
Abstract
The development of air quality management (AQM) strategies provides opportunities to improve public health and reduce health inequalities. This study evaluates health and inequality impacts of alternate SO2 control strategies in Detroit, MI, a designated non-attainment area. Control alternatives include uniform reductions across sources, ranking approaches based on total emissions and health impacts per ton of pollutant emitted, and optimizations that meet concentration and health goals. Using dispersion modeling and quantitative health impact assessment (HIA), these strategies are evaluated in terms of ambient concentrations, health impacts, and the inequality in health risks. The health burden attributable to SO2 emissions in Detroit falls primarily among children and includes 70 hospitalizations and 6000 asthma-related respiratory symptom days annually, equivalent to 7 disability-adjusted life years (DALYs). The health burden disproportionately falls on Hispanic/Latino residents, residents with less than a high school diploma, and foreign-born residents. Control strategies that target smaller facilities near exposed populations provide the greatest benefit in terms of the overall health burden reductions and the inequality of attributable health risk; conventional strategies that target the largest emission sources can increase inequality and provide only modest health benefits. The assessment is novel in using spatial analyses that account for urban scale gradients in exposure, demographics, vulnerability, and population health. We show that quantitative HIA methods can be used to develop AQM strategies that simultaneously meet environmental, public health, and environmental justice goals, advancing AQM beyond its current compliance-oriented focus.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Background
Air quality management (AQM) is an iterative process that involves setting standards for air quality, designing and implementing control strategies to achieve these standards, and then assessing air quality status and progress towards these standards (NRC 2004). In the USA, states and the federal government use the National Ambient Air Quality Standards (NAAQS), which are intended to be protective of public health with an adequate margin of safety for sensitive subpopulations (NRC 2004). Currently, AQM focuses on compliance with these standards. However, this may not provide the desired level of public health protection for several reasons. First, NAAQS compliance is based on concentrations measured at a limited number of fixed monitoring stations, which may not reflect the spatial variation in concentrations and the true exposure of the population (Levy and Hanna 2011; Matte et al. 2013). Second, the NAAQS may fall short of protecting individuals and groups who are susceptible, that is, at increased risk of adverse health effects at a particular concentration due to characteristics that increase their sensitivity, e.g., respiratory disease, as well as vulnerable, that is, at greater likelihood of higher exposure due to factors that reduce the ability to avoid or mitigate high exposures, e.g., low socioeconomic status (SES) and residence location (O’Neill et al. 2012; Sacks et al. 2011). Vulnerability and susceptibility vary spatially, and subpopulations having both high sensitivity and high exposure are more likely to experience adverse health impacts than the general population. Third, it is challenging or perhaps impossible to select a sufficiently protective regulatory standard when no effect threshold (i.e., a level below which health effects do not occur) has been identified. Ambient air quality standards are informed by integrated science assessments (previously called “criteria documents”) and staff papers which summarize and synthesize the exposure, toxicological, and epidemiological literature, but ultimately, the designation of the standard is a policy decision made by the US EPA Administrator (NRC 2004). Additional concerns for AQM strategies based on NAAQS compliance include the single pollutant approach (i.e., the exclusion of cumulative impacts), delays in attaining compliance (in part due to the need for multiple years of monitoring data), and the technical, administrative, and legal steps involved in establishing and implementing policies to attain the NAAQS.
Health impact assessment (HIA) uses a comprehensive approach to evaluate health impacts that arise from programs, projects, or policies (Bhatia et al. 2014; Dannenberg 2016). HIA is becoming an accepted approach for estimating health impacts of air quality and the benefits of AQM options, and HIA tools have been developed to facilitate HIA analyses (Anenberg et al. 2015). HIAs for AQM can incorporate information from air quality models, ambient air monitoring, population demographics, environmental epidemiology, and other sources. In a “full” HIA, quantitative assessments estimate the morbidity and mortality attributable to pollutant exposure (US EPA 2010a), and complementary qualitative analyses evaluate the benefits and adverse impacts that are not included in the quantitative assessment. HIAs have been used to examine potential impacts from power plants and other emission sources at regional and national levels (e.g., Buonocore et al. 2014; Fann et al. 2009). Impacts of specific pollution sources at local or urban levels can be examined given appropriate input data, e.g., baseline health outcome incidence rates and exposure estimates (Hubbell et al. 2009).
Inequality metrics quantify the distribution of health impacts or benefits across space (e.g., census blocks) or groups (e.g., minority populations). These metrics can indicate how an AQM option affects the outcome distribution (Maguire and Sheriff 2011), key information for environmental justice analyses that evaluate whether certain groups experience disproportionate adverse effects from environmental hazards (Brulle and Pellow 2006). Preferred indicators or metrics for environmental justice analyses have been identified (Levy et al. 2006). For example, the Atkinson index (AI), originally developed as an income inequality parameter, evaluates inequality across individuals or units (e.g., census blocks). It includes a subjective “inequality aversion” parameter, which accounts for societal attitudes towards inequality, and it can be decomposed to examine differences between groups, e.g., race and ethnicity groups (Levy et al. 2006). Larger AI values indicate greater inequality in the distribution of risk. Another inequality metric, the concentration index (CI), examines the distribution of health burdens across population subgroups ranked by social status (O’Donnell et al. 2008). The CI plots the cumulative distribution of health risks against the cumulative ranking of census blocks ordered by the selected demographic or SES variable, and is calculated as the area under the 1:1 line minus the area under the concentration curve. Negative CI values indicate that less socially advantaged groups carry disproportionately heavier health burdens. This metric has been used to evaluate a variety of environmental hazards, e.g., PM2.5, ozone, traffic density, and proximity to toxic release sites (Cushing et al. 2015; Sadd et al. 2011; Su et al. 2009, 2012). Despite their usefulness in quantifying environmental inequalities, inequality metrics are not routinely used in regulatory or other analyses (Harper et al. 2013).
Determining whether an AQM strategy will attain ambient standards, minimize health impacts, and reduce inequalities requires combining health impact metrics with inequality metrics and possibly other information. For example, a study examining power plant emissions in the USA found that controlling sources with the largest health impacts per unit emissions conferred the greatest health benefits and inequality reductions (Levy et al. 2007). A study investigating controls for PM2.5 and ozone precursors in Detroit, MI, showed that a multipollutant approach achieved better health and inequality benefits compared to single pollutant strategies (Fann et al. 2011; Wesson et al. 2010). These examples combined quantitative health impact and inequality metrics either using large study areas with coarsely resolved exposure and health data (Levy et al. 2007) or pollutants with low spatial variability, e.g., ozone and PM2.5 (Fann et al. 2011; Wesson et al. 2010). AQM strategies evaluating health impacts and inequalities have not been applied to pollutants that have significant spatial variability at the intra-urban scale, despite their considerable promise to benefit populations and their relevance to many environmental justice applications.
Objectives
This study investigates emission control strategies aimed at reducing the burden of disease and health burden inequalities. Alternative strategies are formulated and evaluated in terms of ambient concentrations, total health benefits, and the distribution of health impacts across an urban population. We quantify the potential trade-offs between emission reductions, health impacts, and inequality and demonstrate how health burden and inequality metrics might be used at an urban scale and in a regulatory context.
Methods
HIA methods are used to estimate the burden of disease attributable to SO2 exposures in southeast Michigan. Two sets of emission control strategies are considered. The first reduces current (ongoing) emissions at major sources in the area, and thus represents actual or typical exposure to SO2 in the study area. The second examines alternatives to a proposed state implementation plan (SIP) that follows EPA guidance, which starts with the maximum allowable emissions based on existing and revised permits (US EPA 2005); this analysis highlights issues related to using the maximum allowable emissions in SIP development. The study area includes Detroit and “downriver” cities and includes the portion of Wayne County designated as non-attainment for the 2010 SO2 ambient air quality standard (MDEQ 2016). The control strategy options, evaluative metrics, and study area are described below. Additional information regarding the HIA methods and data sources is provided in the Supplemental Materials.
SO2 emission inventory and estimates of population exposures
SO2 emission estimates are derived from 2010 to 2014 stack-level data retrieved from the Michigan Air Emissions Reporting System (MAERS; MDEQ 2001). For major sources in the region (i.e., sources emitting more than 100 t of SO2 per year), emissions are modeled at the stack level; for other sources, facility-level emissions are used. Eight major SO2 sources fall within the SO2 non-attainment area (Fig. 1): three coal-powered electrical generating facilities (DTE Trenton Channel, DTE River Rouge, Dearborn Industrial Generation), two large steel facilities (US Steel at Zug Island and Ecorse, Severstal/AK Steel), two lime and coke facilities (EES Coke, Carmeuse Lime), and an oil refinery (Marathon). None of these facilities use add-on control technologies for SO2 (MDEQ 2016). The analysis also includes 126 other point source facilities in the area, including the DTE Monroe power plant. This facility, located approximately 60 km south of Detroit, is the state’s largest coal-fired power plant (3300 MW) and recently installed scrubbers to significantly reduce SO2 emissions. The nine largest sources account for 92% of SO2 point source emissions in southeast Michigan. Because reported emissions fluctuate annually, we averaged emissions for the 2010 to 2014 period. In cases, only the more recent data were used to account for known changes over time. These represent current or “base case” emissions.

Study area, boundaries of the SO2 non-attainment area, and locations of major point sources of SO2
Population-level exposures are estimated using the Framework for Rapid Emissions Scenario and Health Impact Estimation (FRESH-EST), a software package that allows rapid assessment of exposures and health impacts due to point source emissions for a given areal unit, e.g., census blocks (Milando et al. 2016). Briefly, ambient SO2 concentrations attributable to point source emissions are estimated at a set of discrete locations (“receptors”) using a source receptor or “transfer coefficient” matrix developed using the AERMOD dispersion model (Cimorelli et al. 2005), local meteorology, and an adaptive receptor grid (200-m spacing near major sources and 1-km spacing elsewhere). We interpolate from the receptor grid to a 25-m raster using inverse-distance weighting and use the average of raster cells overlapping census block polygons to estimate exposure concentrations. FRESH-EST includes an optimization module to minimize point source emissions to attain specified receptor concentrations or maximize health benefits, subject to other constraints.
Census blocks are used as the spatial unit of analysis, balancing the need for accurate exposure assessment with the available population and baseline health data (Batterman et al. 2014). Time-activity patterns that account for working and living in areas with different pollutant levels are not considered. Although this may lead to exposure measurement errors and possible biases in health impact estimates, the epidemiological studies underlying the concentration-response coefficients mostly rely on area monitors and residence locations to assign exposures.
SO2 emission control alternatives
Strategies to reduce emissions of SO2
Baseline emissions from point sources are used to represent “current” exposures and health impacts attributable to these sources under current operating conditions; this is the base case strategy designated “S0.” Five types of strategies are considered (Table 1). Each is evaluated at six levels that represent 15, 30, 45, 60, 75, and 90% reductions in aggregate SO2 emissions from baseline levels. Individual major sources can reduce emissions by up to 90%, the maximum control attainable with add-on technologies, e.g., flue gas desulfurization (Srivastava and Jozewicz 2001). We focus on reducing emissions at the eight major sources located within the non-attainment area.
The simplest approaches apply uniform reductions across all sources (strategy S1) or controls at the largest facilities first (S2) to meet reduction goals. The “health impact ranking” strategy (S3) ranks sources by the health impacts per ton of SO2 emitted, and imposes reductions on the highest ranked sources first until the emissions target is met (Levy et al. 2007). Strategies S4 and S5 minimize receptor concentrations and maximize health benefits (i.e., minimizing disability-adjusted life years (DALYs)), respectively, using the FRESH-EST optimization module with constraints that limit emissions at each source (allowing between 10 and 100% of baseline emissions) and that attain the emission target (summed across major sources). For all of these strategies, emissions at DTE Monroe and the 125 minor facilities remain at baseline.
SIP base case, control strategy, and optimized alternatives
The SIP strategy proposed by Michigan Department of Environmental Quality (MDEQ) started with the maximum allowable SO2 emissions and considered SO2 monitoring data, dispersion modeling, and Reasonably Achievable Control Technology (RACT) analyses (MDEQ 2016). It identified five culpable sources after conducting a hotspot analysis (DTE River Rouge, DTE Trenton Channel, US Steel, EES Coke, Carmeuse Lime), and called for emission reductions at the DTE plants and US Steel, the shutdown of specific boilers at the DTE plants, and the construction of a taller stack at Carmeuse Lime; no changes were required at EES Coke (MDEQ 2016). In the “SIP maximum allowable case” (strategy S6), we use the existing maximum allowable emissions at major sources (MDEQ 2016, pp. 15–16) and current emissions at other sources (as described in “SO2 emission inventory and estimates of population exposures” section). The “SIP control strategy” (S7) implements the MDEQ SIP strategy (MDEQ 2016) with other emissions unchanged from S6.
Two additional alternatives that attain the overall SO2 reduction specified in the SIP (26,418 t per year) are evaluated. Strategy S8 minimizes the maximum receptor concentration, and strategy S9 maximizes health benefit. Both allow emission reductions at only the five culpable sources identified by MDEQ; stack heights are unchanged. For strategies S7–S9, the SIP maximum allowable case (S6) serves as the comparison (base case) strategy.
Health impact assessment
Outcomes associated with SO2 exposure include hospitalizations for respiratory diseases, asthma-related emergency department visits, and asthma symptom days among children. FRESH-EST uses health impact functions to estimate the numbers of these outcomes attributable to SO2, similar to those in other HIA tools (e.g., US EPA 2015). Only health outcomes for which a causal relationship with SO2 exposure has been established are considered, as determined by US EPA (US EPA 2008, 2016a), which may under-predict the true health burden. We assume a no-threshold concentration-response (CR) relationship between SO2 exposures and health effects, consistent with US EPA conclusions regarding the lack of evidence of a population-level exposure threshold (US EPA 2008, 2016a). Health impacts are calculated using 24-h average SO2 concentrations, which is consistent with the epidemiological studies from which CR coefficients are drawn. Uncertainty in the health impact estimates, represented as a 95% confidence interval, is estimated using the uncertainty around the CR coefficient, which has been shown to account for substantial portion of the total uncertainty in quantitative health impact estimates (Chart-asa and Gibson 2015).
Evaluative metrics
Control strategies are evaluated using concentration, health impact, and inequality metrics. For the concentration metric, we use the fourth highest 1-h daily maximum SO2 concentration at non-fenceline receptors. This is similar but not identical to the form of the SO2 NAAQS definition, which uses the 3-year average of the annual fourth highest 1-h daily maximum concentrations (US EPA 2010b). Health impacts are reported as the number of attributable cases and DALYs, which aggregate the health outcomes into a single summary metric based on time lost to poor health (Murray 1994). DALYs provide a measure of the total health burden, including hospitalizations and asthma exacerbations in older adults and children, respectively, by more heavily weighting more severe but less frequent outcomes, e.g., hospitalizations, than more frequent but less severe outcomes, e.g., days with asthma symptoms. Disability weights and durations for DALYs are drawn from existing studies (CDC 2012; de Hollander et al. 1999; Murray 1994; Ostro 1987). Attributable cases are monetized using values (in 2010$ adjusted to a 2020 income level) reported by the US EPA in the most recent Regulatory Impact Assessment for fine particulate matter (US EPA 2012).
Inequality of the health burden is examined using the AI and the CI. For the AI, the inequality parameter is set to 0.75 following prior AQM work (Fann et al. 2011). For the CI, the required spatially resolved demographic and SES data to rank the vulnerability of census blocks uses seven (block group level) variables from the 2014 5-year American Community Survey (Supplemental Fig. 2): percentage of the population that is non-white, Hispanic or Latino, persons of color, foreign born, or with less than a high school diploma; median household income (inflation-adjusted 2014 dollars); and percentage of households with past year income below the poverty level (US Census Bureau 2014).
The inequality of the health burden is based on the risk of SO2-attributable DALYs. The use of attributable (rather than total) DALYs helps assess whether the SO2 reduction strategies result in “fair treatment” of all population subgroups, i.e., that each subgroup receives a benefit as a result of AQM actions (US EPA 2016b). The mean estimate of DALYs generated by the health impact functions is used to assess health impact and inequality metrics.
Description of the study area and population
The study area includes much of Detroit and Wayne County in southeast Michigan, including the designated SO2 non-attainment area (MDEQ 2016) (Fig. 1). A total of 1,136,696 people lives in the study area (US Census Bureau 2014). Air pollution has been and remains an important environmental health concern for southeast Michigan residents. Due to its industrial legacy, Detroit contains many large SO2 sources. Detroit has experienced substantial outmigration, and residents remaining may be vulnerable to adverse health effects of air pollutant exposures. The population is mostly minority (83% non-Hispanic Black, 7% Latino or Hispanic), and 39% live below the poverty line (US Census Bureau 2015). Access to health care is an important challenge, e.g., 25% of Detroit adults report not having seen a doctor at least once in the last year for cost reasons, a rate significantly higher than the state average of 15% (MDHHS 2015). Health disparities are significant, particularly for diseases associated with air pollution, e.g., rates of asthma hospitalizations and deaths in Detroit exceed state averages by 3.5 and 2.4 times, respectively (DeGuire et al. 2016).
Results
Exposures and burden of disease
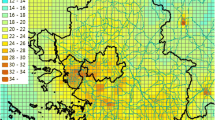
SO2 exposures across the study area vary considerably. Figure 2a maps annual mean concentrations for the base case (S0). Levels are highest in southwest Detroit where several major sources are clustered (Fig. 1). The fourth highest 1-h daily maximum concentration occurs in this area, but areas to the north also experience high concentrations (Fig. 2b). (The fourth highest 1-h daily max concentrations shown are not necessarily contemporaneous.) Table 2 summarizes the distribution of hourly SO2 concentrations at receptors, daily mean SO2 concentrations at the census block level, and daily 1-h maximum SO2 concentrations at the Southwest High School (SWHS) monitoring site. Comparisons of predicted and observed daily mean SO2 concentrations at SWHS, which recorded the highest SO2 levels in the area, showed no significant differences (K-S test, p > 0.05, Supplemental Fig. 3), suggesting that point source emissions account for SO2 concentrations in the area and that the dispersion model replicates the observed distribution.

Annual mean (a) and fourth highest 1-h daily maximum (b) SO2 concentrations (ppb) for the base case (S0). Based on 5-year average emissions of SO2, 2012 meteorology, and all point sources. The solid blue line shows the HIA study area; the dashed green line shows the SO2 non-attainment area
The burden of disease from SO2 falls mostly among children. For the base case, health impacts include 7 hospitalizations for asthma, 95 ED visits for asthma, and over 6000 days with asthma-related respiratory symptoms (i.e., exacerbations; Supplemental Table 3). This is equivalent to 7 DALYs and $2.7 million in monetized impacts each year, most (> 90%) of which is from asthma-related respiratory symptom days. Asthma exacerbations increase fourfold using a Detroit-specific CR coefficient (Batterman et al., manuscript in preparation), reflecting the potentially higher vulnerability of Detroit children to SO2 exposures. These estimates only reflect health impacts from SO2 exposures and do not include health impacts that would result from the formation of secondary aerosols (e.g., PM2.5) from SO2, which may substantially exceed the impacts from SO2 alone (US EPA 2010a).
Health impacts by sources
Table 3 lists SO2 emissions, attributable health impacts as DALYs per year, and annual health impacts per 100 t of SO2 emitted by the major sources, information which guides the emissions and health-oriented ranking strategies (S2 and S3). (For comparison, the table includes DTE Monroe, which was excluded from the control strategies as its location is outside the non-attainment area.) The 125 minor sources emit 8% of the SO2 in the inventory and cause 11% of the health burden. Importantly, rankings of major sources by emissions, DALYs, and health impacts differ, e.g., the highest ranked source for total emissions (excluding DTE Monroe) is DTE Trenton Channel; the top source for DALYs is US Steel, and the top source for DALYs per 100 t SO2 is Carmeuse Lime. Although SO2 emissions from Carmeuse Lime, Detroit Industrial Generation, and Severstal/AK Steel are relatively small (< 800 t per year each), their proximity to residential neighborhoods and low stack heights increase SO2 exposure per ton of emissions, thus increasing the burden attributable to these facilities.
Comparison of SO2 control strategies
Fourth highest 1-h daily maximum SO2 concentration
The “peak” (fourth highest 1-h daily maximum) SO2 concentrations for six control strategies are shown in Table 4. For the base case (0% reduction), the peak (79.5 ppb) exceeds the NAAQS concentration (75 ppb). At each SO2 reduction target, the “largest emissions first” (S2) approach gives the highest peak concentration; the “receptor-concentration optimization” (S4) gives the lowest. With full (90%) reductions, the peak concentration falls to 56.2 ppb. Despite the high level of SO2 emission reductions, peak concentrations do not drop further because emissions from excluded facilities (DTE Monroe and the minor facilities), which emit nearly 60% of the total SO2 emissions in the area combined, remain unchanged from baseline.
Total attributable health burden
Trade-offs between health improvements (DALYs per year) and inequality (AI) are depicted in Fig. 3 for each control strategy type. (Comparable figures showing the trade-offs between health impacts and the CI are provided in the Supplemental Materials). The health burden decreases from 7.0 DALYs per year for the base case to 2.6 DALYs per year for 90% emission reductions (Table 5). The health burden falls less than 90% since emissions at DTE Monroe and the minor point sources do not change. While any emission reduction lowers the health burden, some strategies are more effective. The uniform reduction strategy (S1) provides nearly linear improvements, as expected. For low to moderate emission reductions (15–45%), reducing emissions at sources with the highest impacts per ton of emissions (S3) yields greater health benefits than the uniform percentage (S1) and the minimal concentration (S4) strategies. Although advantages diminish beyond 60% reductions, strategy S3 still outperforms S1 and S2 due to its emphasis on reducing emissions at sources near large populations, i.e., sources with the highest health impact per unit emissions (Table 3). The concentration optimization strategy (S4) outperforms the uniform reduction approach for smaller reduction targets (15–45%), but benefits diminish at higher reduction goals. Results for health ranking (S3) and health optimization (S5) strategies are nearly identical for 30, 45, and 60% reduction goals, and the simpler health-based ranking approach (S3) achieves near-optimal results.

Attributable health burden (DALYs per year) versus Atkinson inequality index for each emission control alternative. Lines connect alternatives with the same SO2 emission reduction target (15 to 90%). AI inequality aversion parameter set to 0.75
Inequality of health impacts
Both inequality metrics suggest an unfair distribution in SO2-related health impacts (AI for the base case = 0.136). The CI indicates that the SO2-related health burden tends to disproportionately affect areas with high proportions of residents who are Hispanic or Latino, have less than a high school diploma, or are foreign-born (Table 5 shows CI metrics for selected reduction targets and blocks ranked by the percentage of Hispanic/Latino residents, persons of color, and median income; Supplemental Table 4 provides metrics for the full set of reduction targets and vulnerability characteristics). In the study area, these variables are moderately correlated (Pearson R 0.35–0.47), and census blocks with the highest proportions of Hispanic or Latino residents coincide with the highest SO2 exposures (southwest Detroit, Fig. 2a, Supplemental Fig. 2).
All of the strategies with one exception reduce the inequality of adverse health impact risks associated with SO2 (Fig. 3, Table 5, Supplemental Table 4). While reducing the overall health burden, the largest emissions-first approach (S2) strategy increases inequality, a result of increasing the relative importance of SO2 “hotspots” produced by smaller facilities. The lowest inequality occurs for the health impact optimization (S5) with a 75% reduction in total emissions (AI = 0.116, DALYs per year = 2.58). Increasing removals to 90% slightly lowers impacts (DALYs per year = 2.57) though inequality slightly increases (AI = 0.117) since reductions at all sources tends to increase inequality (as discussed above). Possibly the most striking result in Fig. 3, however, is the very large improvement in inequality and DALYs yielded by a very modest (15%) reduction of SO2 emissions with the health impact optimization (S5) strategy due to the high benefits per ton removed for targeted sources (Table 3); this strategy reduces emissions by 90% at AK Steel, Marathon, Dearborn Industrial Generation, Carmeuse Lime, and US Steel, and by 60% at EES Coke, while emissions at DTE Trenton Channel and DTE River Rouge are unchanged.
The distribution of benefits from SO2 reductions across social groups is strategy-dependent. The largest changes in the CI at intermediate SO2 reduction targets occur for the largest health impacts-first (S3) and the health optimization (S5) strategies. These strategies benefit Hispanic/Latino, low educational attainment, and foreign-born populations; this is important because these groups bear heavier burdens in the base case (Table 5, Supplemental Table 4, Supplemental Fig. 4). The “percentage of the population of persons of color” variable does not indicate a disproportionately high health burden from SO2 because most (> 90%) individuals in the study area identify as non-Hispanic Black or Hispanic/Latino (US Census Bureau 2015); aggregating these groups using a single variable ignores important demographic patterns across the city.
SIP versus optimized strategies
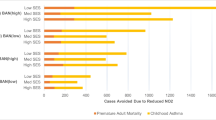
Since maximum allowable emissions are approximately twice that of the actual emissions, the SIP maximum allowable case (S6), SIP (S7), and optimized (S8 and S9) strategies give considerably higher concentrations and exposures (Supplemental Table 5) than those using actual emissions (Tables 2 and 4). The peak concentration (111 ppb for strategy S7) differs from the SIP (74 ppb; MDEQ 2016, p. 34) due to differences in receptor grids, years modeled, and the treatment of background. (A more detailed hotspot analysis, as performed by MDEQ, would be needed to ensure that the alternative strategies achieve the NAAQS and comply with US EPA criteria.) Like strategies based on actual emissions, reducing the maximum allowable emissions yields health benefits, and all strategies based on maximum allowable emissions reduce inequalities (Fig. 4). The SIP control (S7) and the concentration optimization (S8) strategies perform similarly; the health optimization alternative (S9) outperforms both of these strategies with respect to exposures, health benefits, and inequality. Note that strategies S7, S8, and S9 reduce emissions by the same amount (26,418 t per year). Based on the CI, the health-based approach is particularly beneficial for disproportionately impacted populations, e.g., areas with high proportions of Hispanic or Latino residents (Supplemental Table 6, Supplemental Fig. 5).

Attributable health burden (DALYs per year) versus Atkinson inequality index (inequality aversion parameter = 0.75) for the SIP maximum allowable (S6), the SIP control (S7), and two optimized (S8 and S9) strategies
Discussion
Health-based AQM strategies can yield large decreases in health burdens and the inequality of health risks, performing better than current strategies that prioritize compliance with the NAAQS. In Detroit, reducing emissions at sources with the largest health impacts (S3, S5) achieved the greatest benefits in attributable health burden and inequality. These sources tend to be smaller and closer to densely populated areas. In contrast, strategies focusing on the largest sources (S2) only modestly reduced health burdens and increased inequality. These sources mostly have tall stacks and are far from populated areas, and their resulting concentrations tend to be low and well dispersed. While emission reductions at these large sources lessen the health burden across broad areas, it increases the relative importance of smaller sources, thus increasing inequality. The inefficiency of the largest emissions-first strategy in terms of health benefits and its tendency to increase inequality is an important result that has not been emphasized elsewhere, in part because earlier studies primarily focused on total health risks rather than pollutant-attributable risks (e.g., Levy et al. 2007).
Benefits of using quantitative HIA analyses in the air quality management process
The development of a control strategy presents a prime opportunity for reducing health burdens and disparities, which is not taken advantage of in the current compliance-oriented approach. For example, the Detroit SO2 SIP submission specifies emission reductions at three facilities and stack height increases at another (MDEQ 2016), an approach derived following US EPA guidelines, negotiations with affected facilities, and RACT analyses. Unfortunately, this plan targets sources that have relatively low health impacts per ton of SO2 emitted (Table 3), and it will not alleviate disparities associated with SO2 exposures. This is supported by the “actual emissions” strategies (S1–S5), which better reflect current exposures than the SIP maximum allowable case (S6). While results in Figs. 3 and 4 are not directly comparable (these figures are based on “actual” and “maximum allowable emissions,” respectively), they each show that health-based strategies can yield bigger improvements in public health and health inequalities.
The use of the maximum allowable emissions is currently required for air quality modeling demonstrations of NAAQS attainment (US EPA 2005). For the nine major SO2 sources in Detroit, these maxima were up to four times higher than actual emissions, depending on the source. Thus, the use of maximum emissions greatly over-estimates health burdens and might not target the sources that actually cause the highest concentration, health, or inequality impacts. The NAAQS must be attained under all circumstance, so this rule is justifiable; however, a second analysis using actual emissions would improve the realism of exposure and health analyses and potentially result in healthier and fairer outcomes. Alternatively, the difference between actual and maximum allowable emissions could be reduced, perhaps to no more than a factor of 1.5, and then, a single analysis could simultaneously demonstrate that a proposed SIP strategy attains the NAAQS, maximizes health benefits, and minimizes inequality.
Multipollutant AQM approaches also can increase health and inequality benefits. An integrated and least-cost approach for PM2.5 and ozone in Detroit using “population-oriented reductions” was predicted to attain standards, lower total health impacts, and reduce inequality compared to strategies that addressed pollutants separately (Fann et al. 2011; Wesson et al. 2010). While we focused on a single pollutant, analyses of other pollutants could inform the evaluation and development of control alternatives.
Evolving towards more comprehensive and equitable air quality management
Reorienting AQM from standards compliance to consideration of site-specific health and inequality concerns is, in part, motivated by environmental justice and cumulative impact concerns. US EPA is becoming increasingly concerned with the “fair treatment” of all social groups when implementing environmental policies, and this extends to the distribution of health benefits as a result of policy actions (US EPA 2016b). The agency has expressed a preference for quantitative EJ analyses that complement other analyses in the rule making process (US EPA 2016c). Several state and local regulators are also formalizing EJ activities, including permitting, compliance, enforcement, and monitoring (e.g., MPCA 2015). These goals can be supported using the CI and other metrics. Our use of the SO2-attributable burden in inequality assessments helps identify whether the benefits of emission control strategies are fairly distributed, and it highlights how some population groups (Hispanic and Latino populations) receive fewer benefits under some of the strategies. Potentially, HIA tools and inequality metrics can show the rate of progress towards eliminating inequality, a potentially important EJ metric.
Quantitative HIA methods can enhance cumulative impact analyses, few of which have quantified health risks or impacts attributable to individual environmental hazards (Cushing et al. 2015). Most of these analyses have focused on assessing exposures to environmental hazards and identifying where minority or low-income populations are affected (e.g., Sadd et al. 2011; Su et al. 2009, 2012). As shown here and elsewhere, health burdens depend on many factors, e.g., exposures from an industrial facility are spatially varying, depending on distance, emissions, meteorology, population size, and vulnerability. Variation at the intra-urban scale can be large, e.g., risks in a small fenceline community near an industrial complex in Texas were lower than in the rest of the city due to prevailing winds (Prochaska et al. 2014). Thus, hazard scores considering only the presence or proximity of hazards may inadequately represent the exposure potential and likely impacts.
Health and inequality metrics could strengthen accountability research, which examines the outcomes of regulatory and other policy decisions (Bell et al. 2011). For example, changes in air pollutant levels improved lung function among children living in Los Angeles, California (Gilliland et al. 2017); health and inequality metrics could show whether these benefits are equitably and effectively distributed.
Considerations for quantitative HIAs
Burden of disease and inequality results can be affected by the location of air pollution sources, dispersion characteristics, the location of vulnerable and susceptible populations, administrative boundaries, and the spatial resolution of the analysis. As examples, estimating the base case health impacts for SO2 emissions at the ZIP code level in Detroit tremendously smooths gradients in exposure and lowers AI values; including areas with a high degree of social advantage (e.g., non-Hispanic white populations) or excluding potentially vulnerable populations can change CI values and possibly the groups identified as disproportionately harmed (Supplemental Table 7). Sensitivity analyses that vary spatial scales and study boundaries can help evaluate the robustness of HIA findings.
Importantly, no standards or thresholds have been established for inequality assessments, and small changes in inequality metrics may not be meaningful. In general, alternatives that decrease inequality relative to the base case will be favored provided that conditions are not worsened for the better-off groups. In Detroit, changes in inequality resulted from decreases in health burdens since emissions were not allowed to increase. In other applications, health burdens may increase, and thus, improvements in inequality must be coupled with an analysis showing how benefits are generated to ensure that no population subgroup is adversely impacted.
We did not consider costs or practicalities of pollution abatement. Costs will vary by source type, size, and other facility-specific factors. Typically, smaller facilities incur greater costs per ton removed due to unavoidable fixed costs, e.g., capital and operational costs (Becker 2005), and marginal costs usually increase at higher removal rates (Hartman et al. 2010). Based on abatement costs expressed as dollars per ton of pollutant removed, controls at large facilities may appear as more cost-effective, while reductions at smaller facilities may seem less economical. However, this accounting is incomplete: the lower per ton control costs at large facilities might yield lower health benefits, while the higher per ton costs at smaller facilities might be offset by greater health benefits. Many practical issues affect such assessments, e.g., the availability and ease of installing SO2 controls. As noted in the SIP, installing end-of-pipe controls at some sources could require substantial retrofitting because these facilities predate the requirement for SO2 removal technologies (MDEQ 2016).
Limitations
The HIA applications have important limitations. First, incidence rates in Detroit were available at county to ZIP code scales, which limits the ability to capture spatial variability. Second, information on individual-level exposures was not used, which can bias health impact estimates when people live in one area and work or attend school in other areas (Baccini et al. 2015; Tchepel and Dias 2011). Third, health impacts from secondary pollutants (e.g., sulfate particles formed from SO2) were not considered. Impacts (especially mortality) from secondary PM2.5 can far exceed those of SO2 (US EPA 2010a); however, secondary pollutant formation at the urban scale, which typically occurs at a regional scale and results in relatively homogeneous PM2.5 concentrations at the intra-urban scale (Turner and Allen 2008), may be modest. Fourth, sensitivity and uncertainty analyses were limited. Potentially important uncertainties include baseline incidence rates, dispersion modeling results, and the CRs (Mesa-Frias et al. 2013; O’Connell and Hurley 2009). Uncertainty in the CR will likely have the largest influence on health impact estimates (Chart-asa and Gibson 2015).
The inequality assessment is limited by the ability to identify all vulnerable or susceptible populations in the area. The American Community Survey (ACS) data allows some analysis by race or Hispanic/Latino ethnicity. In Detroit, 90% of the population identifies as Hispanic/Latino or non-Hispanic Black (US Census Bureau 2015). However, our study area also included the city of Dearborn, which is approximately 30% Arab or Arab-American (de la Cruz and Brittingham 2003), ethnicity data not yet routinely collected by the US Census Bureau. Many Arab and Arab American residents experience high exposures to social stressors, e.g., discrimination (Padela and Heisler 2010; Samari 2016), and therefore would be an important subpopulation to include in EJ and CI analyses.
Another limitation of this and other urban-scale assessments is their site-specific nature. The trade-offs between emission reduction, health burden, and inequality demonstrated for Detroit are site- and scenario-specific, driven by the unique combination of high degrees of population vulnerability and susceptibility, the proximity of several large sources, the spatially-variable pollutant concentrations, and other factors. We expect that results would differ for urban areas where sources are more distant or for analyses of regional pollutant such as ozone. Still, our findings appear broadly applicable. For example, a national assessment of power plants showed that reducing emissions at sources with the highest health impacts per ton of pollutant emitted maximizes improvements in health and inequality (Levy et al. 2007). Trends similar to those determined for Detroit are expected in other urban areas that have high concentrations of spatially varying pollutants, e.g., SO2, and industry and residential areas interspersed.
Conclusions
Air quality management (AQM) and control strategies can be improved by incorporating health and inequality metrics. The combination of spatially-variable exposures and known inequalities in susceptibility and vulnerability motivates the use of spatially resolved HIAs to assess health inequality as well as the health burden. In Detroit, MI, a designated SO2 non-attainment area, SO2 continues to have a substantial impact on the health of the population, particularly among children and Hispanic or Latino populations. AQM strategies that focused on emission sources with the highest health impacts per ton of pollutant emitted provided the greatest health benefit per ton of pollutant reduced; these strategies also reduced the inequality of health risks. In contrast, strategies targeting the larger emitters increased inequalities and sometimes provided minimal health benefits. Assessments that incorporate HIA techniques and inequality metrics are feasible and allow AQM to move beyond compliance with ambient standards towards strategies that promote health and equity.
References
Anenberg SC, Belova A, Brandt J, Fann N, Greco S, Guttikunda S, Heroux M-E, Hurley F, Krzyzanowski M, Medina S, Miller B, Pandey K, Roos J, Van Dingenen R (2015) Survey of ambient air pollution health risk assessment tools. Risk Anal:1–19. https://doi.org/10.1111/risa.12540
Baccini M, Grisotto L, Catelan D, Consonni D, Bertazzi PA, Biggeri A (2015) Commuting-adjusted short-term health impact assessment of airborne fine particles with uncertainty quantification via Monte Carlo simulation. Environ Health Perspect 123:27–33. https://doi.org/10.1289/ehp.1408218
Batterman S, Chambliss S, Isakov V (2014) Spatial resolution requirements for traffic-related air pollutant exposure evaluations. Atmos Environ 94:518–528. https://doi.org/10.1016/j.atmosenv.2014.05.065
Becker RA (2005) Air pollution abatement costs under the Clean Air Act: evidence from the PACE survey. J Environ Econ Manag 50(1):144-169. https://doi.org/10.1016/j.jeem.2004.09.001
Bell ML, Morgenstern RD, Harrington W (2011) Quantifying the human health benefits of air pollution policies: review of recent studies and new directions in accountability research. Environ Sci Pol 14:357–368. https://doi.org/10.1016/j.envsci.2011.02.006
Bhatia R, Farhang L, Heller J, Orenstein M, Richardson M, Wernham A (2014) Minimum elements and practice standards for health impact assessments, Version 3
Brulle RJ, Pellow DN (2006) Environmental justice: human health and environmental inequalities. Annu Rev Public Health 27:103–124. https://doi.org/10.1146/annurev.publhealth.27.021405.102124
Buonocore JJ, Dong X, Spengler JD, Fu JS, Levy JI (2014) Using the Community Multiscale Air Quality (CMAQ) model to estimate public health impacts of PM2.5 from individual power plants. Environ Int 68:200–208. https://doi.org/10.1016/j.envint.2014.03.031
Centers for Disease Control and Prevention [CDC] (2012) National Hospital Discharge Survey 2010. Selected Data Tables [WWW Document]. URL http://www.cdc.gov/nchs/nhds/nhds_tables.htm#number. Accessed 12.2.14
Chart-asa C, Gibson JM (2015) Health impact assessment of traffic-related air pollution at the urban project scale: influence of variability and uncertainty. Sci Total Environ 506–507:409–421. https://doi.org/10.1016/j.scitotenv.2014.11.020
Cimorelli AJ, Perry SG, Venkatram A, Weil JC, Paine RJ, Wilson RB, Lee RF, Peters WD, Brode RW (2005) AERMOD: a dispersion model for industrial source applications. Part I: general model formulation and boundary layer characterization. J Appl Meteorol 44:682–693. https://doi.org/10.1175/JAM2227.1
Cushing L, Faust J, August LM, Cendak R, Wieland W, Alexeeff G (2015) Racial/ethnic disparities in cumulative environmental health impacts in California: evidence from a statewide environmental justice screening tool (CalEnviroScreen 1.1). Am J Public Health 105:2341–2348. https://doi.org/10.2105/AJPH.2015.302643
Dannenberg AL (2016) A brief history of health impact assessment in the United States. Chron Health Impact Assess 1. https://doi.org/10.18060/21348
de Hollander AE, Melse JM, Lebret E, Kramers PG (1999) An aggregate public health indicator to represent the impact of multiple environmental exposures. Epidemiol Camb Mass 10:606–617
de la Cruz P, Brittingham A (2003) The Arab Population: 2000. [WWW Document]. URL: https://www.census.gov/prod/2003pubs/c2kbr-23.pdf. Accessed 11.16.16
DeGuire P, Cao B, Wisnieski L, Strane D, Wahl R, Lyon-Callo S, Garcia E (2016) Detroit: the current status of the asthma burden. Michigan Department of Health and Human Services, Lansing
Fann N, Fulcher CM, Hubbell BJ (2009) The influence of location, source, and emission type in estimates of the human health benefits of reducing a ton of air pollution. Air Qual Atmos Health 2:169–176. https://doi.org/10.1007/s11869-009-0044-0
Fann N, Roman HA, Fulcher CM, Gentile MA, Hubbell BJ, Wesson K, Levy JI (2011) Maximizing health benefits and minimizing inequality: incorporating local-scale data in the design and evaluation of air quality policies. Risk Anal 31:908–922. https://doi.org/10.1111/j.1539-6924.2011.01629.x
Gilliland F, Avol E, McConnell R, Berhane K, Gauderman WJ, Lurmann FW, Urman R, Chang R, Rappaport EB, Howland S (2017) The effects of policy-driven air quality improvements on children’s respiratory health (No. Research Report 190). Health Effects Institute, Boston
Harper S, Ruder E, Roman HA, Geggel A, Nweke O, Payne-Sturges D, Levy JI (2013) Using inequality measures to incorporate environmental justice into regulatory analyses. Int J Environ Res Public Health 10:4039–4059. https://doi.org/10.3390/ijerph10094039
Hartman RS, Wheeler D, Singh M (2010) The cost of air pollution abatement. Appl Econ 29:759–774. https://doi.org/10.1080/000368497326688
Hubbell BJ, Fann N, Levy JI (2009) Methodological considerations in developing local-scale health impact assessments: balancing national, regional, and local data. Air Qual Atmos Health 2:99–110. https://doi.org/10.1007/s11869-009-0037-z
Levy JI, Chemerynski SM, Tuchmann JL (2006) Incorporating concepts of inequality and inequity into health benefits analysis. Int J Equity Health 5:2. https://doi.org/10.1186/1475-9276-5-2
Levy JI, Hanna SR (2011) Spatial and temporal variability in urban fine particulate matter concentrations. Environ Pollut Barking Essex 1987 159:2009–2015. https://doi.org/10.1016/j.envpol.2010.11.013
Levy JI, Wilson AM, Zwack LM (2007) Quantifying the efficiency and equity implications of power plant air pollution control strategies in the United States. Environ Health Perspect 115:743–750. https://doi.org/10.1289/ehp.9712
Maguire K, Sheriff G (2011) Comparing distributions of environmental outcomes for regulatory environmental justice analysis. Int J Environ Res Public Health 8:1707–1726. https://doi.org/10.3390/ijerph8051707
Matte TD, Ross Z, Kheirbek I, Eisl H, Johnson S, Gorczynski JE, Kass D, Markowitz S, Pezeshki G, Clougherty JE (2013) Monitoring intraurban spatial patterns of multiple combustion air pollutants in New York City: design and implementation. J Expo Sci Environ Epidemiol 23:223–231. https://doi.org/10.1038/jes.2012.126
Mesa-Frias M, Chalabi Z, Vanni T, Foss AM (2013) Uncertainty in environmental health impact assessment: quantitative methods and perspectives. Int J Environ Health Res 23:16–30. https://doi.org/10.1080/09603123.2012.678002
Michigan Department of Environmental Quality [MDEQ] (2016) Sulfur dioxide one-hour national ambient air quality standard nonattainment state implementation plan for Wayne county (partial). Lansing, MI
Michigan Department of Environmental Quality [MDEQ] (2001) MDEQ - Michigan Air Emissions Reporting System (MAERS) Annual Pollutant Totals Query [WWW Document]. URL http://www.deq.state.mi.us/maers/emissions_query.asp. Accessed 3.25.16
Michigan Department of Health and Human Services [MDHHS] (2015) Chronic disease and health indicators [WWW Document]. URL http://www.michigan.gov/mdch/0,4612,7-132-2944_67827---,00.html. Accessed 6.22.15
Milando CW, Martenies SE, Batterman SA (2016) Assessing concentrations and health impacts of air quality management strategies: framework for Rapid Emission Scenario and Health impact ESTimation (FRESH-EST). Environ Int. https://doi.org/10.1016/j.envint.2016.06.005
Minnesota Pollution Control Agency [MPCA] (2015) Environmental justice framework 2015–2018
Murray CJ (1994) Quantifying the burden of disease: the technical basis for disability-adjusted life years. Bull World Health Organ 72:429–445
National Research Council [NRC] (2004) Air quality management in the United States. National Academies Press, Washington, DC
O’Connell E, Hurley F (2009) A review of the strengths and weaknesses of quantitative methods used in health impact assessment. Public Health 123:306–310. https://doi.org/10.1016/j.puhe.2009.02.008
O’Donnell O, van Doorslaer E, Wagstaff A, Lindelow M (2008) Analyzing health equity using household survey data: a guide to techniques and their implementation. The World Bank
O’Neill MS, Breton CV, Devlin RB, Utell MJ (2012) Air pollution and health: emerging information on susceptible populations. Air Qual Atmos Health 5:189–201. https://doi.org/10.1007/s11869-011-0150-7
Ostro BD (1987) Air pollution and morbidity revisited: a specification test. J Environ Econ Manag 14:87–98. https://doi.org/10.1016/0095-0696(87)90008-8
Padela AI, Heisler M (2010) The Association of Perceived Abuse and Discrimination after September 11, 2001, with psychological distress, level of happiness, and health status among Arab Americans. Am J Public Health 100:284–291. https://doi.org/10.2105/AJPH.2009.164954
Prochaska JD, Nolen AB, Kelley H, Sexton K, Linder SH, Sullivan J (2014) Social determinants of health in environmental justice communities: examining cumulative risk in terms of environmental exposures and social determinants of health. Hum Ecol Risk Assess 20:980–994. https://doi.org/10.1080/10807039.2013.805957
Sacks JD, Stanek LW, Luben TJ, Johns DO, Buckley BJ, Brown JS, Ross M (2011) Particulate matter-induced health effects: who is susceptible? Environ Health Perspect 119:446–454. https://doi.org/10.1289/ehp.1002255
Sadd JL, Pastor M, Morello-Frosch R, Scoggins J, Jesdale B (2011) Playing it safe: assessing cumulative impact and social vulnerability through an environmental justice screening method in the South Coast Air Basin, California. Int J Environ Res Public Health 8:1441–1459. https://doi.org/10.3390/ijerph8051441
Samari G (2016) Islamophobia and public health in the United States. Am J Public Health 106:1920–1925. https://doi.org/10.2105/AJPH.2016.303374
Srivastava RK, Jozewicz W (2001) Flue gas desulfurization: the state of the art. J Air Waste Manage Assoc 51:1676–1688. https://doi.org/10.1080/10473289.2001.10464387
Su JG, Jerrett M, Morello-Frosch R, Jesdale BM, Kyle AD (2012) Inequalities in cumulative environmental burdens among three urbanized counties in California. Environ Int 40:79–87. https://doi.org/10.1016/j.envint.2011.11.003
Su JG, Morello-Frosch R, Jesdale BM, Kyle AD, Shamasunder B, Jerrett M (2009) An index for assessing demographic inequalities in cumulative environmental hazards with application to Los Angeles, California. Environ Sci Technol 43:7626–7634. https://doi.org/10.1021/es901041p
Tchepel O, Dias D (2011) Quantification of health benefits related with reduction of atmospheric PM10 levels: implementation of population mobility approach. Int J Environ Health Res 21:189–200. https://doi.org/10.1080/09603123.2010.520117
Turner JR, Allen DT (2008) Transport of atmospheric fine particulate matter: part 2—findings from recent field programs on the intraurban variability in fine particulate matter. J Air Waste Manage Assoc 58:196–215. https://doi.org/10.3155/1047-3289.58.2.196
US Census Bureau (2015) Detroit QuickFacts [WWW Document]. URL http://quickfacts.census.gov/qfd/states/26/2622000.html. Accessed 6.9.15
US Census Bureau (2014) 2010–2014 American Community Survey (ACS) 5-year Estimates [WWW Document]. URL https://www.census.gov/programs-surveys/acs/. Accessed 10.6.16
US Environmental Protection Agency [US EPA] (2016a) Integrated science assessment (ISA) for sulfur oxides—health criteria (second external review draft) (No. EPA/600/R-16/351). U.S. Environmental Protection Agency, Washington, DC
US Environmental Protection Agency [US EPA] (2016b) EJ 2020 action agenda: environmental justice strategic plan 2016–2020. Washington, DC
US Environmental Protection Agency [US EPA] (2016c) Technical guidance for assessing environmental justice in regulatory analysis. Washington, DC
US Environmental Protection Agency [US EPA] (2015) BenMAP user’s manual. Research Triangle Park, NC
US Environmental Protection Agency [US EPA] (2012) Regulatory impact analysis for the final revisions to the national ambient air quality standards for particulate matter. Office of Air Quality Planning and Standards, Research Triangle Park, NC
US Environmental Protection Agency [US EPA] (2010a) Final Regulatory Impact Analysis (RIA) for the SO2 National Ambient Air Quality Standards (NAAQS). Office of Air Quality Planning and Standards, Research Triangle Park, NC
US Environmental Protection Agency [US EPA] (2010b) Primary national ambient air quality standard for sulfur dioxide. Fed Regist 75:35519–35603
US Environmental Protection Agency [US EPA] (2008) Integrated science assessment (ISA) for sulfur dioxide (health criteria). National Center for Environmental Assessment, Washington, DC
US Environmental Protection Agency [US EPA] (2005) Appendix W to part 51—guideline on air quality models. Fed Regist 70:68217–68261
Wesson K, Fann N, Morris M, Fox T, Hubbell B (2010) A multi-pollutant, risk-based approach to air quality management: case study for Detroit. Atmos Pollut Res 1:296–304
Acknowledgements
We thank Robert Sills and Keisha Williams at the Michigan Department of Environmental Quality Air Quality Division for their thoughtful comments and review of this manuscript
Funding
This research was funded by grant 5R01ES022616 from the National Institute of Environmental Health Sciences and by grant T42 OH008455 from the National Institute of Occupational Safety and Health. Additional support for this research was provided by grant P30ES017885 from the National Institute of Environmental Health Sciences, National Institutes of Health. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare they have no conflict of interest.
Electronic supplementary material
ESM 1
(DOCX 5106 kb)
Rights and permissions
About this article

Cite this article
Martenies, S.E., Milando, C.W. & Batterman, S.A. Air pollutant strategies to reduce adverse health impacts and health inequalities: a quantitative assessment for Detroit, Michigan. Air Qual Atmos Health 11, 409–422 (2018). https://doi.org/10.1007/s11869-017-0543-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11869-017-0543-3