
Abstract
Currently, preventing and controlling air pollution and inhibiting the excessively rapid growth of medical expenditures to reduce the living burden of residents have become a focus of general concern of society as a whole. It is of great significance to conduct an in-depth study of the relationship between air pollution and public health expenditure and clarify to what extent air pollution affects health expenditure. Thus, this paper adopted spatial econometric methods to measure the impact of air pollution on residents’ health expenditure via panel data from 16 core cities in the Yangtze River Delta in China from 2005 to 2017. The results indicate that (1) at present, the air pollution in the Yangtze River Delta core urban agglomeration is still relatively prominent and has obvious spatial aggregation phenomena, and the particulate matter 2.5 (PM2.5) concentration shows the characteristic of decreasing gradually from northwest to southeast; (2) air pollution is the main factor that promotes the increase in residents’ health expenditure; (3) the spatial spillover effect of air pollution is obvious, accounting for half of the total effect; and (4) the impact of government public services on residents’ health expenditure varies. Finally, this paper proposes corresponding policy implications based on the findings.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Improving the quality of the air environment and the health level of the people to alleviate the burden of medical expenses on residents is a proposition put forward by major national strategies in China, such as ecological civilization construction and healthy China. Air pollution has become the greatest adverse environmental factor causing premature human death (Zhou et al. 2019). The main pollutants considered by environmental protection departments in China to evaluate and rank the air quality of cities are sulfur dioxide (SO2), nitrogen dioxide (NO2), inhalable particulate matter (PM10), particulate matter (PM2.5), carbon monoxide (CO), and ozone (O3). Atmospheric particulate matter (PM), especially with a diameter less than 2.5 μm (PM2.5), is considered one of the priority pollutants in the atmosphere. PM2.5 is rich in a large number of toxic and harmful substances and easily enters the blood through the lungs; thus, frequent exposure to PM2.5 can cause damage to human health.
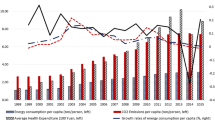
According to the most recent “Global Burden of Disease Report” released by The Lancet magazine in 2019, China and India are the countries with the highest disease burden of air pollution in the world. In recent years, China’s per capita health care expenditure has increased significantly not only in absolute terms but also in proportion to disposable income. According to the National Bureau of Statistics, from 1990 to 2019, China’s urban residents’ per capita health care expenditure increased from 25.67 CNY to 2283 CNY, accounting for 1.85 to 5.39% of per capita disposable income. A large number of studies have shown that air pollution has adverse effects on multiple systems of the human body and directly or indirectly causes damage to residents' health, leading to an increase or aggravation of disease symptoms (Garcia et al. 2015; To et al. 2015), an increase in the number of outpatient and inpatient visits in hospitals (Bloemsma et al. 2016; Cai et al. 2015; Zeng et al. 2019), and an increase in long-term or short-term mortality (Balakrishnan et al. 2019; Carvalho 2019; Chen et al. 2012; Wu et al. 2019). In addition, the health and economic losses from diseases or deaths caused by air pollution are enormous (Du et al. 2016; Fan et al. 2019; Han et al. 2019; Lu et al. 2016; Zhao et al. 2016). Air pollution has increased the risk of disease and stimulated residents’ demand for health services, which has caused an increase in health expenditure and further increased residents’ living burden (Chen et al. 2019; Hadian et al. 2020).
In recent years, medical expenditures caused by air pollution have aroused widespread concern among scholars. Currently, air pollution is creating a non-negligible living burden on humans. Using the China Urban Household Survey (UHS) Database, Yang and Zhang (2018) estimated the effect of air pollution exposure on household healthcare expenditure. Zeng and He (2019) took industrial exhaust emissions as a proxy indicator for regional air pollution and concluded that air pollution increases people’s medical expenditure. Blázquez-Fernández et al. (2019) studied the relationship between air pollution and health expenditure in 29 OECD countries over the period 1995–2014. Raeissi et al. (2018) concluded that environmental quality and contaminants played the most important role among the factors affecting health expenditures, and air pollution had a greater impact on health expenditures in the long term than in the short term.
On the whole, there have been a large number of in-depth studies on the relationship between air pollution and health. While most of the existing studies focus on the assessment of residents’ health risks and economic losses caused by air pollution, there are relatively few studies on the relationship between air pollution and health expenditure. While there are studies on the relationship between air pollution and health expenditure, assuming that the regions are independent of each other, some studies have proven that air pollution has obvious spatial characteristics. Ignoring the existence of spatial autocorrelation can lead to errors in the estimation of the public health effects of air pollution, so the results should be treated with caution (Chen et al. 2017b). Furthermore, most of the previous studies have been carried out from provincial areas or based on individual cities and used the emission level of pollutants, such as industrial exhaust gas, as a proxy index to measure local air pollution, with fewer studies considering PM2.5 concentration as an important pollutant. Moreover, currently, the basic research work is relatively fragmented in view of the regional urban agglomeration haze pollution and health expenditure level, and there is a lack of comprehensive understanding of the governance of haze pollution and health expenditure levels in urban agglomerations.
The Yangtze River Delta urban agglomeration is the most developed urbanization area and one of the areas with serious air pollution in China. PM2.5 is considered one of the priority pollutants in the atmosphere. Therefore, this paper selects the Yangtze River Delta urban agglomeration as the research object, takes the PM2.5 concentration as the proxy index of air pollution, and uses spatial econometrics methods to analyze the impact of regional air pollution and the spillover effect on residents’ health expenditure from the macro level. It not only makes up for the research defects in related fields but also provides a reference for the decision-making of policy interventions in the areas of atmospheric environment management and medical care in this region and even the whole country.
Research design
Model construction
Air pollution flows between regions are not independent of each other, and the flow of air pollution in a certain area may affect the health behavior of residents in other regions (Bao et al. 2015). Therefore, this paper adopted spatial econometric models to explore the relationships between areas. Different types of spatial econometric models assume different spatial transmission mechanisms, and the economic implications they represent differ. Formulations (2) and (3) are the spatial Durbin model (SDM) and spatial autocorrelation (SAC) model, respectively, while (4)–(5) are the spatial autoregressive (SAR) model and spatial error model (SEM) obtained by attaching certain restrictions to the model. The calculation formulas are as follows:
When the spatial interaction investigated by the SDM does not exist, there is only a single spatial correlation between regions; that is, when θi = 0 (i = 1, 2), or when the coefficient of the spatial error term λ = 0 in the spatial SAC model, the corresponding SAR model is adopted:
When the coefficient of the spatial interaction term θi, the spatial lag coefficient δ of the dependent variable, and the coefficients βi between the regression satisfy θi = -δβi in the SDM, or the coefficient of the spatial lag term δ = 0 in the SAC model, the corresponding spatial SEM is adopted:
Among them, HE refers to the health expenditure level of urban residents, PM2.5 is a key indicator to measure air pollution, and Xcontrol is a series of control variables. The specific definitions of all variables are shown in Table 1. There are also several factors that can affect health, such as differences in the individual characteristics and lifestyle habits of residents and differences in dietary habits in different regions. Because these microlevel data are difficult to obtain, it is difficult to control these variables in the model. W is the spatial weight matrix. This paper mainly uses the adjacent spatial weight matrix. u it and εit are disturbance terms with an independent and identical distribution and satisfy u it ~ iid(0,σ2), εit ~ iid(0,σ2). β0, β1, and β2 are the regression coefficients of the corresponding variables (for specific definitions, see Table 1).
Variable selection
The research on the impact of environmental pollution on residents’ health is based on the health production function initiated by Grossman (1972), who notes that age, gender, race, education, personal income, marital status, medical services, personal behaviors (such as drinking, smoking, inactivity), and environmental pollution can all have a large and lasting impact on a health level. Since then, scholars have conducted detailed studies on the relationship between residents’ health and influencing indicators, which can mainly be divided into environmental factors, economic factors, social factors, medical service factors, and educational factors (Chen et al. 2017a; Deng et al. 2020; Xu et al. 2019). On this basis, this paper takes urban residents’ health care expenditure as the explained variable and the PM2.5 concentration as the core explanatory variable (environmental factor). This paper selects commonly adopted variables reflecting economic, social, medical service, and educational factors as the control variables to analyze the influence of air pollution on urban residents’ health expenditure. The definitions and descriptive statistics of all variables are listed in Table 1.
Data sources
This study focused on the impact of regional air pollution and spillover effects on residents’ health expenditure. This paper selects 16 core cities in the Yangtze River Delta urban agglomeration of China from 2005 to 2017 as the study area (see in Fig. 1 for more details). PM2.5 concentration data are derived from the results of the Atmospheric Composition Analysis Group of Dalhousie University in Canada and satellite-derived PM2.5 concentration datasets (Van Donkelaar et al. 2019) (for more details, see in the Electronic Supplementary Material (Supplementary Table 1)). Other data are taken from the statistical yearbooks of various cities (2005–2017), “Jiangsu Statistical Yearbook” (2005–2017), “Zhejiang Statistical Yearbook” (2005–2017), and “China Environmental Statistics Yearbook” (2005–2017). Restricted by the availability of data, the data of Taizhou’s medical expenditure in 2007 and 2010 were obtained by interpolation. Indicator data that cannot be obtained directly are obtained by converting the relevant original data. All time-valued data are adjusted for the base period of 2005 to eliminate the impact of price changes. The variables were processed by logarithm to control the influence of heteroscedasticity.

Distribution of the cities in the study area
Spatial-temporal distribution and spatial correlation test
Spatial-temporal distribution characteristics of air pollution
From the perspective of the time dimension, the number of high-concentration polluted cities in the Yangtze River Delta shows an increasing trend. As shown in Fig. 2, the number of cities with PM2.5 concentrations above 55 μg/m3 in the Yangtze River Delta shows an increasing trend, with 5, 9, 9, and 10 cities in 2005, 2009, 2013, and 2017, respectively, indicating that the current air pollution situation in the Yangtze River Delta region is still severe and that air pollution control is a protracted battle. From the perspective of spatial distribution, the air pollution in the Yangtze River Delta region has the phenomenon of spatial aggregation, showing the characteristics of decreasing gradually from northwest to southeast. Overall, among the 16 core cities in the Yangtze River Delta, air pollution in the northwest direction is the most serious, mainly concentrated in 8 cities in Jiangsu Province, followed by Shanghai, and the least polluted cities are in the southeast direction, mainly concentrated in 7 cities in Jiangsu Province (see Fig. 2).

Spatial-temporal distribution of PM2.5 concentration
Spatial correlation test of air pollution
As seen from Fig. 2, air pollution in the Yangtze River Delta has an obvious spatial agglomeration phenomenon, which is consistent with Li et al. (2018). Spatial dependence is generally identified by Moran’s I index. According to the calculation method of Moran’s I index, Fig. 3 shows the global Moran’s I index and the test results of the 16 core urban agglomerations in the Yangtze River Delta from 2005 to 2017. It can be seen that Moran’s I index of PM2.5 concentration in all years is positive, and the significance levels all pass the 1% significance test. In recent years, the Moran’s I index has shown a rising trend fluctuating between 0.491 and 0.643, which indicates that the air pollution in the urban agglomerations of the Yangtze River Delta shows a strong spatial agglomeration that continues to increase.

Spatial correlation identification of air pollution
Results analysis and discussion
Estimation without considering spatial factors
First, this paper did not consider the spatial effect and carried out regression analysis with OLS and ordinary panel (fixed effect and random effect) methods. Then, the F test, LR test, and Hausman test were carried out, and the results showed that the fixed effect was suitable for this data set (see in the Electronic Supplementary Material-Supplementary Table 2). The estimation results of the OLS, FE, and RE models all show that the core explanatory variable PM2.5 concentration of air pollution has a significant positive impact on residents’ health expenditures, which increases the burden on residents. For the core explanatory variable, the coefficients of PM2.5 concentration range from 0.19 to 0.29 and are relatively stable. Judging from the estimated results of the control variables, the other controlled pollution variables (g and d) have no significant impact on the increase in residents’ health expenditure. In addition, the coefficient of PM2.5 pollutant is larger than the coefficients of other pollutants, so in the following analysis, the control variables of other pollutants are eliminated.
Estimation considering spatial factors
Spatial model selection
In terms of model selection, this study follows the judgement rules proposed by LeSage and Pace (2009) and Elhorst (2010). Researchers should start with the SDM as a general specification and test alternatives. Then, Wald and LR tests were conducted to determine the adaptation of the SAC and SEM. The test results showed that the Wald and LR test results rejected the assumptions of θ = 0 and θ = −βρ; clearly, the SAR model and SEM are not applicable for our dataset. Next, we sought to choose between SAC and SDM. Since the SAC model and SDM are non-nested, information standards can be used to judge their suitability. According to the test results, the AIC and BIC values decrease after adding the error lag item. Finally, all research test results show that the SAC model is more suitable for this study. Furthermore, by the Hausman test, the fixed effect model was selected for the spatial panel model. This can be seen from the results in the Electronic Supplementary Material (Supplementary Table 3).
Results analysis and discussion
The core explanatory variable is air pollution
The elasticity of the influence of air pollution on the growth of health expenditure is 0.123, and it has a significant positive effect on the health care expenditure of urban residents at a level of 10%, which is consistent with the findings of Li et al. (2020). The main reason is that the air pollution in the Yangtze River Delta is still serious: first, the coal-based energy structure in the Yangtze River Delta has not undergone fundamental changes, and soot-type pollution has long existed as the main type of pollution (He et al. 2019). Second, the regional economy continued to grow in scale and was dominated by heavy industry in the early years; from 2005 to 2013, the total output value of heavy industry increased by more than 6%. In addition, secondary industry has long been the traditional advantage and pillar industry of economic development in the Yangtze River Delta. In 2017, the proportion of industry reached 42.9%. Third, car exhaust pollution in the region is becoming increasingly serious, and compound air pollutants, such as haze, photochemical smog, and acid rain, are becoming increasingly prominent (Chen et al. 2020; Zhao et al. 2020). Therefore, the severe ambient air quality in this area is bound to increase residents' health risks, thereby increasing their health expenditure.
The impact of control variables on the health expenditure
-
1.
The economic factor. Disposable income has a nonsignificant positive effect on the health expenditure of residents in the Yangtze River Delta. The increase in income level can improve the ability of residents to resist risks, but its impact on health expenditure may be nonsignificant because the per capita medical and health expenditure level of residents in the Yangtze River Delta region is not consistent with the per capita disposable income level. This has a certain relationship with the local cost of living, residents’ consumption awareness, and the local medical insurance system.
-
2.
Medical service factor. The impact of indicators that reflect the local medical and health level on residents’ health expenditures varies. Specifically, the local medical investment level has shown a restraining effect on the growth of health expenditure of residents in the Yangtze River Delta but failed to pass the 10% significance test; at the significance level of 1%, the number of medical professionals per ten thousand people promotes the growth of residents’ health expenditure, and the elasticity of health expenditure is 0.007; the number of hospital beds per ten thousand people has a nonsignificant positive effect on the health care expenditure of residents in the Yangtze River Delta.
-
3.
The education factor and social factor. The education level and the area of greenery per capita showed an opposite direction of change to urban residents’ health expenditures, and all suppressed the growth of residents’ health expenditures at a significance level of 1%. Specifically, for an increase of one unit of education level and the area of greenery per capita, the corresponding expenditure on residents’ health fell by 0.003 and 0.065 units, respectively. This shows that the provision of public services can significantly reduce residents’ health expenditure. The provision of education can improve people’s health awareness and guide them to take measures to make themselves less exposed in high-risk places, such as wearing masks when going out in highly polluted weather. Urban green spaces provide multiple ecosystem services to city residents (Enssle and Kabisch 2020). Urban infrastructure construction—the improvement in garden greening level—can improve air quality, thereby promoting the improvement of residents’ health and reducing health expenditure.
Effect decomposition
When there is a spatial spillover effect, the influence of various factors on health expenditure can be further decomposed to calculate the direct effect, indirect effect, and feedback effect. Supplementary Table 4 in the Electronic Supplementary Material shows that the direct effects, spillover effects, and total effects of air pollution, the core explanatory variable, all passed the significance test at the 10% level and all positively affected residents’ health expenditure. Observing the spillover effect (0.158) and the total effect (0.303) of air pollution, we find that the impact of air pollution on health expenditure had not only a direct effect but also a significant spatial spillover effect, and the spatial spillover effect accounted for approximately half of the total effect. Compared with the estimated coefficients of OLS and ordinary panels that did not consider spatial factors, the direct impacts of air pollution, the number of medical professionals per ten thousand people, the number of junior high school graduates per ten thousand people, and the area of greenery per capita on health expenditure were smaller, which indicated that the OLS estimation to a certain extent overestimated the direct effect of each influencing factor because it did not consider the spatial influence.
Robustness test
This study took the mean value of the PM2.5 concentration as the core explanatory variable to analyze the spatial impact of PM2.5 exposure on residents’ health expenditure. To avoid the selection bias of the explanatory variable, the maximum value of PM2.5 concentration was selected as the substitution variable of PM2.5 exposure for the robustness test. The results are given in the Electronic Supplementary Material (Supplementary Table 5) and are consistent with the above conclusions, indicating that the results are stable and reliable.
Conclusions and policy implications
Based on the analysis of the empirical results, the findings of this study are as follows:
-
1.
At present, the air pollution in the Yangtze River Delta core urban agglomeration is still relatively prominent and has obvious spatial aggregation, and the PM2.5 concentration shows the characteristic of decreasing gradually from northwest to southeast.
-
2.
For the variables that reflect environmental factors, economic factors, social factors, medical service factors, and education factors, the estimation results indicate that air pollution is the main factor affecting residents’ health expenditure regardless of whether spatial factors are considered.
-
3.
Air pollution has a significant promoting effect on the growth of residents’ health expenditure, and the spillover effect is obvious, accounting for half of the total effect.
-
4.
The impact of public services on public health expenditure varies. The medical care level has a significant positive impact on health expenditure, while education level and urban greening level significantly inhibit the growth of health expenditure, and all three have a certain spatial spillover effect.
Based on the above conclusions and analysis, this paper puts forward the following suggestions:
-
1.
Strengthen regional environmental protection and control, promote the joint prevention and co-management of regional air pollution, and bring into play the effect of collaborative governance.
-
2.
Optimize the composition of public services while increasing their supply.
Since government public services have different impacts on residents’ health expenditures, the government should focus on which public services increase health expenditure and which public services reduce it. Education level and urban greening construction can reduce residents’ health expenditure to a certain extent, while air pollution and medical care level increase health expenditure. Therefore, the government should further increase the investment in education, environmental protection, and governance and consider its positive impact on health expenditure while improving the regional medical care level. In addition, the rate of medical reimbursement can be appropriately increased to reduce the burden on residents.
References
Balakrishnan K et al (2019) The impact of air pollution on deaths, disease burden, and life expectancy across the states of India: the Global Burden of Disease Study 2017. Lancet Planet Health 3:e26–e39. https://doi.org/10.1016/S2542-5196(18)30261-4
Bao J, Yang X, Zhao Z, Wang Z, Yu C, Li X (2015) The spatial-temporal characteristics of air pollution in China from 2001-2014. Int J Environ Res Public Health 12:15875–15887. https://doi.org/10.3390/ijerph121215029
Blázquez-Fernández C, Cantarero-Prieto D, Pascual-Sáez M (2019) On the nexus of air pollution and health expenditures: new empirical evidence. Gac Sanit 33:389–394. https://doi.org/10.1016/j.gaceta.2018.01.006
Bloemsma LD, Hoek G, Smit LAM (2016) Panel studies of air pollution in patients with COPD: Systematic review and meta-analysis. Environ Res 151:458–468. https://doi.org/10.1016/j.envres.2016.08.018
Cai Y, Shao Y, Wang C (2015) The association of air pollution with the patients' visits to the department of respiratory diseases. J Clin Med Res 7:551–555. https://doi.org/10.14740/jocmr2174e
Carvalho H (2019) Air pollution-related deaths in Europe - time for action. J Glob Health 9:020308. https://doi.org/10.7189/jogh.09.020308
Chen R et al (2012) Association of particulate air pollution with daily mortality: the China air pollution and health effects study. Am J Epidemiol 175:1173–1181. https://doi.org/10.1093/aje/kwr425
Chen H, Liu Y, Zhu Z, Li Z (2017a) Does where you live matter to your health? Investigating factors that influence the self-rated health of urban and rural Chinese residents: evidence drawn from Chinese General Social Survey data. Health Qual Life Outcomes 15:78–11. https://doi.org/10.1186/s12955-017-0658-0
Chen X, Shao S, Tian Z, Xie Z, Yin P (2017b) Impacts of air pollution and its spatial spillover effect on public health based on China’s big data sample. J Clean Prod 142:915–925. https://doi.org/10.1016/j.jclepro.2016.02.119
Chen J, Chen K, Wang G, Chen R, Liu X, Wei G (2019) Indirect economic impact incurred by haze pollution: an econometric and input–output joint model. Int J Environ Res Public Health 16:2328. https://doi.org/10.3390/ijerph16132328
Chen H, Zhang L, Zou W, Gao Q, Zhao H (2020) Regional differences of air pollution in China: comparison of clustering analysis and systematic clustering methods of panel data based on gray relational analysis. Air Qual Atmos Health. https://doi.org/10.1007/s11869-020-00880-0
Deng QZ, Yi YY, Yu KM (2020) Influencing factors and countermeasures of the health of residents in the city clusters along the middle reaches of the Yangtze River. Healthc 8:93. https://doi.org/10.3390/healthcare8020093
Du Y, Du Y, Li T, Li T (2016) Assessment of health-based economic costs linked to fine particulate (PM2.5) pollution: a case study of haze during January 2013 in Beijing, China. Air Qual Atmos Health 9:439–445. https://doi.org/10.1007/s11869-015-0387-7
Elhorst JP (2010) Specification and estimation of spatial panel data models. Int Reg Sci Rev 26:244–268
Enssle F, Kabisch N (2020) Urban green spaces for the social interaction, health and well-being of older people— An integrated view of urban ecosystem services and socio-environmental justice. Environ Sci Policy 109:36–44. https://doi.org/10.1016/j.envsci.2020.04.008
Fan F, Lei Y, Li L (2019) Health damage assessment of particulate matter pollution in Jing-Jin-Ji region of China. Environ Sci Pollut Res Int 26:7883–7895. https://doi.org/10.1007/s11356-018-04116-8
Garcia E, Hurley S, Nelson DO, Hertz A, Reynolds P (2015) Hazardous air pollutants and breast cancer risk in California teachers: a cohort study. Environ Health 14:14–14. https://doi.org/10.1186/1476-069X-14-14
Grossman M (1972) On the concept of health capital and the demand for health. J Polit Econ 80:223–255. https://doi.org/10.1086/259880
Hadian M, Raeissi P, Khalilabad TH (2020) The economic burden of mortality and morbidity due to air pollution in Tehran, Iran: a systematic review. Air Qual Atmos Health 13:1001–1011. https://doi.org/10.1007/s11869-020-00861-3
Han F, Lu X, Xiao C, Chang M, Huang K (2019) Estimation of Health Effects and Economic Losses from Ambient Air Pollution in Undeveloped Areas: Evidence from Guangxi, China. Int J Environ Res Public Health 16:2707. https://doi.org/10.3390/ijerph16152707
He L, Zhang L, Liu R (2019) Energy consumption, air quality, and air pollution spatial spillover effects: evidence from the Yangtze River Delta of China. Chin J Popul Resour Environ 17:329–340. https://doi.org/10.1080/10042857.2019.1650245
LeSage J, Pace RK (2009) Bayesian Spatial Econometric Models. In. Chapman and Hall/CRC, pp 145-176.
Li H, Li H, Song Y, Song Y, Zhang M, Zhang M (2018) Study on the gravity center evolution of air pollution in Yangtze River Delta of China. Nat Hazards (Dordr) 90:1447–1459. https://doi.org/10.1007/s11069-017-3110-1
Li H, Lu J, Li B (2020) Does pollution-intensive industrial agglomeration increase residents’ health expenditure? Sustain Cities Soc 56:102092. https://doi.org/10.1016/j.scs.2020.102092
Lu X, Yao T, Fung JCH, Lin C (2016) Estimation of health and economic costs of air pollution over the Pearl River Delta region in China. Sci Total Environ 566-567:134–143. https://doi.org/10.1016/j.scitotenv.2016.05.060
Raeissi P, Harati-Khalilabad T, Rezapour A, Hashemi SY, Mousavi A, Khodabakhshzadeh S (2018) Effects of air pollution on public and private health expenditures in Iran: a time series study (1972-2014). J Prev Med Public Health 51:140–147. https://doi.org/10.3961/jpmph.17.153
To T et al (2015) Chronic disease prevalence in women and air pollution — A 30-year longitudinal cohort study. Environ Int 80:26–32. https://doi.org/10.1016/j.envint.2015.03.017
Van Donkelaar A, Martin RV, Li C, Burnett RT (2019) Regional estimates of chemical composition of fine particulate matter using a combined geoscience-statistical method with information from satellites, models, and monitors. Environ Sci Technol 53:2595–2611. https://doi.org/10.1021/acs.est.8b06392
Wu Z, Zhang Y, Zhang L, Huang M, Zhong L, Chen D, Wang X (2019) Trends of outdoor air pollution and the impact on premature mortality in the Pearl River Delta region of southern China during 2006–2015. Sci Total Environ 690:248–260. https://doi.org/10.1016/j.scitotenv.2019.06.401
Xu X, Xu Z, Chen L, Li C (2019) How does industrial waste gas emission affect health care expenditure in different regions of China: an application of Bayesian quantile regression. Int J Environ Res Public Health 16:2748. https://doi.org/10.3390/ijerph16152748
Yang J, Zhang B (2018) Air pollution and healthcare expenditure: implication for the benefit of air pollution control in China. Environ Int 120:443–455. https://doi.org/10.1016/j.envint.2018.08.011
Zeng J, He Q (2019) Does industrial air pollution drive health care expenditures? Spatial evidence from China. J Clean Prod 218:400–408. https://doi.org/10.1016/j.jclepro.2019.01.288
Zeng, Du, Zhang (2019) Spatial-temporal effects of PM2.5 on health burden: evidence from China. Int J Environ Res Public Health 16:4695. https://doi.org/10.3390/ijerph16234695
Zhao X, Yu X, Wang Y, Fan C (2016) Economic evaluation of health losses from air pollution in Beijing, China. Environ Sci Pollut Res 23:11716–11728. https://doi.org/10.1007/s11356-016-6270-8
Zhao H, Cao X, Ma T (2020) A spatial econometric empirical research on the impact of industrial agglomeration on haze pollution in China. Air Qual Atmos Health. https://doi.org/10.1007/s11869-020-00884-w
Zhou M et al (2019) Mortality, morbidity, and risk factors in China and its provinces, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet 394:1145–1158. https://doi.org/10.1016/S0140-6736(19)30427-1
Funding
This research is supported by the Project of National Social Science Foundation of China (NSSFC): Study on the Spatial Effects and Governance Strategies of the Impact of Urban Haze Pollution on Public Health (No. 17BJY063).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interests
The authors declare that they have no conflict of interest.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
ESM 1
(DOCX 37 kb).
Rights and permissions
About this article

Cite this article
Sun, H., Leng, Z., Zhao, H. et al. The impact of air pollution on urban residents’ health expenditure: spatial evidence from Yangtze River Delta, China. Air Qual Atmos Health 14, 343–350 (2021). https://doi.org/10.1007/s11869-020-00939-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11869-020-00939-y