
Abstract
Purpose
Most patients undergoing bariatric surgery (BS) are fertile women whose postoperative (post-op) hormonal balance and weight loss increases fertility, frequently leading to pregnancy. This study aims to analyze supplementation adherence of pregnant women after BS and perinatal outcomes.
Materials and Methods
This retrospective study analyzed records from women after BS who consulted nutritionists at least twice during pregnancy. Each patient received nutritional guidance about vitamin and mineral supplementation and protein intake. Demographic data, body mass index (BMI), percentage of weight loss (%WL) at conception, maximum post-op BMI and %WL, post-op time at conception, supplementation adherence, biochemical data, possible gestational complications, and infant’s birth weight were collected.
Results
Data was obtained from 23 women (mean age 33 ± 4 years). On average, patients became pregnant 43 months after surgery. The mean preoperative BMI was 40.2 kg/m2, the maximum post-op %WL was 36.6%, and the mean %WL at conception was 32.0%. No gestational intercurrence was related to biochemical data. Supplementation adherence was 34.7% for one multivitamin and 34.7% for two multivitamins; 43.5% for iron, 43.5% for omega 3, 39.1% for folic acid, 17.4% for B complex, and 60.8% for calcium. Mean infant birth weight was 3.0 kg, and it was not associated with maximum %WL, % WL at conception, and time since BS at conception.
Conclusion
Our data indicate satisfactory adherence to post-op micronutrient supplementation and few gestational complications following BS. Moreover, child’s birth weight was not associated with maximum %WL, %WL at conception, or time since BS.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Bariatric surgery (BS), allied to adequate follow-up by health professionals, is a well-established procedure for treating clinically severe obesity. Roux-en-Y gastric bypass (RYGB) is the most frequently performed procedure worldwide and is effective in reducing excess body weight and its comorbidities. The alterations in the digestive system following BS lead to food restriction and, to a lesser extent, nutrient malabsorption [1], thereby creating a nutritional risk. However, this can be prevented by adequate nutritional supplementation [2].
After BS, patients should be followed up by a multidisciplinary team to sustain their weight loss, while preventing complications, and be informed about nutritional supplementation. Despite these precautions, 60% of patients still present micronutrient deficiency, which can be attributed to inadequate adherence to nutritional supplementation. Non-adherence to supplementation correlates with higher rates of anemia, neurologic disorders, and bone diseases [3].
Most patients undergoing BS (around 70–80%) are fertile women [4]. Hormonal balance and weight loss increase fertility and therefore it is common that women get pregnant after BS [5, 6]. Also, when compared to women with obesity, post-BS patients present lower risk of GDM, large-for-gestational-age (LGA) infants, and an increased risk of small-for-gestational-age (SGA) infants and perioperative complications [7].
Pregnant women have increased nutritional requirements due to intense fetal and tissue growth, raising the risk of maternal and infant deficiencies. This leads to greater challenges to reach nutritional demands in post-BS pregnancies and makes supplementation more necessary. Therefore, the healthcare team should support these patients in maintaining their compliance [8]. This study aimed to analyze the adherence of post-BS pregnant women to supplementation recommendations and their perinatal outcomes.
Methods
This study was approved by the institutional review board of the School of Health Sciences of the University of Brasilia, and every participant gave a written informed consent.
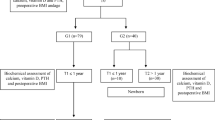
The records from patients followed up at least twice during gestation by nutritionists at a bariatric clinic were examined retrospectively. Inclusion criteria were as follows: post-RYGB females, conception post-BS, and at least two consultations during gestation with the abovementioned nutritionists.
The minimum sample size of 20 post-BS pregnant women was calculated based on a sample error of 20%, for a significance level of 5% and a nutritional deficiency prevalence of 27% [9].
During follow-up, all patients received nutritional supplementation prescription, i.e., daily use of two multivitamins, iron (oral and/or intravenous), calcium, vitamin D, omega 3 (DHA 100 mg, EPA 200 mg), B complex (oral and/or intravenous), and folic acid. They were also instructed to consume 80 g of protein/day.
We collected demographic data, %WL at conception, maximum post-BS %WL, post-op time at conception, supplementation adherence (adherence was considered as the intake of at least one multivitamin supplement daily), biochemical data (hemoglobin, hematocrit, serum ferritin, serum iron, transferrin, serum folic acid, fasting glycemia, serum vitamin B12), possible gestational complications (nausea, vomiting, dizziness, weakness, hypoglycemia, GDM, hypertension, placenta displacement), and infant birth weight.
Statistical analysis was conducted using SAS program, version 9.4 (SAS, Institute, Cary, NC, USA). Data from biochemical variables obtained in the first trimester of pregnancy were compared with those obtained in the second trimester. For variables showing Gaussian distribution in both quarters, the Student’s t test was used and the non-parametric Mann-Whitney test for those variables that did not present Gaussian distribution in both quarters. To compare the proportions of patients with pregnancy intercurrences or supplementation adherence among patients with or without biochemical abnormalities, Fisher’s exact test was used. To evaluate whether the maximum %WL, the %WL at conception, and the post-op time since BS before conception could explain infant birth weight, a multiple linear regression model was used, in which the infant birth weight was considered as a dependent variable, and the maximum %WL, %WL at conception, and post-op time since BS at conception as independent variables. The results were expressed by Pearson’s partial correlation coefficient, and p values < 0.05 were considered statistically significant.
Results
The data from 23 pregnant women (mean age of 33 ± 4 years) were analyzed. On average, patients became pregnant 43 months (± 32) postoperatively. The mean pre-op BMI was 40.2 kg/m2, the lowest mean post-BS BMI was 26.8 kg/m2, the maximum mean post-op %WL was 36.6%, the mean %WL at conception was 32.0%, and the mean pre-gestational BMI was 27.5 kg/m2.
Among the participants, 34.7% took one multivitamin supplement; 34.7%, two multivitamin supplements daily; 43.5%, iron and omega 3 supplementation; 39.1%, folic acid; 17.4%, B complex and 60.8%, calcium supplementation.
Biochemical data related to nutritional complications and supplementation adherence were overall within the normal range and showed no difference among the first and second trimesters of pregnancy (Table 1).
Concerning gestational intercurrences, 47.8% women reported nausea; 21.7%, vomiting; 21.7%, weakness and 8.6%, GDM. None was related to biochemical data. There were three cases of placental displacement and no cases of hypertension. There was no significant difference in weight gain, serum vitamin B12, and fasting glycemia levels between women reporting nausea, vomiting, and GDM and those not reporting these complications. Furthermore, there were no significant differences in hemoglobin, ferritin, serum iron, transferrin, fasting glycemia, and serum vitamin B12 between women reporting weakness, when compared to those not experiencing this symptom.
Regarding supplementation adherence, no significant differences occurred between the means of serum vitamin B12 among the pregnant women showing or not adherence to vitamin B complex supplementation. Similarly, no significant difference occurred between the means of serum folic acid among the pregnant women adhering or not to their specific multivitamin supplementation and no significant difference occurred between the means of hemoglobin, hematocrit, ferritin, serum iron, and transferrin among the pregnant women adhering or not to oral iron supplementation.
The mean infant birth weight was 3.0 kg. Multiple regression analysis indicated that infant birth weight was not associated with maximum %WL, %WL at conception, or time since BS at conception (Table 2).
Discussion
Our findings indicate that gestational intercurrences were mild and unrelated to nutritional deficiencies, as supplementation adherence was not associated with changes in biochemical tests. Moreover, the maximum %WL pre-gestation did not correlate with higher infant birth weight.
Data from previous studies suggest that gestation should occur at least 12 months post-BS, or that even longer periods following BS, from 18 [2] to 24 months [10, 11], may be necessary to optimize nutritional-related pregnancy outcomes. The first year post-BS is characterized by greater weight loss and low caloric intake (1100 to 1400 kcal), possibly related to nutritional deficiencies [11,12,13]. Besides the risk of prematurity, fetal nutrition may be impaired if gestation occurs in the first year post-op, since a diet of less than 1500 kcal is associated with risks of infant ketonemia and a low IQ after 2 years of age [10].
In our study, the post-op time for most patients was over 12 months, which is associated with a lower occurrence nutritional deficiency and weight loss problems. In Dixon et al. and Sheiner et al., only half of the patients became pregnant during the first year post-op, but no significant differences occurred in the prevalence of complications among them and those who became pregnant after the first year post-op [14, 15]. This is due to 100 and 61.5% of patients in these studies, respectively, were submitted to the adjustable gastric band (AGB) procedure, while only 3.8% of patients of Sheiner et al. were submitted to RYGB, more associated with nutritional deficiencies and greater short-term weight loss than AGB. Patel et al. assessed 26 RYGB patients and found no significant difference in relation to complications among BS patients who became pregnant shortly after and 2 years after surgery, explained by the small number of bariatric participants in the study [16]. Thus, more prospective studies with more participants are needed to evaluate the influence of time post-op on the proportion of post-RYGB gestational complications. Pre-op orientation, age, and multidisciplinary team care are important for the patient to instruct herself and prevent an early pregnancy. Fertile patients should be instructed to use contraceptives in the first year post-BS, seeking alternatives to the oral contraceptive in cases of mixed and malabsorptive procedures, such as the Mirena IUD and condom [17, 18]. Pregnancy occurring 18 months post-BS is considered safe, with constant monitoring of fetal growth, maternal weight gain, and biochemical tests [17].
The majority of the patients included in this study were close to or older than 35 years of age, which may correlate with a higher probability of intercurrences [19]. Notwithstanding, the frequency of intercurrences described in the medical records, such as GDM, vomiting, weakness, and hypertension was null or low. BS is capable of minimizing the occurrence of some pregnancy-related complications, such as gestational hypertension-preeclampsia (GH-P), GDM, LGA infants, and neonatal ICU admission [20]. However, BS may increase the risk of maternal anemia, prematurity, and hyperemesis gravidarum (more common in restrictive and mixed procedures) [20, 21]. To prevent anemia and hyperemesis gravidarum, nutritional guidelines, such as dividing intake among five to six meals, and using iron and thiamine supplementation, respectively, are necessary [9, 22]. The gestational intercurrences were not associated with nutrient deficiency in biochemical tests. Specifically, the 47.8% prevalence of nausea were not related to nutrient deficiency and may be explained by the hormonal changes that pregnant women suffer, especially in the first trimester, such as the increase of human chorionic gonadotropin (HCG) and progesterone [23].
Supplementation adherence assessed in this study was suboptimal but overall satisfactory, since over 60% of women were taking at least one multivitamin supplement and over 40% was taking except for iron, omega 3, and calcium. Other studies addressing supplementation adherence found similar adherence [10]. In the study by Dixon et al., analyzing supplementation of AGB patients, evidence showed that only 59% ingested supplements regularly and 23% had never ingested supplements [24]. A study by Hazart et al. found that only 37% of post-BS pregnant women routinely performed nutritional monitoring and that only 23.5% adhered to the proposed post-op supplementation, which increased to 56.8% in the periconceptional period, 77.8% in the first trimester, 96.3% in the second trimester, and 100% in the third trimester, after adequate orientation [25]. Thus, patients who lack nutritional guidance before gestation may not reach adequate gestational supplementation adherence [10]. In Devllieger et al., adherence to multivitamin, iron, and vitamin B12 supplementation ranged from 8.2 to 57.1%, depending on the trimester, with the highest in the first and the lowest in the third trimester, indicating a need of constant monitoring and encouragement [9]. It is necessary that the BS multidisciplinary teams have sufficient knowledge and information to instruct post-BS pregnant women, transmitting security and confidence, so that the supplementation adherence is effective. A recent study indicates that only 48% of the evaluated obstetricians felt “very comfortable” in caring for these patients, showing that the role of teamwork is essential to assist pregnant women with obstetricians [26].
In addition to the suboptimal despite satisfactory supplementation adherence by post-BS pregnant women, a study by Gadgil et al. indicates that the performance of laboratory tests for the diagnosis of nutritional deficiencies of bariatric patients in general is from 2 to 51%, depending on the vitamin, which increases significantly during gestation for some types of vitamin, but does not include more than 51% of pregnant women [27].
In this study, compliance, even if suboptimal, was not associated with intercurrences or nutritional deficiencies, indicating that prophylactic supplementation is efficient [28]. Considering the follow-up by a BS multidisciplinary team, these women may have been followed up pre-BS and have possibly received guidelines and prescriptions for correction and prevention of nutritional deficiencies from the outset. Prior to conception, bariatric women should receive specialized nutritional monitoring to correct possible nutritional deficiencies, including adequate intake of calories, proteins, and folic acid [11, 13, 28]. Adherence to folic acid supplementation, if low, underestimates the supplementation of this nutrient, since it is present in all multivitamins and some brands of complex B. Studies indicate cases of myelomeningocele in infants of bariatric women who did not adhere to folic acid supplementation [29] and a case of spina bifida due to deficiency of this nutrient [25].
Although there was no correlation between the maximum %WL and infant birth weight, the effective and maintained weight loss post-RYGB should be stimulated to prevent the occurrence of SGA newborns. In the literature, the relationship between BS (except Sleeve and AGB) and the birth of SGA infants, as well as the relationship between obesity and GDM and the birth of LGA infants are discussed [20]. Therefore, weight loss, as well as its maintenance, are benefits of BS that should be stimulated so that children develop adequately.
This study’s limitations include the lack of a control group, such as non-bariatric pregnant obese women or healthy-weight non-bariatric women. Also, because it was not a prospective study, there was no possibility of analyzing cause and effect relationships among several variables evaluated, such as biochemical data, supplementation adherence, and gestational intercurrences. Another limitation was the lack of follow-up of pregnant women until delivery, because it was a retrospective analysis of medical records, which, possibly, underestimated the prevalence of intercurrences, not allowing for analysis of other factors, such as gestational weight gain.
Conclusion
In conclusion, we found a suboptimal but overall satisfactory frequency of adequate adherence to nutritional supplementation among women who became pregnant after BS, and a low frequency of gestational complications and nutritional deficiencies. Moreover, infant birth weight was not associated with the maximum %WL, %WL at conception, or time since BS. These findings reinforce pregnancy safety following BS in women who receive nutritional follow-up in the setting of a multidisciplinary BS team, from the pre-op period, to correct and prevent possible nutritional deficiencies.
References
O’Kane M, Barth JH. Nutritional follow-up of patients after obesity surgery: best practice. Clin Endocrinol. 2016;84(5):658–61.
Mechanick JI, Youdim A, Jones DB, et al. Clinical practice guidelines for the perioperative nutritional, metabolic, and nonsurgical support of the bariatric surgery patient—2013 update: cosponsored by American Association of Clinical Endocrinologists, the Obesity Society, and American Society for Metabolic & Bariatric Surgery. Endocr Pract. 2013;19(2):337–72.
Goldenberg L, Pomp A. Management of Nutritional Complications. In: Nguyen N, Blackstone R, Morton J, Ponce J, Rosenthal R, editors. The ASMBS textbook of bariatric surgery. New York: Springer; 2015. p. 257–66.
Gimenes JC, Nicoletti CF, de Souza Pinhel MA, et al. Pregnancy after Roux en Y gastric bypass: nutritional and biochemical aspects. Obes Surg. 2017;27(7):1815–21.
Kothari SN. Impact of bariatric surgery on infertility. In: Nguyen N, Blackstone R, Morton J, Ponce J, Rosenthal R, editors. The ASMBS textbook of bariatric surgery. New York: Springer; 2015. p. 433–5.
Milone M, De Placido G, Musella M, et al. Incidence of successful pregnancy after weight loss interventions in infertile women: a systematic review and meta-analysis of the literature. Obes Surg. 2016;26(2):443–51.
Johansson K, Cnattingius S, Näslund I, et al. Outcomes of pregnancy after bariatric surgery. N Engl J Med. 2015;372(9):814–24.
Marangoni F, Cetin I, Verduci E, et al. Maternal diet and nutrient requirements in pregnancy and breastfeeding. An Italian consensus document. Nutrients. 2016;8(10):629.
Devllieger R, Guelinckx I, Jans G, et al. Micronutrient levels and supplement intake in pregnancy after bariatric surgery: a prospective cohort study. PLoS One. 2014;9(12):e114192.
The American College of Obstetricians and Gynecologists. Clinical Management Guidelines For Obstetrician–Gynecologists. ACOG practice bulletin no. 105: bariatric surgery and pregnancy. Obstet Gynecol. 2009;113(6):1405–13.
Narayanan RP, Syed AA. Pregnancy following bariatric surgery — medical complications and management. Obes Surg. 2016;26(10):2523–9.
Olbers T, Bjorkman S, Lindroos A, et al. Body composition, dietary intake, and energy expenditure after laparoscopic Roux-en-Y gastric bypass and laparoscopic vertical banded gastroplasty: a randomized clinical trial. Ann Surg. 2006;244(5):715–22.
Slater C, Morris L, Ellison J, et al. Nutrition in pregnancy following bariatric surgery. Nutrients. 2017;9(12):1338.
Dixon JB, Dixon ME, O’Brien PE. Birth outcomes in obese women after laparoscopic adjustable gastric banding. Obstet Gynecol. 2005;106(5 Pt1):965–72.
Sheiner E, Edri A, Balaban E, et al. Pregnancy outcome of patients who conceive during or after the first year following bariatric surgery. Am J Obstet Gynecol. 2011;204(1):50.e1–6.
Patel JA, Patel NA, Thomas RL, et al. Pregnancy outcomes after laparoscopic Roux-en-Y gastric bypass. Surg Obes Relat Dis. 2008;4(1):39–45.
Jans G, Matthys C, Bogaerts A, et al. Maternal micronutrient deficiencies and related adverse neonatal outcomes after bariatric surgery: a systematic review. Adv Nutr. 2015;6(4):420–9.
Uzoma A, Keriakos R. Pregnancy management following bariatric surgery. J Obstet Gynaecol. 2013;33(2):109–14.
Lean SC, Derricott H, Jones RL, et al. Advanced maternal age and adverse pregnancy outcomes: a systematic review and meta-analysis. PLoS One. 2017;12(10):e0186287.
Galazis N, Docheva N, Simillis C, et al. Maternal and neonatal outcomes in women undergoing bariatric surgery: a systematic review and meta-analysis. Eur J Obstet Gynecol Reprod Biol. 2014;181:45–53.
Kaska L, Kobiela J, Abacjew-Chmylko A, et al. Nutrition and pregnancy after bariatric surgery. IRSN Obes. 2013;2013:492060.
Kreykes A, Choxi H, Rothberg A. Post-bariatric surgery patients: your role in their long-term care. J Fam Pract. 2017;66(6):356–63.
Verberg MFG, Gillott DJ, Al-Fardan N, et al. Hyperemesis gravidarum, a literature review. Hum Reprod Update. 2005;11(5):527–39.
Dixon JB, Dixon ME, O’Brien PE. Elevated homocysteine levels with weight loss after Lap-Band surgery: higher folate and vitamin B12 levels required to maintain homocysteine level. Int J Obes Relat Metab Disord. 2001;25(2):219–27.
Hazart L, Le Guennec D, Accoceberry M, et al. Maternal nutritional deficiencies and small-for-gestational-age neonates at birth of women who have undergone bariatric surgery. J Pregnancy. 2017;2017:4168541.
Smid MC, Dotters-Katz SK, Mcelwain CA, et al. Pregnancy after bariatric surgery: national survey of obstetrician’s comfort, knowledge, and practice patterns. Obes Surg. 2017;27(9):2354–9.
Gadgil MD, Chang HY, Richards TM, et al. Laboratory testing for and diagnosis of nutritional deficiencies in pregnancy before and after bariatric surgery. J Women's Health (Larchmt). 2014;23(2):129–37.
Giridi M, Greer IA. Pregnancy after bariatric surgery: no problem? Obstet Med. 2009;2(1):11–6.
Moliterno JA, DiLuna ML, Sood S, et al. Gastric bypass: a risk factor for neural tube defects? J Neurosurg Pediatr. 2008;1(5):406–9.
Acknowledgments
The authors are greatly indebted to Mr. William Vitelli for English translation and revision.
Funding
This study was funded by Gastrocirurgia Clinic, Brasilia, Brazil.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare that they have no conflict of interest.
Ethical Approval Statement
All procedures performed in this study were in accordance with the ethical standards of the institutional research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed Consent Statement
Informed consent was obtained from all individual participants included in the study.
Rights and permissions
About this article

Cite this article
Faria, S.L., Faria, O.P., de Gouvêa, H.R. et al. Supplementation Adherence and Outcomes Among Pregnant Women After Bariatric Surgery. OBES SURG 29, 178–182 (2019). https://doi.org/10.1007/s11695-018-3499-y
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11695-018-3499-y