
Abstract
A new organ-based tube current modulation (NOB-TCM) method was designed with the intent to decrease tube current by 30% over a prescribed 90° radial arc across the anterior aspect of the radiosensitive organ, without increasing tube current in the remaining radial arc. We compared a reference scan and five other dose-reducing methods with regard to effects on dose, practicality, and image quality to determine the most effective method for the reduction of the radiation dose to the eyes during CT examinations of the head. We compared the radiation doses to the eyes and physical image quality in different regions of interest for TCM and shielding scans. Three types of TCM scans were performed: longitudinal TCM, angular TCM, and NOB-TCM. A bismuth sheet and lead goggles were each applied for the shielding scan. Relative to the reference scan, the dose to the eye was reduced to 25.88% with NOB-TCM, 44.53% with lead goggles, and 36.91% with a bismuth shield. Relative to the reference scan, the mean signal-to-noise ratio (SNR) was decreased to 8.02% with NOB-TCM, 28.36% with lead goggles, and 32.95% with the bismuth shield. The SNR of the anterior region of interest was decreased to 11.89% with NOB-TCM and 87.89% with the bismuth shield. The average figure of merit was increased by 11.7% with longitudinal TCM and 13.39% with NOB-TCM, compared with the reference scan. NOB-TCM is a superior solution for head CT, including the orbital area, due to the reduction in radiation exposure without significant loss in image quality.
Similar content being viewed by others
Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Since its public introduction in the early 1970s, computed tomography (CT) has revolutionized not only diagnostic radiology, but also the overall field of medicine. Compared to regular radiographs, head CT scans provide more detailed information about head injuries, strokes, brain tumors, and other brain diseases. CT manufacturers have contributed dose reduction technologies while maintaining image quality such as automatic exposure control and iterative reconstruction algorithms. Iterative reconstruction can allow radiation dose reduction for head and neck. But this algorithm cannot be applied for specific organ dose reduction. Head CT dose optimization is important because of the direct exposure to radiosensitive organs. The eyes, which are radiosensitive organ, are included in the area exposed to radiation during CT scans of the head. In particular, the eye lenses are at risk of radiation exposure when the head and sinuses are scanned, and the radiation effect is thought to represent a deterministic model. During head CT scans, the eyes are exposed to an approximate dose of 50 mGy [1–3]. Recently introduced multi-detector CT (MDCT) systems provide better image quality and better resolution compared to spiral CT; however, these systems also cause increased radiation exposure during CT procedures [4]. According to the International Commission on Radiological Protection (ICRP) Publication 103, the tissue weighting factors for the breast and thyroid are 0.12 and 0.04, respectively. The International Commission on Radiological Protection recommended that the equivalent dose limit for the lens of the eye be decreased from 150 to 20 mSv/y averaged over 5 years [5]. The eye lens is also considered an organ-at-risk during exposure to lower-dose radiation, especially because of the potential for cataract induction.
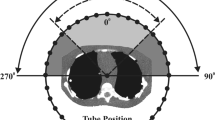
The use of a heavy metal in-plane shield protects sensitive organs such as the breast, thyroid, and eye lens [6]. Bismuth shielding is a commercially available option for superficial radiosensitive organ protection [7]. These techniques are mainly used to shield the breast, thyroid, and eye lens during CT to protect the organs at risk from direct exposure. However, bismuth shields are associated with potential image quality issues due to increased image noise over the covered area. Image noise from bismuth shield in head CT examinations will reduces the diagnostic value of images. Therefore, CT manufacturers have developed dose reduction techniques that do not reduce image quality. Tube-current modulation (TCM) techniques automatically adjust the tube current in the xy-plane (angular modulation), along the craniocaudal axis (z-axis modulation), or both, according to the attenuation of the patient and the X-ray beam direction [8]. In organ-based tube current modulation (OB-TCM) techniques, the X-ray tube current is reduced in real-time when the X-ray beam is directed toward the breasts or other dose-sensitive organs such as the thyroid gland and eye lens. However, the first commercially available OB-TCM was implemented during MDCT to reduce the dose to radiosensitive organs through a 30% decrease in the tube current over a prescribed 90º radial arc across the anterior aspect of the patient, while increasing the tube current in the remaining radial arc. Thus, the patient dose was relatively increased when the patient was shifted downward in the gantry. New organ-based tube current modulation (NOB-TCM) was designed and developed with the intent to decrease the tube current by 30% over a prescribed 90º radial arc across the anterior aspect of the radiosensitive organ without increasing the tube current in the remaining radial arc [9].
In this study, we compared the feasibility of NOB-TCM with other dose reduction methods in terms of its effectiveness for dose reduction to the eye and for image quality during head CT. We used a bismuth shielding material and lead glasses as the in-plane shielding technique. Other dose reduction techniques involved two types of TCMs (longitudinal TCM and angular TCM).
Methods
Scanning technique
This study was performed using a 64 MDCT scanner (Optima660; GE Healthcare, Milwaukee, WI, USA). An anthropomorphic head phantom (PBU-60; Kyoto Kagaku, Kyoto, Japan), CT dose index (CTDI) head phantom (16-cm diameter) and a GE performance phantom were scanned using routine adult head CT protocols (Table 1). Scan protocol was used in all in-plane shielding methods and TCM techniques.
Three types of TCMs were implemented using commercial options, which are as follows: 1, longitudinal TCM (Auto mA); 2, angular TCM (Smart scan); and 3, NOB-TCM (Smart mA). A bismuth sheet and lead goggles were applied for an in-plane shield scan (Table 2). To further compare radiation exposure, additional reference scans that excluded scans of the eyeball region but included CT gantry angle adjustments were performed. The general rotation during a CT scan that includes the eyeball region was 72.3 ± 7.1°. Shielding materials were placed on the eyes after acquiring a topogram.
To evaluate the radiation, the CTDI volume (CTDIvol) and dose length product (DLP) were calculated based on a scan of the 20-mm central region of the CTDI head phantom. A multimeter (mult-O-Meter, Model 601; Unfors Instrument, Billdal, Sweden) was used at the phantom hole for radiation dose measurement (Fig. 1). To measure the radiation dose to the eyes on the anthropomorphic head phantom, 10-mm × 10-mm optically stimulated luminescence dosimeters (nanoDot, Landauer Inc., Glenwood, IL, USA) with ± 5% repeatability and a radiation dosimeter from the same manufacturer (microStar InLight System, Landauer Inc.) were used.

a The bismuth shield and lead glasses used in this study. b The computed tomography (CT) dose index head phantom, ionization chamber, and multimeter used in this study. c The three regions of interest of GE performance phantom used to measure image noise and CT numbers
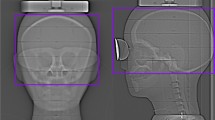
The energy revision coefficient (k) was 1.12 at 120 kV for each component. An optically stimulated luminescent dosimeter was located on the center of the eyeball before each scan. If radiation reduction techniques were used, the eyeball and dosimeter were fully shaded by shielding materials (Fig. 2).

a Nanodot dosimeters are placed on the surfaces of the eye lenses of the anthropomorphic head phantom. b A bismuth shield is placed over the eyes of the anthropomorphic head phantom
We evaluated the quantitative image quality by measuring the CT number, noise, SNR, and figure of merit (FOM) at the GE performance phantom images. FOM was defined by the following equation that included the SNR and exposure dose (X inc):
A higher FOM value results in better image quality capability in terms of SNR at a lower exposure. Using Image J software (1.46r; National Institutes of Health, Bethesda, MD, USA), pixel values were acquired based on a ROI size of 100 pixels around the centers of three holes (anterior hole, mid-central hole, posterior hole) located inside the GE performance phantom (Fig. 3). SNR was defined by the following equation as the ratio of the power of a signal (meaningful information) and the power of background noise (unwanted signal). CT number of ROI was signal and standard deviations of ROI was background noise.

Images of the GE performance phantom obtained using different scanning techniques. a New organ-based tube current modulation image of the phantom. b Phantom image obtained with a bismuth shield. c Phantom image obtained with lead glasses
Results
Compared with the reference scan, the doses to the eye were reduced to 25.88% with NOB-TCM, 44.53% with lead goggles, and 36.91% with the bismuth shield (Table 3). Table 4 presents the CTDIvol and DLP at the CTDI head phantom using different TCM techniques. The CTDIvol and DLP at the CTDI head phantom were reduced to 9.39% with NOB-TCM.
The noise indicates differences in the CT number and the signal in the three-point ROI (anterior hole, mid-central hole, posterior hole) with respect to radiation exposure to the GE performance phantom (Table 5). A miscellaneous increase (<1%) in the average CT number relative to the reference scan (115.8) was observed with every TCM. Trends were also observed with regard to the differences in the CT numbers at each hole, positive values at the anterior hole, and negative values at the mid-central hole. Regarding radiation shields, the average CT numbers were increased by 38.86% with a bismuth shield, and 96.72% with lead glasses, compared with the reference scan. In particular, the CT numbers at the anterior hole with a bismuth shield and lead glasses exhibited dramatic increases of 111.52 and 282.52%, compared with the reference scan.
The noise and SNR values of each ROI were compared with those of the reference scan; the average SNR was decreased to 8.02% with NOB-TCM, 28.36% with lead goggles, and 32.95% with the bismuth shield, respectively (Table 6). The SNR of the anterior hole was decreased to 11.89% with NOB-TCM and 87.89% with the bismuth shield. Average increases in noise of 0.90, 6.29, and 8.38% relative to the reference scan were observed with longitudinal-TCM, angular-TCM, and NOB-TCM, respectively. In particular, the ROI noise increased notably at the posterior hole with longitudinal-TCM and angular-TCM. However, a similar notable increase at the anterior hole was observed for NOB-TCM. In addition, huge increases in average noise were observed with the bismuth shield (499.10%) and lead glasses (411.08%), especially at the anterior hole (Table 7; Fig. 4).

Signal-to-noise ratios (SNRs) of the GE performance phantom with different scanning techniques. TCM tube current modulation, OB organ-based
The average FOM was increased by 11.7% with longitudinal TCM and by 13.39% with NOB-TCM, compared with the reference scan. However, angular TCM, bismuth shield, and lead glasses were associated with decreases of 0.8, 9.2, and 3.6%, respectively (Fig. 5).

Figures of merit (FOMs) at the GE performance phantom achieved with different scanning techniques. TCM tube current modulation, OB organ-based
Discussion
By the early 1990s, CT scans of the brain and body contributed approximately 20% of the collective dose of radiation to the general population [10]. As of 2006, the number of CT examinations was reported to have increased by 10% per year over the past 10–15 years, and accounts for 49% of the total collective radiation dose administered to patients undergoing radiological examination; this corresponds to a 120-fold increase in the CT collective dose since the 1980s [11]. Eye lens is radiosensitive organ. In ICRP Publication 60, the limit on equivalent dose to eye lens of 150 mSv in a year was based on a dose threshold of 0.5–2 Gy for a single exposure [12]. In 2011 the ICRP recommended that the occupational dose limit for an equivalent dose for the lens of the eye to be reduced from 150 to 20 mSv per year, averaged over defined periods of 5 years, with no single year exceeding 50 mSv. The new limit is a substantial reduction of the previously recommended annual eye lens limit of 150 mSv. In ICRP report 118, the threshold value for the absorbed dose to the eye lens was set at 0.5 Gy for acute or protracted exposure [13]. For members of the public, the dose limit was recommended as a maximum of 15 mSv per year [14]. Eye lens turbidity can be induced at radiation exposure doses below the brain CT radiation value of 0.5–2 Gy, and cataracts and secondary vision disorders can be induced at values of 4 Gy or higher [12, 15]. However, current studies suggest that eye lenses are much more radiation sensitive than earlier reports indicated [16].
The older OB-TCM method used to reduce the radiation dose to the eye resulted in a reduction in CT radiation output at the anterior side of the head, whereas radiation at the posterior side was increased as a compensatory mechanism to ensure image quality. Therefore, a reasonable reduction in the total amount of X-ray radiation to the head was not achieved. NOB-TCM can reduce the tube current to the anterior side of the head (i.e., radiosensitive eye location) and maintain the radiation doses to other areas of the body. Therefore, this technique reduces the dose to the eye and head more effectively without a loss of image quality.
In this study, NOB-TCM was applied to an anthropomorphic head phantom, and a decrease in CTDIvol of 16.31% (48.20 mGy) relative to the reference scan (57.59 mGy) was observed; this was the largest decrease among the measured CTDIvol values obtained with all tested TCM methods. This finding differs considerably from the result obtained by Want et al. in which OB-TCM yielded a 1.6% dose reduction [16]. According to radiation exposure measurements obtained with a photosensitive fluorescent dosimeter in our study, NOB-TCM reduced radiation exposure by 25.88%. Radiation shielding methods reduce the dose from a primary X-ray beam by 30–50% when placed on the surface of the target organ [16].
In this study, an in-plane shielding CT examination with bismuth shields yielded a 36.91% reduction in radiation exposure, which was similar to the dose reduction rates reported for other studies and much higher than that obtained with NOB-TCM. Similarly, shielding with lead glasses led to a 44.53% dose reduction. However, a scan that excluded the eye region and adjusted the gantry scanning angle yielded the highest reduction rate of 89.85% (4.61 mGy), compared with the reference scan. These results suggest that excluding the eye region from the CT scan is the best solution for reducing radiation exposure to the eyes. However, NOB-TCM or shielding materials are alternative solutions in cases of head CT involving the orbital region.
In the evaluation of the image quality with the GE performance phantom conducted in this study, CT numbers obtained with NOB-TCM differed little from the reference scan (0.47% increase at the anterior hole, 0.21% decrease at the posterior hole). However, with NOB-TCM, the noise was increased by 13.9% at the anterior hole and 6.5% at the posterior hole from the reference scan. The CT-number and noise was increased to a greater extent at the anterior hole than at the posterior hole. The SNR value decreased by 11.86% at the anterior hole and 6.16% at the posterior hole, with an average SNR decrease of 8.02% from the reference scan. This result was due to a reduction in tube current at the anterior region on the GE performance phantom images.
The bismuth shield and lead glasses reduced radiation exposure to a greater extent than NOB-TCM. However, these techniques also increased the CT number and noise value at the anterior hole, compared to the reference scan. Accordingly, the SNR at the anterior hole and average SNR were decreased. These characteristics resulted in greater variation than that achieved with NOB-TCM. This large-scale reduction in radiation exposure not only affected the CT numbers of images, but also increased the noise. This technique may have a negative effect on the image quality.
The average FOM of the GE performance phantom image was increased with longitudinal-TCM and NOB-TCM, when compared with the reference scan. In contrast, the average FOM of the GE performance phantom image was decreased with the bismuth shield and lead glasses. Because a high FOM value indicates a relatively better system performance from the ROI of radiation exposure and SNR, the TCM can improve the image quality rather than the reference CT scan. Considering the FOM, the TCM was more efficient than bismuth and lead glasses shield scans. The NOB-TCM was still the most effective technique for combined dose reduction to the eye and image quality.
Conclusion
The NOB-TCM was more efficient than in-plane shielding techniques in terms of reducing the radiation dose to the eyes and ensuring image quality. This method can be used to reduce the radiation dose to the eyes when the head CT includes the orbital area.
References
Moström U, Ytterbergh C, Bergström K (1986) Eye lens dose in cranial computed tomography with reference to the technical development of CT scanners. Acta Radiol Diagn 27:599–606
Tweed JJ, Davies ML, Faulkner K, Rawlings DJ, Forster E (1991) Patient dose and associated risk due to radiological investigation of the internal auditory meatus. Br J Radiol 64:447–451
Lund E, Halaburt H (1982) Irradiation dose to the lens of the eye during CT of the head. Neuroradiology 22:181–184
Kohl G (2005) The evolution and state-of-the-art principles of multislice computed tomography. Proc Am Thoracic Soc 2:470–476
Bouffler S, Ainsbury E, Gilvin P, Harrison J (2012) Radiation-induced cataracts: the health protection agency’s response to the ICRP statement on tissue reactions and recommendation on the dose limit for the eye lens. J Radiol Prot 32(4):479
Hohl C, Wildberger JE, Süß C et al (2006) Radiation dose reduction to breast and thyroid during MDCT: effectiveness of an in-plane bismuth shield. Acta Radiol 47:562–567
Geleijns J, Salvadó Artells M, Veldkamp WJH, López Tortosa M, Calzado Cantera A (2006) Quantitative assessment of selective in-plane shielding of tissues in computed tomography through evaluation of absorbed dose and image quality. Eur Radiol 16:2234–2320
Duan X, Wang J, Christner JA, Leng S, Grant KL, McCollough CH (2011) Dose reduction to anterior surfaces with organ-based tube-current modulation: evaluation of performance in a phantom study. Am J Roentgenol 197:689–695
Kudomi S, Yurino F, Hashimoto A, Ueda Y, Ueda K (2014) Off-center effect of a new organ-based tube-current modulation on the image quality and dose reduction to the eye lens. Euro Congress of Radiology. doi:10.1594/ecr2014/C-1357
Maclennan AC, Hadley DM (1995) Radiation dose to the lens from computed tomography scanning in a neuroradiology department. Br J Radiol 68:19–22
Cho PK (2013) The development of a diagnostic reference level on patient dose for head computed tomography angiography examinations in Korea. Radiat Prot Dosim 154:505–509
International Commission on Radiological Protection (1991) ICRP Publication 60: Recommendations of the International Commission on radiological protection, vol 60. Elsevier Health Sciences, Amsterdam
Carinou E, Ferrari P, Bjelac OC, Gingaume M, Merce MS, O’Connor U (2015) Eye lens monitoring for interventional radiology personnel: dosemeters, calibration and practical aspects of H p (3) monitoring. A 2015 review. J Radiol Prot 35(3):R17
International Commission on Radiological Protection (2007) ICRP Publication 103: the 2007 recommendations of the International Commission on radiological protection, vol 103. Elsevier Health Sciences, Amsterdam
National Council on Radiation Protection and Measurements (1993) NCRP report 116: limitation of exposure to ionizing radiation. National Council on Radiation Protection and Measurements, Bethesda, MD
Wang J, Duan X, Christner JA, Leng S, Grant KL, McCollough CH (2012) Bismuth shielding, organ-based tube current modulation, and global reduction of tube current for dose reduction to the eye at head CT. Radiology 262:191–198
Acknowledgements
The authors thank Kyoung-A Um and Minjeong Yun for their help in preparing the CT scanning.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
Author Jung-Su Kim declares that he has no conflict of interest. Author Soon-Mu Kwon declares that he has no conflict of interest. Author Jung-Min Kim declares that he has no conflict of interest. Author Sang-Wook Yoon declares that he has no conflict of interest.
Ethical approval
All procedures performed in studies involves phantom study.
Informed consent
Informed consent is not required for this phantom study.
Rights and permissions
About this article

Cite this article
Kim, JS., Kwon, SM., Kim, JM. et al. New organ-based tube current modulation method to reduce the radiation dose during computed tomography of the head: evaluation of image quality and radiation dose to the eyes in the phantom study. Radiol med 122, 601–608 (2017). https://doi.org/10.1007/s11547-017-0755-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11547-017-0755-5