
Abstract
The link between mixed heavy metals (mercury, lead, and cadmium), prediabetes, and type 2 diabetes mellitus (T2DM), especially molecular mechanisms, is poorly understood. Thus, we aimed to identify the association between mixed heavy metals and T2DM and its components using a data set from the Korean National Health and Nutrition Examination Survey. We further analyzed the main molecular mechanisms implicated in T2DM development induced by mixed heavy metals using in-silico analysis. Our findings observed that serum mercury was associated with prediabetes, elevated glucose, and ln2-transformed glucose when using different statistical methods. "AGE-RAGE signaling pathway in diabetic complications", "non-alcoholic fatty liver disease", "metabolic Syndrome X", and three miRNAs (hsa-miR-98-5p, hsa-let-7a-5p, and hsa-miR-34a-5p) were listed as the most important molecular mechanisms related to T2DM development caused by mixed heavy metals. These miRNA sponge structures were created and examined, and they may be beneficial in the treatment of T2DM. The predicted cutoff values for three heavy metal levels linked to T2DM and its components were specifically identified. Our results imply that chronic exposure to heavy metals, particularly mercury, may contribute to the development of T2DM. To understand the changes in the pathophysiology of T2DM brought on by a combination of heavy metals, more research is required.
Graphical abstract

Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Diabetes is a chronic metabolic condition characterized by increased blood glucose levels that cause catastrophic damage to various organs such as the cardiovascular system, kidneys, eyes, and nerves over time. Diabetes affects approximately 422 million people worldwide, the vast majority of whom live in low- and middle-income countries, and is responsible for 1.5 million deaths each year (WHO 2021). Therefore, it is important that risk factors and diabetes be controlled to improve quality of life and minimize the societal disease burden.
Genetics, ethnicity, age, acanthosis nigricans, overweight, obesity, prediabetes, dyslipidemia, physical inactivity, depression, and gestational diabetes have been identified as the risk factors contributing to the development of diabetes. Many of the causes of diabetes, such as being overweight, being obese, and being physical inactive, can be prevented and reversed. Nevertheless, both the incidence and prevalence of diabetes have been gradually increasing, especially type 2 diabetes (T2DM), over the last few decades. This condition can be explained for a variety of reasons. First, as worldwide diets have altered over the previous decades, consumption of energy-dense foods high in fat and free sugars has surged (Duc et al. 2021b; Duc et al. 2021c; Nguyen and Kim 2021; Nguyen et al. 2021a; Nguyen 2022a). Second, the percentage of the aging population is increasing in parallel with the prevalence of non-communicable diseases (Organization 2021). Third, the changing nature of various types of jobs, the increasing availability of transportation, and increased urbanization have all contributed to a reduction in physical exercise (WHO 2021). Last but not least, as global urbanization and industrialization have accelerated, heavy metal exposure has surged (Duc et al. 2021a; Nguyen and Kim 2021; Nguyen et al. 2021a; Nguyen et al. 2021d).
Heavy metals play a vital role in the pathogenesis of obesity, metabolic syndrome, and diabetes (Tinkov et al. 2017a, 2017b; Duc et al. 2021b; Nguyen et al. 2021a; Nguyen et al. 2021c; Nguyen et al. 2021d). Heavy metals (such as cadmium, lead, and mercury) are chronic environmental pollutants; thus, humans are directly exposed to them through eating, drinking, and breathing (Duc et al. 2021a; Nguyen et al. 2021a; Nguyen et al. 2021c; Nguyen et al. 2021d). Therefore, it is unavoidable in reality that prevalent environmental pollutants can be exposed at the same time. However, most previous research concentrated on the effects of a single heavy metal on the etiology of diabetes (Asif 2017; Tinkov et al. 2017a, 2017b; Ji et al. 2021a, 2021b). Single metals should correspond to mixed heavy metals, and diverse statistical approaches are necessary when studying chemical exposure in recent years (Keil Alexander et al. n.d.; Bobb 2015).
The link between heavy metals and diabetes is still controversial. Several studies reported a positive association between heavy metals and diabetes, but others found a negative association or no association between heavy metals and diabetes (Moon 2013; Rotter et al. 2015; Wu et al. 2017; Wang et al. 2018; Ji et al. 2021a, 2021b). Though numerous researchers have attempted to evaluate the link between heavy metals and diabetes, little is known about the molecular mechanisms related to diabetes induced by heavy metals. Therefore, the environmental predisposing factors and molecular mechanisms for diabetes should be documented to help in the prevention and early control of the disease. The present study aimed to (1) identify the relationship between a mixture of serum heavy metals, including cadmium, lead, and mercury, and T2DM and its components in Korean individuals aged ≥18 years and (2) determine the possible molecular mechanisms of mixed heavy metal-induced T2DM.
Material and Methods
Study participants
A data set from the Korean National Health and Nutrition Examination Survey (KNHANES), from 2009-2013 to 2016-2017, was used to examine the association between a mixture of heavy metals and T2DM (Duc et al. 2021b; Welfare 2021). The KNHANES surveys, which are a national surveillance system, used a multi-stage, stratified cluster-sampling method that considered the geographic region, the level of urbanization, the stage of economic growth, and the distribution of age and gender conducted by the Korean Ministry of Health and Welfare and the Korea Centers for Disease Control and Prevention (KCDC). These surveys, which are nationally representative cross-sectional studies, recruit approximately 10,000 participants each year. These surveys include three sections: a health examination, a health interview, and a nutrition survey, which were used to obtain information on health-related behaviors, biochemical and clinical characteristics for dietary intakes and common diseases, socioeconomic status, quality of life, healthcare utilization, and anthropometric measures. These surveys were conducted at a mobile evaluation center or participants’ homes, by trained workers, including health interviewers, doctors, and medical technicians (Kweon et al. 2014). In total, 60,362 individuals participated in these surveys from 2009 to 2017. We removed 13,281 participants less than 18 years old and 41,477 without data, including serum heavy metals (28,783), diabetes (3,474), glycated hemoglobin (HbA1c, 3652), energy intake (893), body mass index (BMI, 17), family history of diabetes (135), and urine cotinine (4,820). Finally, a total of 5,304 participants were eligible for data analysis (Fig. S1) (Nguyen et al. 2021a).
Serum heavy metal measurement
Analyses of mercury, lead, and cadmium have been previously reported (Nguyen, 2021; Nguyen et al, 2021b, e). Briefly, after an eight-hour fast, blood samples were evaluated in accordance with protocol during a medical checkup. Blood samples were rapidly prepared, refrigerated, and sent to the main testing center in cold storage (NeoDin Medical Institute, Seoul, South Korea). All samples underwent 24-hour analyses. Graphite furnace atomic absorption spectrometry (model AAnalyst 600; Perkin Elmer, Turku, Finland) was used to quantify serum lead and cadmium levels. A direct mercury analyzer (type DMA-80 Analyzer; Bergamo, Italy) and gold amalgam (Korea Centers for Disease Control and Prevention) were used to measure the serum total mercury levels. Commercial standards (Lyphochek Whole Blood Metals, Bio-Rad, CA, USA) were used as reference materials for internal quality assurance and control. The limits of detection for these heavy metals were 0.223 μg/dL for lead, 0.05 μg/L for mercury, and 0.087 μg/L for cadmium.
Covariates
Sociodemographic information (such as cotinine levels, age group, etc.,) as well as detailed information on laboratory data were available elsewhere (Duc et al. 2021b; Duc et al. 2021c; Yun et al. 2021). Potential covariates in the present study were applied based on the previous study (Duc et al. 2021a). Continuous variables were energy consumption (kcal), BMI (kg/m2), age (years), and ln2-transformed cotinine levels. Other covariates included: family history of diabetes (yes, no), smoking (non/ex-smoker, current smoker), educational level (≤ middle school, high school, ≥ college), physical activity (yes, no), monthly household incomes (< 2,000, ≥ 2,000 and < 4,000, ≥ 4,000 and < 6,000, ≥ 6,000), sex (males, females).
Outcomes
The HbA1c levels (%) were determined using high performance liquid chromatography-723G7 (Tosoh, Tokyo, Japan). A Hitachi automatic analyzer 7600 was used to measure fasting glucose levels (mg/dL) (Hitachi, Tokyo, Japan). The intra- and inter-assay coefficients of variation for HbA1c were 3.12% and 2.80%, respectively, and 2.93% and 2.41 percent for fasting glucose levels (Nguyen et al. 2021d). T2DM, elevated glucose, and elevated HbA1c were identified according to the American Diabetes Association criteria. Serum HbA1c of ≥6.0% was considered elevated. Elevated fasting glucose was defined as a fasting glucose level of ≥100 mg/dL or the use of a drug to treat elevated fasting glucose. Prediabetes was defined as having a fasting glucose ranging from 100-125 mg/dL, or an HbA1c ranging from 5.7 to 6.4% without a previous diabetes diagnosis. T2DM was defined as having a HbA1c of ≥ 6.5%, fasting plasma glucose of ≥126 mg/dl, or being on anti-diabetic medication (Association 2021).
Statistical analysis
The statistical analysis was performed by using STATA (version 16.0; StataCorp, Texas, USA) and R (version 4.1.0) (Nguyen et al. 2021c; Nguyen 2022a). Heavy metal levels were ln2 transformed in this investigation because the range of heavy metals was right-skewed (Nguyen et al. 2021c; Nguyen 2022b).
Logistic and linear regression approaches
First, we used multivariate logistic regression to compare the higher quartiles to the lowest quartile of studied heavy metals to examine the link between each heavy metal and T2DM and its components (Duc et al. 2021b). Second, we looked at multivariate linear regression using the ln2-transformed levels of each heavy metal and the ln2-transformed glucose, and ln2-HbA1c as continuous outcome variables. Third, we further analyzed how these heavy metals interacted with T2DM and its components. Fourth, we analyzed threshold regression (Duc Nguyen et al. 2022b).
Secondary analysis approaches
The three most popular novel methodologies used to assess the effects of a chemical combination are well known: Bayesian kernel machine regression (BKMR), quantile g-computation (qgcomp), and weighted quantile sum (WQS) regression (Bobb et al. 2015; Renzetti et al. 2016; Keil et al. 2020). However, each approach has a unique set of drawbacks (Duc Nguyen et al. 2022b; Nguyen 2022c; Nguyen 2022d). Thus, we evaluated the impact of mixed heavy metals on diabetes and its components using these approaches to ensure the results are reliable (Nguyen 2022c; Nguyen 2022e).
Weighted quantile sum (WQS) regression model
This approach has previously been reported (Duc et al. 2021a; Nguyen et al. 2021c). In summary, as part of the strategy, the study population was randomly split into a training dataset (40 percent, n = 2,212) and a validation dataset (60 percent, n = 3,182). Bootstrapping was employed to determine empirical weights for each heavy metal in the mixture using the training dataset. In this study, heavy metals with estimated weights greater than 0.333 (1/3) were found to have a significant impact on the WQS score (Duc et al. 2021b). Because the WQS technique predicts that all mixture components will act in the same directionality on T2DM and its components, we developed and examined both a positive and a negative WQS score. gWQS, a R package, was used to do the analysis (Nguyen 2022d).
Quantile G-Computation (qgcomp)
The purpose and process of this technique have been described elsewhere (Duc et al. 2021a; Nguyen et al. 2021c). In brief, the gqcomp.noboot function, which separates all heavy metals into quintiles, gives a positive or negative weight to each heavy metal, and fits a linear model for continuous outcomes using Bayesian variable penalization, was used to assess exposure effects. In the current study, heavy metals with an estimated weight greater than 0.05 were determined to have a significant impact on the gqcomp score. gqcomp.boot was also used to assess the linearity of the overall exposure effect. To represent the joint intervention levels of heavy metal exposure to T2DM and its components, the plot was created using g-computation and bootstrap variance with B up to 200. The analysis was carried out using the qgcomp package.
Bayesian kernel machine regression (BKMR) model
This approach's aim and process have been discussed elsewhere (Duc et al. 2021b; Nguyen et al. 2021c). In this study, a Gaussian kernel function was applied with a component-wise variable technique to set a Gaussian kernel function. After setting the final model with the Markov Chain Monte Carlo sampler for 10,000 iterations, the posterior inclusion probabilities (PIPs) for each heavy metal were measured, and estimations of the exposure-outcome function were established (Duc et al. 2021a). The analysis was carried out using the R package bkmr (Nguyen 2022e).
In silico analysis for mixed heavy metals and T2DM
The purpose of this method and its methodology have been described elsewhere (Nguyen 2022f, 2022g, 2022h). The link between T2DM and mixed heavy metals was determined by using data from the Comparative Toxicogenomics Database (CTD, (http://CTD.mdibl.org) (Duc Nguyen et al. 2022a; Nguyen 2022h, 2022i). The data downloaded on July 21, 2022, was used for the analysis reported in this study. Then, it was determined which genes contributed to the development of T2DM and heavy metal toxicity. We developed a network of overlapping genes activated by the examined heavy metals as well as other relevant genes associated with T2DM using GeneMANIA (http://geneMANIA.org/plug-in/) (Nguyen 2022c). The ToppGeneSuite portal (https://toppgene.cchmc.org) and its ToppFun function (https://toppgene.cchmc.org/enrichment.jsp) were used to connect T2DM-related molecular mechanisms (e.g., diseases, biological processes, and signaling pathways) to heavy metal mixture-induced genes. miRNA-target interaction networks and miRNA sponge structure were constructed and analyzed using MIENTURNET (http://userver.bio.uniroma1.it/apps/mienturnet/), and miRNAsong (http://www.med.muni.cz/histology/miRNAsong), respectively (Licursi et al. 2019; Duc Nguyen et al. 2022a; Nguyen 2022i).
Results
Study participant characteristics
This study comprised 912 adult individuals with T2DM, 2,134 individuals with prediabetes, 1950 individuals with elevated glucose, and 1,222 individuals with elevated HbA1c. Table 1 shows demographic information stratified by the presence or absence of T2DM, elevated glucose, and elevated HbA1c. Participants with T2DM, elevated glucose, and elevated HbA1c were more likely to be older, married, live in rural areas, be unemployed, be less educated, come from low-income families, usually drink, and have a family history of diabetes and dyslipidemia. Also, compared to their counterparts, they had significantly higher body mass index, waist circumference, triglycerides, high-sensitivity C-reaction protein, systolic and diastolic blood pressure, aspartate aminotransferase, and alanine aminotransferase.
Characteristics of heavy metal exposure
Table 2 shows the mean and geometric mean levels stratified by the presence or absence of T2DM, prediabetes, elevated glucose, and elevated HbA1c of three heavy metals. Serum levels of the studied heavy metals were more likely to be higher in subjects with T2DM, prediabetes, elevated glucose, and elevated HbA1c compared with those that did not.
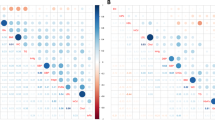
The Pearson correlation coefficients (r) between serum heavy metals and cardiometabolic risk variables are shown in Fig. 1 (P value<0.001, r ranged from -0.36 to 0.85). ln2-transformed fasting glucose and ln2-transformed HbA1c (r= 0.80), body mass index and waist circumference (r= 0.85), and diastolic blood pressure and systolic blood pressure (r= 0.63) all had a strong correlation. The rest of the relationships were weak to moderate. For instance, the link between ln2-transformed serum lead and cadmium (r=0.32) and ln2-transformed serum mercury and cadmium (r =0.14).

Pairwise Pearson correlations among cardiometabolic risk factors and ln2-transformed levels of heavy metals (n = 5,304), KNHANES, Korean, 2009–2017. BMI: body mass index, WC: waist circumference, DBP: diastolic blood pressure, SBP: systolic blood pressure, EN: energy, HDL-C: High-density lipoprotein cholesterol, ln2Glu: ln2-transformed glucose, ln2COT: ln2-transformed cotinine; Chol: cholesterol.
Findings from multivariate logistic and linear regression models
Serum cadmium showed a significant trend (P for trend <0.001) with prediabetes, ln2-transformed glucose, and ln2-transformed HbA1c) in the upper two quartiles. There were significant links between serum mercury, prediabetes, elevated HbA1c, elevated glucose, and ln2-transformed glucose, with a significant trend (P for trend <0.001). Serum lead, on the other hand, was linked to prediabetes and ln2-transformed HbA1c in the fourth quartiles (P for trend <0.001).. Next, we analyzed the relationship between heavy metals and T2DM and its components when the studied heavy metals were considered continuous variables. Serum cadmium was linked to T2DM, elevated glucose, prediabetes, ln2-transformed glucose, and ln2-HbA1c. Prediabetes, elevated glucose, HbA1c, and ln2-glucose were found to be associated with serum mercury. We further investigated how heavy metals interact with T2DM and its components. After adjusting for potential variables, we found an interaction between serum lead and mercury levels and elevated glucose levels, as well as between mixed three heavy metals and prediabetes and elevated glucose levels (Tables S1A and 1B).
Findings from the WQS models
The WQS indices were found to be associated with prediabetes, elevated glucose, and ln2-transformed glucose (Table S2 and Fig. 2A-F). In fully adjusted models, the WQS indexes were found to be associated with prediabetes (OR: 1.92, 95%CI: 1.22–3.01), elevated glucose (OR: 1.86, 95%CI: 1.14–3.02), and ln2-transformed glucose (OR: 1.03, 95%CI: 1.02–1.05). In almost all models, serum mercury had the highest weight. The serum cadmium was then given a medium weight, while the serum lead was given the lightest (Table S3).

WQS model regression index weights for (A) type 2 diabetes (positive weights), (B) prediabetes (positive weights), (C) elevated glucose (positive weights), (D) elevated HbA1c (positive weights), (E) ln2 glucose (positive weights), and (F) ln2 HbA1c (negative weights). Models were adjusted for sex (males, females), BMI (kg/m2), age (years), energy intake (kcal), family history of diabetes (yes, no), physical activity (yes, no), smoking (non/ex-smoker, current smoker), ln2 cotinine (mg/dL), educational level (≤ middle school, high school, ≥ college), monthly household incomes (< 2,000, ≥ 2,000 and < 4,000, ≥ 4,000 and < 6,000, ≥ 6,000).
Findings from the gqcomp models
The gqcomp indices were found to be significantly linked with prediabetes. In the fully adjusted models, a quartile increase in the gpcomp index was significantly related to prediabetes (OR = 1.53, 95%CI: 1.25–1.88) (Table S4). The predicted weights of heavy metals for each gqcomp index, as well as the joint effect of mixed heavy metals on T2DM and its components, are shown in Table S5 and Fig. 3A-F. In almost all models, serum mercury had the largest positive weight, similar to the WQS model. After that, serum cadmium observed a moderately negative weight, while serum Pb observed the lowest weight.


gqcomp model regression index weights and Joint effects (95% CI) of the mixture on (A) type 2 diabetes, (B) prediabetes, (C) elevated glucose, (D) elevated HbA1c, (E) ln2 glucose, and (F) ln2 HbA1c. Models were adjusted for sex (males, females), BMI (kg/m2), age (years), energy intake (kcal), family history of diabetes (yes, no), physical activity (yes, no), smoking (non/ex-smoker, current smoker), ln2 cotinine (mg/dL), educational level (≤ middle school, high school, ≥ college), monthly household incomes (< 2,000, ≥ 2,000 and < 4,000, ≥ 4,000 and < 6,000, ≥ 6,000).
Findings from the BKMR models
In order to further analyze the effects of combining three heavy metals, we applied the BKMR method due to the linearity and interaction limitations of the earlier techniques. In all models in the current study, the PIPs of serum mercury were shown to be greater than those of other heavy metals in all models (Table S6).
Figures 4 A-F show the overall relationships between the mixed heavy metals, T2DM, and its components. When mixed heavy metals were at or above the 60th percentile compared to the 50th percentile, prediabetes, elevated glucose, and ln2-transformed glucose increased considerably, demonstrating significant positive associations with prediabetes, elevated glucose, and ln2-transformed glucose, respectively. Despite the lack of statistical significance between the T2DM, elevated HbA1c, and ln2-transformed HbA1c models, there was an increased and decreased inclination, respectively.

Cumulative effect (95% CI) of the heavy metal mixture on (A) type 2 diabetes, (B) elevated glucose, (C) elevated HbA1c, (D) ln2 glucose, and (E) ln2 HbA1c, when all the heavy metals at particular percentiles were compared to all the chemicals at their 50th percentile. The results were assessed by the BKMR models, adjusted for sex (males, females), BMI (kg/m2), age (years), energy intake (kcal), family history of diabetes (yes, no), physical activity (yes, no), smoking (non/ex-smoker, current smoker), ln2 cotinine (mg/dL), educational level (≤ middle school, high school, ≥ college), monthly household incomes (< 2,000, ≥ 2,000 and < 4,000, ≥ 4,000 and < 6,000, ≥ 6,000).
On the other hand, we investigated the univariate (independently heavy metal) exposure-response functions of T2DM and its components after being exposed to heavy metal (Fig. S2 A-E). Serum mercury, cadmium, and lead revealed growing associations with T2DM and its components at the highest levels when these heavy metals were at their median levels. Three heavy metals were observed to have a positive relationship with prediabetes, elevated glucose, and ln2-transformed glucose, respectively. Furthermore, the investigated heavy metals in this study were found to interact (Fig. S3 A-F). Table 3 presents the results of four distinct statistical models. In these models, we observed that mercury and cadmium had the strongest negative or positive associations.
Molecular mechanisms related to mixed heavy metals and type 2 diabetes
As shown in Table 4A, cadmium, mercury, and lead altered 60, 35, and 39 genes that were involved in the pathogenesis of T2DM, respectively (Table 4A). Eighteen genes were impacted by mixed heavy metals, and this interaction was linked to the development of T2DM (Fig. 5A). The most prominent interactions between T2DM genes were identified as “physical interactions” (32.8%), “co-expressions” (28.9%), and “predicted by the server” (26.2%) (Fig. 5B). "Apoptosis", "AGE-RAGE signaling pathway in diabetic complications", "oxidative stress", and "IL-18 signaling pathway" were key signaling pathways implicated in combined heavy metals and T2DM. "Oxidative stress" and "apoptosis" were found to be the two main biological processes that were related to the etiology of T2DM induced by mixed heavy metals. The most prevalent condition associated with combined heavy metals was "diabetes" (Table 4B).

Key molecular mechanisms implicated in type 2 diabetes induced by mixed heavy metals. Venn diagram for the differentially expressed genes induced by studied heavy metals (A). A network of overlapping genes induced by mixed heavy metals (Pb, Hg, and Cd) was created, as well as 18 type-2-diabetes-related genes (B). miRNA–target interaction network for miRNAs derived from the list of genes associated with type 2 diabetes and the mixed heavy metals (C-D), pink dots represent miRNA targets, blue dots represent target genes (CTD Database (http://CTD.mdibl.org). signaling pathways and diseases related to type 2 diabetes and mixed heavy metals (E-F). miRNA sponge structures for four selected miRNAs (G). FDR: False Discovery Rate.
We next assessed the association between single and mixed heavy metals in the pathophysiology of T2DM. As shown in Fig. S4, cadmium altered two key miRNAs (hsa-miR-155-5p and hsa-miR-34a-5p), lead altered three key miRNAs (hsa-miR-34a-5p, hsa-miR-155a-5p, and hsa-miR-21-5p), whereas mercury altered five key miRNAs (hsa-miR-34a-5p, hsa-miR-98-5p, hsa-let-7a-5p, has-miR-9-5p, and hsa-miR-155-5p). "AGE-RAGE pathway”, "non-alcoholic fatty liver disease”, "gestational diabetes”, and “type 2 diabetes mellitus” were listed as the most important signaling pathways and related diseases induced by cadmium, lead, and mercury (Fig. S5 and Table S7). In terms of mixed heavy metals, the key miRNAs associated with T2DM and mixed heavy metals were identified as hsa-miR-98-5p, hsa-let-7a-5p, and hsa-miR-34a-5p (Fig. 5 C-D). "AGE-RAGE signaling pathway in diabetic complications" and "non-alcoholic fatty liver disease”, "metabolic syndrome X", "gestational diabetes”, and “type 2 diabetes mellitus” were listed as key signaling pathways associated with T2DM and mixed heavy metals (Fig. 5 E-F). The template of the miRNA sponges for these miRNAs was then generated and analyzed (Fig. 5 G and Table S8) (Barta et al. 2016).
Discussion
Four different statistical models were used in this study to explore the impact of heavy metal combinations on T2DM and its components in Korean people aged ≥18 years. We found that serum mercury was the most powerful predictor of T2DM and its components (prediabetes, elevated glucose, elevated HbA1c, ln2-transformed glucose, and ln2-transformed HbA1c) in the generalized linear regression. Prediabetes and elevated glucose interacted with all serum cadmium, mercury, and lead levels. Furthermore, prediabetes, elevated glucose, and ln2-transformed glucose were demonstrated to be influenced by mixed heavy metals, particularly serum mercury, in the QWS and gqcomp models (only for prediabetes). The BKMR model revealed a positive relationship between prediabetes, elevated glucose, ln2-transformed glucose, and serum levels of the heavy metals studied. Prediabetes, elevated glucose, and ln2-transformed glucose were also found to have a significant relationship with overall mixed exposure. Although there was no statistically significant association between overall mixed exposure and T2DM, elevated HbA1c, or ln2-transformed HbA1c, an increasing and decreasing tendency were observed, respectively. These findings imply that long-term exposure to heavy metals, especially mercury, will induce the development of T2DM.
We observed that mercury was the most important heavy metal related to the risk of T2DM, prediabetes, elevated glucose, and elevated HbA1c. This result can be attributed to the consumption of more tainted seafood in Korea, such as crabs, fish, and shellfish, as well as the consumption of tainted water from defunct mines (Choi et al. 2017; Kim et al. 2021; Duc Nguyen et al. 2022b). In the current study, we found that a combination of heavy metals, notably serum mercury, was not significantly related to the prevalence of T2DM in Korean adults, which concurs with the previous studies (Moon 2013; Wu et al. 2017). Moon et al. observed that there was no significant association between serum lead (geometric mean (GM) of 2.47 μg/dL), cadmium (1.16 μg/L), and mercury (4.42 μg/L) and diabetes in Korean adults during 2009-2010 (Moon 2013). A systematic review and meta-analysis of 11 cohort and cross-sectional studies observed that urine and serum cadmium were not linked with an increased risk of T2DM (OR = 1.16; 95% CI = 0.84-1.62) in the general population (Wu et al. 2017). However, our findings were inconsistent with previous research findings. A study in the US population reported a positive association between mixed heavy metals (cadmium (mean 0.37 μg/L), lead (1.32 μg/dL), and mercury (0.93 μg/L)) and the risk of T2DM (Wang et al. 2018). Several cross-sectional studies conducted in China observed that blood cadmium (mean of 1.70 μg/L) was linked to prediabetes (Nie et al. 2016; Chang et al. 2021). A cross-sectional study of Taiwanese adults observed that blood mercury levels (geometric mean of 18.95 ppb (95%CI, 15.66, 22.93)) were linked with T2DM risk (Tsai et al. 2019). Participants in these investigations had lower levels or similar levels of cadmium, lead, and mercury exposure than those in the current study. The findings of this study suggest that low levels of cadmium, lead, and mercury exposure may not be linked with T2DM development. The primary source of exposure, the study's design, the age of the participants, the route of exposure, the length of time they were exposed, the size of the sample, and the location of the study can all be used to explain the significant differences between these studies (Nguyen 2022g, 2022h). Because T2DM is a chronic disease, detecting heavy metals only once may underestimate the true level of exposure and increase the risk of T2DM. The diet or drinks consumed just before the survey could have an impact on the internal heavy metal exposure level. Therefore, a longer assessment of exposure, like evaluating the heavy metals at least twice, would be more important to assess the link between T2DM risk and heavy metals. Having in mind that the cutoff criteria for clinically meaningful exposure levels are necessary, we calculated the cutoff values for exposure levels that are important for T2DM and its components (Table S9).
Interestingly, we observed that the link between prediabetes and elevated glucose was related to mixed heavy metals. According to a meta-analysis review, the risk of diabetes rises above 1 μg/L of serum cadmium levels, whereas the risk of prediabetes rises until it reaches 2 μg/g creatinine, at which point it plateaus (Filippini et al. 2022). A prospective cohort of 3,875 American adults aged 20 to 32 years discovered that high mercury exposure in adolescence can increase the risk of diabetes later in life. Furthermore, higher mercury levels were associated with higher glucose and insulin levels, a lower HOMA of the β-cell function index, and a higher HOMA-IR (He et al. 2013). In an in vivo study, lead exposure can cause prediabetes in obese rats via fasting hyperglycemia and glucose intolerance (Tyrrell et al. 2017). In a case-control study of 45 Nigerian individuals, the authors reported that participants with poor glycemic control had considerably greater cadmium levels than those with good glycemic control (Anetor et al. 2016).
We also found that mixed heavy metals were not significantly related to HbA1c, which was consistent with a previous study. A cross-sectional study of Chinese adults aged ≥ 30 years reported that serum lead (median 5.18 μg/dL), cadmium (0.19 μg/L) were not significantly linked with HbA1c (Cai et al. 2022). However, another cross-sectional study of Taiwanese adults observed a strong positive link between serum lead (mean 17 μg/L) and HbA1c in a non-diabetic population (Chang et al. 2021). It could be explained that low levels of heavy metal exposure may not be linked with HbA1c.
Chemicals, including heavy metals, from the environment are metabolized in the liver and then discharged into the intestines through bile (Klaassen 2013; Duc Nguyen et al. 2022b). Only around 5% of environmental chemicals are eliminated in the feces, while 90–95% could be reabsorbed through the enterohepatic circulation (Dawson 2018). The etiology of T2DM is implicated in a disruption in hepatic glucose homeostasis. Furthermore, elevated serum glucose levels are caused by impaired liver and kidney functions, as well as diminished pancreatic and muscle function. When heavy metals enter the human body, they accumulate in the liver, kidneys, and pancreas, where they disrupt glucose metabolism and its interactions with other metabolic pathways, particularly glycolysis, glycogenesis, and gluconeogenesis, by changing and affecting the specific activity of important enzymes and by damaging the pancreas and adrenal glands. Therefore, heavy metals play an important role in the pathogenesis of T2DM (Javaid et al. 2021).
There is a potential biological link between heavy metals and the development of T2DM. Although the majority of cadmium is deposited in the kidney, chronic exposure has been linked to cadmium accumulation in the pancreas, particularly in the beta islets. Cadmium poisoning can impair the antioxidant system and energy metabolism, as well as cause inflammation and mitochondrial damage in pancreatic beta cells (Buha et al. 2020). Furthermore, cadmium may activate gluconeogenesis through decreased insulin sensitivity by changing glucose transporter expression and increasing the activity of gluconeogenic enzymes, resulting in decreased glucose uptake (Edwards and Ackerman 2016). An elevation in blood glucose and a reduction in insulin levels could be caused by damage to the pancreas (Tinkov et al. 2017a, 2017b). Although the precise mechanism linking mercury to diabetes is uncertain, mercury is a well-known oxidative stress-causing toxin. A literature review found that mercury may cause T2DM by causing hyperglycemia and disrupting pancreatic function through oxidative stress on the mitochondria or stimulation of the c-JunN-terminal kinase signaling pathway (Schumacher and Abbott 2017). An in vivo study revealed that mercury-induced oxidative stress produces apoptosis in cells and in the isolated mouse pancreas, in addition to pancreatic beta-cell failure (Chen et al. 2006b). Another in vivo study observed that mercury could induce the activation of phosphoinositide 3-kinase and the production of reactive oxygen species, causing inhibition of insulin secretion and pancreatic beta-cell dysfunction via the Akt signaling pathway (Chen et al. 2006a). On the other hand, lead can cause oxidative stress, which is a risk factor for T2DM (Fridlyand and Philipson 2006). Lead elevates resting intracellular Ca2+, which could have a direct impact on calcineurin function and, as a result, alter calcineurin-dependent cellular processes like insulin-producing pancreatic beta-cells (Soleimanpour et al. 2010). Lead exposure can also cause increased gluconeogenesis by lowering the inhibitory effect of Rev-erb-alpha on gluconeogenic gene expression (Leff et al. 2018).
As mentioned above, oxidative stress and apoptosis play important roles in the etiology of T2DM. According to our in-silico analysis, the main pathways that mixed heavy metals induce in relation to the development of T2DM are oxidative stress and apoptosis. Furthermore, we observed the “AGE-RAGE signaling pathway in the diabetic complication pathway” was one of the key pathways caused by mixed heavy metals linked with T2DM development. The AGE/RAGE signaling pathway has been extensively researched in a variety of disease conditions, including T2DM. It has been known that AGEs may be a crucial component in the development of diabetes complications. These AGEs can cause an inflammatory response and raise oxidative stress in the body through numerous pathways, which has a significant impact on the onset and worsening of diabetic vascular problems (Rhee and Kim 2018). A literature review reported that through activation of TGF-beta-mediated fibrosis, Nox-1, ERK1/2 pathways, NFkB, and decreased SOD-1 expression, the AGE/RAGE signaling pathway has been linked to oxidative stress associated with diabetes-induced vascular calcification (Kay et al. 2016). On the other hand, the IL-18 signaling pathway, and non-alcoholic fatty liver disease were involved in the pathogenesis of T2DM induced by mixed heavy metals. A case-control study of Bulgarian adults observed that the serum level of IL-18 in T2DM patients was higher than in healthy controls (Zaharieva et al. 2018). In an in vivo study, systemic IL-18 treatment was found to increase diabetes development in young nonobese diabetic mice (Oikawa et al. 2003). T2DM risk in patients with nonalcoholic fatty liver disease is five times higher than in those without (Hazlehurst et al. 2016).
In terms of miRNAs, we observed that hsa-miR-98-5p, hsa-let-7a-5p, and hsa-miR-34a-5p had the highest expression and interactions induced by mixed heavy metals and were related to T2DM development. Khan et al. indicated that miR-98-5p was significantly downregulated in five adult T2DM subjects and that miR-98-5p may stimulate apoptosis and inhibit proliferation by targeting PPP1R15B in keratinocytes (Khan et al. 2020). An in vivo study found the level of miR98 expression in SW480 cells cultured under high glucose conditions was considerably lower than in frequently cultured colon cancer SW480 cells. Colon cancer cell growth and invasion are inhibited by increased expression of miR98. By targeting the target gene IGF1R, miR98 can prevent colon cancer cells from proliferating and invading (Liu et al. 2020). Mononen et al. reported that hsa-let-7a-5p level was linked with glycemic status in Young Finns Study participants (n = 871) (Mononen et al. 2019). Let-7a-5p was also found to be downregulated in diabetic nephropathy by Wang et al., suggesting that it may play a role in diabetic nephropathy pathogenesis through modulating high-mobility group AT-hook 2 expression and the PI3K-AKT signaling pathway (Wang et al. 2019). MiR-34a-5p expression was increased in Zucker diabetic fatty rats fed a high-fat diet. In comparison to Zucker lean rats, the authors suggested that miR-34a-5p could inhibit pancreatic cell proliferation by interacting with the Wnt signaling pathway. MiR-34a-5p was also observed to affect blood glucose levels via regulating insulin secretion via the insulin signaling system (Su et al. 2021). Furthermore, silencing miR-34a-5p in hepatocyte HepG2 cells reduced the formation of cellular triglycerides caused by high glucose + oleic acid/palmitic acid combination (Lee et al. 2022). Having in mind that sponges play an important role in the process of miRNA regulation, we designed and tested a miRNA sponge structure. These miRNA sponges can suppress all seed family members and the entire miRNA cluster, making them potentially useful in T2DM therapy (Barta et al. 2016; Nguyen 2022e, 2022f).
Limitations
To our knowledge, this is the first large-scale study in Korea to investigate the cumulative effects of heavy metals on T2DM and its components in participants aged 18 and older. Our findings were supported by the secondary analyses, which employed three unique mixture modeling methodologies. This study, however, has several drawbacks. First, the cross-sectional technique cannot determine whether heavy metals and T2DM are causally related. Second, a single serum sample was used to assess heavy metal exposure. Thus, the evaluations may not have accurately reflected long-lasting exposure circumstances because T2DM is a long-term illness (Nguyen et al. 2021c; Duc Nguyen et al. 2022b). Third, this study only focused on the mixed effects of three common heavy metals that were available in the KNHANES database; other potential heavy metals that were also related to TD2M (such as arsenic, nickel, chromium, etc.) were not analyzed. Fourth, the in silico toxicogenomic assessment used in the present study to determine the molecular processes involved in the etiology of combined heavy metals and diabetes should primarily be viewed as preliminary screening results. More work (in vivo or in vitro) is required to confirm our findings. The miRNA sponges developed in this study can only be useful in some cases; therefore, these findings should be seen as a precursor to more comprehensive in-vitro and in-vivo laboratory testing (Nguyen 2022g, 2022h). Fifth, even though the CTD database is different from the KNHANES database, the findings from the CTD database partly support the link between heavy metal exposure and T2DM.
Conclusions
The combined effect of heavy metals was found to be substantially associated with prediabetes and elevated glucose levels. The most important component related to prediabetes and elevated glucose was found to be serum mercury, which indicated positive trends. In silico assessment reveal that mixed heavy metals interacted with 18 genes and were linked to T2DM. Among T2DM-related genes, physical interactions were found to be the most common (32.8 percent). “AGE-RAGE signaling pathway in diabetic complications”, "non-alcoholic fatty liver disease," apoptosis, and the “IL-18 signaling pathway”), "type 2 diabetes”, "metabolic Syndrome X", hsa-miR-98-5p, hsa-let-7a-5p, and hsa-miR-34a-5p have been identified as key molecular mechanisms associated with heavy metals and T2DM development. The cutoff thresholds for exposure levels associated with T2DM and its components, in particular, were described. In summary, our findings suggest that long-term exposure to heavy metals, particularly mercury, may play a role in the progression of T2DM.
Availability of data and materials
The datasets examined during this study are available on request at the Korea Centers for Disease Control and Prevention (https://knhanes.kdca.go.kr/knhanes/main.do).
References
Anetor JI, Uche CZ, Ayita EB, Adedapo SK, Adeleye JO, Anetor GO, Akinlade SK (2016) Cadmium Level, Glycemic Control, and Indices of Renal Function in Treated Type II Diabetics: Implications for Polluted Environments. 4
Asif MJC (2017) Role of heavy metals in human health and particularly in respect to diabetic patients. 7: 1.1-1.10
Association AD (2021) Understanding A1C: Diagnosis. Book Understanding A1C: Diagnosis, City
Barta T, Peskova L, Hampl A (2016) miRNAsong: a web-based tool for generation and testing of miRNA sponge constructs in silico. Sci Rep 6:36625
Bobb JF, Valeri L, Claus Henn B, Christiani DC, Wright RO, Mazumdar M, Godleski JJ, Coull BA (2015) Bayesian kernel machine regression for estimating the health effects of multi-pollutant mixtures. Biostatistics 16:493–508
Bobb JF (2015) Bayesian kernel machine regression for estimating the health effects of multi-pollutant mixtures. Biostatistics; 16
Buha A, Đukić-Ćosić D, Ćurčić M, Bulat Z, Antonijević B, Moulis J-M, Goumenou M, Wallace DJT (2020) Emerging links between cadmium exposure and insulin resistance: Human, animal, and cell study data. 8: 63
Cai J, Li Y, Liu S, Liu Q, Min X, Zhang J, Wei Y, Mo X, Lin Y, Tang X et al (2022) Associations between multiple heavy metals exposure and glycated hemoglobin in a Chinese population. Chemosphere 287:132159
Chang C-W, Wang C-W, Wu D-W, Lee W-H, Chen Y-C, Liu Y-H, Li C-H, Tsai C-C, Lin W-Y, Chen S-CJD et al. (2021) Significant association between blood lead (Pb) level and haemoglobin A1c in non-diabetic population. 47: 101233
Chen YW, Huang CF, Tsai KS, Yang RS, Yen CC, Yang CY, Lin-Shiau SY, Liu SH (2006a) Methylmercury induces pancreatic beta-cell apoptosis and dysfunction. Chem Res Toxicol 19:1080–1085
Chen YW, Huang CF, Tsai KS, Yang RS, Yen CC, Yang CY, Lin-Shiau SY, Liu SH (2006b) The role of phosphoinositide 3-kinase/Akt signaling in low-dose mercury-induced mouse pancreatic beta-cell dysfunction in vitro and in vivo. Diabetes 55:1614–1624
Choi W, Kim S, Baek Y-W, Choi K, Lee K, Kim S, Yu SD, Choi K (2017) Exposure to environmental chemicals among Korean adults-updates from the second Korean National Environmental Health Survey (2012–2014). Int J Hyg Environ Health 220:29–35
Dawson PAJPotgt (2018) Bile formation and the enterohepatic circulation. 931-56
Duc HN, Oh H, Kim M-S (2021a) The Effect of Mixture of Heavy Metals on Obesity in Individuals ≥50 Years of Age. Biological Trace Element Research
Duc HN, Oh H, Kim MS (2021b) Effects of Antioxidant Vitamins, Curry Consumption, and Heavy Metal Levels on Metabolic Syndrome with Comorbidities: A Korean Community-Based Cross-Sectional Study. Antioxidants (Basel); 10
Duc HN, Oh H, Yoon IM, Kim M-S (2021c) Association between levels of thiamine intake, diabetes, cardiovascular diseases and depression in Korea: a national cross-sectional study. J Nutrition Sci 10:e31
Duc Nguyen H, Hee Jo W, Hong Minh Hoang N, Kim M-S (2022a) Anti-inflammatory effects of B vitamins protect against tau hyperphosphorylation and cognitive impairment induced by 1,2 diacetyl benzene: An in vitro and in silico study. Int Immunopharmacol 108:108736
Duc Nguyen H, Oh H, Kim M-S (2022b) Association between exposure to chemical mixtures in relation to serum total IgE among adults 19–86 years old. Int Immunopharmacol 102:108428
Edwards J, Ackerman CJCDR (2016) A review of diabetes mellitus and exposure to the environmental toxicant cadmium with an emphasis on likely mechanisms of action. 12: 252-58
Filippini T, Wise LA, Vinceti M (2022) Cadmium exposure and risk of diabetes and prediabetes: A systematic review and dose-response meta-analysis. Environ Int 158:106920
Fridlyand LE, Philipson LH (2006) Reactive species and early manifestation of insulin resistance in type 2 diabetes. Diabetes Obes Metab 8:136–145
Hazlehurst JM, Woods C, Marjot T, Cobbold JF, Tomlinson JW (2016) Non-alcoholic fatty liver disease and diabetes. Metab Clin Exp 65:1096–1108
He K, Xun P, Liu K, Morris S, Reis J, Guallar E (2013) Mercury exposure in young adulthood and incidence of diabetes later in life: the CARDIA Trace Element Study. Diabetes Care 36:1584–1589
Javaid A, Akbar I, Javed H, Khan U, Iftikhar H, Zahra D, Rashid F, Ashfaq UA (2021) Role of Heavy Metals in Diabetes: Mechanisms and Treatment Strategies. Crit Rev Eukaryot Gene Expr 31:65–80
Ji JH, Jin MH, Kang J-H, Lee SI, Lee S, Kim S-H, Oh SY (2021a) Relationship between heavy metal exposure and type 2 diabetes: a large-scale retrospective cohort study using occupational health examinations. BMJ Open 11:e039541–e039e41
Ji JH, Jin MH, Kang JH, Lee SI, Lee S, Kim SH, Oh SY (2021b) Relationship between heavy metal exposure and type 2 diabetes: a large-scale retrospective cohort study using occupational health examinations. BMJ Open 11:e039541
Kay AM, Simpson CL, Stewart JA Jr (2016) The Role of AGE/RAGE Signaling in Diabetes-Mediated Vascular Calcification. J Diabetes Res 2016:6809703–6809703
Keil Alexander P, Buckley Jessie P, O’Brien Katie M, Ferguson Kelly K, Zhao S, White AJ (n.d.) A Quantile-Based g-Computation Approach to Addressing the Effects of Exposure Mixtures. Environ Health Perspect 128:047004
Keil AP, Buckley JP, O’Brien KM, Ferguson KK, Zhao S, White AJJEhp (2020) A quantile-based g-computation approach to addressing the effects of exposure mixtures. 128: 047004
Khan R, Kadamkode V, Kesharwani D, Purkayastha S, Banerjee G, Datta M (2020) Circulatory miR-98-5p levels are deregulated during diabetes and it inhibits proliferation and promotes apoptosis by targeting PPP1R15B in keratinocytes. RNA Biol 17:188–201
Kim DW, Ock J, Moon KW, Park CH (2021) Association between Pb, Cd, and Hg Exposure and Liver Injury among Korean Adults. Intl J Environ Res Public Health 18
Klaassen CD (2013) Casarett and Doull's toxicology: the basic science of poisons: McGraw-Hill New York
Kweon S, Kim Y, Jang MJ, Kim Y, Kim K, Choi S, Chun C, Khang YH, Oh K (2014) Data resource profile: the Korea National Health and Nutrition Examination Survey (KNHANES). Int J Epidemiol 43:69–77
Lee A-T, Yang M-Y, Lee Y-J, Yang T-W, Wang C-C, Wang C-J (2022) Gallic Acid Improves Diabetic Steatosis by Downregulating MicroRNA-34a-5p through Targeting NFE2L2 Expression in High-Fat Diet-Fed db/db Mice. Antioxidants; 11
Leff T, Stemmer P, Tyrrell J, Jog R (2018) Diabetes and Exposure to Environmental Lead (Pb). Toxics 6:54
Licursi V, Conte F, Fiscon G, Paci P (2019) MIENTURNET: an interactive web tool for microRNA-target enrichment and network-based analysis. BMC Bioinformatics 20:545
Liu S, Zhou Y, Zhou Y, Wang J, Ji R (2020) Mechanism of miR-98 inhibiting tumor proliferation and invasion by targeting IGF1R in diabetic patients combined with colon cancer. Oncol Lett 20:1719–1726
Mononen N, Lyytikäinen L-P, Seppälä I, Mishra PP, Juonala M, Waldenberger M, Klopp N, Illig T, Leiviskä J, Loo B-M et al (2019) Whole blood microRNA levels associate with glycemic status and correlate with target mRNAs in pathways important to type 2 diabetes. Sci Rep 9:8887–8887
Moon SS (2013) Association of lead, mercury and cadmium with diabetes in the Korean population: the Korea National Health and Nutrition Examination Survey (KNHANES) 2009-2010. Diabet Med 30:e143–e148
Nguyen HD, Kim M-S (2021) Effects of heavy metal, vitamin, and curry consumption on metabolic syndrome during menopause: a Korean community-based cross-sectional study. J Menopause 28:1
Nguyen HD (2022a) Cadmium, lead, and mercury mixtures interact with non-alcoholic fatty liver diseases. Environ Pollut 309:119780
Nguyen HD (2022b) Effects of chemical mixtures on liver function biomarkers in the Korean adult population: thresholds and molecular mechanisms for non-alcoholic fatty liver disease involved. Environ Sci Pollut Res
Nguyen HD . (2022c) Effects of heavy metals on cardiovascular diseases in pre and post-menopausal women: from big data to molecular mechanism involved. Environ Sci Pollut Res
Nguyen HD (2022d) Exposure to a mixture of heavy metals induces cognitive impairment: genes and microRNAs involved. Toxicology; 153164
Nguyen HD (2022e) The protective effects of curcumin on metabolic syndrome and its components: In-silico analysis for genes, transcription factors, and microRNAs involved. Arch Biochem Biophys 727:109326
Nguyen HD (2022f) The protective effects of curcumin on metabolic syndrome and its components: In-silico analysis for genes, transcription factors, and microRNAs involved. Arch Biochem Biophys 109326
Nguyen HD (2022g) The role of mixed B vitamin intakes on cognitive performance: Modeling, genes and miRNAs involved. J Psychiatr Res 152:38–56
Nguyen HD (2022h) The effects of chemical mixtures on lipid profiles in the Korean adult population: threshold and molecular mechanisms for dyslipidemia involved. Environ Sci Pollut Res
Nguyen HD (2022i) Mixtures modeling identifies vitamin B1 and B3 intakes associated with depression. J Affect Disord 301:68–80
Nguyen HD (2021) Higher intakes of nutrients are linked with a lower risk of cardiovascular diseases, type 2 diabetes mellitus, arthritis, and depression among Korean adults. Nutrition Research
Nguyen HD, Oh H, Hoang NHM, Kim M-S (2021a) Association between heavy metals, high-sensitivity C-reaction protein and 10-year risk of cardiovascular diseases among adult Korean population. Sci Rep 11:14664
Nguyen HD, Oh H, Hoang NHM, Kim MS (2021b) Association between heavy metals, high-sensitivity C-reaction protein and 10-year risk of cardiovascular diseases among adult Korean population. Sci Rep 11
Nguyen HD, Oh H, Jo WH, Hoang NHM, Kim MS (2021c) Mixtures modeling identifies heavy metals and pyrethroid insecticide metabolites associated with obesity. Environ Sci Pollut Res Intl
Nguyen HD, Oh H, Kim M-S (2021d) Effects of heavy metals on hypertension during menopause: a Korean community-based cross-sectional study. Menopause 28
Nguyen HD, Oh H, Kim MS (2021e) Effects of heavy metals on hypertension during menopause: a Korean community-based cross-sectional study. Menopause
Nie X, Wang N, Chen Y, Chen C, Han B, Zhu C, Chen Y, Xia F, Cang Z, Lu MJES et al. (2016) Blood cadmium in Chinese adults and its relationships with diabetes and obesity. 23: 18714-23
Oikawa Y, Shimada A, Kasuga A, Morimoto J, Osaki T, Tahara H, Miyazaki T, Tashiro F, Yamato E, Miyazaki J-i et al (2003) Systemic Administration of IL-18 Promotes Diabetes Development in Young Nonobese Diabetic Mice. J Immunol 171:5865
Organization WH (2021) Ageing and health. Book Ageing and health, City
Renzetti S, Curtin P, Just A, Gennings CJRpv (2016) Gwqs: Generalized weighted quantile sum regression. 1
Rhee SY, Kim YS (2018) The Role of Advanced Glycation End Products in Diabetic Vascular Complications. dmj 42:188–195
Rotter I, Kosik-Bogacka D, Dołęgowska B, Safranow K, Lubkowska A, Laszczyńska M (2015) Relationship between the concentrations of heavy metals and bioelements in aging men with metabolic syndrome. Int J Environ Res Public Health 12:3944–3961
Schumacher L, Abbott LC (2017) Effects of methyl mercury exposure on pancreatic beta cell development and function. J Appl Toxicol 37:4–12
Soleimanpour SA, Crutchlow MF, Ferrari AM, Raum JC, Groff DN, Rankin MM, Liu C, De León DD, Naji A, Kushner JA et al (2010) Calcineurin signaling regulates human islet {beta}-cell survival. J Biol Chem 285:40050–40059
Su T, Hou J, Liu T, Dai P, Qin L, Ding L, Hu Y, Guo X (2021) MiR-34a-5p and miR-452-5p: The Novel Regulators of Pancreatic Endocrine Dysfunction in Diabetic Zucker Rats? Int J Med Sci 18:3171–3181
Tinkov AA, Filippini T, Ajsuvakova OP, Aaseth J, Gluhcheva YG, Ivanova JM, Bjørklund G, Skalnaya MG, Gatiatulina ER, Popova EV (2017a) The role of cadmium in obesity and diabetes. Sci Total Environ 601:741–755
Tinkov AA, Filippini T, Ajsuvakova OP, Aaseth J, Gluhcheva YG, Ivanova JM, Bjørklund G, Skalnaya MG, Gatiatulina ER, Popova EVJSoTTE (2017b) The role of cadmium in obesity and diabetes. 601: 741-55
Tsai T-L, Kuo C-C, Pan W-H, Wu T-N, Lin P, Wang S-L (2019) Type 2 diabetes occurrence and mercury exposure – From the National Nutrition and Health Survey in Taiwan. Environ Int 126:260–267
Tyrrell JB, Hafida S, Stemmer P, Adhami A, Leff T (2017) Lead (Pb) exposure promotes diabetes in obese rodents. J Trace Elem Med Biol 39:221–226
Wang T, Zhu H, Yang S, Fei X (2019) Let-7a-5p may participate in the pathogenesis of diabetic nephropathy through targeting HMGA2. Mol Med Rep 19:4229–4237
Wang X, Mukherjee B, Park SK (2018) Associations of cumulative exposure to heavy metal mixtures with obesity and its comorbidities among U.S. adults in NHANES 2003-2014. Environ Int 121:683–694
Welfare KMoHa (2021) Korea National Health & Nutrition Examination Survey. Book Korea National Health & Nutrition Examination Survey, City
WHO (2021) Obesity. Available at: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight. Accessed 1 Aug 2022
Wu M, Song J, Zhu C, Wang Y, Yin X, Huang G, Zhao K, Zhu J, Duan Z, Su L (2017) Association between cadmium exposure and diabetes mellitus risk: a prisma-compliant systematic review and meta-analysis. Oncotarget 8:113129–113141
Yun S, Nguyen HD, Park JS, Oh C, Kim MS (2021) The association between the metabolic syndrome and iron status in pre- and postmenopausal women: Korean National Health and Nutrition Examination Survey (KNHANES) in 2012. Br J Nutr:1–11
Zaharieva E, Kamenov Z, Velikova T, Tsakova A, El-Darawish Y, Okamura H (2018) Interleukin-18 serum level is elevated in type 2 diabetes and latent autoimmune diabetes. Endocr Connect 7:179–185
Acknowledgements
The authors thank all research staff that contributed to the data collection.
Author information
Authors and Affiliations
Contributions
Hai Duc Nguyen: Conceptualization, Methodology, Formal analysis, Investigation, Resources, Data curation, Writing – original draft, Writing – review & editing, Visualization.
Corresponding author
Ethics declarations
Ethical Approval
The KNHANES investigation commission accepted this study (IRB Approval numbers: 2009-01CON-03-2C, 2010-02CON-21-C, 2011-02CON-06-C, 2012-01EXP-01-2C, 2013-07CON-03-4C, 2013-12EXP-03-5C). KNHANES was excluded from assessment on research ethics under the Bioethics and Safety Act from 2016 to 2017.
Consent to Participate
All KNHANES participants submitted written informed permission prior to the investigations, which were carried out by the Korea Centers for Disease Control and Prevention's Health and Nutrition Examination Department.
Consent to Publish
Not applicable.
Competing interests
The authors have no conflict of interest to declare.
Additional information
Responsible Editor: Lotfi Aleya
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Highlights
• Mixed chemicals were related to the risk of prediabetes and elevated glucose.
• 18 genes were related to mixed chemicals and T2DM development.
• Key molecular mechanisms affected by T2DM-related combined chemicals were described.
• Chemicals’ cutoff thresholds related to the risk of T2DM were provided.
• miRNAs implicated in T2DM development were reported.
Supplementary Information
ESM 1
(DOCX 3748 kb)
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Nguyen, H.D. An evaluation of the effects of mixed heavy metals on prediabetes and type 2 diabetes: epidemiological and toxicogenomic analysis. Environ Sci Pollut Res 30, 82437–82457 (2023). https://doi.org/10.1007/s11356-023-28037-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11356-023-28037-3