
Abstract
Summary
Population ageing presents significant challenges for many developed nations. Accurately forecasting the likely future burden of age-related medical conditions, such as hip fracture, is critical. In this study, we present estimates of the current and future burden of hip fracture in NSW, Australia, providing crucial information for future health care planning.
Purpose
The aims of this study were to investigate the burden of hip fracture in Australia’s largest state, New South Wales (NSW), and to build a prediction model to forecast the likely future burden of hip fracture from 2016 to 2036 in persons aged 50 years or more.
Methods
A retrospective population-based cohort study was conducted using NSW hospitalisation data. Standardised incident hip fracture rates and hip fracture-related acute care length of stay and costs were estimated. Predictive negative binomial regression modelling using age, gender and local health district and year covariates together with projected NSW populations was applied to forecast future hip fractures.
Results
Total incident hip fractures increased 8.8 % over a 12-year period from 2000/2001 to 2011/2012 despite declining age-standardised rates. Estimates of acute care length of stay for the treatment of hip fracture ranged from 10 to 15 days and acute care costs ranged between 21 and 29,000 Australian dollars per fracture. By 2036, incident hip fractures are projected to rise by 35.2 %, assuming a continued decline in the rate of hip fracture or by 107.5 % if the current decline in the rate does not continue. Acute care length of stay and costs are each predicted to rise between 37.1 and 110.4 % by 2036.
Conclusion
An ageing population and changing demographics will continue to drive the increasing burden of incident hip fractures in NSW and Australia in the foreseeable future. These anticipated changes provide important information for the planning and management of future hip fracture care.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
An osteoporotic hip fracture is a devastating event for an older person, associated with significant excess mortality, decreased ability to function independently and reduced quality of life [1–4]. In Australia, hip fracture is the most common low trauma osteoporotic fracture necessitating hospitalisation, accounting for over 40 % of incident fall-related fracture hospitalisations [5, 6]. Aside from the enormous human cost, hip fracture is associated with significant health care expenditure with estimates of acute care costs alone ranging from $2,000 to $20,000 Australian dollars ($AUD) per fracture [7]. Data from the USA show that hip fracture accounts for 72 % of the financial burden whilst only accounting for 14 % of all incident fractures [8].
In Australia, a nationwide study by the Australian Institute of Health and Welfare (AIHW) showed that the absolute number of incident hip fractures steadily increased over 10 years from 1997/1998 to 2006/2007 corresponding to an 11 % rise over the study period [7]. However, this percentage rise was well below the 36 % increase predicted by a forecast analysis of the population-based Geelong Osteoporosis Study over a similar timeframe (1996–2006) [9]. The difference in the observed and predicted increase is in part explained by the decreasing standardised rates of hip fracture seen in Australia. Whilst the reasons underpinning the observed decrease in the standardised rate of hip fracture are not fully understood, what is clear in Australia and many other developed countries is that population ageing will continue to increase the absolute number of older persons sustaining hip fractures into the foreseeable future [10–15]. Therefore, it is important that forecasts of the likely future burden of hip fracture are generated with the anticipation that the knowledge will be used to inform health policy, planning and practice.
The aim of this study was to utilise New South Wales (NSW) admitted patient hospital data, which provides complete state-wide coverage of incident hip fracture cases, to generate forecasts of the likely future burden of hip fracture in NSW in persons aged 50 years or above. This study explores the patterns of incident hip fractures in NSW, Australia’s most populous state, and derives estimates of hip fracture-related acute care length of stay and costs by age group and gender. Statistical modelling is used to generate a prediction model for incident hip fracture and is combined with projected changes in NSW populations to forecast the future burden of incident hip fractures in NSW, Australia, to inform policy and planning of future health care services.
Study population and statistical methods
Study design
This is a retrospective population-based cohort study.
Data sources
NSW is the largest state in Australia with an estimated residential population of 7.4 million in 2013. NSW accounts for approximately one third of the total Australian population and constitutes a large representative sample of the general population. Hospitalisation data used for the study was from the NSW admitted patient data collection (APDC). The APDC is a census of all inpatient hospital separations from public and private institutions in NSW, Australia. For the APDC, separations are classified as occurring when a patient is discharged, transferred to another hospital, assigned a new type of care (statistical discharge) or dies. Each APDC record contains multiple diagnosis fields that are coded according to the International Statistical Classification of Diseases and Related Health Problems, Tenth Revision, Australian Modification (ICD-10-AM) [16]. The study population comprised all NSW residents aged 50 years or more admitted to a hospital with a primary diagnosis of hip fracture (ICD-10-AM S72.0 to S72.2) over the period 1 July 2000 to 30 June 2012. The study population was restricted to incident cases by omitting transfers from other hospitals and by excluding statistical discharges. An estimate of the number of incident hospitalisations for NSW residents that occurred whilst they were interstate was obtained for the two most recent financial years (2010 and 2011) based on the average of the three previous years.
Demographic variables used in the study were obtained from the NSW APDC and included age (in 5-year age groups), gender, financial year and NSW Local Health District (LHD) to provide a measure of geographical area of residence. Age- and sex-specific estimated residential populations (ERPs) for the 15 NSW LHDs as on 31 December for the calendar years 2000 to 2012 were obtained from the NSW Ministry of Health. The ERPs were used to calculate age- and sex-standardised hospitalisation rates and to build a prediction model for forecasting future incident hip fracture hospitalisations. ERPs were based on Australian Bureau of Statistics (ABS) mid-year population estimates and derived from cubic spline interpolation. The NSW APDC and ERP datasets were accessed through the NSW Ministry of Health’s Secure Analytics for Population Health Research and Intelligence (SAPHaRI) system. NSW Local Government Area (LGA) age- and sex-specific projected populations for 2016 to 2036 were obtained from the NSW Department of Planning and Infrastructure [17]. The projected populations were available in 5-year intervals commencing with the year 2016. LGA-projected populations were mapped to LHDs within the SAPHaRI environment to generate LHD projected populations. Projected populations take into consideration the findings from the 2006 Australian census, published ABS ERPs for the period 2006–2009 and current information on fertility, migration and mortality [17].
Statistical and projection analysis
Direct age- and sex-standardised incident hip fracture hospitalisations were calculated using the NSW residential population as on 30 June 2001 as the reference population, according to the recommendations of the ABS and the AIHW [18]. For the building of a prediction model, Poisson regression was initially fitted to the data but model diagnostics indicated that incident hip fracture rates were over-dispersed. A negative binomial regression, which accommodates for increased variance in the outcome, was then used to model incident hip fracture hospitalisation rates with year, age group, gender, and LHD (for the modelling of area specific effects) as covariates. Two-way interaction terms for age group and year, and gender and year were tested but did not improve goodness of fit and were excluded from the final model. Natural logarithm-transformed ERPs for each age-sex-year-LHD strata group were included in the models as an offset variable. Estimated parameters for year, age group, gender and LHD were used in conjunction with projected populations to forecast incident hip fracture hospitalisations into the future. Two projection scenarios were used for the forecasting of hospitalisations by 5-year intervals from 2016 to 2036:
-
(1)
Demographic changes only
The estimated effects for gender, age group and LHD were applied to the projected changes in demographics to forecast the number of incident hip fracture hospitalisations into the future. This scenario does not take into account the recent observed decline in standardised incident hip fracture rates and effectively models the influence of projected changes in demographics. It assumes that incident hip fracture rates will continue at 2011 financial year levels into the future and provides a likely upper estimate of future hip fracture cases.
-
(2)
Demographic changes assuming a decline in hip fracture rates into the future
The recent observed decline in standardised hip fracture hospitalisation rates was included in the forecast model. All estimated parameters from the negative binomial model were used with projected population data to forecast incident hip fracture hospitalisations into the future. This projection scenario provides a likely lower boundary of future hip fracture cases.
The use of two projection scenarios provides a mechanism to cater for the uncertainty of potentially changing hip fracture rates into the future. It is possible that the current decline in hip fracture rates will continue into the near future. However, this decline will not continue indefinitely and at some stage will lessen or stabilise. When this change will occur is unknown, the two projection scenarios provide an interval that is more likely to capture the true future burden, helping accommodate the uncertainty associated with extrapolating hip fracture rates into the future.
For the estimation of mean acute care length of stay and costs, information was captured across all relevant hospital records by using the complete hospitalisation dataset including new (incident) admissions, transfers and changes in service type. This dataset is identical to the dataset used to estimate incident hip fracture cases (described above) but includes hospital transfer admissions and care-type change admissions. To minimise the potential influence of extreme outlier observations, hospital admissions with length of stay greater than 70 days (the 99th percentile) were trimmed to 70 days. Mean acute care length of stay was estimated by summing length of stay across APDC records by age group and gender, and then dividing the summed length of stay by the corresponding estimated number incident hip fractures. Acute care length of stay was projected into the future by multiplying age-group and gender-specific estimated mean acute care length of stay by projected incident hip fracture cases for the two projection scenarios.
To derive mean acute care costs, a measure of the standard cost of care in the form of cost weights for each APDC record with a primary diagnosis of hip fracture was generated. Episode of care costs was derived according to the New South Wales Cost of Care Standards 2009/2010 [19]. Standard costs of admitted acute care services were estimated from the 2006/2007 NSW Hospital Cost Data Collection (HCDC). The HCDC includes data from 83 hospitals throughout NSW and was used to estimate the average cost of treatment for each Australian Refined Diagnosis Related Group (AR-DRG). AR-DRGs represent a classification system used to group hospital admissions with similar clinical conditions into categories that reflect similar usage of hospital resources and services. An AR-DRG is assigned to each hospital admission and provides a basis for funding. To estimate costs, relative costs (cost weights) supplied in the Cost of Care Standards were assigned to each hospital admission by matching on AR-DRG. Adjustments to cost weights for transfers, in-hospital deaths and long lengths of stay were made as per the cost of care standards [19]. The cost for records with infrequent or missing AR-DRGs was obtained by applying the average inlier, outlier and transfer cost weights and average high trim point based on the 95.3 % of records covered by the top six AR-DRGs. Due to the changing pattern of AR-DRG usage for hip fracture over time, acute care costs were estimated over the 2-year period from 1 July 2010 to 30 June 2012, reflecting the most recent pattern of stable AR-DRG usage. Cost weights were summed across APDC records by age group and gender and then divided by the number of incident hip fractures to derive mean acute care cost weights. Due to small numbers, cost weights for the 50–54-year age group were estimated based on a combined group of males and females. Dollar costs ($AUD) were obtained by multiplying the cost weights by $4,280, the average dollar amount of a cost weight in 2009/2010 [19], and final costs were escalated to include Sydney, NSW health care sector rates of inflation [20] for the financial years 2010 to 2012 to reflect 2013 costs. We assumed that the average AR-DRG charges were reflective of the real costs of health care provision. Acute care costs were projected into the future using the same methodology applied to forecast acute care length of stay.
All data manipulations, statistical analyses and projection of incident hip fracture hospitalisations, acute care length of stay and acute care costs into the future were carried out in SAS Enterprise Guide, version 5.1 (SAS Institute, Inc., Cary, NC, USA). Tables were generated in Microsoft Excel and figures were created in R 2.15.1. Years are financial unless otherwise stated.
Results
Patterns of incident hip fracture in NSW
Over the 12-year period from 1 July 2000 to 30 June 2012, there were 71,566 incident hip fractures in persons aged 50 years or more in NSW, Australia. Unintentional falls were the primary external cause of injury for 65,957 (91.9 %) of the cases and females accounted for 72.2 % of incident hip fractures. Over the study period, 89.4 % of incident hip fractures occurred in those aged 70 years or greater and persons aged 85 years or more accounted for 43.7 %.
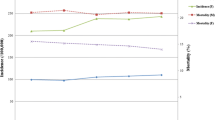
The number of annual incident hip fracture hospitalisations increased over the study period from 5,777 in 2000 to 6,287 in 2011, representing an 8.8 % rise. Despite the rise in the total number of incident hip fractures over time, standardised incident hip fracture rates for males and females declined over the time period (Table 1). For females, the standardised rate was 438.7 fractures per 100,000 in the year 2000 and declined to 342.9 fractures per 100,000 by 2011 (a change of −21.8 %). For males, the standardised rate was 162.2 per 100,000 in 2000 and decreased to 139.1 in 2011 (a change of −14.2 %).
When studied by 5-year age group, incident hip fracture rates declined significantly over the study period for all age groups aged 65 years or more, displaying mean annual percentage changes ranging from −0.8 to −2.4 %. Hip fracture rates were stable over the study period for the 50–54-, 55–59- and 60–64-year age groups. Standardised hip fracture rates were strongly correlated with age group and displayed an exponential rise with increasing age. The lowest rates were observed in those aged 50–54 years (e.g. 14.4 per 100,000 in 2011) and were greatest in those aged 85 years or more (e.g. 2078.9 per 100,000 in 2011).
Table 2 highlights the distribution of AR-DRGs assigned to incident hip fractures by age group over the period 1 July 2010 to 30 June 2012. Six major AR-DRGs were assigned to 95.3 % of all incident hip fracture cases with the remaining 4.7 % of patients distributed across less frequent AR-DRGs or missing an AR-DRG. The six major AR-DRGs related to procedures of the hip, femur or neck of femur. When AR-DRGs were analysed by age group, a changing pattern in the distribution of AR-DRGs was observed, whereby the proportion of AR-DRGs associated with comorbidities and complications increased with increasing age (Table 2 and Fig. 1a).

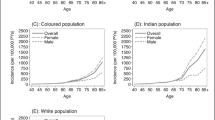
a Percentage of hip fracture-related AR-DRGs with and without complications by age group. b Mean acute care length of stay (hospital bed days) by gender and age group for the treatment of hip fracture. c Hip fracture-related mean acute care costs by gender and age group in Australian dollars ($AUD). d 2011 NSW estimated residential populations and 2036 projected populations by age group and gender. In b and c, dotted lines represent non-parametric LOESS smoothed curves
Mean acute care length of stay (acute bed days) and mean acute care costs were estimated by gender and age group (Fig. 1b, c). Mean acute care length of stay ranged from 10.5 to 15.0 days for males and from 10.6 to 13.8 days for females. Increasing age was associated with an increased length of stay, and this effect was seen in both males and females. Males had a higher acute care length of stay in all age groups with the exception of those aged 50–54 years. Acute care costs based on AR-DRG increased with age, ranging from AUD$20,980 per incident hip fracture in people aged 50–54 years to AUD$26,760 for females and AUD$28,270 for males aged 85+ years.
Projected changes in NSW populations by age group and gender
The NSW population as estimated on 30 June 2011 was 7,357,300 with 2,369,800 (32.2 %), aged 50 years or greater. By 2036, it is expected that the total NSW population will increase by 29.4 % to 9,521,400 persons and 3,626,900 (38.1 %) will be aged 50 years or more. Over this 25-year period, the population growth experienced in those aged 50 years or older is projected to be 53.0 %. The breakdown of the projected populations by gender and age group in persons aged 50 years or more was examined from 2016 to 2036 in 5-year intervals (Online Resource 1 and Fig. 1d).
Projection of incident hip fractures and related acute care length of stay and costs in NSW
A negative binomial prediction model for incident hip fracture was generated and used in conjunction with projected changes in demographics to estimate the future burden of incident hip fractures in NSW over the period 2016 to 2036 (Table 3). Incident hip fracture predictions were combined with age- and gender-specific estimates of acute care length of stay and acute care costs to obtain projections for these outcomes. Two scenarios were used to forecast incident hip fractures into the future. Projections were plotted against year by gender and age group (Fig. 2 and Online Resource 2). Demographic changes alone are expected to drive an increase in the absolute number of incident hip fractures into the future. Even in the best case scenario where fracture rates are assumed to continue declining into the future, incident hip fractures are projected to rise by 14.3 % in 2026 and by 35.2 % in 2036, representing absolute incident hip fractures of 7,188 and 8,498, respectively. If the current decline in fracture rate does not continue, then incident hip fractures are projected to increase by 46.8 % in 2026 and by 107.5 % in 2036 equating to 9,228 and 13,043 absolute hip fractures, respectively. The largest increases in the number of incident hip fractures are projected to occur in the older age groups. By 2026, 90 % of all incident hip fractures are projected to occur in persons aged 70 or more and this number is set to rise to 93 % by 2036. The proportion of hip fractures accounted for by women is projected to decline slightly from 71 % in 2011 to 68.5 % by 2026 and to 68 % by 2036.

Observed (2000 to 2011) and projected (2016 to 2036) incident hip fracture hospitalisations by gender and age group for two projection scenarios. Solid lines represent the assumption that incident hip fracture rates will continue to decline into the future and dashed lines assume that incident hip fracture rates remain at 2011 levels into the future
Based on current estimates of acute care costs and acute care length of stay, and assuming a continued decline in the rate of hip fracture, total acute bed days are projected to rise from 85,884 in 2011 to 98,915 (15.2 % increase) by 2026 and to 117,729 (37.1 %) by 2036 (Fig. 3a and Online Resource 3). In the absence of a further decline in the rate of hip fracture, total acute bed days are projected to increase to 126,996 (47.9 %) by 2026 and to 180,689 by 2036 (110.4 %, Fig. 3a and Online Resource 3). Using both scenarios, acute care costs are projected to rise from AUD$163.9 million in 2011 to between AUD$188.9 and AUD$242.5 million in 2026 and to between AUD$224.8 and AUD$345.0 million in 2036 (Fig. 3b and Online Resource 4).

a Projected incident hip fracture acute care length of stay (bed days) and b projected incident hip fracture acute care costs ($AUD). a, b are presented by gender and age group for two projection scenarios assuming that incident hip fracture rates continue to decline (solid lines) or remain at 2011 levels (dashed lines) into the future
Discussion
This study provides clear evidence of the substantial impact that incident hip fracture continues to have on our health systems despite the observed decrease in rates over time. A fall is the dominant precipitant of the fracture event which in turn is more common in females and in the older old, both factors associated with an increased likelihood of osteoporosis [21, 22]. Our findings are consistent with a number of other Australian and international studies which have shown that age-standardised hip fracture rates for both males and females have declined over recent years [5, 7, 15, 23–28]. A number of hypotheses have been proposed to explain the observed decline, the two most common of which relate to use of pharmacological agents for osteoporosis and implementation of effective falls prevention strategies. A recent report from NSW, Australia [29] shows that whilst hip fracture-related hospitalisation is decreasing, the overall rate of fall-related hospitalisation continues to increase by 3.8 % per annum and does not support the argument of effective implementation of falls prevention strategies. Equally, the report challenges the argument that the decline is related to successful treatment of osteoporosis as the rate of fall-related fracture hospitalisations continues to increase at 0.5 % per annum. As an example, the standardised rate of low trauma leg, ankle and foot fractures has risen by 1.3 % per year between 1998/1999 and 2011/2012 [29]. What the report also highlights is the disproportionate increase in non-fracture fall-related hospitalisations (5.9 % per annum), which is being driven by the oldest old (6.9 % per annum).
Other potential hypotheses include the “healthy cohort effect” [27] and the “healthy migrant effect” [30]. The healthy cohort effect is the phenomenon of general improved health of later birth cohorts, which can lead to consistent declines in incident hip fracture rates in successive generations [27]. The healthy migrant effect reflects the fact that people immigrating to Australia are selected on numerous factors including health and are likely to have equal or better health than the general Australian population [30]. A recently published paper provides some evidence that overweight and obesity may confer a protective effect on fracture risk [31]. This is not through a decreased falls risk, as the data shows an increased risk of falls, but could reflect better bone stock from increased loading [32] or the protective effects of adipose tissue as an energy absorber at the time of a fall event [33].
We also investigated the burden of hip fracture in NSW by estimating hip fracture-related acute care length of stay and costs. Acute care length of stay and associated acute care costs increased with age and were generally higher in men. This is likely to reflect a combination of increasing comorbidity and complications with age and the fact that these people are often slower to recover after major surgery compared to a younger hip fracture patient. This is relevant to future cost projections given the changing demography and the increasing number of the older old population. Our estimates place acute care costs for the treatment of hip fracture between AUD$20,000 and AUD$30,000 per fracture, totalling $165 million in 2011/2012. Also of note is that the estimate of cost only represents the financial burden attributable to acute care, and costs related to hip fracture following acute treatment including rehabilitation in the hospital or at home, and long-term care and support either in the community or in residential aged care facilities are often not factored into the calculation of the true societal impact of hip fracture [34, 35]. It is clear that in many countries, incident hip fractures remain a significant health and financial burden despite recently declining fracture rates. Increases in the absolute number of hip fractures over time reflect the impact of rising populations and increasing age in driving an increased burden.
To gain an understanding of future health care demand and burden, we used statistical modelling to predict the number of incident hip fractures into the future. We implemented two projection scenarios providing upper and lower prediction limits representing what are likely to be the best and worst case scenarios for future demand. By 2036, the number of incident cases is predicted to range between 8,498 and 13,043 with the lower limit representing a 35 % increase in number of hip fractures relative to 2011 and the upper limit reflecting an increase of more than 100 % relative to 2011. These results are comparable to the 100 % increase in incident hip fracture cases projected to occur in Ireland over a similar time period based entirely on demographic changes [11]. Likewise, recent projection studies have predicted substantial rises in the number of incident hip fracture cases in other countries, such as a potential doubling of cases in England over the 25-year period (2008–2033) [27], a similar doubling in the annual number of cases in Sweden between 2002 and 2050, and a greater than 20 % rise over the 10-year period from 2010 to 2020 in Italy [13–15]. Significantly, even when declining annual hip fracture rates are extrapolated into the future, the annual number of hip fractures is still projected to increase by 12 % from 2010 to 2030 in the USA and by 22 % in Norway between 2008 and 2040 [12, 36]. Furthermore, the estimated mean annual percentage changes in hip fracture rates required to counteract the effects of population ageing in Norway, the UK, Germany, France and the USA ranged between −1.1 and −2.2 %, and highlights the strength of the projected growth in elderly populations in driving increased hip fracture burden into the future [12]. Our analysis also shows that the burden of hip fractures is likely to shift slightly from females to males reflecting the fact that males are projected to experience larger population growth in the older age groups. In the absence of new innovations and approaches to care, population ageing alone will lead to a disproportionate increase in both length of acute stay and cost of acute care. Whilst NSW is just one state in Australia, it is the most populated and is considered representative of Australia more generally. These projections are relevant beyond NSW.
A previous Australian fracture projection study by Saunders et al. [9] overestimated the future burden of hip fracture in Australia by a substantial margin and reflects the difficulty in generating accurate forecasts in the face of changing hip fracture trends. We have attempted to address this uncertainty by utilising two projection scenarios which take into consideration the current decline in hip fracture rates whilst also generating forecasts based on rates remaining at current levels. The two scenarios create an interval that expands into the future, reflecting increased uncertainty of longer-term projections and which is more likely to contain the true future burden. Our population-based study also benefitted from a considerably larger sample compared to Saunders et al. (all of NSW versus Barwon Statistical Division), leading to more precise estimation of age- and sex-specific hip fracture rates for use in projections.
The main limitation of the study is the absence of information validating the coverage and accuracy of hip fracture data in the APDC. However, the validity of administrative data to identify hip fracture in several other countries has been shown to be high and supports the use of administrative data to reliably enumerate hip fractures [37]. The forecasting of hip fractures into the future is also reliant on several other critical assumptions. The projected populations used in the study were forecasts themselves and, as such, were likely to contain uncertainty that would be transferred to the forecasts. Any changes to the estimates used to calculate projected populations including base populations, birth rates, mortality rates, immigration and emigration, could impact hip fracture projections. A further limitation is the uncertainty of extrapolating current standardised hip fracture rate trends into the future. We have attempted to capture some of this uncertainty by utilising two projection scenarios based on declining and stable hip fracture rates to create projection intervals. However, uncertainty in the extrapolation scenarios remains.
Our work suggests that the future burden of hip fracture in NSW and Australia is likely to be substantial. The challenge remains as to how to best alter this trend in hip fracture-related hospitalisation in Australia and beyond. There is a wealth of evidence to support the benefits of treating osteoporosis [38–42], yet our approach to care in this area is still fragmented and not systematised, with many people not offered treatments from which they stand to benefit [40]. Evidence also exists to highlight the potential effects of high quality models of care that proactively address secondary fracture prevention and where fracture rates at a population level have been reduced through a systematised approach to care [43]. Equally important is the need to ensure that falls prevention strategies are applied. A robust evidence base exists to support a number of different approaches to falls prevention and it is the ability to implement the evidence where gaps still exist [44, 45].
There is also much that can be done at a population and health promotion level to reduce falls and fractures through nutrition, maintenance of a healthy weight, exercise, smoking cessation, alcohol minimisation and sensible sunlight exposure. These interventions need to span the life cycle and have the potential to deliver a number of positive health outcomes including falls and fracture prevention in older age [40]. Only when we see all these elements coming together are we likely to see a significant change in the number of people being admitted to hospital every day with what is a devastating injury for the person and a costly one both to the health system and society more generally.
In conclusion, we applied statistical modelling to forecast the likely future burden of hip fracture in NSW, Australia, using projected changes in demographics and trending hip fracture information. The results show that the future burden of hip fracture is likely to be significant, even with a continuing decline in hip fracture rates. It highlights the need for implementation of known effective strategies to reduce falls and prevent and treat osteoporosis. It also provides vital information for health care administrations to adequately plan services to meet the future needs of the ageing NSW and Australian population.
References
Abrahamsen B, van Staa T, Ariely R, Olson M, Cooper C (2009) Excess mortality following hip fracture: a systematic epidemiological review. Osteoporos Int 20:1633–1650
Bertram M, Norman R, Kemp L, Vos T (2011) Review of the long-term disability associated with hip fractures. Inj Prev 17:365–370
Hindmarsh DM, Hayen A, Finch CF, Close JC (2009) Relative survival after hospitalisation for hip fracture in older people in New South Wales, Australia. Osteoporos Int 20:221–229
Vochteloo AJ, Moerman S, Tuinebreijer WE, Maier AB, de Vries MR, Bloem RM, Nelissen RG, Pilot P (2013) More than half of hip fracture patients do not regain mobility in the first postoperative year. Geriatr Gerontol Int 13:334–341
Cassell E, Clapperton A (2013) A decreasing trend in fall-related hip fracture incidence in Victoria, Australia. Osteoporos Int 24:99–109
Australian Institute of Health and Welfare (2011) A snapshot of osteoporosis in Australia 2011, vol 15, PHE 137th edn, Arthritis. AIHW, Canberra
Australian Institute of Health and Welfare (2010) The problem of osteoporotic hip fracture in Australia, vol 76, AUS 121st edn, Bulletin. AIHW, Canberra
Burge R, Dawson-Hughes B, Solomon DH, Wong JB, King A, Tosteson A (2007) Incidence and economic burden of osteoporosis-related fractures in the United States, 2005–2025. J Bone Miner Res 22:465–475
Sanders KM, Nicholson GC, Ugoni AM, Pasco JA, Seeman E, Kotowicz MA (1999) Health burden of hip and other fractures in Australia beyond 2000. Projections based on the Geelong Osteoporosis Study. Med J Aust 170:467–470
Australian Bureau of Statistics (2013) Population Projections, Australia, 2012 (base) to 2101, Nov 2013. ABS Catalogue no. 3222.0
Dodds MK, Codd MB, Looney A, Mulhall KJ (2009) Incidence of hip fracture in the Republic of Ireland and future projections: a population-based study. Osteoporos Int 20:2105–2110
Omsland TK, Magnus JH (2014) Forecasting the burden of future postmenopausal hip fractures. Osteoporos Int 25:2493–2496
Piscitelli P, Brandi M, Cawston H, Gauthier A, Kanis JA, Compston J, Borgstrom F, Cooper C, McCloskey E (2014) Epidemiological burden of postmenopausal osteoporosis in Italy from 2010 to 2020: estimations from a disease model. Calcif Tissue Int
Rosengren BE, Karlsson MK (2014) The annual number of hip fractures in Sweden will double from year 2002 to 2050. Acta Orthop 85:234–237
White SM, Griffiths R (2011) Projected incidence of proximal femoral fracture in England: a report from the NHS Hip fracture anaesthesia network (HIPFAN). Injury 42:1230–1233
National Centre for Classification in Health (NCCH) (2008) The international statistical classification of diseases and related health problems, tenth revision, Australian modification (ICD-10-AM), 6th edn. NCCH, Faculty of Health Sciences, The University of Sydney, Sydney
NSW Department of Planning and Infractructure (2013) NSW State & Regional Population Projections—2010 interim release. NSW, Australia
Australian Bureau of Statistics (2013) Australian demographic statistics, Mar 2013. ABS Catalogue no. 3101.0
NSW Department of Health (2011) NSW costs of care standards 2009/10. NSW Department of Health, Sydney, p 2011
Australian Bureau of Statistics (2013) Consumer Price Index, Australia, Sep 2013. ABS Catalogue no. 6401.0. Table 5, Canberra
Kanis JA, Burlet N, Cooper C, Delmas PD, Reginster JY, Borgstrom F, Rizzoli R (2008) European guidance for the diagnosis and management of osteoporosis in postmenopausal women. Osteoporos Int 19:399–428
Mitchell RJ, Watson WL, Milat A, Chung AZ, Lord S (2013) Health and lifestyle risk factors for falls in a large population-based sample of older people in Australia. J Saf Res 45:7–13
Watson WL, Mitchell R (2011) Conflicting trends in fall-related injury hospitalisations among older people: variations by injury type. Osteoporos Int 22:2623–2631
Brauer CA, Coca-Perraillon M, Cutler DM, Rosen AB (2009) Incidence and mortality of hip fractures in the United States. JAMA 302:1573–1579
Holt G, Smith R, Duncan K, Hutchison JD, Reid D (2009) Changes in population demographics and the future incidence of hip fracture. Injury 40:722–726
Kannus P, Niemi S, Parkkari J, Palvanen M, Vuori I, Jarvinen M (2006) Nationwide decline in incidence of hip fracture. J Bone Miner Res 21:1836–1838
Langley J, Samaranayaka A, Davie G, Campbell AJ (2011) Age, cohort and period effects on hip fracture incidence: analysis and predictions from New Zealand data 1974–2007. Osteoporos Int 22:105–111
Nymark T, Lauritsen JM, Ovesen O, Rock ND, Jeune B (2006) Decreasing incidence of hip fracture in the Funen County, Denmark. Acta Orthop 77:109–113
Harvey LA, Close JCT (2013) Trends in fall-related hospitalisations, persons aged 65 years and over, NSW, 1998–99 to 2011–12. Falls and Injury Prevention Group, Neuroscience Research Australia, Sydney
Australian Institute of Health and Welfare (2012) Australia’s health 2012. Australia’s health series no.13. Cat. no. AUS 156. Canberra: AIHW
Mitchell RJ, Lord SR, Harvey LA, Close JC (2014) Associations between obesity and overweight and fall risk, health status and quality of life in older people. Aust N Z J Public Health 38:13–18
Dimitri P, Bishop N, Walsh JS, Eastell R (2012) Obesity is a risk factor for fracture in children but is protective against fracture in adults: a paradox. Bone 50:457–466
Yang S, Nguyen ND, Center JR, Eisman JA, Nguyen TV (2013) Association between abdominal obesity and fracture risk: a prospective study. J Clin Endocrinol Metab 98:2478–2483
Bleibler F, Konnopka A, Benzinger P, Rapp K, Konig HH (2013) The health burden and costs of incident fractures attributable to osteoporosis from 2010 to 2050 in Germany—a demographic simulation model. Osteoporos Int 24:835–847
Nikitovic M, Wodchis WP, Krahn MD, Cadarette SM (2013) Direct health-care costs attributed to hip fractures among seniors: a matched cohort study. Osteoporos Int 24:659–669
Stevens JA, Rudd RA (2013) The impact of decreasing U.S. hip fracture rates on future hip fracture estimates. Osteoporos Int 24:2725–2728
Hudson M, Avina-Zubieta A, Lacaille D, Bernatsky S, Lix L, Jean S (2013) The validity of administrative data to identify hip fractures is high—a systematic review. J Clin Epidemiol 66:278–285
Bischoff-Ferrari HA, Willett WC, Wong JB, Stuck AE, Staehelin HB, Orav EJ, Thoma A, Kiel DP, Henschkowski J (2009) Prevention of nonvertebral fractures with oral vitamin D and dose dependency: a meta-analysis of randomized controlled trials. Arch Intern Med 169:551–561
Cummings SR, San Martin J, McClung MR et al (2009) Denosumab for prevention of fractures in postmenopausal women with osteoporosis. N Engl J Med 361:756–765
Ebeling PR, Daly RM, Kerr DA, Kimlin MG (2013) Building healthy bones throughout life: an evidence-informed strategy to prevent osteoporosis in Australia. Med J Aust Open Suppl 1(2):1–46
Lyles KW, Colon-Emeric CS, Magaziner JS et al (2007) Zoledronic acid and clinical fractures and mortality after hip fracture. N Engl J Med 357:1799–1809
Shea B, Wells G, Cranney A et al (2002) Meta-analyses of therapies for postmenopausal osteoporosis. VII. Meta-analysis of calcium supplementation for the prevention of postmenopausal osteoporosis. Endocr Rev 23:552–559
McLellan AR, Wolowacz SE, Zimovetz EA, Beard SM, Lock S, McCrink L, Adekunle F, Roberts D (2011) Fracture liaison services for the evaluation and management of patients with osteoporotic fracture: a cost-effectiveness evaluation based on data collected over 8 years of service provision. Osteoporos Int 22:2083–2098
Cameron ID, Gillespie LD, Robertson MC, Murray GR, Hill KD, Cumming RG, Kerse N (2012) Interventions for preventing falls in older people in care facilities and hospitals. Cochrane Database Syst Rev 12, CD005465
Gillespie LD, Robertson MC, Gillespie WJ, Sherrington C, Gates S, Clemson LM, Lamb SE (2012) Interventions for preventing falls in older people living in the community. Cochrane Database Syst Rev 9, CD007146
Acknowledgments
Alexandre Stephens was supported by the NSW Ministry of Health Biostatistical Officer Training Program. The authors would like to thank the Centre for Epidemiology and Evidence, NSW Ministry of Health, for the provision of access to the population health data used in the study. The authors would like to thank Dr Katie Powell for critically reviewing the manuscript.
Conflicts of interest
None.
Author information
Authors and Affiliations
Corresponding author
Electronic supplementary material
Below is the link to the electronic supplementary material.
ESM 1
(DOCX 37 kb)
Rights and permissions
About this article

Cite this article
Stephens, A.S., Toson, B. & Close, J.C.T. Current and future burden of incident hip fractures in New South Wales, Australia. Arch Osteoporos 9, 200 (2014). https://doi.org/10.1007/s11657-014-0200-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s11657-014-0200-5