
Abstract
Aim
To describe our experience of all patients presenting to a tertiary referral centre over a 5-year time period with acute scrotum and to investigate the role of Doppler ultrasonography (DUS) for investigating this group of patients.
Method
A retrospective analysis was performed on all patients presenting to the emergency department (ED) of a level 1 trauma centre with acute scrotum from 2009 to 2014 inclusive. Inclusion criteria included all patients who underwent an investigatory DUS and/or emergency scrotal exploration. Recorded patient demographics included age, presenting symptoms, duration of symptoms and relevant examination findings.
Result
Three-hundred and twelve patients were included with a mean age of 15 years (range 1 day–40 years). In total, 106 patients underwent immediate scrotal exploration, and testicular torsion (TT) was found in 30 % (n = 32/106). Two-hundred and twenty-two patients were initially investigated with DUS and 16 (7.2 %) proceeded to scrotal exploration. Of this sub-group, 2/16 presented with a history <24 h and exploration was negative for TT. In comparison, 14/16 presented with a history >24 h, and DUS findings were consistent with TT. No patients with a normal DUS represented to the ED after discharge.
Conclusion
DUS may prevent unnecessary scrotal exploration in patients presenting with acute scrotal pain and is useful for diagnosing TT in patients presenting with symptoms >24 h.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Acute scrotal pain is a common presentation to the emergency department (ED) with testicular torsion (TT) accounting for 25–35 % of acute paediatric scrotal disease [1]. If TT is suspected, early diagnosis and definitive management are essential for preventing testicular loss. Classically, TT presents with acute pain often associated with gastrointestinal symptoms such as nausea and vomiting. Important findings on clinical examination are a swollen high riding testis with an abnormal lie. Tenderness is maximal over the affect testis, and an absent cremasteric reflex is often found.
The clinical diagnosis of TT can be difficult as a number of infective testicular pathologies are also included in the differential diagnosis for the “acute scrotum” [2]. Scrotal exploration in the setting of a non-torted testis can prolong recovery times or exacerbate an infective process. Accurate selection of patients for urgent scrotal exploration is typically based on clinical parameters such as a convincing patient history, physical examination and urinalysis [3]. The use of Doppler ultrasonography (DUS) in the setting of an acute scrotum is controversial. Some clinicians advocate its routine use to contribute to the diagnostic process and others believe that DUS may delay definitive management thereby reducing the potential for testicular salvage [3–5].
Formal DUS is readily available in our ED and has been increasingly incorporated to contribute to clinical decision making for testicular pain; particularly, when the duration of presenting symptoms are greater than 24 h. The primary aim of the present study was to investigate and define a role for DUS in investigating acute scrotal pain. We also aimed to provide an overview of our management strategies for all patients presenting with an acute scrotum to the ED.
Materials and methods
Patient demographics
A retrospective analysis was performed on a prospectively maintained database of all patients who presented to the (ED) at a level 1 trauma centre [Cork University Hospital (CUH)] with acute scrotal pain between January 2009 and December 2014 inclusive. The recorded patient demographics included age, presenting symptoms, duration of symptoms and relevant examination findings. Dipstick urinalysis was performed on all patients, and the findings were recorded.
Patient classification
Patients were sub-classified into two sub-groups; those who had immediate scrotal exploration and those who underwent DUS examination proceeded by either surgical or conservative management. The histopathology reports of all patients who underwent orchidectomy at scrotal exploration were recorded. In patients undergoing DUS, the ultrasound was performed by a senior trainee or consultant radiologist using a linear high-frequency transducer in longitudinal and transverse planes to accurately assess the integrity of the testis. Colour Doppler was performed to establish vascular flow, and the contralateral testis was imaged for comparative purposes in all cases. In addition, the duration from presentation to DUS and from presentation to surgery was recorded and compared.
Follow-up
All patients undergoing scrotal exploration were offered follow-up 6 weeks after their initial presentation with clinical examination and repeat ultrasonography as indicated to evaluate testicular atrophy and discuss the option of a testicular prosthesis. Thereafter, further outpatient appointments and repeat ultrasonography were offered as indicated.
Results
Patient demographics
In total, 312 patients presented to ED with acute scrotal pain during the study period. Their relevant presenting symptoms and examination findings are demonstrated in Table 1. The mean age was 15 years (range 1 day–40 years), and the mean duration of history was 21 h (range 2–96 h). Ninety patients (29 %) underwent immediate scrotal exploration due to a high index of suspicion for TT and 222 patients (71 %) underwent DUS. After DUS, 16 patients (7 %) subsequently proceeded to scrotal exploration.
Doppler ultrasonography (DUS)
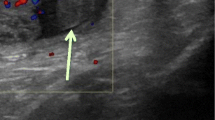
In total, 7 % (n = 16/222) of patients who underwent DUS had features of TT. Sonographic features consistent with testicular torsion included reduced or absent blood supply to the affected testis, heterogenous or hypoechoic appearance of the affected testis indicating necrosis and areas of echogenicity in the affected testis representing haemorrhage. Two patients had a duration of history <24 h and DUS was equivocal for TT. Subsequent scrotal exploration demonstrated a torted epididymal appendage in one and idiopathic scrotal oedema (ISO) in the other patient. Fourteen patients presented with a history >24 h and had DUS findings suggestive of TT. Intra-operatively, 11/14 patients had TT and 10 required orchidectomy, 3 patients had no macroscopic scrotal pathology and 1 patient underwent detorsion and bilateral orchidopexy. Figure 1 compares the timeframe of performing DUS relative to presentation with acute scrotum and the presence or absence of blood flow on DUS.

Timeframe of performing DUS relative to presentation with acute scrotum. Also compared is the presence or absence of blood flow on DUS over time. The majority of the patients (n = 70/106) presented during on-call service hours and the remainder (n = 36/106) presented between 9:00 and 17:00. Among the 70 patients presenting on-call, the mean duration from presentation to surgery was 2.4 h. This timeframe increased to 3.3 h in patients who underwent DUS prior to surgery. The interval from presentation to surgery was longer in patients presenting between 9:00 and 17:00 at 4.7 and 4.9 h with and without DUS, respectively. DUS was performed in 4/30 patients who presented during weekend hours. The interval to surgery was 4.3 h in the DUS group compared to 2.1 h in the group undergoing direct surgical exploration
Eighty-four patients (41 %) had features on ultrasonography that were consistent with an infective process (i.e. orchitis, epididymo-orchitis or epididymitis), and 80 patients (36 %) had no relevant scrotal pathology on DUS. Sonographic features consistent with an infective process included increased vascularity within the affected gonad, epididymal and/or testicular swelling with a reactive hydrocele in some cases. The pathology of the remaining patients is demonstrated in Table 2. No patients with a normal DUS represented to the ED after discharge.
Immediate scrotal exploration
The mean duration from presentation to surgery was 2.5 (range 0.5–6) hours in patients undergoing immediate scrotal exploration (n = 90). This increased to 4 (range 1.5–10.5 h) hours when DUS was performed initially (n = 16). The relevant intra-operative findings are demonstrated in Table 3. TT occurred in 32/106 (30 %) of patients undergoing immediate scrotal exploration and 15/32 (47 %) required orchidectomy. Within this sub-group all patients presented with testicular pain, 16 (50 %) with vomiting and 6 with a history of trauma (19 %). Clinically, 29 (91 %) had hemiscrotal swelling, 18 (56 %) had a high riding testicle or horizontal lie and 25 (78 %) had an absent cremasteric reflex on the side of the affected gonad (Table 4). Ten patients diagnosed with TT attended their 6 week follow-up outpatient review.
Discussion
There is increasing evidence for the routine use of DUS in evaluating patients with scrotal pain when this imaging modality is readily available. Waldert et al. prospectively assessed the diagnostic value of DUS in 236 patients with suspected TT and demonstrated that normal intratesticular perfusion obviates the need for scrotal exploration [3]. Although these findings are notable, caution should be observed with DUS when the history is <24 h as torted vessels may not immediately occlude testicular blood flow. During the ischaemic process, venous congestion initially occurs followed by oedema and the arterial supply only occludes when this process is at an advanced stage after 2 h with irreversible testicular damage occurs after 6 h. Although DUS is considered part of the diagnostic work up for acute scrotum in our institution, we acknowledge that multiple cases of missed torsions are described in the literature. Therefore, our policy is to explore all patients with symptoms and signs of TT as demonstrated by our initial exploration rate of 29 % (n = 90/312). However, the main finding of the present study is that DUS provides a useful adjunct in the diagnosis and management of patients presenting with scrotal pain >24 h in duration. Furthermore, our results also demonstrate that DUS may prevent unnecessary scrotal exploration in patients presenting with an acute scrotum.
There are a number of potential advantages for performing DUS in patients presenting with scrotal symptoms >24 h. After this timeframe, anatomical landmarks are difficult to appreciate on clinical examination and it can be difficult to differentiate TT from epididymo-orchitis (EO). In addition, surgeons may be able to confidently indicate to parents that orchidectomy will be necessary when patients are being consented for theatre. Formal DUS may also provide reassurance to patients presenting with an acute scrotum as no patients represented to the ED after the reassurance of a normal DUS. Other potential advantages are the avoidance of unnecessary surgical intervention with prolonged recovery and the cost benefit of preventing an unnecessary surgical procedure. Furthermore, a minority of patients presenting with an acute scrotum are diagnosed with testicular tumours. Radical orchidectomy necessitates an inguinal incision as opposed to a scrotal incision and this can be planned preoperatively if required.
Another important finding noted in the present study is that 19 % (n = 32) presented with a history of scrotal trauma. Based on this relatively high percentage, we would argue that a recent history of scrotal trauma cannot exclude testicular torsion, and an index of suspicion should be adopted in these specific cases. It should also be noted that torted appendices of the testis or epididymis are the most common cause for scrotal exploration in patients presenting with an acute scrotum, and our results are consistent with this finding (Table 3). Torsion of an epididymal or testicular appendage typically occurs in boys’ age 7–14 years, and tenderness is maximal over a palpable (blue) nodule on the antero-superior aspect of testis. Patients with epididymo-orchitis (EO), epididymitis or orchitis may present with a preceding history of lower urinary tract symptoms (LUTS) and associated pyrexia over a period of days. Infective pathologies and torted appendages can be successfully managed with conservative supportive measures.
Approximately, 90 % of torted testes are salvaged when patients present within 6 h of the onset of symptoms, and <10 % are salvaged when the presentation is >24 h after the onset. Our findings are consistent with these data as the salvage rate was 9 % (n = 1/11) in patients presenting with symptoms for >24 h. Moreover, the overall testicular salvage rate for torted testes in the present study was 53 % which is comparable to published reports that describe salvage rates ranging from 39 to 79 % [2, 6]. Previous reports have advocated scoring systems and nomograms based on clinical signs and symptoms to determine the risk of testicular torsion [7–10]. However, these studies are limited by their retrospective nature. Our analysis suggests that a combination of testicular pain and hemiscrotal swelling and the absence of a cremasteric reflex are red-flag symptoms and signs, and urgent scrotal exploration is merited in this setting.
A potential limitation of this study is its retrospective nature. Another limitation is the poor outpatient follow-up attendance rates. Patients with a history of TT are traditionally poor outpatient attendees during their follow-up, and this feature is evident in our study where only 10/32 (31 %) attended their 6 weeks review [11]. Another possible limitation is the lack of a formal cost benefit assessment for DUS and TT. The estimated cost of scrotal exploration and overnight hospital stay is €1700. In our study, 74 patients underwent scrotal exploration with negative findings for testicular torsion. Arguably, this approximates to an unnecessary cost of €125,000/$140,000/. The median indemnity payment for a missed torsion is approximately $45,000 as demonstrated in a retrospective study by Matterson et al. and this feature could be investigated in greater detail in a future study [12].
Conclusion
Our study demonstrates that approximately 30 % of patients presenting with acute scrotum are explored and 10 % have TT. When readily available DUS should be offered to patients presenting with an unconvincing history and inconsistent examination findings for TT as it may prevent unnecessary surgical intervention. This study also demonstrates that DUS contributes to the diagnostic process for patients presenting with scrotal pain with symptoms >24 h.
References
McAndrew HF, Pemberton R, Kikiros CS et al (2002) The incidence and investigation of acute scrotal problems in children. Pediatr Surg Int 18(5–6):435–437
Molokwu CN, Somani BK, Goodman CM (2011) Outcomes of scrotal exploration for acute scrotal pain suspicious of testicular torsion: a consecutive case series of 173 patients. BJU Int 107(6):990–993
Waldert M, Klatte T, Schmidbauer J et al (2010) Color Doppler sonography reliably identifies testicular torsion in boys. Urology 75(5):1170–1174
Altinkilic B, Pilatz A, Weidner W (2013) Detection of normal intratesticular perfusion using color coded duplex sonography obviates need for scrotal exploration in patients with suspected testicular torsion. J Urol 189(5):1853–1858
Tajchner L, Larkin JO, Bourke MG et al (2009) Management of the acute scrotum in a district general hospital: 10-year experience. ScientificWorldJournal 28(9):281–286
Yang C, Song B, Tan J et al (2011) Testicular torsion in children: a 20-year retrospective study in a single institution. ScientificWorldJournal 11:362–368
Boettcher M, Bergholz R, Krebs TF et al (2012) Clinical predictors of testicular torsion in children. Urology 79(3):670–674
Barbosa JA, Tiseo B, Barayan GA et al (2013) Development and initial validation of a scoring system to diagnose testicular torsion in children. J Urol 189(5):1859–1864
Pepe P, Panella P, Pennisi M et al (2006) Does color Doppler sonography improve the clinical assessment of patients with acute scrotum? Eur J Radiol 60(1):120–124
Baker LA, Sigman D, Mathew RI et al (2000) An analysis of clinical outcome using Color Doppler testicular ultrasound for testicular torsion. J Pediatr 105:604–607
Dalton DM, Davis NF, O’Neill DC et al (2014) Aetiology, epidemiology and management strategies for blunt scrotal trauma. Surgeon. doi:10.1016/j.surge.2014.06.006
Matteson JR, Stock JA, Hanna MK et al (2001) Medicolegal aspects of testicular torsion. 7:783–786 (discussion 786–787)
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
None.
Rights and permissions
About this article

Cite this article
Mohammed, W.M., Davis, N.F., O’Connor, K.M. et al. Re-evaluating the role of Doppler ultrasonography in patients presenting with scrotal pain. Ir J Med Sci 185, 705–709 (2016). https://doi.org/10.1007/s11845-015-1349-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11845-015-1349-7