
Abstract
In the current century, non-communicable diseases (NCDs), particularly cardiovascular diseases, diabetes, cancer, and chronic respiratory diseases, are the most important cause of mortality all over the world. Given the effect of the built environment on people’s health, the present study seeks to conduct a systematic review in order to investigate the relationship between urban form and these four major NCDs as well as their main risk factors. Two independent reviewers in November 2020 after an extensive search through PubMed and Scopus identified 77 studies. Studies published in English were included if they addressed one or more attributes of urban form in relation to any major NCDs and their main risk factors. Publication date, country, geographical scale, study design, methods of built environment measurement, and findings of the relationships among variables were extracted from eligible studies. The findings suggest that the elements of urban form (density, transportation and accessibility, characteristics of building and streetscape, land use, spatial layouts and configuration) could increase or inhibit these diseases through their effect on physical activity, diet, air pollution, blood pressure, and obesity. However, there are study shortages, contradictions, and ambiguities in these relationships which are mainly due to methodological and conceptual challenges. As a result, more in-depth research is needed to achieve solid and consistent results that could be made into clear guidelines for planning and designing healthier cities.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
Introduction
While in this century, non-communicable diseases (NCDs) are the main cause of death around the world, the environment, especially the built environment, is increasingly being recognized as a key factor in promotion of health and prevention of these diseases [1, 2]. Each year, NCDs cause 41 million out of the 57 million deaths in the world (more than 70%), of which 15 million are early deaths [3]. These diseases are a big challenge to public health and may affect different aspects of one’s health [4]. More than 80% of the mortality of NCDs is caused by cardiovascular diseases (46%), cancer (22%), chronic respiratory diseases (11%), and diabetes (4%). The World Health Organization (WHO) has recognized physical inactivity, tobacco use, unhealthy diet, and harmful use of alcohol as the main risk factors of these diseases [3] and added air pollution to its list in 2018 [5]. These factors contribute to the diseases through major metabolic/physiological changes in the body such as raised blood pressure, increased weight/obesity, and increased blood glucose and lipids [3]. Some of these factors are beyond an individual’s control and affected by the policies of urban planning and design which, if regulated during the design, development, and management of the built environment of everyday life, may decrease health risks, NCD rates, and health inequities [6, 7]. Evidence shows that the urban environment may enhance the physical and mental health of the society through their direct and indirect effects on behaviors and activities, air quality, access to healthy water and nutrition, accidents, injuries, and social capital [1, 8,9,10]; therefore, by putting the issue of health at the heart of the new agenda of world cities, WHO has emphasized the importance urban management and planning as key determinants of health justice [11]. In line with this, urban form is regarded as an important concept in urban planning and design which influences the patterns of use, movement, activity, and recreation among citizens. Urban form refers to a number of physical and non-physical features of the city such as size, shape, scale, density, land use, building type, arrangement of urban blocks, and distribution of green space [12]. This notion can be studied on different geographical scales like region, city, neighborhood, block, and street, and scale is central to its understanding, formulation, measurement, and analysis [13]. In general, the urban form consists of five main elements, i.e. density, transportation infrastructure and accessibility, land use, building/housing type, and layout [12]. Understanding how the components of urban form can affect NCDs provides evidence to support interventions that would improve public health outcomes.
So far, several review studies have associated some elements of urban form with health, but mostly with respect to one or two risk factors [14,15,16,17], especially physical activity and obesity [18,19,20], and limited to a certain geographical region [21,22,23]. However, none of them has explicitly established a correlation between the elements of urban form and a specific set of NCDs as well as their risk factors apart from a certain geographical context. Due to the significant role of urban environments in people’s health and the complicated nature of these environments, treating the burden of these diseases and health inequities in cities entails analysis of the role of different dimensions of urban design and planning, including the urban form and structure. This could help decision-makers, planners, urban designers, and health-care experts to understand the factors at work, perform better, and create healthy places. Therefore, the present study provides a systematic review of the literature to synthesize evidence from research findings about the association between the elements of urban form and the four major NCDs as well as their risk factors. This way the diseases and risk factors with the strongest relationship to urban form could be identified and examined with the aim of addressing the challenges and shortcomings in research and informing the agenda of the theory and practice of planning healthy cities.
Method
Search Strategy
We performed a systematic review of the literature on the effects of urban form on major NCDs as well as their risk factors. This search was performed in November 2020 without applying any time limit. Given the wide scope of research in medical science and urban planning, PubMed (a respected database in medical science) and Scopus were used as the databases of the research. The following terms were searched for in the keywords of Scopus articles and in the title and abstract of PubMed articles: “urban form” or “urban morphology” AND “health” or “disease” or “morbidity” or “heart” or “cardiovascular” or “cancer” or “respiratory” or “obstructive pulmonary” or “diabetes” or “risk factors” or “diet” or “food” or “tobacco” or “alcohol” or “air pollution” or “physical activity” or “overweight” or “obesity” or “body mass index” or “blood pressure” or “blood glucose” or “blood lipid” or “cholesterol” (Table S1). The search was limited to scientific journal articles in published in English.
Study Selection
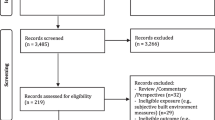
The initial search resulted in 256 articles, including 123 articles from Scopus and 133 articles from PubMed. A step-by-step method was performed to identify the relevant studies. In the first step, duplicate articles (n = 35) were removed using the EndNote software. Then, two independent reviewer checked titles and abstracts of all articles to exclude irrelevant items. In case of disagreement, they screened full-text and discussed to reach agreement. If necessary and in case of disagreement between those two reviewers, the third individual decides to make the final decision. Next, two reviewers independently screened full-text articles for final inclusion. Again, in case of disagreement, the third reviewer decides to make the final decision. The flow of documents through the review is shown in the PRISMA diagram (Fig. 1). The inclusion criteria were as follows:
-
The article must address one or more elements of urban form as independent variables. Those articles that only address the natural environment, socioeconomic environment, or any other component of the built environment in isolation should be removed.
-
The article should consider one or more variables related to major NCDs as dependent variables. These variables include the morbidity and mortality rates of the diseases, their main risk factors (air pollution, physical activity, smoking, alcohol consumption, and diet), and key metabolic symptoms (obesity, being overweight, body mass index (BMI), blood pressure, and blood glucose and lipids). The studies concerning mental or communicable diseases should be removed from the list.
-
The study should address an urban area. Articles about rural areas or those which compare urban and rural areas should be removed.
-
Studies that focus on the participants’ workplace or those which address the scale of architecture and indoor spaces should be removed.
-
Studies of animal subjects should be removed.
-
Studies whose statistical population are from defined clinical subgroups (e.g., those with diabetes, heart stroke) should be removed.
-
Modeling/simulation studies should be removed, as they would not be independent sources of evidence.
-
Protocol studies, studies of legal issues, and studies that introduce guidelines or instructions should be removed.
-
Review, opinion, and commentary articles should be removed.
-
Studies published in languages other than English should be removed.

Flow diagram of the study selection process, following PRISMA reporting style [24]
Finally, here is no limitation concerning geographical context and date of publication. Reasons for excluding studies based on full-text review are shown in Table S2.
Data Extraction and Synthesis
Selected articles were closely studied and data extraction started. For this step and in order to classify data, a data extraction form based on previous studies [15, 21, 22] was designed in Microsoft Excel. The data include publication date, country of study, geographical scale of the study of urban form, research design and methodology (type of study design and measurement of urban form variables), dependent and independent variables (NCD-related variables, and criteria and indices of urban form), and findings of the relationships among variables (positive, negative, contradictory, or lack of relationship). Also, the criteria and indices of urban form defined in the articles were extracted and categorized according to five main elements of urban form (density, transportation and accessibility, characteristics of building and streetscape, land use, spatial layouts and configuration). The frequency of data and their relationships were analyzed based on distinguished categories. These include five elements of urban form and three categories of main NCD-related variables (i.e., presence of NCD, metabolic issues, and risk factors). In order to clarify the association between the elements of urban form and NCD-related variables, the findings were classified in four types: positive, negative, contradictory, and lack of relationship.
Results
Study Characteristics
This review incorporates 77 articles (Table S3). About 43% of the articles (n = 33) were published in 2016–2020 and no article before 2002 was qualified for inclusion. Forty-one percent of selected articles have been conducted in the United State, followed by Canada (17%), China (16%), and Australia (5%). The majority of studies (about 67%) examine the elements of urban form on neighborhood scale, in buffers of 500–2000 m around residential areas and census blocks and districts. Thirty-one percent (n = 24) of the articles address a macroscale (city, region, county, suburban). Stockton and colleagues simultaneously study macroscale and microscales of the urban form [25]. There are also differences in the measurement of environment and study design. Most of the studies (89%) are cross-sectional and only 7% are longitudinal. Furthermore, two studies enjoy both cross-sectional and longitudinal designs [26, 27]. For measuring the environment, the most common method is the objective measurement through using tools such as Geographic Information System (GIS) dependent on the existing spatial data, systematic observation, and modeling software (86%). Only two of the studies quantify the perceived environment and its effect on physical activity through a questionnaire [28, 29]. In addition, about 12% of the studies used both objective and subjective methods to measure the elements of urban form. Characteristics of the 77 studies reviewed are shown in Table 1.
Criteria and Indices of Urban Form in Relation to the Variables of Major NCDs
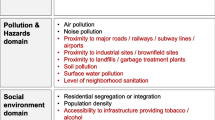
In the “Introduction” section, we named the five main elements of urban form (density, land use, transportation and accessibility, building/housing type, and spatial layout). Given the planning and physical design of urban spaces, each element has a set of criteria and indices [12]. The criteria and indices of urban form related to major NCDs and their risk factors were extracted from the 77 articles and categorized with slight modifications according to our fivefold classification of urban form elements. The categorization is shown in Table 2.
NCDs Variables Related to Urban Form
Table 3 shows the number of studies addressing any one of the urban form elements in relation to NCDs based on the variables in three main groups of health components (i.e., Presence of NCD, metabolic issues, and risk factors). As can be seen in the table, physical inactivity (n = 38) and air pollution (n = 20) were the exposure categories most frequently published with regard to urban form. In the category of metabolic issues, most studies focus on overweightness and obesity (n = 15). Also, the relationship of one or more major NCDs and their mortality rate to urban form was the topic of 9 articles. There was no study about tobacco use, harmful use of alcohol, and raised blood glucose and lipids.
The Association Between the Elements of Urban Form and NCD-Related Variables
How the relationship between the elements of urban form and NCD-related variables extracted from the literature’s findings, and classified in four types (positive, negative, contradictory, and lack of relationship) (Table 4). The results for each element of urban form present below.
Density
Density has been studied in 49 articles according to five criteria (population density, floor area ratio (FAR), residential density, site coverage ratio, and construction volume density). The results mostly associate increased density with reduced physical activity [30,31,32,33], obesity [34,35,36], cardiovascular diseases [37, 38], cancer, and diabetes [39]. By contrast, studies about air pollution and chronic respiratory diseases confirm a direct relationship between densities with air pollution, which will increase the rate of respiratory diseases [40,41,42]. Moreover, two studies have found a positive relationship between unhealthy diet and population density residential density due to the increase in the number of fast-food stores and retail stores [43, 44]. In other words, density has a differential effect on health. For example, a study has concluded that high-walkability neighborhoods with high residential density may contribute to lower mortality due to cardiovascular diseases by promoting physical activity whereas they suffer from more air pollution [45].
Other studies offer different and sometimes contradictory results about the relationship between the criteria of density and their consequences for urban health. This may be explained by various reasons such as the varying effect of the environment on different air pollutants [46,47,48], differences in the concept and effect of density on different geographical scales and buffers [36, 49], and different effects of density on different aspects of physical activity [50, 51].
Land Use
The relationship of this element of urban form with NCD-related variables has been addressed in 51 studies. The majority of these studies indicate that higher proportions of non-residential uses (commercial, community, etc.), recreational land uses, green space and water area, and food environment as well as land use mix and diversity is associated with increased physical activity [28, 52,53,54,55,56,57,58] and reduction in obesity [35, 59, 60] and other major NCDs [39, 61, 62]. As with diet, several studies have associated it with access to healthy and unhealthy environments and land use mix independently or along with other walkability indices [43, 50, 63]. In general, land use mix has shown a positive and synergistic effect on different health variables (particularly physical activity). However, a number of studies have discovered unexpected, inconsistent relationships or found no relationship at all among these variables. For example, Luan et al. associate increased air pollution with higher density of green areas and lower density of water areas; also, they associate dispersion of green areas with the concentration of air pollutants in a 500 m buffer whereas this association does not exist for 1000 m and 2000 m buffers [64]. It seems that these differing results are due to differences in the geographical scales and buffers under study, considering statistical samples of a specific age [65], the effects of geographical context and its specific attributes [66,67,68], lack of correspondence between objective and self-reported measures of built environment [69], varying effects on the different aspects of physical activity [51, 70] and different air pollutants [48]. Also, each of the criteria of land use and its indices can bring about different consequences for the variables of health. For example, Gao et al. show that air pollution is positively correlated with commercial land uses while it has a negative relationship with green space [71].
Characteristics of Building and Streetscape
This element of urban form has been less studied than other elements (n = 17). According to the literature, increased visibility of the street (influence on security) and aesthetic features (street lighting, trees, landmark buildings, etc.) are major factors in improving health due to their effect on physical activity [29, 52, 72, 73], blood pressure, obesity, cardiovascular diseases, and diabetes [61, 65, 74]. Also, decreased height difference and average building height on the scale of neighborhoods is associated with lower air pollution [64], although a study has resulted in a non-linear relationship between height and air pollutant [71]. As to the age and type of buildings, there have been heterogeneous results concerning its association with physical activity [75, 76], cardiovascular diseases [38], and chronic respiratory diseases [41], which may be due to the lack of moderation of effective factors and differences in statistical population. A number of studies deny the relationship of aesthetic characteristics and visibility of the street to physical activity owing to the subjective measurement of the environment and the influence of other social and psychological factors [69, 77].
Transportation and Accessibility
As another element of urban form, transportation and accessibility have been addressed in 59 articles, most of which have indicated that enhancement of the infrastructure of public transportation, walking and cycling, accessibility of destinations and streets (density of intersections and block size), and road management can significantly contribute to the prevention of major NCDs as well as their risk factors [37], particularly physical inactivity [78,79,80,81,82,83] and obesity [59, 60, 84]. Concerning the infrastructure of private transportation, higher density of length and area of main streets and facilities for private transportation (parking and gas station) contribute to the use of private cars and find a positive association with air pollution [40, 64, 85], unhealthy diet [86], cardiovascular diseases [87], and respiratory diseases [41]. However, a number of studies have achieved contradictory or unexpected results or discovered no relationship at all between some of the criteria of this element and health risks. One reason for this is the varying effects of this element on different physical activities. For example, Kaplan et al. mention the inconsistent role of some variables on two types of active travel (walking and cycling) and associate higher public transportation stations with increased walking but decreased cycling [88]. Other reasons to explain this inconsistency in results include differences in geographical scales and buffers [71], differences in statistical population and research methods [26, 89], different geographical contexts [66, 67, 87], and the effect of mediating factors [90, 91].
Spatial Layout and Configuration
Spatial layout and configuration are other elements of urban form which has been investigated in 27 studies, particularly in relation to air pollution. Most studies confirm the positive relationship of air pollution to the area size, complexity and irregularity of the city’s shape, urban fragmentation, and urban sprawl [92,93,94,95,96,97]. There are also different and inconsistent results which may be explained by differences in the geographical context and other environmental, economic, and social factors of sites [98, 99], the city’s size and the geographical scale in question [100], and difference in research and analysis methods [46]. For example, in a longitudinal study in China, Zhou et al. confirm a negative relationship between city size and air pollution and state that, in contrast to European and American cities, urban development in China has made use of clean energies and contributed to the reduction of air pollution [99]. Conversely, Liu et al. have studied cities with different sizes in different seasons and obtained inconsistent results about this relationship [100].
Concerning physical activity, this element of urban form has only been studied in terms of space syntax indexes [61, 65, 101, 102], and one article, in terms of urban sprawl [36].
Discussion and Conclusion
This study systematically investigated the relationship between urban form and major NCDs which are the main cause of mortality in the current century. The aim was to identify the health benefits and risks of planning and designing the different elements of urban form. For this purpose, after studying 77 scientific articles and then extracting the criteria and indices of urban form that affect NCDs and their risk factors, their relationships, as well as the shortcomings of research in this field, were studied. The findings of this study are indicative of a significant relationship between the elements of urban form and the risk factors as well as the morbidity rate of NCDs. These findings conform to previous studies which associated urban form with physical inactivity [19, 103], obesity [20], hypertension, diabetes [14, 15], cardiovascular diseases [16, 104], and other aspects of physical health [21, 23, 105].
Concerning research into relationship of the elements of urban form to three main groups of NCDs components (i.e. major NCDs, metabolic issues, and risk factors), the issue of physical inactivity on the microscale and the issue of air pollution on the macroscale were the most recurrent topics in the reviewed articles. Following these two factors, obesity (among the metabolic issues) and cardiovascular diseases (among the four major NCDs) were the most frequently published topics identified with regard to urban form. This point clarifies the influence of physical activity and air pollution on the built environment and related diseases and other risk factors investigated in those researches. The predominance of these two subjects could be contextual. For instance, most of the studies reviewed have been done in developed countries specifically in the USA. Therefore, the prevalence could be the result of the challenges of those geographic areas.
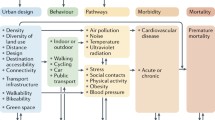
Considering a set of variables and the synthetic approach of this study, and based on the relationships among risk factors, metabolic changes, and NCDs, we developed a framework for gaining a more comprehensive understanding of the complicated relationships between health and the built environment (Fig. 2). According to this framework, the quality and quantity of the elements of urban form (including density, transportation and accessibility, characteristics of building and streetscape, land use, and spatial layout and configuration) affect the three main risk factors (amount and duration of physical activity, access to and consumption of healthy food, emission and concentration of air pollutants) and are associated with the metabolic issues of citizens (raised blood pressure, obesity, and overweightness) as well as with preventing or increasing the morbidity of major NCDs including cardiovascular diseases, chronic respiratory diseases, diabetes, and cancer. As with physical activity, different factors of urban form and the environment of everyday life, particularly upgrade of public transportation, walking, and cycling infrastructures, higher density of intersections, easier access to destinations, green space, increased land uses mix, continuity of the city, and higher density of population and housing, can encourage citizens to perform physical activity, which in turn contributes to the prevention of obesity and high blood pressure that are two major factors in cardiovascular diseases and diabetes. This supports other work like Giles-Corti et al. in the Lancet, 2016 [7]. In addition, the majority of studies have focused on the relation between air pollution and spatial configuration and density on the city scale, associating urban sprawl, complexity and irregularity of the city’s shape, population density, green space, density of streets, and height differences in blocks and streets with factors such as traffic density, wind stream, and emission and concentration of air pollutants which may lead to hypertension and respiratory diseases. Some studies, which were mostly performed on the neighborhood scale, have associated diet with food environment, land use mix, access to destinations, and density.

Framework of association between urban form and non-communicable diseases
The findings suggest that there are research shortcomings, inconsistencies, and ambiguities in the relationships between health and urban form. This is a challenge in the way of achieving solid and consistent results that could be turned into clear guidelines for urban planners and policy-makers. The first challenge is the contradictory and differential effects of some elements of urban form on the components of health. Thus, improving one component can sometimes be harmful to another component. Therefore, in order to implement the components of health-oriented urban form, researchers should examine and quantify these ambivalent effects. The second challenge of planning and policy-making in this field is the inconsistent results concerning each component. For example, although most studies have confirmed a positive association between urban sprawl and air pollution, some researchers have discovered an inverse relationship. A large part of these contradictions and ambiguities results from methodological and conceptual challenges which are listed below:
-
Prevalence of cross-sectional rather than longitudinal studies: many of the reviewed studies have implemented cross-sectional designs which may not be able to successfully demonstrate causative, moderated, and non-linear relationships.
-
Varying effects of urban form on different urban scales and vagueness in the definition of the districts of the physical environment: for instance, improving one criterion on the city scale may aggravate the health status on the neighborhood scale, or the effect of a criterion on health in large cities may be different from that in smaller cities. Inconsistent definitions of the districts of the physical environment such as neighborhood and varying sizes of residential buffers in the studies may also contribute to the difference in results.
-
Difference in objective and perceived measures of built environment: lack of correspondence between the perceived and objective environments is another reason for inconsistent results. For example, McCormack and Mardinger report a positive association between the objective walkability of neighborhood and physical activity while they reject any significant relationship between the subjective walkability and physical activity [69].
-
Ignoring the mediating variables and not moderating them: there are various factors such as social, environmental, and individual features which may affect the relationships between health and urban form. Moderating or not moderating these factors in a study can led to different results.
-
Difference in the effect of environment on different air pollutants and physical activity: some of the criteria have shown different effects on the indices of each group. For example, high density of public transportation stations around one’s house may encourage students to walk to school while at the same time decrease the use of bicycle [88].
In addition to these reasons, it seems that differences in geographical context, difference in statistical population (gender and age), lack of reliability and validity of self-selection of a residential environment, ignoring non-linear relationships, and different research and analysis methods may explain the inconsistency of results. Future studies should consider these ambiguities and move toward obtaining more solid results that could be efficiently implemented in urban planning. Another challenge in this field is the inadequacy of the evidence for some relationships (e.g., relationship between diet and urban form) and the effects of other variables as well as more recent issues in urban design (smart city, complete street, pedestrian network, etc.) which require further investigation.
One of the advantages of the present study is that it is the first systematic examination of the effects of the elements of urban form on NCDs and their risk factors (as indicators of physical health) without any geographical limitation. Simultaneous investigation of different health components and a synthetic approach contribute to a comprehensive understanding of the complicated and sometimes contradictory relationships between these components and urban form, while at the same time providing a reference framework for future research in this field and guiding the policies and actions of urban designers and planners toward developing healthier cities. In addition, the present study has moved beyond previous studies which mainly addressed the health-related urban elements in general with the aim of extracting the criteria and indices of those studies and investigating their effectiveness. However, there are also limitations to this study. Although the search strategy was used due to make as comprehensive a selection of articles as possible, some studies may have been missed as a result of limited search conditions, parameters, keywords, and databases. Furthermore, restriction to the English language while understandable is a limitation that could be acknowledged, in that it could be associated with some unintended geographic bias toward studies in English-speaking countries. In addition, the majority of studies in this review have made use of cross-sectional designs which cannot make solid conclusions about the real cause-and-effect relationships. There were no accompanying meta-analysis synthesizing results for strength of association across the studies. Furthermore, the risk of bias was not discussed in this study.
Due to continuous rise in the number of studies in this field, we should make some suggestions for further research. First, there is a need to focus more on longitudinal studies to allow for more solid conclusions about causative relationships. Second, the possible mediating factors should be studied. Third, future studies should systematically consider the different criteria of urban form on different scales as well as their effect on the components of health. Fourth, they should endeavor to determine a minimum threshold for each criterion to have a positive effect on the components of health. Finally, more research is needed into the relationship of the criteria of urban form to diet, blood pressure, and the four major NCDs.
In general, the findings indicate that urban planning and design play a crucial role in creating healthy cities. By manipulating the elements of urban form, health risks such as physical inactivity and air pollution could be reduced and the morbidity of NCDs could be decreased. Although having a healthy physical environment is not a sufficient condition for improving public health, this improvement is only possible when the policies of urban planning and design are supported by the concepts of health.
References
Lopez RP. The built environment and public health. 1st ed. John Wiley & Sons; 2012.
Prüss-Üstün A, Wolf J, Corvalán C, Bos R, Neira M. Preventing disease through healthy environments: a global assessment of the burden of disease from environmental risks. World Health Organization; 2016. https://apps.who.int/iris/handle/10665/204585. Accessed 14 Oct 2020.
World Health Organization. Noncommunicable diseases country profiles 2018. World Health Organization. 2018. https://apps.who.int/iris/handle/10665/274512. Accessed 13 June 2021.
World Health Organization. Global action plan for the prevention and control of noncommunicable diseases 2013–2020. World Health Organization; 2013. https://apps.who.int/iris/rest/bitstreams/442296/retrieve. Accessed 14 Oct 2020.
World Health Organization. Noncommunicable diseases and air pollution: WHO European high-level conference on noncommunicable diseases. World Health Organization. 2019. https://www.euro.who.int/__data/assets/pdf_file/0005/397787/Air-Pollution-and-NCDs.pdf. Accessed 13 June 2021.
World Health Organization. Noncommunicable diseases: progress monitor 2020. World Health Organization. 2020. https://apps.who.int/iris/rest/bitstreams/1267930/retrieve. Accessed 19 Oct 2020.
Giles-Corti B, Vernez-Moudon A, Reis R, et al. City planning and population health: a global challenge. Lancet. 2016;388(10062):2912–24. https://doi.org/10.1016/S0140-6736(16)30066-6.
Northridge ME, Sclar ED, Biswas P. Sorting out the connections between the built environment and health: a conceptual framework for navigating pathways and planning healthy cities. J Urban Health. 2003;80(4):556–68. https://doi.org/10.1093/jurban/jtg064.
Vlahov D, Freudenberg N, Proietti F, et al. Urban as a determinant of health. J Urban Health. 2007;84(1):16–26. https://doi.org/10.1007/s11524-007-9169-3.
Northridge ME, Freeman L. Urban planning and health equity. J Urban Health. 2011;88(3):582–97. https://doi.org/10.1007/s11524-011-9558-5.
World Health Organization. Health as the pulse of the new urban agenda: United Nations conference on housing and sustainable urban development, Quito, October 2016. 2016. https://apps.who.int/iris/rest/bitstreams/1061550/retrieve. Accessed 6 Mar 2021.
Dempsey N, Brown C, Raman S, et al. Elements of urban form. In: Jenks M, Jones C, editors. Dimensions of the sustainable city. Future City, vol 2. Springer, Dordrecht; 2010. p. 21–51. https://doi.org/10.1007/978-1-4020-8647-2_2.
Živković J. Urban form and function. Clim Action. 2020:862–871. https://doi.org/10.1007/978-3-319-95885-9_78.
Chandrabose M, Rachele JN, Gunn L, et al. Built environment and cardio-metabolic health: systematic review and meta-analysis of longitudinal studies. Obes Rev. 2019;20(1):41–54. https://doi.org/10.1111/obr.12759.
Dendup T, Feng X, Clingan S, Astell-Burt T. Environmental risk factors for developing type 2 diabetes mellitus: a systematic review. Int J Environ Res Public Health. 2018;15(1):78. https://doi.org/10.3390/ijerph15010078.
Malambo P, Kengne AP, De Villiers A, Lambert EV, Puoane T. Built environment, selected risk factors and major cardiovascular disease outcomes: a systematic review. PLoS ONE. 2016;11(11):e0166846. https://doi.org/10.1371/journal.pone.0166846.
Wray AJD, Minaker LM. Is cancer prevention influenced by the built environment? A multidisciplinary scoping review. Cancer. 2019;125(19):3299–311. https://doi.org/10.1002/cncr.32376.
McCormack GR, Shiell A. In search of causality: a systematic review of the relationship between the built environment and physical activity among adults. Int J Behav Nutr Phys Act. 2011;8(1):1–11. https://doi.org/10.1186/1479-5868-8-125.
Kärmeniemi M, Lankila T, Ikäheimo T, Koivumaa-Honkanen H, Korpelainen R. The built environment as a determinant of physical activity: a systematic review of longitudinal studies and natural experiments. Ann Behav Med. 2018;52(3):239–51. https://doi.org/10.1093/abm/kax043.
Durand CP, Andalib M, Dunton GF, Wolch J, Pentz MA. A systematic review of built environment factors related to physical activity and obesity risk: implications for smart growth urban planning. Obes Rev. 2011;12(5):e173–82. https://doi.org/10.1111/j.1467-789X.2010.00826.x.
Schulz M, Romppel M, Grande G. Built environment and health: a systematic review of studies in Germany. J Public Health. 2018;40(1):8–15. https://doi.org/10.1093/pubmed/fdw141.
Kim DH, Yoo S. How does the built environment in compact metropolitan cities affect health? A systematic review of Korean studies. Int J Environ Res Public Health. 2019;16(16):2921. https://doi.org/10.3390/ijerph16162921.
McCormack GR, Cabaj J, Orpana H, et al. Evidence synthesis A scoping review on the relations between urban form and health: a focus on Canadian quantitative evidence. Health Promot Chronic Dis Prev Can. 2019;39(5):187. https://doi.org/10.24095/hpcdp.39.5.03.
Page MJ, McKenzie JE, Bossuyt PM, The PRISMA, et al. statement: an updated guideline for reporting systematic reviews. BMJ. 2020;2021:372. https://doi.org/10.1016/j.ijsu.2021.105906.
Stockton JC, Duke-Williams O, Stamatakis E, Mindell JS, Brunner EJ, Shelton NJ. Development of a novel walkability index for London, United Kingdom: cross-sectional application to the Whitehall II Study. BMC Public Health. 2016;16:416. https://doi.org/10.1186/s12866-020-01731-9.
Timperio A, Crawford D, Ball K, Salmon J. Typologies of neighbourhood environments and children’s physical activity, sedentary time and television viewing. Health Place. 2017;43:121–7. https://doi.org/10.1016/j.healthplace.2016.10.004.
Ewing R, Brownson RC, Berrigan D. Relationship between urban sprawl and weight of United States youth. Am J Prev Med. 2006;31(6):464–74. https://doi.org/10.1016/j.amepre.2006.08.020.
McCormack GR, Friedenreich CM, Giles-Corti B, Doyle-Baker PK, Shiell A. Do motivation-related cognitions explain the relationship between perceptions of urban form and neighborhood walking? J Phys Act Health. 2013;10(7):961–73. https://doi.org/10.1123/jpah.10.7.961.
King AC, Toobert D, Ahn D, et al. Perceived environments as physical activity correlates and moderators of intervention in five studies. Article. Am J Health Promot. 2006;21(1):24–35. https://doi.org/10.4278/0890-1171-21.1.24.
McCormack GR, Shiell A, Doyle-Baker PK, Friedenreich CM, Sandalack BA. Subpopulation differences in the association between neighborhood urban form and neighborhood-based physical activity. Health Place. 2014;28:109–15. https://doi.org/10.1016/j.healthplace.2014.04.001.
Siu VW, Lambert WE, Fu R, Hillier TA, Bosworth M, Michael YL. Built environment and its influences on walking among older women: use of standardized geographic units to define urban forms. J Environ Public Health. 2012;2012:203141. https://doi.org/10.1155/2012/203141.
de Sa E, Ardern CI. Associations between the built environment, total, recreational, and transit-related physical activity. BMC Public Health. 2014;14:693. https://doi.org/10.1186/1471-2458-14-693.
Rundle AG, Sheehan DM, Quinn JW, et al. Using GPS data to study neighborhood walkability and physical activity. Am J Prev Med. 2016;50(3):e65–72. https://doi.org/10.1016/j.amepre.2015.07.033.
Rundle A, Diez Roux AV, Free LM, Miller D, Neckerman KM, Weiss CC. The urban built environment and obesity in New York City: a multilevel analysis. Am J Health Promot. 2007;21(4 Suppl):326–334. https://doi.org/10.4278/0890-1171-21.4s.326.
Koohsari MJ, Kaczynski AT, Hanibuchi T, et al. Physical activity environment and Japanese adults’ body mass index. Article. Int J Environ Res Public Health. 2018;15(4)596. https://doi.org/10.3390/ijerph15040596.
Ewing R, Schmid T, Killingsworth R, Zlot A, Raudenbush S. Relationship between urban sprawl and physical activity, obesity, and morbidity. Am J Health Promot. 2003;18(1):47–57. https://doi.org/10.4278/0890-1171-18.1.47.
Shoultz G, Givens J, Drane JW. Urban form, heart disease, and geography: a case study in composite index formation and bayesian spatial modeling. Article. Popul Res Policy Rev. 2007;26(5–6):661–85. https://doi.org/10.1007/s11113-007-9049-2.
Réquia Júnior WJ, Roig HL, Koutrakis P. A novel land use approach for assessment of human health: the relationship between urban structure types and cardiorespiratory disease risk. Article. Environ Int. 2015;85:334–42. https://doi.org/10.1016/j.envint.2015.09.026.
Sturm R, Cohen DA. Suburban sprawl and physical and mental health. Article. Public Health. 2004;118(7):488–96. https://doi.org/10.1016/j.puhe.2004.02.007.
Clark LP, Millet DB, Marshall JD. Air quality and urban form in U.S. urban areas: evidence from regulatory monitors. Article. Environ Sci Technol. 2011;45(16):7028–7035. https://doi.org/10.1021/es2006786.
Monteiro A, Carvalho V, Velho S, Sousa C. Assessing and monitoring urban resilience using COPD in Porto. Article. Sci Total Environ. 2012;414:113–9. https://doi.org/10.1016/j.scitotenv.2011.11.009.
Li C, Song Y, Tian L, Ouyang W. Urban form, air quality, and cardiorespiratory mortality: a path analysis. Article. Int J Environ Res Public Health. 2020;17(4)1202. https://doi.org/10.3390/ijerph17041202.
Polsky JY, Moineddin R, Glazier RH, Dunn JR, Booth GL. Foodscapes of southern Ontario: neighbourhood deprivation and access to healthy and unhealthy food retail. Can J Public Health = Revue canadienne de sante publique. 2014;105(5):e369–75. https://doi.org/10.17269/cjph.105.4541.
Murphy M, Badland H, Jordan H, Koohsari MJ, Giles-Corti B. Local food environments, suburban development, and BMI: a mixed methods study. Int J Environ Res Public Health. 2018;15(7). https://doi.org/10.3390/ijerph15071392.
Hankey S, Marshall JD, Brauer M. Health impacts of the built environment: within-urban variability in physical inactivity, air pollution, and ischemic heart disease mortality. Article. Environ Health Perspect. 2012;120(2):247–53. https://doi.org/10.1289/ehp.1103806.
Fan C, Tian L, Zhou L, et al. Examining the impacts of urban form on air pollutant emissions: evidence from China. Article. J Environ Manag. 2018;212:405–14. https://doi.org/10.1016/j.jenvman.2018.02.001.
He L, Liu Y, He P, Zhou H. Relationship between air pollution and urban forms: evidence from prefecture-level cities of the yangtze river Basin. Article. Int J Environ Res Public Health. 2019;16(18)3459. https://doi.org/10.3390/ijerph16183459.
Li C, Wang Z, Li B, Peng ZR, Fu Q. Investigating the relationship between air pollution variation and urban form. Article. Build Environ. 2019;147:559–68. https://doi.org/10.1016/j.buildenv.2018.06.038.
Bereitschaft B, Debbage K. Urban form, air pollution, and CO2 emissions in large U.S. metropolitan areas. Article. Prof Geogr. 2013;65(4):612–635. https://doi.org/10.1080/00330124.2013.799991.
Cerin E, Frank LD, Sallis JF, et al. From neighborhood design and food options to residents’ weight status. Appetite. 2011;56(3):693–703. https://doi.org/10.1016/j.appet.2011.02.006.
McCormack GR. Neighbourhood built environment characteristics associated with different types of physical activity in Canadian adults. Article. Health Promot Chronic Dis Prev Can. 2017;37(6):175–185. https://doi.org/10.24095/hpcdp.37.6.01.
Collins PA, Tait J, Fein A, Dunn JR. Residential moves, neighbourhood walkability, and physical activity: a longitudinal pilot study in Ontario Canada. BMC Public Health. 2018;18(1):933. https://doi.org/10.1186/s12889-018-5858-y.
Wei YD, Xiao W, Medina R, Tian G. Effects of neighborhood environment, safety, and urban amenities on origins and destinations of walking behavior. Article. Urban Geogr. 2019. https://doi.org/10.1080/02723638.2019.1699731.
Lee JS. Urban form, children’s active travel to/from school, and travel related physical activity. Article. Int Rev Spat Plann Sustain Dev. 2020;8(1):21–38. https://doi.org/10.14246/IRSPSD.8.1_21.
McCormack GR, Shiell A, Giles-Corti B, et al. The association between sidewalk length and walking for different purposes in established neighborhoods. Article. Int J Behav Nutr Phys Act. 2012;992. https://doi.org/10.1186/1479-5868-9-92.
Cutumisu N, Spence JC. Sport fields as potential catalysts for physical activity in the neighbourhood. Article. Int J Environ Res Public Health. 2012;9(1):294–314. https://doi.org/10.3390/ijerph9010294.
Patterson PK, Chapman NJ. Urban form and older residents’ service use, walking, driving, quality of life, and neighborhood satisfaction. Am J Health Promot. 2004;19(1):45–52. https://doi.org/10.4278/0890-1171-19.1.45.
McCormack GR, McLaren L, Salvo G, Blackstaffe A. Changes in objectively-determined walkability and physical activity in adults: a quasi-longitudinal residential relocation study. Int J Environ Res Public Health. 2017;14(5). https://doi.org/10.3390/ijerph14050551.
Rundle AG, Chen Y, Quinn JW, et al. Development of a neighborhood walkability index for studying neighborhood physical activity contexts in communities across the U.S. over the past three decades. J Urban Health. 2019;96(4):583–590. https://doi.org/10.1007/s11524-019-00370-4.
Frank LD, Andresen MA, Schmid TL. Obesity relationships with community design, physical activity, and time spent in cars. Am J Prev Med. 2004;27(2):87–96. https://doi.org/10.1016/j.amepre.2004.04.011.
Fathi S, Sajadzadeh H, Sheshkal FM, et al. The role of urban morphology design on enhancing physical activity and public health. Article. Int J Environ Res Public Health. 2020;17(7)2359. https://doi.org/10.3390/ijerph17072359.
Shen YS, Lung SC. Multiple impacts and pathways of urban form and environmental factors on cardiovascular mortality. Sci Total Environ. 2020;738:139512. https://doi.org/10.1016/j.scitotenv.2020.139512.
Kerr J, Frank L, Sallis JF, Saelens B, Glanz K, Chapman J. Predictors of trips to food destinations. Article. Int J Behav Nutr Phys Act. 2012;958. https://doi.org/10.1186/1479-5868-9-58.
Luan Q, Jiang W, Liu S, Guo H. Impact of urban 3D morphology on particulate matter 2.5 (PM2.5) concentrations: case study of Beijing, China. Article. Chin Geogr Sci. 2020;30(2):294–308. https://doi.org/10.1007/s11769-020-1112-5.
Özbil A, Yeşiltepe D, Argın G. Home and school environmental correlates of childhood BMI. Article. J Transp Health. 2020;16100823. https://doi.org/10.1016/j.jth.2020.100823.
Charreire H, Weber C, Chaix B, et al. Identifying built environmental patterns using cluster analysis and GIS: relationships with walking, cycling and body mass index in French adults. Article. Int J Behav Nutr Phys Act. 2012;959. https://doi.org/10.1186/1479-5868-9-59.
Ahn Y, Park J, Bruckner TA, Choi S. Do local employment centers modify the association between neighborhood urban form and individual obesity? Article. Environ Plann A. 2018;50(5):1128–43. https://doi.org/10.1177/0308518X18765478.
Richardson EA, Mitchell R, Hartig T, de Vries S, Astell-Burt T, Frumkin H. Green cities and health: a question of scale? J Epidemiol Community Health. 2012;66(2):160–5. https://doi.org/10.1136/jech.2011.137240.
McCormack GR, Mardinger C. Neighbourhood urban form and individual-level correlates of leisure-based screen time in Canadian adults. BMJ Open. 2015;5(11):e009418. https://doi.org/10.1136/bmjopen-2015-009418.
Koohsari MJ, Shibata A, Ishii K, et al. Built environment correlates of objectively-measured sedentary behaviours in densely-populated areas. Article. Health Place. 2020;66102447. https://doi.org/10.1016/j.healthplace.2020.102447.
Gao Y, Wang Z, Liu C, Peng ZR. Assessing neighborhood air pollution exposure and its relationship with the urban form. Article. Build Environ. 2019;155:15–24. https://doi.org/10.1016/j.buildenv.2018.12.044.
McMillan TE. The relative influence of urban form on a child’s travel mode to school. Article. Transp Res Part A: Policy Pract. 2007;41(1):69–79. https://doi.org/10.1016/j.tra.2006.05.011.
Jack E, McCormack GR. The associations between objectively-determined and self-reported urban form characteristics and neighborhood-based walking in adults. Int J Behav Nutr Phys Act. 2014;11:71. https://doi.org/10.1186/1479-5868-11-71.
Lovasi GS, Bader MD, Quinn J, Neckerman K, Weiss C, Rundle A. Body mass index, safety hazards, and neighborhood attractiveness. Am J Prev Med. 2012;43(4):378–84. https://doi.org/10.1016/j.amepre.2012.06.018.
Berrigan D, Troiano RP. The association between urban form and physical activity in U.S. adults. Am J Prev Med. 2002;23(2 Suppl):74–9. https://doi.org/10.1016/s0749-3797(02)00476-2.
King WC, Belle SH, Brach JS, Simkin-Silverman LR, Soska T, Kriska AM. Objective measures of neighborhood environment and physical activity in older women. Am J Prev Med. 2005;28(5):461–9. https://doi.org/10.1016/j.amepre.2005.02.001.
Beenackers MA, Kamphuis CB, Prins RG, Mackenbach JP, Burdorf A, van Lenthe FJ. Urban form and psychosocial factors: do they interact for leisure-time walking? Med Sci Sports Exerc. 2014;46(2):293–301. https://doi.org/10.1249/mss.0000000000000017.
Drewnowski A, Moudon AV, Jiao J, Aggarwal A, Charreire H, Chaix B. Food environment and socioeconomic status influence obesity rates in Seattle and in Paris. Int J Obes (2005). 2014;38(2):306–14. https://doi.org/10.1038/ijo.2013.97.
Holt NL, Spence JC, Sehn ZL, Cutumisu N. Neighborhood and developmental differences in children’s perceptions of opportunities for play and physical activity. Article. Health Place. 2008;14(1):2–14. https://doi.org/10.1016/j.healthplace.2007.03.002.
Koohsari MJ, Sugiyama T, Lamb KE, Villanueva K, Owen N. Street connectivity and walking for transport: role of neighborhood destinations. Article. Prev Med. 2014;66:118–22. https://doi.org/10.1016/j.ypmed.2014.06.019.
Frank LD, Schmid TL, Sallis JF, Chapman J, Saelens BE. Linking objectively measured physical activity with objectively measured urban form: findings from SMARTRAQ. Am J Prev Med. 2005;28(2 Suppl 2):117–25. https://doi.org/10.1016/j.amepre.2004.11.001.
Kerr J, Norman G, Millstein R, et al. Neighborhood environment and physical activity among older women: findings from the San Diego cohort of the women’s health initiative. Article. J Phys Act Health. 2014;11(6):1070–1077. https://doi.org/10.1123/jpah.2012-0159.
Ribeiro AI, Hoffimann E. Development of a neighbourhood walkability index for porto metropolitan area. How strongly is walkability associated with walking for transport? Article. Int J Environ Res Public Health. 2018;15(12)2767. https://doi.org/10.3390/ijerph15122767.
Coogan PF, White LF, Evans SR, et al. Longitudinal assessment of urban form and weight gain in African-American women. Am J Prev Med. 2011;40(4):411–8. https://doi.org/10.1016/j.amepre.2010.12.013.
Su JG, Apte JS, Lipsitt J, et al. Populations potentially exposed to traffic-related air pollution in seven world cities. Article. Environ Int. 2015;78:82–9. https://doi.org/10.1016/j.envint.2014.12.007.
Daniel M, Kestens Y, Paquet C. Demographic and urban form correlates of healthful and unhealthful food availability in Montréal, Canada. Can J Public Health = Revue canadienne de sante publique. 2009;100(3):189–93. https://doi.org/10.1007/bf03405538.
Fecht D, Fortunato L, Morley D, Hansell AL, Gulliver J. Associations between urban metrics and mortality rates in England. Environ Health. 2016;15 Suppl 1(Suppl 1):34. https://doi.org/10.1186/s12940-016-0106-3.
Kaplan S, Nielsen TAS, Prato CG. Walking, cycling and the urban form: a Heckman selection model of active travel mode and distance by young adolescents. Article. Transp Res Part D: Transp Environ. 2016;44:55–65. https://doi.org/10.1016/j.trd.2016.02.011.
Li F, Fisher KJ, Brownson RC, Bosworth M. Multilevel modelling of built environment characteristics related to neighbourhood walking activity in older adults. J Epidemiol Community Health. 2005;59(7):558–64. https://doi.org/10.1136/jech.2004.028399.
Lee C. Impacts of urban form on air quality: emissions on the road and concentrations in the US metropolitan areas. Article. J Environ Manag. 2019;246:192–202. https://doi.org/10.1016/j.jenvman.2019.05.146.
Coogan PF, White LF, Adler TJ, Hathaway KM, Palmer JR, Rosenberg L. Prospective study of urban form and physical activity in the Black Women’s Health Study. Am J Epidemiol. 2009;170(9):1105–17. https://doi.org/10.1093/aje/kwp264.
Liang Z, Wei F, Wang Y, et al. The context-dependent effect of urban form on air pollution: a panel data analysis. Article. Remote Sens. 2020;12(11)1793. https://doi.org/10.3390/rs12111793.
She Q, Peng X, Xu Q, et al. Air quality and its response to satellite-derived urban form in the Yangtze River Delta, China. Article. Ecol Indic. 2017;75:297–306. https://doi.org/10.1016/j.ecolind.2016.12.045.
Liu Y, Wu J, Yu D. Disentangling the complex effects of socioeconomic, climatic, and urban form factors on air pollution: a case study of China. Article. Sustainability (Switzerland). 2018;10(3)776. https://doi.org/10.3390/su10030776.
Bechle MJ, Millet DB, Marshall JD. Effects of income and urban form on urban NO2: global evidence from satellites. Article. Environ Sci Technol. 2011;45(11):4914–9. https://doi.org/10.1021/es103866b.
Yang J, Shi B, Zheng Y, Shi Y, Xia G. Urban form and air pollution disperse: key indexes and mitigation strategies. Article. Sustain Cities Soc. 2020;57101955. https://doi.org/10.1016/j.scs.2019.101955.
Stone B Jr. Urban sprawl and air quality in large US cities. Article. J Environ Manag. 2008;86(4):688–98. https://doi.org/10.1016/j.jenvman.2006.12.034.
Mou Y, Song Y, Xu Q, He Q, Hu A. Influence of urban-growth pattern on air quality in China: a study of 338 cities. Article. Int J Environ Res Public Health. 2018;15(9)1805. https://doi.org/10.3390/ijerph15091805.
Zhou C, Li S, Wang S. Examining the impacts of urban form on air pollution in developing countries: a case study of China’s megacities. Article. Int J Environ Res Public Health. 2018;15(8)1565. https://doi.org/10.3390/ijerph15081565.
Liu Y, Wu J, Yu D, Ma Q. The relationship between urban form and air pollution depends on seasonality and city size. Article. Environ Sci Pollut Res. 2018;25(16):15554–67. https://doi.org/10.1007/s11356-018-1743-6.
Wineman JD, Marans RW, Schulz AJ, van der Westhuizen DL, Mentz GB, Max P. Designing healthy neighborhoods: contributions of the built environment to physical activity in Detroit. Article. J Plann Educ Res. 2014;34(2):180–189. https://doi.org/10.1177/0739456X14531829.
McCormack GR, Koohsari MJ, Turley L, et al. Evidence for urban design and public health policy and practice: space syntax metrics and neighborhood walking. Article. Health Place. 2019;102277. https://doi.org/10.1016/j.healthplace.2019.102277.
Smith M, Hosking J, Woodward A, et al. Systematic literature review of built environment effects on physical activity and active transport–an update and new findings on health equity. Int J Behav Nutr Phys Act. 2017;14(1):1–27. https://doi.org/10.1186/s12966-017-0613-9.
Roux AVD. Residential environments and cardiovascular risk. J Urban Health. 2003;80(4):569–89. https://doi.org/10.1093/jurban/jtg065.
Sun W, Bao P, Zhao X, Tang J, Wang L. Road traffic and urban form factors correlated with the incidence of lung cancer in high-density areas: an ecological study in Downtown Shanghai, China. J Urban Health. 2021:1–16. https://doi.org/10.1007/s11524-021-00529-y.
Acknowledgements
This article was extracted from a M.s thesis. The authors acknowledge the Department of Urban design and planning, Tarbiat Modares University for the support of the research.
Author information
Authors and Affiliations
Corresponding author
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Fazeli Dehkordi, Z.S., Khatami, S.M. & Ranjbar, E. The Associations Between Urban Form and Major Non-communicable Diseases: a Systematic Review. J Urban Health 99, 941–958 (2022). https://doi.org/10.1007/s11524-022-00652-4
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11524-022-00652-4