researchers in different studies. Some studies use a static placement of the sampling device, whilst others adopt a personal device which yields PM2.5 concentrations as experienced by occupants within the study households (Adgate et al. 2003). This variability in measurement methods makes direct comparison across studies difficult. In addition to this challenge, results are reported using a wide range of averaging times and various measures of central tendency. For instance, studies that only report PM2.5 concentrations during the activity may produce exceptionally high values and thus not reflect a 24-h period rendering them incomparable against the WHO AQG 24-h level. As described earlier, the majority of studies were rated as having medium or high risk of bias due to exposure measurement methods failing to sample for more than 72 h. However, even with longer sampling periods, many behavioural variabilities may not be captured, making it difficult to estimate an annual average exposure, another WHO AQG metric. These factors highlight that without a standardised approach to the measurement and reporting of household PM2.5 concentrations, any meaningful comparison of data between studies is not only difficult but may also lack any validity. This closely echoes the conclusions and findings of another systematic review by Younger et al. (2022).
There would also appear to be a great degree of variability in the measured PM2.5 concentrations from the same source across and within studies, although, as just discussed, it is perhaps difficult to distinguish true variation in a source of exposure from the variation and uncertainty of the measurement device and method. Another consideration that may greatly impact measured values is contextual outdoor PM2.5 concentration. This significantly differs both temporally and spatially and will influence indoor PM2.5 concentration during the sampling, depending on house location and time of day and season (Cyrys et al. 2004; Chen and Zhao 2011). Among the studies herein collated, 31 of the 49 made reference to and had extractable outdoor PM2.5 measurements from either central monitoring sites or directly outside of participating homes. It is clear that outdoor concentrations are a consideration among researchers in the field. However, the overwhelming majority fail to report metrics such as building characteristics, ventilation and air exchange rate, among other structural and meteorological factors that would be required to comment on the effect that outdoor PM2.5 infiltration has on indoor measurements.
Further research is clearly required to build a more comprehensive picture of the exposure to indoor PM2.5 in homes within HICs. The contribution to this understanding, however, must be conducted and presented in a way that allows for ease of direct comparison between individual studies, such that meaningful conclusions may be drawn. Thus, there is an obvious need for standardised methods in both the measurement and reporting of indoor PM2.5 concentrations in this field of research. Such standardisation would perhaps be analogous to that called for in occupational exposure to hazardous substances (National Institute for Occupational Safety and Health 2002; Kromhout 2002). Parameters such as sources of exposure, times, locations and households would all need to be considered in such a standardised framework. Researchers should ensure that sampling devices, whether they be based on optical and gravimetric technologies, produce accurate, reliable and comparable values. This may be achieved by calibrating optical instruments by co-locating with reference gravimetric samplers. Values from optical instruments can then be reported after adjustment with these gravimetrically-derived calibrations (Wang et al. 2016; Vogt et al. 2021). Defining and standardising a minimum sampling duration that is representative of a household’s activity is another consideration that would greatly improve the validity of intra- and inter-study comparison. This data should then be reported in a standardised time weighted average and perhaps be consistent with that of the WHO AQG, which currently uses 24-h and annual average intervals for PM2.5 exposure. To allow for the comprehensive interpretation of data, as advocated in the field of occupational exposure, the collection and reporting of certain contextual information should be mandated. Examples of such information should include corresponding outdoor PM2.5 concentrations, building characteristics and ventilation conditions as a minimum.
An extrapolation that is pertinent to this review is the potential benefit of a low-cost PM2.5 monitor that provides instantaneous feedback. As already discussed, people in HICs spend a significant amount of time at home, and thus household sources that generate high levels of PM2.5 pose potential health risks to occupants that are unknowingly exposed for extended periods of time. Having easy and reliable access to real-time PM2.5 values may prompt residents to alter behaviours and limit their own exposures. This may include opening windows when cooking or minimising the use of candles. Such devices would provide the most benefit to individuals with existing respiratory conditions as a means of preventing the exacerbation of their illnesses which in turn may maintain or improve health, and reduce avoidable burden on the healthcare system.
Strengths and weaknesses
There are several limitations to this systematic review. Firstly, the use of a single database for literature search may result in a very small number of studies being neglected from inclusion. PubMed, however, is likely to be the most comprehensive database for literature on indoor air quality in homes; thus, the omission should be minimum. Returned studies were single-screened based on their titles and abstracts by one researcher in the selection stage. Although 10% of these were independently assessed by a second researcher, it is still possible that relevant, but less explicitly so, studies were overlooked and not included. Their inclusion would not have been possible without screening the full-texts, an impracticable task for any systematic review of this kind. As only articles published in English were included, this systematic review would also have neglected a very small number of studies concerning indoor PM2.5 concentrations that have only been published in other languages. In addition to the limitation associated with the exclusion of potentially relevant studies, there are limitations associated with the extracted data itself. Due to the highly varied sample sizes and recruitment methods used across the included studies, the studies’ samples may not be representative of the target population, introducing bias and lowering the generalisability of the conclusions drawn from the review. The quality appraisal tool implemented in this systematic review to assess the risk of bias for the exposure assessment methods rather than the actual study designs themselves. It is therefore possible that this review includes studies with low external validity. The last noteworthy limitation pertains to the current lack of standardised methods for the measurement of PM2.5, with different studies using a variety of measurement devices and sampling durations, as discussed earlier. The potential observational errors in the included studies themselves can again negatively impact on the conclusions drawn.
Conclusion
This systematic review collates existing studies concerning indoor PM2.5 concentrations associated with common household sources in HICs and reveals that these can, at times, generate PM2.5 concentrations inside homes that exceed the WHO AQG. The small number of studies identified in this review highlights the need for more research into concentrations of PM2.5 in homes within HICs. This review also provides insight into the current indoor PM2.5 measuring and reporting techniques which were found to vary greatly between studies. This high degree of variability in exposure assessments and the presentations of results suggests that more uniform and standardised methodologies are needed in future research. Most importantly, this systematic review highlights the need to promote public education around PM2.5 pollution in home settings and guide people to make more informed choices in lifestyles or behaviour. This should consequently reduce the health risks associated with exposure to high concentrations of PM2.5, and ultimately protect the health of people in HICs.
Data availability
Not applicable.
Notes
This systematic review only included data from non-smoking homes; however, individual studies may have also reported data for smoking households.
References
Abt E, Suh HH, Allen G, Koutrakis P (2000) Characterization of indoor particle sources: a study conducted in the metropolitan Boston area. Environ Health Perspect 108:35–44. https://doi.org/10.1289/ehp.0010835
Adgate JL, Ramachandran G, Pratt GC et al (2003) Longitudinal variability in outdoor, indoor, and personal PM2.5 exposure in healthy non-smoking adults. Atmos Environ 37:993–1002. https://doi.org/10.1016/S1352-2310(02)00978-0
Air Quality in Scotland (2022) Latest pollution map. https://www.scottishairquality.scot/latest. Accessed 26 Feb 2022
Allen R, Wallace L, Larson T et al (2004) Estimated hourly personal exposures to ambient and nonambient particulate matter among sensitive populations in Seattle, Washington. J Air Waste Manage Assoc 54:1197–1211. https://doi.org/10.1080/10473289.2004.10470988
Allen RW, Mar T, Koenig J et al (2008) Changes in lung function and airway inflammation among asthmatic children residing in a woodsmoke-impacted urban area. Inhalation Toxicol 20:423–433. https://doi.org/10.1080/08958370801903826
Allen RW, Leckie S, Millar G, Brauer M (2009) The impact of wood stove technology upgrades on indoor residential air quality. Atmos Environ 43:5908–5915. https://doi.org/10.1016/j.atmosenv.2009.08.016
Alves C, Vicente A, Oliveira AR et al (2020) Fine particulate matter and gaseous compounds in kitchens and outdoor air of different dwellings. Int J Environ Res Public Health 17:5256. https://doi.org/10.3390/ijerph17145256
Arden Pope C, Burnett RT, Turner MC et al (2011) Lung cancer and cardiovascular disease mortality associated with ambient air pollution and cigarette smoke: shape of the exposure-response relationships. Environ Health Perspect 119:1616–1621. https://doi.org/10.1289/ehp.1103639
Arden Pope C, Coleman N, Pond ZA, Burnett RT (2020) Fine particulate air pollution and human mortality: 25+ years of cohort studies. Environ Res 183. https://doi.org/10.1016/j.envres.2019.108924
Arif M, Parveen S (2021) Carcinogenic effects of indoor black carbon and particulate matters (PM2.5 and PM10) in rural households of India. Environ Sci Pollut Res 28:2082–2096. https://doi.org/10.1007/s11356-020-10668-5
Assimakopoulos VD, Bekiari T, Pateraki S et al (2018) Assessing personal exposure to PM using data from an integrated indoor-outdoor experiment in Athens-Greece. Sci Total Environ 636:1303–1320. https://doi.org/10.1016/j.scitotenv.2018.04.249
Baxter LK, Clougherty JE, Laden F, Levy JI (2007) Predictors of concentrations of nitrogen dioxide, fine particulate matter, and particle constituents inside of lower socioeconomic status urban homes. J Epos Sci Environ Epidemiol 17:433–444. https://doi.org/10.1038/sj.jes.7500532
Bonjour S, Adair-Rohani H, Wolf J et al (2013) Solid fuel use for household cooking: country and regional estimates for 1980–2010. Environ Health Perspect 121:784–790. https://doi.org/10.1289/ehp.1205987
Bowe B, Xie Y, Yan Y, Al-Aly Z (2019) Burden of cause-specific mortality associated with PM 2.5 air pollution in the United States. JAMA Network Open 2:e1915834. https://doi.org/10.1001/jamanetworkopen.2019.15834
Braithwaite I, Zhang S, Kirkbride JB et al (2019) Air pollution (particulate matter) exposure and associations with depression, anxiety, bipolar, psychosis and suicide risk: a systematic review and meta-analysis. Environ Health Perspect 127:126002. https://doi.org/10.1289/EHP4595
Brown KW, Sarnat JA, Suh HH et al (2009) Factors influencing relationships between personal and ambient concentrations of gaseous and particulate pollutants. Sci Total Environ 407:3754–3765. https://doi.org/10.1016/j.scitotenv.2009.02.016
Brugge D, Vallarino J, Ascolillo L et al (2003) Comparison of multiple environmental factors for asthmatic children in public housing. Indoor Air 13:18–27. https://doi.org/10.1034/j.1600-0668.2003.01130.x
Budya H, Yasir Arofat M (2011) Providing cleaner energy access in Indonesia through the megaproject of kerosene conversion to LPG. Energy Policy 39:7575–7586. https://doi.org/10.1016/j.enpol.2011.02.061
Carey IM, Anderson HR, Atkinson RW et al (2018) Are noise and air pollution related to the incidence of dementia? A cohort study in London. England BMJ Open 8:e022404. https://doi.org/10.1136/bmjopen-2018-022404
Carrion-Matta A, Kang C-M, Gaffin JM et al (2019) Classroom indoor PM2.5 sources and exposures in inner-city schools. Environ Int 131:104968. https://doi.org/10.1016/j.envint.2019.104968
Centers for Disease Control and Prevention (2021) Air pollutants. https://www.cdc.gov/air/pollutants.htm. Accessed 25 Feb 2022
Centre for Reviews and Dissemination (2009) Systematic reviews: CRD’s guidance for undertaking reviews in health care. CRD, University of York, York
Chakraborty R, Heydon J, Mayfield M, Mihaylova L (2020) Indoor air pollution from residential stoves: examining the flooding of particulate matter into homes during real-world use. Atmosphere (Basel) 11:1326. https://doi.org/10.3390/atmos11121326
Chen C, Zhao B (2011) Review of relationship between indoor and outdoor particles: I/O ratio, infiltration factor and penetration factor. Atmos Environ 45:275–288. https://doi.org/10.1016/j.atmosenv.2010.09.048
Cyrys J, Pitz M, Bischof W et al (2004) Relationship between indoor and outdoor levels of fine particle mass, particle number concentrations and black smoke under different ventilation conditions. J Eposure Sci Environ Epidemiol 14:275–283. https://doi.org/10.1038/sj.jea.7500317
Delgado-Saborit JM, Aquilina NJ, Meddings C et al (2011) Relationship of personal exposure to volatile organic compounds to home, work and fixed site outdoor concentrations. Sci Total Environ 409:478–488. https://doi.org/10.1016/j.scitotenv.2010.10.014
Department for Environment Food & Rural Affairs (2022) Interactive monitoring network map. https://uk-air.defra.gov.uk/interactive-map. Accessed 26 Feb 2022
Du Y, Xu X, Chu M et al (2016) Air particulate matter and cardiovascular disease: the epidemiological, biomedical and clinical evidence. J Thorac Dis 8:E8–E19. https://doi.org/10.3978/j.issn.2072-1439.2015.11.37
El-Sharkawy MF, Javed W (2018) Study of indoor air quality level in various restaurants in Saudi Arabia. Environ Prog Sustain Energy 37:1713–1721. https://doi.org/10.1002/ep.12859
Fleisch AF, Rokoff LB, Garshick E et al (2020) Residential wood stove use and indoor exposure to PM2.5 and its components in Northern New England. J Eposure Sci Environ Epidemiol 30:350–361. https://doi.org/10.1038/s41370-019-0151-4
Frasca D, Marcoccia M, Tofful L et al (2018) Influence of advanced wood-fired appliances for residential heating on indoor air quality. Chemosphere 211:62–71. https://doi.org/10.1016/j.chemosphere.2018.07.102
Ghazi L, Drawz PE, Berman JD (2021) The association between fine particulate matter (PM2.5) and chronic kidney disease using electronic health record data in urban Minnesota. J Exposure Sci Environ Epidemiol. https://doi.org/10.1038/s41370-021-00351-3
Habre R, Coull B, Moshier E et al (2014) Sources of indoor air pollution in New York City residences of asthmatic children. J Eposure Sci Environ Epidemiol 24:269–278. https://doi.org/10.1038/jes.2013.74
Hadeed SJ, O’Rourke MK, Canales RA et al (2021) Household and behavioral determinants of indoor PM 2.5 in a rural solid fuel burning Native American community. Indoor Air 31:2008–2019. https://doi.org/10.1111/ina.12904
Hanna R, Duflo E, Greenstone M (2012) Up in smoke: the influence of household behavior on the long-run impact of improved cooking stoves. Cambridge
Hart JF, Ward TJ, Spear TM et al (2011) Evaluating the effectiveness of a commercial portable air purifier in homes with wood burning stoves: a preliminary study. J Environ Public Health 2011:1–7. https://doi.org/10.1155/2011/324809
Hayes RB, Lim C, Zhang Y et al (2020) PM2.5 air pollution and cause-specific cardiovascular disease mortality. Int J Epidemiol 49:25–35. https://doi.org/10.1093/ije/dyz114
Jedrychowski WA, Perera FP, Pac A et al (2006) Variability of total exposure to PM2.5 related to indoor and outdoor pollution sources. Sci Total Environ 366:47–54. https://doi.org/10.1016/j.scitotenv.2005.08.001
Jeong C-H, Salehi S, Wu J et al (2019) Indoor measurements of air pollutants in residential houses in urban and suburban areas: indoor versus ambient concentrations. Sci Total Environ 693:133446. https://doi.org/10.1016/j.scitotenv.2019.07.252
Jones ER, Cedeño Laurent JG, Young AS et al (2021) The effects of ventilation and filtration on indoor PM2.5 in office buildings in four countries. Build Environ 200:107975. https://doi.org/10.1016/j.buildenv.2021.107975
Karottki DG, Bekö G, Clausen G et al (2014) Cardiovascular and lung function in relation to outdoor and indoor exposure to fine and ultrafine particulate matter in middle-aged subjects. Environ Int 73:372–381. https://doi.org/10.1016/j.envint.2014.08.019
Kelly FJ, Fussell JC (2015) Air pollution and public health: emerging hazards and improved understanding of risk. Environ Geochem Health 37:631–649. https://doi.org/10.1007/s10653-015-9720-1
Klepeis NE, Nelson WC, Ott WR et al (2001) The National Human Activity Pattern Survey (NHAPS): a resource for assessing exposure to environmental pollutants. J Eposure Sci Environ Epidemiol 11:231–252. https://doi.org/10.1038/sj.jea.7500165
Kromhout H (2002) Design of measurement strategies for workplace exposures. Occup Environ Med 59:349–354. https://doi.org/10.1136/oem.59.5.349
Lam J, Sutton P, Kalkbrenner A et al (2016) A systematic review and meta-analysis of multiple airborne pollutants and autism spectrum disorder. PLoS ONE 11:e0161851. https://doi.org/10.1371/journal.pone.0161851
Lanki T, Alm S, Ruuskanen J et al (2002) Photometrically measured continuous personal PM2.5 exposure: levels and correlation to a gravimetric method. J Eposure Sci Environ Epidemiol 12:172–178. https://doi.org/10.1038/sj.jea.7500218
Li X, Huang S, Jiao A et al (2017) Association between ambient fine particulate matter and preterm birth or term low birth weight: an updated systematic review and meta-analysis. Environ Pollut 227:596–605. https://doi.org/10.1016/j.envpol.2017.03.055
Lim M, Myagmarchuluun S, Ban H et al (2018) Characteristics of indoor PM2.5 concentration in Gers using coal stoves in Ulaanbaatar, Mongolia. Int J Environ Res Public Health 15:2524. https://doi.org/10.3390/ijerph15112524
Lim S, Bassey E, Bos B et al (2022) Comparing human exposure to fine particulate matter in low and high-income countries: a systematic review of studies measuring personal PM2.5 exposure. Sci Total Environ 833:155207. https://doi.org/10.1016/j.scitotenv.2022.155207
MacNeill M, Kearney J, Wallace L et al (2014) Quantifying the contribution of ambient and indoor-generated fine particles to indoor air in residential environments. Indoor Air 24:362–375. https://doi.org/10.1111/ina.12084
Madureira J, Slezakova K, Costa C et al (2020) Assessment of indoor air exposure among newborns and their mothers: levels and sources of PM10, PM2.5 and ultrafine particles at 65 home environments. Environ Pollut 264:114746. https://doi.org/10.1016/j.envpol.2020.114746
Marques G, Pitarma R (2020) Particulate matter monitoring and assessment through Internet of Things: a health information system for enhanced living environments. J Med Syst 44:207. https://doi.org/10.1007/s10916-020-01674-8
Mazaheri M, Clifford S, Yeganeh B et al (2018) Investigations into factors affecting personal exposure to particles in urban microenvironments using low-cost sensors. Environ Int 120:496–504. https://doi.org/10.1016/j.envint.2018.08.033
McNamara M, Thornburg J, Semmens E et al (2013) Coarse particulate matter and airborne endotoxin within wood stove homes. Indoor Air 23:498–505. https://doi.org/10.1111/ina.12043
Mendell AY, Mahdavi A, Siegel JA (2022) Particulate matter concentrations in social housing. Sustain Cities Soc 76:103503. https://doi.org/10.1016/j.scs.2021.103503
Molnar P, Gustafson P, Johannesson S et al (2005) Domestic wood burning and PM trace elements: Personal exposures, indoor and outdoor levels. Atmos Environ 39:2643–2653. https://doi.org/10.1016/j.atmosenv.2005.01.016
Monn Ch, Fuchs A, Högger D et al (1997) Particulate matter less than 10 μm (PM10) and fine particles less than 2.5 μm (PM2.5): relationships between indoor, outdoor and personal concentrations. Sci Total Environ 208:15–21. https://doi.org/10.1016/S0048-9697(97)00271-4
Mortimer K, Ndamala CB, Naunje AW et al (2017) A cleaner burning biomass-fuelled cookstove intervention to prevent pneumonia in children under 5 years old in rural Malawi (the Cooking and Pneumonia Study): a cluster randomised controlled trial. Lancet 389:167–175. https://doi.org/10.1016/S0140-6736(16)32507-7
Nasir ZA, Colbeck I (2013) Particulate pollution in different housing types in a UK suburban location. Sci Total Environ 445–446:165–176. https://doi.org/10.1016/j.scitotenv.2012.12.042
National Institute for Occupational Safety and Health (2002) Exposure assessment methods: research needs and priorities
National Institutes of Health (2021) Study quality assessment tools. https://www.nhlbi.nih.gov/health-topics/study-quality-assessment-tools. Accessed 1 Mar 2022
Noonan CW, Navidi W, Sheppard L et al (2012) Residential indoor PM 2.5 in wood stove homes: follow-up of the Libby changeout program. Indoor Air 22:492–500. https://doi.org/10.1111/j.1600-0668.2012.00789.x
O’Donnell R, Eadie D, Stead M et al (2021) ‘I was smoking a lot more during lockdown because I can’: a qualitative study of how UK smokers responded to the Covid-19 lockdown. Int J Environ Res Public Health 18:5816. https://doi.org/10.3390/ijerph18115816
Ohura T, Noda T, Amagai T, Fusaya M (2005) Prediction of personal exposure to PM 2.5 and carcinogenic polycyclic aromatic hydrocarbons by their concentrations in residential microenvironments. Environ Sci Technol 39:5592–5599. https://doi.org/10.1021/es050571x
O’Leary C, Jones B, Hall I (2018) An intervention study of PM2.5 concentrations measured in domestic kitchens. In: 39th Air Infiltration and Ventilation Centre Conference: Smart Ventilation for Buildings
Olson DA, Burke JM (2006) Distributions of PM 2.5 source strengths for cooking from the research triangle park particulate matter panel study. Environ Sci Technol 40:163–169. https://doi.org/10.1021/es050359t
Omelekhina Y, Nordquist B, Alce G et al (2022) Effect of energy renovation and occupants’ activities on airborne particle concentrations in Swedish rental apartments. Sci Total Environ 806:149995. https://doi.org/10.1016/j.scitotenv.2021.149995
Page MJ, McKenzie JE, Bossuyt PM, et al (2021) The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ n71. https://doi.org/10.1136/bmj.n71
Paulin LM, Williams D, Oberweiser C et al (2013) Indoor air quality in central Appalachia homes impacted by wood and coal use. J Environ Prot 04:67–71. https://doi.org/10.4236/jep.2013.41007
Pietrogrande MC, Casari L, Demaria G, Russo M (2021) Indoor air quality in domestic environments during periods close to Italian COVID-19 lockdown. Int J Environ Res Public Health 18:4060. https://doi.org/10.3390/ijerph18084060
Pope D, Bruce N, Dherani M et al (2017) Real-life effectiveness of ‘improved’ stoves and clean fuels in reducing PM 2.5 and CO: Systematic review and meta-analysis. Environ Int 101:7–18. https://doi.org/10.1016/j.envint.2017.01.012
PurpleAir (2022) Cleaner air begins with you. https://www2.purpleair.com/. Accessed 26 Feb 2022
Quansah R, Semple S, Ochieng CA et al (2017) Effectiveness of interventions to reduce household air pollution and/or improve health in homes using solid fuel in low-and-middle income countries: a systematic review and meta-analysis. Environ Int 103:73–90. https://doi.org/10.1016/j.envint.2017.03.010
Rojas-Bracho L, Suh HH, Oyola P, Koutrakis P (2002) Measurements of children’s exposures to particles and nitrogen dioxide in Santiago, Chile. Sci Total Environ 287:249–264. https://doi.org/10.1016/S0048-9697(01)00987-1
Rojas-Bracho L, Suh HH, Catalano PJ, Koutrakis P (2004) Personal exposures to particles and their relationships with personal activities for chronic obstructive pulmonary disease patients living in Boston. J Air Waste Manage Assoc 54:207–217. https://doi.org/10.1080/10473289.2004.10470897
Salthammer T, Schripp T, Wientzek S, Wensing M (2014) Impact of operating wood-burning fireplace ovens on indoor air quality. Chemosphere 103:205–211. https://doi.org/10.1016/j.chemosphere.2013.11.067
Sarigiannis DΑ, Karakitsios SP, Kermenidou M et al (2014) Total exposure to airborne particulate matter in cities: the effect of biomass combustion. Sci Total Environ 493:795–805. https://doi.org/10.1016/j.scitotenv.2014.06.055
Schluger N (2014) Household air quality in high-income countries: forgotten but not gone. Lancet Respir Med 2:781–783. https://doi.org/10.1016/S2213-2600(14)70183-3
Schraufnagel DE, Balmes JR, Cowl CT et al (2019) Air pollution and noncommunicable diseases. Chest 155:417–426. https://doi.org/10.1016/j.chest.2018.10.041
Semmens EO, Noonan CW, Allen RW et al (2015) Indoor particulate matter in rural, wood stove heated homes. Environ Res 138:93–100. https://doi.org/10.1016/j.envres.2015.02.005
Semple S, Garden C, Coggins M et al (2012) Contribution of solid fuel, gas combustion, or tobacco smoke to indoor air pollutant concentrations in Irish and Scottish homes. Indoor Air 22:212–223. https://doi.org/10.1111/j.1600-0668.2011.00755.x
Semple S, Apsley A, Azmina Ibrahim T et al (2015) Fine particulate matter concentrations in smoking households: just how much secondhand smoke do you breathe in if you live with a smoker who smokes indoors? Tob Control 24:e205–e211. https://doi.org/10.1136/tobaccocontrol-2014-051635
Semple S, Sweeting H, Demou E et al (2017) Characterising the exposure of prison staff to second-hand tobacco smoke. Ann Work Expos Health 61:809–821. https://doi.org/10.1093/annweh/wxx058
Shehab M, Pope FD, Delgado-Saborit JM (2021) The contribution of cooking appliances and residential traffic proximity to aerosol personal exposure. J Environ Health Sci Eng 19:307–318. https://doi.org/10.1007/s40201-020-00604-7
Shi L, Wu X, Danesh Yazdi M et al (2020) Long-term effects of PM2·5 on neurological disorders in the American Medicare population: a longitudinal cohort study. Lancet Planet Health 4:e557–e565. https://doi.org/10.1016/S2542-5196(20)30227-8
Siponen T, Yli-Tuomi T, Tiittanen P et al (2019) Wood stove use and other determinants of personal and indoor exposures to particulate air pollution and ozone among elderly persons in a Northern Suburb. Indoor Air 29:413–422. https://doi.org/10.1111/ina.12538
Stranger M, Potgietervermaak S, Vangrieken R (2009) Particulate matter and gaseous pollutants in residences in Antwerp, Belgium. Sci Total Environ 407:1182–1192. https://doi.org/10.1016/j.scitotenv.2008.10.019
The World Bank (2021) High income. https://data.worldbank.org/country/XD. Accessed 1 Dec 2021
Vogt M, Schneider P, Castell N, Hamer P (2021) Assessment of low-cost particulate matter sensor systems against optical and gravimetric methods in a field co-location in Norway. Atmosphere (Basel) 12:961. https://doi.org/10.3390/atmos12080961
Wallace LA, Mitchell H, O’Connor GT et al (2003) Particle concentrations in inner-city homes of children with asthma: the effect of smoking, cooking, and outdoor pollution. Environ Health Perspect 111:1265–1272. https://doi.org/10.1289/ehp.6135
Wallace LA, Wheeler AJ, Kearney J et al (2011) Validation of continuous particle monitors for personal, indoor, and outdoor exposures. J Eposure Sci Environ Epidemiol 21:49–64. https://doi.org/10.1038/jes.2010.15
Wang Z, Calderón L, Patton AP et al (2016) Comparison of real-time instruments and gravimetric method when measuring particulate matter in a residential building. J Air Waste Manage Assoc 66:1109–1120. https://doi.org/10.1080/10962247.2016.1201022
Ward T, Boulafentis J, Simpson J et al (2011) Lessons learned from a woodstove changeout on the Nez Perce Reservation. Sci Total Environ 409:664–670. https://doi.org/10.1016/j.scitotenv.2010.11.006
Wheeler AJ, Gibson MD, MacNeill M et al (2014) Impacts of air cleaners on indoor air quality in residences impacted by wood smoke. Environ Sci Technol 48:12157–12163. https://doi.org/10.1021/es503144h
Wigzell E, Kendall M, Nieuwenhuijsen MJ (2000) The spatial and temporal variation of particulate matter within the home. J Eposure Sci Environ Epidemiol 10:307–314. https://doi.org/10.1038/sj.jea.7500091
World Health Organization (2021a) Ambient (outdoor) air pollution. https://www.who.int/news-room/fact-sheets/detail/ambient-(outdoor)-air-quality-and-health. Accessed 25 Feb 2022
World Health Organization (2021b) WHO global air quality guidelines: particulate matter (PM2.5 and PM10), ozone, nitrogen dioxide, sulfur dioxide and carbon monoxide. https://apps.who.int/iris/handle/10665/345329. Accessed 25 Feb 2022
Wyss AB, Jones AC, Bølling AK, et al (2016) Particulate matter 2.5 exposure and self-reported use of wood stoves and other indoor combustion sources in urban nonsmoking homes in Norway. PLOS ONE 11:e0166440. https://doi.org/10.1371/journal.pone.0166440
Xing YF, Xu YH, Shi MH, Lian YX (2016) The impact of PM2.5 on the human respiratory system. J Thorac Dis 8:E69–E74. https://doi.org/10.3978/j.issn.2072-1439.2016.01.19
Yassin MF, AlThaqeb BEY, Al-Mutiri EAE (2012) Assessment of indoor PM2.5 in different residential environments. Atmos Environ 56:65–68. https://doi.org/10.1016/j.atmosenv.2012.03.051
Young BN, Clark ML, Rajkumar S et al (2019) Exposure to household air pollution from biomass cookstoves and blood pressure among women in rural Honduras: A cross-sectional study. Indoor Air 29:130–142. https://doi.org/10.1111/ina.12507
Younger A, Alkon A, Harknett K et al (2022) Adverse birth outcomes associated with household air pollution from unclean cooking fuels in low- and middle-income countries: a systematic review. Environ Res 204:112274. https://doi.org/10.1016/j.envres.2021.112274
Zhang T, Chillrud SN, Yang Q et al (2020) Characterizing peak exposure of secondhand smoke using a real-time PM 2.5 monitor. Indoor Air 30:98–107. https://doi.org/10.1111/ina.12611
Zhao H, Chan WR, Delp WW et al (2020) Factors impacting range hood use in California houses and low-income apartments. Int J Environ Res Public Health 17:8870. https://doi.org/10.3390/ijerph17238870
Funding
S. Semple declares that no funds, grants, or other support were received during the preparation of this manuscript. S. Wei was awarded £1000 from Nottingham Hospitals Charity for her Master of Public Health dissertation module at the University of Stirling.
Author information
Authors and Affiliations
Contributions
Both authors contributed to the study conception and design. Material preparation, data collection and analysis were performed by SW and SS. The first draft of the manuscript was written by SW, and SS commented on previous versions of the manuscript. Both authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval
The ethical approach of this review was approved by the University of Stirling Research Ethics Committee.
Consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Wei, S., Semple, S. Exposure to fine particulate matter (PM2.5) from non-tobacco sources in homes within high-income countries: a systematic review. Air Qual Atmos Health 16, 553–566 (2023). https://doi.org/10.1007/s11869-022-01288-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11869-022-01288-8