
Abstract
Introduction
Anatomical and functional influences on gastric bypass (GBP) results are often poorly evaluated and not yet fully understood.
Purpose
The purpose of this study is to evaluate the influence of the gastric pouch volume and its emptying rate on long-term weight loss and food tolerance after GBP.
Materials and Methods
Weight loss, food tolerance, pouch volumetry (V) by three-dimensional reconstruction, and pouch emptying rate by 4 h scintigraphy were evaluated in 67 patients. Cutoffs were identified for V and retention percentage (%Ret) at 1 h (%Ret1). From these parameters, the sample was categorized, looking for associations between V, %Ret, weight loss, and food tolerance, assessed by a questionnaire for quick assessment of food tolerance (SS).
Results
PO median follow-up time was 47 months; median V was 28 mL; %Ret at 1, 2, and 4 h were 8, 2, and 1%, respectively. There were associations between V ≤ 40 mL and higher emptying rates up to 2 h (V ≤ 40 mL: %Ret1 = 6, %Ret2 = 2, p = 0.009; V > 40 mL: %Ret1 = 44, %Ret2 = 13.5, p = 0.045). An association was found between higher emptying speed in 1 h and higher late weight loss (WL), represented by lower percentage of excess weight loss (%EWL) regain (p = 0.036) and higher %EWL (p = 0.033) in the group with %Ret1 ≤ 12%, compared to the group %Ret1 ≥ 25%. Better food tolerance (SS > 24), was associated with lower %Ret1 (p = 0.003).
Conclusion
Smaller pouch size is associated with a faster gastric emptying, greater WL maintenance, and better food tolerance. These data suggest that a small pouch with rapid emptying rate is an important technical parameter for good outcomes in GBP.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Roux-en-Y gastric bypass (GBP) is the most performed bariatric procedure worldwide and presents tens of technical variations [1]. Gastric pouch can vary widely in length and width, depending on the different techniques. This can generate reservoirs of different volumes and shapes, with putative functional repercussions still not fully understood [2,3,4].
Although, in the past, the restrictive surgery was a unanimous concept for the treatment of obesity, today, its use is more controversial. Due to new evidence of the metabolic effects in gastric bypass, the traditional relationship between contention from gastric emptying and weight loss seems paradoxical [5,6,7,8]. Anatomical effects of gastric pouch may be important due to morphofunctional modulation of entero-hormonal phenomena [9].
Anatomical evaluation is commonly done to analyze the possible causes of suboptimal results or weight regain [10]. Upper GI series and endoscopy are the most common investigational tools [11, 12]. However, even when performed in combination, these tests provide limited information about post-surgical anatomy. Therefore, the evidence of the real contribution of morphofunctional aspects in the results of GBP, as well as the interaction between them, remains unclear.
The use of helical computed tomography with three-dimensional reconstruction (3DCT) in bariatric surgery is relatively recent [13]. This method allows more detailed morphological analysis of the gastric pouch, and more precise volumetric study, and could be an important tool in the postoperative evaluation after GBP [14].
The study of gastric emptying may play a key role in GBP functional evaluation. One is able to determine pouch emptying delay and restriction, or fast emptying, which can be associated with a greater entero-hormonal stimulus. Scintigraphy is nowadays the gold standard test for evaluation of gastric emptying [15, 16].
A more detailed morphological and functional assessment of the GBP may lead to a better understanding of the interrelationships between the surgical anatomy, functional mechanisms, and surgical outcomes. To our knowledge, there is no study evaluating the volume and emptying of the gastric pouch with three-dimensional tomography and scintigraphy and late postoperative result parameters.
The objective of our study is to correlate gastric pouch volume and emptying rate with weight loss and food tolerance in late follow-up of patients submitted to GBP.
Materials and Methods
Patients with severe obesity over 18 years of age, followed-up for more than 18 months after GBP, were included. The standardized surgical technique was described elsewhere [17]. Exclusion criteria included patients with banded gastric bypass, gastrojejunal anastomosis stenosis, and gastro-gastric fistula (factors that could influence gastric emptying or pouch size measurement), as well pre-existing medical conditions and medication use with possible influence on weight loss.
Eighty patients were randomly selected and subjected to an initial assessment of weight loss, clinical evaluation, medical record review, consultation with nutritionist and psychologist, endoscopy, and upper GI series. Four patients were excluded: three with gastro-gastric fistula and one with substenosis of the gastrojejunostomy. No other exclusion criteria were found. Nine patients dropped out. Finally, 67 were included in the study.
Food tolerance was assessed by a questionnaire described by Suter et al. [18]. Patients were then submitted to 3DCT for evaluation of gastric pouch volume and scintigraphic pouch emptying time study. Weight loss data were assessed by percentage of excess weight loss (%EWL) considering initial weight, initial height, and ideal weight for BMI 25 kg/m2, using the formula IBW = 25 × (height)2.
3DCT and Pouch Volumetry Protocol
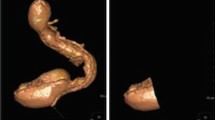
All CT scans were performed using the CT scanner Aquilion CXL 128-slice CT scanner (Toshiba Medical Systems Corporation, Otawara-shi, Japan). After 8 h fasting, patients received 400 mL of a 30% solution of iodinated contrast agent Ultravist 300 (Bayer Healthcare, Berlin, Germany) orally, to be taken at the maximum possible speed immediately before the positioning for acquiring images. The images obtained were used for the 3D reconstruction and multiplanar reformatting of the gastric pouch, calculating the pouch volume, in milliliter, through Vitrea® software (Vital Images, Minnetonka, USA) (Fig. 1).

3DCT volumetry: gastric pouch of small volume (V = 36 mL)
Scintigraphic Gastric Emptying Protocol
Gastric scintigraphy was performed in SPECT with two detectors Discovery NM 630 (GE Medical Systems Functional Imaging, Haifa, Israel). The test meal was marked by incorporation of 99 m Tc-colloid at a dose of 1 mCi or 37 MBq. The test meal consisted of two eggs added to a sandwich made with two slices of bread and 30 g of strawberry jam, and it should be taken up in the SPECT room with 120 mL of water at a maximum of 10 min. Immediately, after the time limit for the meal, the patient was positioned to start capturing images.
With the patient in the supine position, images of a minute long were obtained in times 0, 1, 2, and 4 h (T0, T1, T2, T4). Between the reading times, the patient remained in fasting and not in bed rest. Using the geometric mean of radioactive counts of anterior and posterior incidences corrected by decay (1 h/0.89, 2 h/0.79, 4 h/0.63), the percentage of gastric pouch retention relative to T0 in subsequent times was calculated, with the construction of the retention curve tracer through the Xeleris software (GE Medical Systems Functional Imaging, Haifa, Israel) (Fig. 2). Retention percentages (%Ret) represent the proportion of test meal that remained in the gastric pouch, as variables used were percentage retention at T1, T2, and T4 (%Ret1, %Ret2, and %Ret4, respectively).

Scintigraphy: gastric pouch with an initially slower emptying time. Images showing anterior and posterior incidences of the pouch in T0, T1, T2, T4 (%Ret1 = 51%; %Ret2 = 4%; %Ret4 = 2%)
Alimentary Tolerance
All patients were evaluated through a questionnaire for quick assessment of food tolerance after bariatric surgery [18].
Statistical Analysis
It consisted of categorizing the sample from cutting points; looking for statistically significant differences for different volumes of the gastric pouch through bivariate analysis, together with the pouch emptying rate, weight loss, and food tolerance; and looking for statistically significant differences for different gastric pouch emptying rates through bivariate analysis, together with the pouch volume, weight loss, and food tolerance. The cutoff points used in the categorization for volume in milliliters, and for emptying rate in %Ret1, considering the other variables, were initially obtained by bivariate analyzes by maximizing the difference between medians [19]. Quantitative variables were described by median (25% quantile–quantile 75%). The qualitative variables were described by percentage and frequency.
For quantitative variables, the comparison between two groups was performed using modified t test and Mann-Whitney. For qualitative variables, Fisher’s exact test was used to compare between groups. All calculations were performed using the R software version 3.1.2 (R Core Team, 2014 The R Foundation, Vienna, Austria). A p value < 0.05 was considered statistically significant.
Results
Eighty patients were enrolled in the protocol between May 2013 and April 2015. Four patients were excluded: three with gastro-gastric fistula and one with substenosis of the gastrojejunostomy. Other nine patients dropped out the protocol, so that, 67 were included in the study (91% female). The median age was 51 years (40.5–57 years). The initial median BMI was 51.4 kg/m2 (46.2–56.1 kg/m2), ranging from 38.5 to 88 kg/m2; 59.7% of patients had initially super obesity. The median follow-up time was 47 months (36–62.5). The median %EWL was 60.3% at the nadir, in median time of 14 months (10–18) postoperatively. After 47 months (36–62.5) postoperatively, the median %EWL was 47.8%, and the median percentage of weight regain from %EWL nadir was 16.1% (%EWL regain).
The average volume (V) of gastric pouches was 28 mL (15.5–43 mL). The median emptying rate of the gastric pouch from the retention percentage was 8% (2–42%) in 1 h, or 92% of the test meal had been emptied of the gastric pouch within the first hour. In 2 h, there was retention of 2% (1–8.5%); in 4 h, the sample showed a median retention of 1% (0–2.5%). The median score of the questionnaire of food tolerance was 21 points (17–23.5 points). The range of scores occurred between a minimum of 10 and maximum of 27 points, with 25.4% of the study group (17 patients) presenting scores ≥ 24.
Analysis of Gastric Pouch Categorized by Volume
The cutoff point for pouch volume obtained was 39.7 mL (p = 0.05). Patients were then divided into two groups: V ≤ 40 mL (n = 49; median pouch volume of 21 mL) and V > 40 mL (n = 18 median pouch volume of 56.5 mL). Both groups were homogeneous for age, sex, initial BMI and weight, and follow-up time (Table 1). The prevalence of super obesity was similar. There were no statistically significant differences in %EWL at the nadir or %EWL regain. For the gastric pouch emptying rate, there were statistically significant differences in %Ret in 1 h (p = 0.009) and 2 h (p = 0.045). There was an association between V ≤ 40 mL and faster emptying of the gastric pouch up to 2 h of scintigraphy (Table 2, Fig. 3). Nevertheless, there were no statistically significant differences in food tolerance scores from the categorization by the gastric pouch volume (Table 2).

Gastric pouch emptying time curves, scintigraphic %Ret in T1, T2, and T4. Comparison between two groups by pouch volume, V ≤ 40 mL and V > 40 mL. Pouches with V ≤ 40 mL showed statistically significant faster emptying rates at the first and second hour, but not at the fourth hour of the scintigraphy
Analysis of Gastric Pouch Categorized by Emptying Rate
Two cutoff points for pouch emptying time were observed: %Ret1 12% and 25% (p = 0.009). Based on that, study population was divided into three categories using the two cutoff points found: %Ret1 ≤ 12% (n = 35), 12% < %Ret1 < 25% (n = 10), and %Ret1 ≥ 25% (n = 22).
There were no significant differences in gender, age, initial BMI, follow-up time, and the presence of super obesity (Table 3). In the analysis of gastric emptying time for a complete scintigraphy of 4 h, there were statistically significant differences in retention percentages in T1, T2 and T4 between the three subgroups (p < 0.001). All three subgroups had similar %EWL at nadir. In the late follow-up, the subgroup with accelerated emptying (%Ret1 ≤ 12%) had less weight regain (%EWL regain) in relation to the subgroup with slower emptying (%Ret1 ≥ 25%) (p = 0.036). The group with faster gastric pouch emptying obtained a greater long-term weight loss compared to those with slower emptying. There was an association between the gastric pouch emptying rate in the first hour of scintigraphy (%Ret1) and food tolerance with higher scores relating with faster emptying times in the first hour. There was a significant difference (p = 0.007) between the subgroups with lower and higher emptying rates (%Ret1 ≤ 12% and %Ret1 ≥ 25%). There was an association between SS over 24 and smaller %Ret1. In the three subgroups, a progressively lower percentage of SS > 24 was observed as the %Ret1 increased (p = 0.03), also demonstrating a correlation of the better food tolerance with the faster emptying of the gastric pouch (Table 4, Fig. 4).

%EWL curves at preoperative time, nadir and actual time. Comparison between three groups by gastric pouch emptying rates, %Ret1 ≤ 12%, 12% < %Ret1 < 25, and %Ret1 ≥ 25%. After a similar %EWL at nadir, gastric pouches with faster emptying rate correlated statistically with greater maintenance of %EWL in late follow-up
Discussion
Weight regain is not negligible after GBP, and their causes are not yet well established [20,21,22]. Its common that the significant inflection of the weight loss curve, as well as surgical failure, is assigned to anatomical issues that could cause loss of restriction, such as pouch dilation or anastomosis enlargement, and consequent increase of the capacity of food consumption [23]. Nevertheless, the parameters of these associations are controversial [24, 25].
The results obtained here suggest that small volumes of the gastric pouch are correlated with an increased gastric emptying rate. On the other hand, the accelerated gastric pouch emptying correlated with higher maintenance of weight loss, as well as with better food tolerance in the late follow-up. The association between faster gastric pouch emptying, lower weight regain, and improved food tolerance is stronger when evaluating patients with very accelerated emptying rate, suggesting that the positive effects will be greater as faster the gastric pouch emptying. In this way, we could establish association between small volumes of gastric pouch, its rapid emptying, and better results in weight loss maintenance and food tolerance.
Postoperative morphofunctional aspects after GBP are in general poorly evaluated. Despite the questions about the influence of the method of volumetric evaluation used, the use of 3DCT scan seems to be an advance compared to the radiographic method normally used. CT scan allowed three-dimensional morphological evaluation of the gastric pouch, and greater accuracy for volume calculation. Our protocol also used fast oral contrast administration in an attempt to minimize the influence of gastric emptying rate in this evaluation.
The association of a functional evaluation through the assessment of gastric emptying was an important differential in our study. Patients with slow gastric emptying, either with small or large pouches, had similarities in reduced late weight loss as well as worse food tolerance. These findings suggest the importance of adequate pouch emptying to obtain the best surgical outcome after GBP. Moreover, smaller pouches showed better late results in weight loss, although with similar food tolerance when compared to larger pouches. These results suggest the importance of a small gastric reservoir volume for better outcomes in GBP. Of note, none of these subgroups diverged at follow-up time, which makes unlikely the significant influence of dietary behavior on dilation of initially small gastric pouches leading to larger pouches. It seems that the inverse relationship is more likely, with the initial volume and emptying of the gastric reservoir influencing eating behavior.
The quality of diet after GBP has an important role in the surgical outcomes, both in quality of life and in the incidence of nutritional complications, and in weight loss. The patient’s own perception of the quality of his feeding is subjective, and adaptive mechanisms, such as changes in diet patterns secondary to food intolerances, may be seen as appropriate as they try to avoid uncomfortable symptoms. The use of a specific tool, such as the questionnaire for quick assessment of food tolerance used in our study, greatly contributed to the identification and interpretation of the observed correlations between morphofunctional aspects of the gastric pouch and surgical outcomes.
Some aspects of the studied group drew our attention and deserve some consideration. The study population was predominantly female. This homogeneity could influence our findings, due to potential differences in food preferences between genders. The predominance of female gender is constant in bariatric surgery series [26, 27]. A comparative evaluation of the food pattern of men and women in patients undergoing GBP evidenced better food tolerance in the female population, with no difference in meat consumption neither in the vomiting frequency [28].
In the nadir of the weight loss curve, we found that the median %EWL was 60.4%, a result which is considered satisfactory. In long-term evaluations, with a median follow-up of 47 months, the average regain of %EWL was 16.1%, and late %EWL was 47.8%. The observed weight loss late results could be considered unsatisfactory if they were analyzed under the Reinhold criteria [29]. Despite of the random inclusion, there may have been sample influence on the observed weight loss. The fraction of patients with super obesity may have been one influence, as weight loss is also influenced by the initial BMI [30]. When we included only the patients with a BMI < 50 kg/m2, the mean current %EWL was 62.2%, and in the group with BMI > 50 kg/m2, the current %EWL was 46%. Nevertheless, a number of super obese patients have not represented a bias in pouch volume and emptying analysis, since BMI distribution in the categorized subgroups was similar.
The volumetry evaluation showed predominantly small gastric pouches. Analyzing the two subgroups, there was a predominance of gastric pouches of lower volume (73%) denoting surgeons’ concern to reach the small size of the reservoir historically widespread as ideal [3, 31,32,33,34]. Intraoperative situations related to gender, BMI, fat distribution, hiatal hernia, previous operations, hepatomegaly, or short mesentery may justify the construction of larger pouches. However, the volume of the gastric pouch was not correlated to initial weight, BMI, super obesity, or gender in our study. On the other hand, the very small pouches observed in our population may have been influenced by rapid emptying when the CT scan was obtained, underestimating their real volume.
The predominance of small pouches, with no difference in follow-up time in volume-stratified groups, suggests the improbability of significant gastric pouch dilatation due to hyperalimentation. In any case, the extremely small or too large pouches did not influence the interrelationships obtained, since the use of medians and quantiles instead of means and ranges in our statistics analysis excluded the discrepant values of the sample studied, avoiding the possible distortion for the presence of outliers.
The gastric pouch emptying rate study showed a predominantly fast emptying. Patients with slower emptying rates (> 25% of retention in the first hour) had more weight regain. This data contradicts the paradigm that associates higher restriction with weight loss maintenance, one of the historical mechanisms of action of gastric bypass. On the other hand, there were associations between larger pouches and slower emptying rates, and this combination could end with changes in food intake, or changes in quality of diet that could justify weight regain.
Furthermore, food intolerance was associated with greater weight regain. This correlation may seem paradoxical at first, but it is justified if we consider the follow-up time. There is a dichotomization of responses to the maintenance of food intolerance after the GBP. Severe intolerance can lead to a global decrease in food intake, or extreme adaptive eating behaviors secondary to the high frequency of vomiting and regurgitation, leading to acute protein-calorie malnutrition. This phenomenon usually occurs in the initial postoperative and demands intervention. It is not uncommon after more restrictive procedures, such as banded GBP, or in the presence of stomal stenosis [35, 36].
In the presence of moderate intolerance to high-protein food and high frequency of vomiting, patients adapt over time through dietary mechanisms, avoiding certain foods, or develops soft calorie syndrome, grazing, snacking, and other diet modifications that do not lead to macronutrient malnutrition, but insidiously can lead to food monotony based on sources of simple carbohydrates, and inversion of the protein-based food pyramid recommended after GBP, paradoxically leading to insufficient weight loss and weight regain [21, 37]. This adaptation mechanism could partially explain our findings.
The dumping syndrome evaluation in our study could provide information regarding its correlation with gastric emptying. Faster pouch emptying could lead to a higher incidence of dumping symptoms, contributing to a lower consumption of hypercaloric carbohydrates and low-consistency foods, thus associating the rapid pouch emptying to the greater maintenance of weight loss. From this point of view, it is of interest to interpret the best scenario: severe restriction leading to limitation of food intake, or rapid pouch emptying inducing dumping and thereby limiting the consumption of high-calorie foods. However, studies have shown no correlation between dumping and weight loss, nor do they associate the severity of dumping to better weight losses, despite the unfavorable condition for consumption of high-calorie foods and sweets [38].
Our findings of faster pouch emptying with better long-term weight loss bring up the controversy over the role of restriction in the GBP results, contrasting with lines of research involving restriction as a strategy for optimization of primary surgical treatment or an option for revisional procedures in weight regain [24, 39, 40]. Gastric bypass-induced entero-hormonal modulation [5, 7, 8] is currently considered the main mechanism of action of surgery and has been associated with increased post-surgical gastric emptying rate and speed of alimentary transit [9, 41]. Previously, our group has found associations between different entero-hormonal responses and distinct results in late maintenance of weight loss after GBP [42]. Based on these data, we could hypothetically attribute the diverse entero-hormonal effects to the diverse emptying of the gastric pouch.
We still do not fully understand all the interrelationships between the changes in the digestive anatomy generated by the GBP, and the metabolic mechanisms involved in the control of energetic homeostasis, hunger, and satiety. Further assessments on the associations between gastric pouch emptying, entero-hormonal responses, and long-term surgical outcomes are necessary to confirm our findings.
Conclusion
The results of this study suggest correlations between the volume of the gastric pouch and its emptying rate in the late follow-up of patients undergoing Roux-en-Y gastric bypass. Gastric pouches with volumes equal or smaller to 40 mL correlated with accelerated emptying up to 2 h after a meal.
There was also a correlation between the gastric pouch emptying and late maintenance of weight loss, as well as food tolerance. Patients with gastric pouch emptying in the first hour of more than 75% of the ingested food had greater late weight loss, lower weight regain, and better food tolerance.
References
Buchwald H, Buchwald JN. Evolution of operative procedures for the management of morbid obesity 1950–2000. Obes Surg. 2002;12:705–17.
Fobi MA, Fleming AW. Vertical banded gastroplasty vs gastric bypass in the treatment of obesity. J Natl Med Assoc. 1986;78(11):1091–8.
Wittgrove AC, Clark GW, Schubert K. Laparoscopic gastric bypass, Roux-en-Y: technique and results 75 patients with 3–30 month follow-up. Obes Surg. 1996;6:500–4.
Capella RF, Iannace VA, Capela JF. An analysis of gastric pouch anatomy in bariatric surgery. Obes Surg. 2008;18:782–90.
le Roux CW, Aylwin SJ, Batterham RL, et al. Gut hormones profiles following bariatric surgery favor an anoretic state, facilitate weight loss, and improve metabolic parameters. Ann Surg. 2006;243(1):108–14.
Näslund E, Kral JG. Impact of gastric bypass surgery on gut hormones and glucose homeostasis in type 2 diabetes. Diabetes. 2006;55(S2):S92–7.
Cummings DE, Overduin J. Gastrointestinal regulation of food intake. J Clin Invest. 2007;117(1):13–23.
Miras AD, le Roux CW. Mechanisms underlying weight loss after bariatric surgery. Nat Rev Gastroenterol Hepatol. 2013;10(10):575–84.
Dirksen C, Damgaard M, Bojsen-Møller KN, et al. Fast pouch emptying, delayed small intestinal transit, and exaggerated gut hormone responses after Roux-en-Y gastric bypass. Neurogastroenterol Motil. 2013;25(4):346–e255.
Karmali S, Balpreet B, Shi X, et al. Weight recidivism post-bariatric surgery: a systematic review. Obes Surg. 2013;23:1922–33.
Toppino M, Cesarini F, Comba A, et al. The role of early radiological studies after gastric bariatric surgery. Obes Surg. 2001;11:447–54.
Brethauer SA, Nfonsam V, Sherman V, et al. Endoscopy and upper gastrointestinal contrast studies are complimentary in evaluation of weight regain after bariatric surgery. Surg Obes Relat Dis. 2006;2(6):643–8.
Alva S, Eisenberg D, Duffy A, et al. A new modality to evaluate the gastric remnant after Roux-en-Y gastric bypass. Surg Obes Relat Dis. 2008;4:46–9.
Blanchet M, Mesmann C, Yanes M, et al. 3D gastric computed tomography as a new imaging in patients with failure or complication after bariatric surgery. Obes Surg. 2010;20:1727–33.
Flanagan L. Measurement of functional pouch volume following the gastric bypass procedure. Obes Surg. 1996;6(1):38–43.
Seok JW. How to interpret gastric emptying scintigraphy. J Neurogastroenterol Motil. 2011;17(2):189–91.
Santo MA, Riccioppo D, Pajecki D, et al. Preoperative weight loss in super-obese patients: study of the rate of weight loss and its effects on surgical morbidity. Clinics (Sao Paulo). 2014;69(12):828–34.
Suter M, Calmes J, Paroz A, et al. A new questionnaire for quick assessment of food tolerance after bariatric surgery. Obes Surg. 2007;17:2–8.
Hothorn T, Lausen B. On the exact distribution of maximally selected rank statistics. Computational Statistics & Data Analysis. 2003;43:121–37.
Magro DO, Geloneze B, Delfini D, et al. Long-term weight regain after gastric bypass: a 5-year prospective study. Obes Surg. 2008;18:648–51.
Faria SL, de Oliveira KE, Faria OP, et al. Snack-eating patients experience lesser weight loss after Roux-en-Y gastric bypass surgery. Obes Surg. 2009;19(9):1293–6.
Hsieh T, Zurita L, Grover H, et al. 10-year outcomes of the vertical transected gastric bypass for obesity: a systematic review. Obes Surg. 2014;24:456–61.
Mechanick JI, Kushner RF, Sugerman HJ, et al. American Association of Clinical Endocrinologists, The Obesity Society, and American Society for Metabolic and Bariatric Surgery medical guide lines for clinical practice for the perioperative nutritional, metabolic and nonsurgical support of the bariatric surgery patient. Surg Obes Relat Dis. 2008;4(5 Suppl):S109–84.
Heneghan HM, Annaberdyev S, Eldar S, et al. Banded Roux-en-Y gastric bypass for the treatment of morbid obesity. Surg Obes Relat Dis. 2014;10(2):210–6.
Ernst B, Thurnheer M, Wilms B, et al. Differential changes in dietary habits after gastric bypass versus gastric banding operations. Obes Surg. 2009;19(3):274–80.
Buchwald H, Avidor Y, Braunwald E, et al. Bariatric surgery: a systematic review and meta analysis. JAMA. 2004;292:1724–37.
Sjöström L. Review of the key results from the Swedish Obese Subjects (SOS) trial—a prospective controlled intervention study of bariatric surgery. J Int Med. 2013;273:219–34.
Valezi AC, Brito SJ, Mali Jr J, et al. Estudo do padrão alimentar tardio em obesos submetidos à derivação gástrica com bandagem em Y-de-Roux: comparação entre homens e mulheres [Late meal pattern in obese people after banded Roux-en-Y gastric bypass: comparison between male and female]. Rev Col Bras Cir. 2008;35(6):387–91.
Reinhold RB. Critical analysis of long-term weight loss following gastric bypass. Surg Gynecol Obstet. 1982;155:385–94.
Higa KD, Ho T, Boone KB. Laparoscopic Roux-en-Y gastric bypass: technique and 3-year follow-up. J Laparoendosc Adv Surg Tech A. 2001;11(6):377–82.
Madan AK, Tichansky DS, Phillips JC. Does pouch size matter? Obes Surg. 2007;17:317–20.
Campos GM, Rabl C, Mulligan K, et al. Factors associated with weight loss after gastric bypass. Arch Surg. 2008;143(9):877–84.
Patel S, Szomstein S, Rosenthal RJ. Reasons and outcomes of reoperative bariatric surgery for failed and complicated procedures (excluding adjustable gastric banding). Obes Surg. 2011;21:1209–19.
Topart P, Becouarn G, Ritz P. Pouch size after gastric bypass does not correlate with weight loss outcome. Obes Surg. 2011;21:1350–4.
Palermo M, Acquafresca PA, Rogula T, et al. Late surgical complications after gastric by-pass: a literature review. Arq Bras Cir Dig. 2015;28(2):139–43.
Rasera Jr I, Coelho TH, Ravelli MN, et al. A comparative, prospective and randomized evaluation of Roux-en-Y gastric bypass with and without the silastic ring: a 2-year follow up preliminary report on weight loss and quality of life. Obes Surg. 2016;26(4):762–8.
Colles SL, Dixon JB, O’Brien PE. Grazing and loss of control related to eating: two high-risk factors following bariatric surgery. Obesity (Silver Spring). 2008;16(3):615–22.
Mallory GN, Macgregor AM, Rand CS. The influence of dumping on weight loss after gastric restrictive surgery for morbid obesity. Obes Surg. 1996;6(6):474–8.
Dapri G, Cadière GB, Himpens J. Laparoscopic placement of non-adjustable silicone ring for weight regain after Roux-en-Y gastric bypass. Obes Surg. 2009;19:650–4.
Horgan S, Jacobsen G, Weiss GD, et al. Incisionless revision of post Roux-en-Y bypass stomal and pouch dilatation: multicenter registry results. Surg Obes Rel Dis. 2010;6:290–5.
Dirksen C, Jørgensen NB, Bojsen-Møller KN, et al. Gut hormones, early dumping and resting energy expenditure in patients with good and poor weight loss response after Roux-en-Y gastric bypass. Int J Obes. 2013;37(11):1452–9.
Santo MA, Riccioppo D, Pajecki D, et al. Weight regain after gastric bypass: influence of gut hormones. Obes Surg. 2016;26(5):919–25.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed consent was obtained from all individual participants included in the study.
Conflict of Interest
The authors declare that they have no conflict of interest.
Rights and permissions
About this article

Cite this article
Riccioppo, D., Santo, M.A., Rocha, M. et al. Small-Volume, Fast-Emptying Gastric Pouch Leads to Better Long-Term Weight Loss and Food Tolerance After Roux-en-Y Gastric Bypass. OBES SURG 28, 693–701 (2018). https://doi.org/10.1007/s11695-017-2922-0
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11695-017-2922-0