
Abstract
PM2.5 pollution exposure is the leading cause of disease burden globally, especially in low- and middle-income countries, including Vietnam. Therefore, economic damage in this context must be quantified. Long An province in the Southern Key Economic (SKE) region was selected as a research area. This study aimed to evaluate PM2.5-related human health effects causing early deaths attributable to respiratory, cardiovascular, and circulatory diseases in all ages and genders. Health end-points and health impact estimation, economic loss model, groups of PM2.5 concentration data, data of exposed population, data of baseline premature mortality rate, and data of health impact functions were used. Hourly PM2.5 concentration data sets were generated specifically using the coupled Weather Research and Forecasting Model (WRF)/Community Multiscale Air Quality Modelling System (CMAQ) models. Daily PM2.5 pollution levels considered mainly in the dry season (from January to April 2018) resulted in 12.9 (95% CI − 0.6; 18.7) all-cause premature deaths per 100,000 population, of which 7.8 (95% CI 1.1; 7.1), 1.5 (95% CI − 0.2; 3.1), and 3.6 (95% CI − 1.5; 8.5) were due to respiratory diseases (RDs; 60.54%), cardiovascular diseases (CVDs; 11.81%), and circulatory system diseases (CSDs; 27.65%) per 100,000 population, respectively. The total economic losses due to acute PM2.5 exposure-related premature mortality cases reached 62.0 (95% CI − 2.7; 89.6) billion VND, equivalent to 8.3 (95% CI − 0.4; 12.0) million USD. The study outcomes contributed remarkably to the generation and development of data sources for effectively managing ambient air quality in Long An.
Similar content being viewed by others
Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
PM2.5 is a term used to refer to particulate matter with kinetic diameters less than or equal to 2.5 µm (Lei Chen et al. 2020a, b; Ha Chi and Kim Oanh 2021; Toledo et al. 2018), which is considered an important parameter in assessing the level of air pollution (Huy et al. 2018). PM2.5 concentrations in Vietnam are often significantly higher than in many other cities of Europe and the United States (Gehrig & Buchmann 2003; Harrison et al. 2012; Levy and Hanna 2011), which indicates that Vietnamese people are breathing in air with high levels of pollutants (Hien et al. 2019).
According to data sources from AirNow (https://www.airnow.gov/), the 2016 annual mean PM2.5 concentration in Hanoi City reached 50.5 µg/m3, which was double the Vietnamese National Ambient Air Quality Standard (NAAQS). Furthermore, this annual average PM2.5 concentration level was five times higher than the threshold recommended in the World Health Organization Air Quality Guidelines (WHO Guidelines) updated in 2005 for PM2.5 (Thuy et al. 2018). By 2019, Hanoi City had surpassed Beijing City in the ranking of global capitals for PM2.5 pollution and was also the most polluted city in Southeast Asia (excluding Indonesia) (IQAir, 2020). Meanwhile, the 2016 annual average PM2.5 concentration was 29.6 µg/m3 in Ho Chi Minh City (HCMC), which exceeded the corresponding thresholds in the NAAQS and WHO Guidelines by 1.2 and 3.0 times, respectively (Thu et al. 2018). In 2017, there were approximately 222 out of 365 days for which PM2.5 levels in HCMC exceeded the 24-h mean threshold in the WHO Guidelines (25 µg/m3) (Thu et al. 2018).
PM2.5 pollution exposure has been shown to be the leading cause of the global burden of disease (Gao et al. 2021; Ke et al. 2022; Xing et al. 2021), especially in low and middle income countries (Forouzanfar et al. 2016; Nhung et al. 2018; Stanaway et al. 2018). Several epidemiological studies have been carried out in Vietnam to investigate the relationship between PM2.5 levels and the risk of hospitalisation for children in Hanoi City (Luong et al. 2017; Nhung et al. 2013, 2019) and HCMC (Luong et al. 2020). A case study by Nhung et al. (2013) showed an increased risk of hospitalization for pneumonia by approximately 5.3% (95% CI 1.9; 8.8) and 6.3% (95% CI 1.1; 11.7) in children aged 0–117 years and 1–5 years, respectively, with an increase in the interquartile range (39.4 µg/m3) of PM2.5. Luong et al. (2017, 2020) reported that each 10 µg/m3 increase in PM2.5 concentration was associated with an increased risk of hospitalisation for respiratory illness in children under 5 years of age in Hanoi City, with approximately 2.3% (95% CI 1.2; 3.1) and 3.51% (95% CI 0.96; 6.12) acute lower respiratory tract infections in children in HCMC. Furthermore, short-term exposure to high concentration of PM2.5 is associated with an increased risk of premature death in humans (Cohen et al. 2017; Landrigan et al. 2018; Lelieveld et al. 2015). Specifically, for every 10 µg/m3 increase in PM2.5, there is a direct increase in mortality rates from lung cancer and from cancer of the respiratory system by 0.07 (95% CI 0.004; 0.010) per 10,000 population and 0.08 (95% CI 0.005; 0.011) per 10,000 population in HCMC (Vien et al. 2021). According to an estimate by Dang et al. (2021) PM2.5 directly caused 327 deaths from cardiovascular disease in HCMC, accounting for 6.4% of cardiovascular deaths (327/5,134) and 1.1% of all-cause deaths (327/29,173) in 2018. Furthermore, previous studies have reported that Vietnam’s economic losses due to air pollution ranged from 10.8 to 13.2 billion USD per year, which contributed to around 5% of the Vietnamese gross domestic product (GDP) (IQAir, 2020). Specifically, economic losses due to air pollution in HCMC reached up to 125.46 million USD in 2018, accounting for 0.052% of Vietnam’s GDP (Dang et al. 2021).
Vietnam is facing the problem of significant PM2.5 risks, but there is still a lack of in-depth, interdisciplinary research on this topic. The objective of this study was to estimate the public health impacts of PM2.5 pollution from premature deaths caused due to respiratory, cardiovascular, and circulatory diseases in all populations and age and sex groups. On this basis, the related preliminary economic loss impacts were quantified.
The 24-h average PM2.5 pollution in the dry season (from January to April 2018) with a spatio-temporal resolution of 9 × 9 km grid obtained from the Weather Research and Forecasting Model (WRF)/Community Multiscale Air Quality Modelling System (CMAQ) was used in this study. Based on results from periodic manual monitoring studies carried out by the Department of Natural Resources and Environment of Long An from 2018 to 2021, the report on the environmental status of Long An from 2016 to 2020 (Long An DNRE 2020), and the research results of Bui et al. (2022), the concentration of PM2.5 in the dry season was always much higher than in the wet season. Conversely, the PM2.5 concentration in the wet season from 2016 to 2021 was continuously lower than the threshold value of NAAQS (known as QCVN 05:2013/BTNMT). Furthermore, unfavorable climatic conditions during the dry season in Vietnam have exacerbated the issue of PM2.5 pollution (Thu et al. 2018). In particular, calm periods, low planetary boundary layer (PBL) levels, frequent daytime temperature inversions, and low precipitation have reduced the diffusion of PM2.5 pollutant precursors, unable to escape to high altitudes and transported far away from other areas. This caused the concentration of PM2.5 to increase significantly in the dry season. Moreover, during the dry season, hot weather and prolonged high temperatures (or heat waves) can lead to hazardous air quality situations. Therefore, the dry season was the time of significant PM2.5 pollution in Long An and is one of the most urgent issues that need to be evaluated to have a basis for formulating future mitigation measures. After that, the Benefits Mapping and Analysis Program-Community Edition (BenMAP-CE) model was applied to estimate public health impacts. These studies were carried out in Long An Province, one of the typical provinces in the SKE region.
Materials and Methods
Study Area
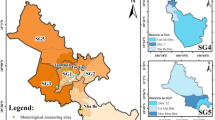
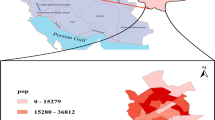
Information and data describing Long An province are provided in Figs. 1 and 2. In particular, Fig. 1 presents the geographical location of the study area within the Mekong Delta region (MDR) in Vietnam and the population size in each district/city of Long An. Figure 2A shows the structure of the population size (A1) and area (A2) in each district/city of Long An. Figure 2B reports the Provincial Competitiveness Index (PCI) values of Long An and other provinces/cities in MDR from 2008 to 2019. Long An is considered the gateway connecting MDR with southeast provinces in Vietnam and is located in both the SKE region and MDR (Fig. 1). The total area of Long An is approximately 4,495 km2 (Long An Provincial Statistics Office 2021); Tan An Town is the smallest with approximately 82 km2 (accounting for 1.82% of the province) of area, whereas Tan Hung District is the largest with approximately 502 km2 (contributing to 11.17%) of area, as shown in Fig. 2-A (A2). By 2018, the population of Long An was 1,678,929 people, contributing to 9% of the MDR’s population (GSO 2019; Long An Provincial Statistics Office 2021), as shown in Fig. 2-A (A1). The economic growth rate of Long An is fast, and there are prominent improvements in several essential indicators of the quality of economic growth, such as shifting the economic structure in a positive direction, deepening international economic integration, and improving the quality of life (Fan et al. 2019; Khanh 2020). Moreover, the gross regional domestic product of Long An reached roughly 78 trillion VND in 2018, with an economic growth rate of 10.36% compared to that in 2017 (9.53%) (GSO 2019). Between 2008 and 2019, the PCI scores of Long An ranged from 59.36 to 68.82 (average 63.70) (Malesky et al. 2020; Vietnam VCCI, 2021), as shown in Fig. 2-B (diagrams (B1) and (B2)). These PCI values reflect the private sector development and improvement in the socio-economic status of Long An. Overall, there are six levels to assess PCI ranking: the ranking scores of very low, low, mid-low, mid-high, high, and excellent levels are 0.0–58.0, 58.0–61.0, 61.0–63.5, 63.5–66.5, 66.5–70.0, and 70.0–100.0, respectively (Vietnam VCCI, 2021). Long An province’s PCI scores continuously achieved high levels from 2014 to 2019. Specifically, the PCI scores ranked second out of thirteen provinces of the MDR in 2014, 2015, 2017, and 2018 (diagram (B3) in Fig. 2-B) (Malesky et al. 2020). The 2018 PCI score of Long An was notably third among all provinces/cities in Vietnam (Malesky et al. 2020).

The geographical location of the study area – Long An province

Description of socio-economic characteristics of Long An province: a the structure of the population size and natural area size by each district/city, and b PCI values of MDR’s provinces from 2008 to 2019
Models
Health Endpoints and Health Impact Estimation
Short-term direct exposure to PM2.5 pollution is considered one of the major risk factors for respiratory diseases (RDs), including lung cancer, cardiovascular diseases (CVDs), and other circulatory system diseases (CSDs) (Kampa and Castanas 2008). This health problem is one of the leading causes of premature death and is defined as the health endpoint (Sacks et al. 2018). Further, following the basis of the International Classification of Diseases, 10th Revision and excluding circumstances that may overlap with other health effects (ICD-10) (ICD-10, 2016), these diseases are identified as all-cause respiratory diseases [I00-I99, excluding I88] and all-cause other circulatory system diseases [I98.8]. Many studies have demonstrated that premature mortality accounts for the highest proportion (up to about 85%) of all forms of health loss due to PM2.5 exposure (Guan et al. 2019; Quan and Shiqiu 2015; Xie et al. 2016). Therefore, the scope of this study was to assess the number of premature deaths (all causes) of the three diseases mentioned above (RDs, CVDs, and CSDs) related to PM2.5 exposure. Estimates of health losses due to short-term exposure to PM2.5 pollution were developed based on the theoretical basis of the Environmental Benefits Mapping and Analysis Program (BenMAP) model (Sacks et al. 2018), which is similar to several previous studies (Li Chen et al. 2017a, b; Linh Nguyen et al. 2022; Sacks et al. 2018) and our own published studies (Bui et al. 2020, 2021; Le Khanh et al. 2022) applying the following Eqs. (1) and (2):
where \(HL_{Dist/City/Town} (C)\) is the total loss of public health (total number of premature deaths) related to PM2.5 pollution; specifically Dist/City/Town are districts in Long An province (Table S1). In Eqs. (1) and (2), i is the type of health damage considered; \(S_{Dist/City/Town}\) is the percentage of days heavily polluted with PM2.5 during the review period in the dry season of 2018, in the districts, cities, and towns in Long An province; \(P_{Dist/City/Town}\) is the background mortality rate for damage type i; and \(BM_{Dist/City/Town,i}\) are the health risk values for each type of health loss i. HR (health risk) values usually have a nonlinear relationship for high levels of PM2.5 pollution (Hoek et al. 2013) and are calculated according to Eq. (2) (Burnett et al. 2014; F. Lu et al. 2015; Xie et al. 2016):
where, \(\beta_{i}\) is the coefficient of the exposure–response for health damage type i, where \(\beta_{i}\), \(\beta_{i,lowerbound}\) (lower bound), and \(\beta_{i,upperbound}\) (upper bound) (with a confidence level of 95% CI) are determined through relative risk (RR) values (Cai et al. 2019; C. Chen et al. 2018; Ferreira et al. 2016; Huang et al. 2012; Kan et al. 2007; Nascimento et al. 2017; Orellano et al. 2020; Qu et al. 2018; Sui et al. 2021); \(C_{Dist/City/Town}\) is the 24-h average, \(C_{0}\) is the PM2.5 concentration level of the days; is the average 24-h threshold of PM2.5 concentration that is not harmful to human health. In this study \(C_{0}\) = 50 µg/m3 according to the Vietnamese National Ambient Air Quality Standard (NAAQS), known as the standard threshold of QCVN 05:2013/BTNTMT. The process of estimating the coefficients of the exposure-interaction functions (\(\beta_{i}\), \(\beta_{i,lowerbound}\), and \(\beta_{i,upperbound}\)) is performed in a manner similar to that described in the studies by Bui et al. (2021); Li Chen et al. (2017a, b); and Le Khanh et al. (2022).
Modelling Changes in PM2.5 Concentration Distributions
The CMAQ simulation is a modern scientific method widely used today, helping to analyse and evaluate physical and chemical processes to determine the transport, formation, and deposition of PM2.5 (Luecken et al. 2019; Ring et al. 2018). In this study, the Weather Research and Forecasting (WRF) model version.3.8 (Byun and Schere 2006; Skamarock et al. 2008) and CMAQ air quality model version 5.2.1 (Borge et al. 2014; Hu et al. 2015; Lang et al. 2017) were used to simulate the distribution of PM2.5 concentrations over the study area. The selected simulation period was the dry season period of 2018, from 00:00 local standard time (LST) of January 1, 2018 to 23:00 local standard time (LST) of the following day April 30, 2018. The dates in the dry season were selected because the measurement results and publications on public health in Vietnam were published for this period (Hien et al. 2019; Long An DNRE 2020; Thu et al. 2018; Thuy et al. 2018). Local environmental agencies warned that pollution levels exceeding NAAQS on days in the dry season were higher than those in the wet season (from May to November). To focus the analysis and evaluate only the impact caused by local pollutants, the zero-out emission method was applied during the development of emission data for the CMAQ simulations (Chen et al. 2017a, b; Pitiranggon et al. 2021; Zhang et al. 2021). In particular, the input emission data for CMAQ simulations were turned off for the anthropogenic emissions of PM2.5 precursors of all grid cells out of Long An province. Based on the inventory of emission sources, primary emissions of PM2.5 and precursor species of PM2.5 were estimated and spatially distributed over the entire study area. The effectiveness of simulating PM2.5 concentration from the CMAQ model has also been validated at the measurement locations (Table S2) through statistical indicators of normalised mean bias (NMB), normalised mean gross error (NME), and correlation coefficient (COR) (Emery et al. 2017), all of which ensure the applicable conditions. NMB ranged from − 3.17 to 3.88%, NME from 3.79 to 10.53%, and COR from 0.91 to 0.97 under conditions including NMB < ± 30%, NME < 50%, and COR > 0.40 (Eder and Yu 2006; Morris et al. 2005) (Table S3).
To generate a dataset about short-term exposure levels for each district/city/town (\(C_{Dist/City/Town}\)) in Long An, daily mean PM2.5 concentration levels were estimated by the ArcGIS 10.4.1 tool based on grid cell-based hourly PM2.5 results from CMAQ simulations for the 2018 dry season. The \(C_{Dist/City/Town}\) from January to April 2018 in this study area is considered a crucial input parameter, which is decisive for the assessment of human health effects and economic losses using public health damage models.
Economic Loss Model
The Value of a Statistical Life (VSL) represents an economic value used to quantify how well a group of people would pay to mitigate the risk of premature death in a population (Persson et al. 2001; Viscusi and Aldy 2003; Yin et al. 2017a, b). It is one of the simplest approaches to assess the economic impact of health losses by multiplying the number of premature deaths with a calculated locally determined VSL (Bayat et al. 2019). In this study, the selected value of VSL in 2018 as the unit economic value of health effects was obtained from research conducted by Bui et al. (2021) as well as Le Khanh et al. (2022). Values were adjusted based on purchasing power parity (PPP), in Eq. (3), according to the “Benefit-Transfer Approach” (Hammitt and Robinson 2011; Johnson et al. 2015; Kim et al. 2019; Narain and Sall 2016). In 2018, the VSL value of the study area was determined as VND 4,788.95 million (approximately USD 0.642 million). Furthermore, based on the assessment of losses of various types of health damage, the total Economic Health Losses (EHL) (in equation [4]) due to short-term exposure to PM2.5 was assessed according to the economic value model for health loss (Ding et al. 2016; X. Lu et al. 2019; J. Wang et al. 2015a, b; H. Yin et al. 2017a, b):
where \(VSL_{VN}\) is the value of Vietnam’s VSL in USD; \(VSL_{OECD}\) is the mean baseline VSL estimated from sample WTP studies in OECD countries; \(Y_{VN}\) is GDP per capita based on Vietnam's PPP in USD; and \(Y_{OECD}\) is the GDP per capita base model of the OECD country group based on PPP in USD. In Eq. (3), e is the income volatility coefficient of VSL, which is chosen to be 1.3, to reflect the significant disparity between Vietnam and developed countries in the OECD group in terms of income levels (L. T. Bui et al. 2020, 2021; OECD 2012). \(EHL_{{_{Dist/City/Town} }} (C)\) are the economic values of the public health loss (early death) from average daily exposure to PM2.5 pollution, also known as the health loss economic value for the districts/Cities/Towns of the study area, respectively; and \(VSL_{{_{Dist/City/Town} }}\) is the statistical life value of the districts/Cities/Towns, respectively, of the study area that the public is willing to pay to minimise the risk of premature death. All quantified health loss values were estimated and converted to monetary equivalents in 2018 (VND and USD).
Data
Population Exposure Data
The impact of short-term PM2.5 pollution on people’s health in the study area of the entire Long An province was analysed and evaluated; therefore, size of the exposed population in Long An province in 2018 was calculated. Population data were obtained from the Long An Statistical Yearbook for the year 2020 (Long An Provincial Statistics Office 2021). In this study, calculations were performed for all age- and sex-groups. The 24-h population-weighted average PM2.5 concentration level (\(C_{Dist/City/Town}{\prime}\)) for all districts/Cities/Towns combined in 2018 of the study area was also transformed by Eq. (5) (Fann et al. 2018):
where \(C_{Dist/City/Town}\) is the 24-h average PM2.5 concentration level in each district/city/town of Long An province in the dry season of 2018, \(P_{Dist/City/Town}\) is the population of the districts/Cities/Towns of the province, respectively, and P is the total population of the entire Long An province in 2018.
Data of Baseline Premature Mortality Rate
The baseline mortality rate (\(BM_{Dist/City/Town,i}\)) is the probability that the population of an area is at risk of premature death from all causes within a given period (Shang et al. 2013). The dataset \(BM_{Dist/City/Town,i}\) of each type of health loss in 2018 for all gender and age groups in the study area was collected from the National Health Statistics Yearbook period 2017–2020 (https://moh.gov.vn/), as announced by the Ministry of Health of Vietnam (Ministry of Health 2019). Furthermore, for compatibility with the calculations of short-term exposure to PM2.5 pollution, the daily value (person/day) was estimated by dividing by 365 days (Shang et al. 2013). This is an important input data source for health loss estimation models. The baseline mortality (\(BM_{Dist/City/Town,i}\)) for the identified damage categories, i.e., early deaths from RDs, CVDs, and CSDs occurring in the study area were 0.00007987, 0.00004142, and 0.00004142, respectively (Ministry of Health 2019).
Health Impact Function Data
Epidemiological studies that construct exposure—interaction (E-R) functions to assess the degree of health risk (HR) by the impact of exposure to PM2.5 short term pollution (24-h average values) are still limited (Li et al. 2019). In this study, the RR values were selected from available epidemiological studies published in other regions of (Cai et al. 2019; C. Chen et al. 2018; Ferreira et al. 2016; Huang et al. 2012; Kan et al. 2007; Nascimento et al. 2017; Orellano et al. 2020; Qu et al. 2018; Sui et al. 2021). These localities also had many similarities in terms of speed, level of socioeconomic development, and population distribution density in the study area. Table 1 presents the RR values with 95% CI from the published results of epidemiological studies. This is the basis for determining the values of the coefficients of the exposure-interaction functions (\(\beta_{i}\), \(\beta_{i,lowerbound}\), and \(\beta_{i,upperbound}\)).
Research Framework and Implementation Steps
Figure 3 describes the research framework in detail. First, the data set related to the CMAQ model, such as the initial conditions, boundary conditions for the model, and the data of the PM2.5 precursor biological and anthropogenic emission datasets are shown. To build a dataset of the spatial distribution of PM2.5 concentrations, WRF model was applied to generate meteorological data (hourly). The coupled WRF/CMAQ models were used to generate the hourly PM2.5 concentration data set used in the next step. Next, the data set on the distribution of 24-h average PM2.5 concentration levels during the dry season in 2018 for districts/Cities/Towns in Long An province were calculated and used. Spatiotemporal variation in the study area was analysed and evaluated. The 24-h average PM2.5 concentration limit according to the threshold value of NAAQS (50 µg/m3) was extracted. The dataset is related to the health loss model, including the health loss functions, damage function coefficient (β), population exposure, and background mortality to estimate and analyse. Assessments of loss of health, specifically the number of premature deaths from respiratory, cardiovascular, and other circulatory diseases (due to all causes) were performed. Combined with VSL values, the corresponding economic loss values owing to the health effects caused by short-term exposure to PM2.5 were also quantified for the entire study area.

Research framework
Results and Discussion
Estimated Daily PM2.5 Exposure Levels
The results of the simulation validation of PM2.5 concentration in the study area estimated through other statistical indicators, including NMB, NME, and COR, gave quite good results. Details are presented in Table 2.
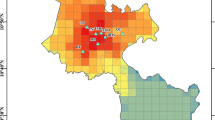
The simulation results from the WRF/CMAQ system show that the 24-h average PM2.5 concentration fluctuations in the dry season months ranged from 63.17 to 82.84 μg/m3. Figures 4 and 5 show the average PM2.5 concentration (24-h) and the spatial and temporal distribution of 24-h average PM2.5 concentrations of three typical periods in a month, namely the period from the beginning of the month (early), from the 1st to the 10th of every month; the middle of the month (Mid), from the 11th to the 20th of every month; and the end of the month (Late), from the 21st to the 28th or the 30th or 31st depending on different months.

Spatio-temporal distributions of 24-h average PM2.5 concentrations of the phases (early, mid, and late) occurring in the 2018 dry season (January – April) in Long An province

Spatio-temporal distribution of the average PM2.5 concentration in the 2018 dry season in Long An province
In January 2018, the 24-h average concentration tended to increase towards the middle of the month and decrease towards the end of the month, and concentrations tended to be higher than those of February, March, and April. From the beginning to the middle and the end of January 2018, the 24-h average PM2.5 concentration ranged from 47.48 to 67.85 μg/m3, 76.17 to 122.01 μg/m3, and 60.29 to 106.33 μg/m3.
These daily mean PM2.5 concentrations exceeded the threshold value (50 μg/m3) of the NAAQS by 1.21 to 2.44 times. From February to April 2018, 24-h mean PM2.5 levels were almost stable and lower than in January 2018, ranging between 53.29 and 84.82 μg/m3. Nevertheless, these values also exceeded the threshold value of NAAQS by 1.07 to 1.70 times. During the dry season, PM2.5-polluted areas where daily mean PM2.5 concentration exceeded NAAQS’ threshold value were commonly allocated in eastern and southeastern areas of Long An, including the Tan Tru, Chau Thanh, Can Duoc, and Can Giuoc Districts, as well as a part of the south and southeast of Thu Thua District, Ben Luc District, and Tan An City. Meanwhile, the west and northwest areas of Long An were often less polluted than other areas; specifically, the 24-h average PM2.5 concentration was lowest in Vinh Hung District, as shown in Fig. 4.
Spatio-temporal distributions of PM2.5 pollution in Long An were mainly influenced by local emission sources and meteorological conditions occurring in the dry season of 2018. Results of emission inventories during the dry season (January to April 2018) for primary PM2.5 (pPM2.5) components (pPM2.5) such as black carbon (BC) and organic carbon (OC) showed that there was a significant decrease over time during the dry season (January > February > March > April) (Fig. 6). Particularly, January 2018 had the highest total BC and OC emissions of around 240 and 2,670 thousand tonnes, respectively. For BC, emission sources contributing mainly from sectors including agricultural waste burning (AWB), residential areas (RES), road transportation (TRO), and industrial processes were approximately 17–66%, 19–49%, 9–20%, and 5–14%, respectively. For OC, emission sources were mainly contributed by AWB and RES from 51.77 to 90.77% and 7.03 to 39.01%, respectively. Meanwhile, precursor emissions involved in chemical processes to form secondary PM2.5 also tended to contribute during the dry season (January > February > March > April), and January 2018 had the highest emissions (Fig. 6). In January 2018, NOx, CO, NH3, and CH4 emissions were about 2,410; 97,570; 1,350; and 4,450 thousand tonnes, respectively. Particularly for VOCs, emission levels in the months of the dry season were quite similar, with the highest emission occurring in February 2018 was about 1,590 thousand tonnes. Therefore, the emissions of pPM2.5 and PM2.5 precursors (such as CO, CH4, NH3, NOx, and VOCs) had a significant contribution from man-made activities in the following order: AWB, RES, TRO, and IND. Notably, AWB sectors, which mainly burned rice straw after harvest from January 2018 to early February 2018 of the winter–spring rice crop in localities where rice was grown with two crops/year and three crops/year. Furthermore, cooking activities mainly using firewood, rice straw, and rice husks considerably contributed to PM2.5 pollution in Long An during this period.

Emissions of pPM2.5 (BC and OC) and PM2.5 precursors (NOx, CO, CH4, NH3, VOCs) contributed from four main sectors (IND, RES, AWB, and TRO) in the 2018 dry season (January – April) in Long An province
The characteristics of unfavorable meteorological conditions in January 2018 compared to other months of the dry season in 2018 in Long An, such as factors of 2-m temperature, 2-m surface pressure, and 10-m wind speed, also contributed significantly to the allocation of PM2.5 concentration. High temperatures promoted the vertical convection of the atmosphere, and high wind speeds accelerated the diffusion of particles in the atmosphere, causing the mass concentration of PM2.5 to decrease markedly in the months towards the end of the dry season (Chen et al. 2020a, b; Wang et al. 2015a, b). The temperature and wind speed showed an increasing trend towards the end of the dry season (Figures S1 and S2). Specifically, the range of temperature and wind speed fluctuations in the months was around 25.7–27.4 °C and 2.1–2.7 m/s (January), 25.4–27.7 °C and 2.1–2.9 m/s (February), 27.1–28.4 °C and 1.8–3.3 m/s (March), and 27.6–30.2 °C and 1.8–3.0 m/s (April), respectively. Meanwhile, the surface pressure factor tended to decrease towards the end of the dry season (Figure S3), in particular about 100.8–101.2 kPa (January), 100.9–101.3 kPa (February), 100.8–101.0 kPa (March), and 100.8–109.6 kPa (April).
PM2.5-attributed Premature Mortality
The average number of premature deaths from PM2.5 daily exposure was assessed to be associated with three types of damage, i.e., deaths from all-caused respiratory diseases and all-caused cardiovascular diseases, and other circulatory diseases of all causes (Table 3 and Fig. 7).

Changes of premature deaths due to short-term PM2.5 exposure in Long An province between January and April 2018
PM2.5 pollution levels during the dry season caused 12.951 (95% CI − 0.560; 18.711) premature deaths (all causes), of which 7.840 (95% CI 1.072; 7.092) cases were due to respiratory system diseases (accounting for 60.54%), 1.530 (95% CI − 0.181; 3.137) cases due to cardiovascular diseases (accounting for 11.81%), and 3.581 (95% CI − 1.451; 8.482) cases due to other circulatory system diseases (accounting for 27.65%).
The highest total number of deaths occurred in the month of January, with 4.695 (95% CI − 0.206; 6.771) cases, details of the number of cases due to three types of damage previously described being 2.836 (95% CI 0.390; 2.558), 0.557 (95% CI − 0.066; 1.141), and 1.302 (95% CI − 0.530; 3.072), respectively. In the following months, the impact gradually decreased and tended to be approximately the same as the total number of deaths from all causes, which were 2.740 (95% CI − 0.118; 3.965) in February 2018, 2.701 (95% CI − 0.116; 3.907) in March 2018, and 2.814 (95% CI − 0.121; 4.069) in April 2018.
Moreover, when assessing the variation in the number of deaths by day, it can be seen that in January, the number of deaths tended to increase sharply from the beginning to the middle of the month, peaking on 15 January with 0.232 (95% CI 0.032; 0.206) respiratory disease, 0.046 (95% CI − 0.005; 0.094) cardiovascular disease, and 0.107 (95% CI − 0.04; 0.250) cases due to other circulatory system diseases; from then to the end of the month, the total number of all-cause deaths dropped sharply to 0.152 (95% CI − 0.007; 0.219) cases on 31 January 2018. In February, the total number of deaths tended to increase in the beginning and middle of the month and decrease sharply towards the end of the month; specifically, the total number of deaths in these three stages was 1.242 (95% CI − 0.053; 1.795), 0.888 (95% CI − 0.038; 1.286), and 0.610 (95% CI − 0.026; 0.883). In March and April 2018, the number of daily premature deaths tended to be similar and both peaked in the middle of the month, namely on 20 March 2018 with a total number of deaths (all causes) of 0.174 (95% CI − 0.008; 0.251) and on 15 April 2018 with 0.225 (95% CI − 0.010; 0.324) premature deaths.
Evaluations based on similar studies conducted in various regions of Vietnam from 2017 to 2019 were also compared with Long An Province, Vietnam (the study area). Generally, the estimated human health impacts due to PM2.5 exposure from these studies are significantly higher than that estimated in Long An province. From a case study by Nhung et al. (2022a), the number of premature deaths (per 100,000 population) in 2019 in HCMC was 45.3 (95% CI 37.5; 52.9), which was higher than about 3.5 times compared to the study area. This is also the same for the studies of Vu et al. (2020) and Bui and Nguyen (2022) in 2017 and 2018, respectively. Meanwhile, for Hanoi Capital, the number of early deaths per 100,000 population in 2019 with 63.2 (95% CI 52.8; 73.1) (Nhung et al. 2022a, 2022b) was about 4.9 times higher than that of Long An province. Based on these comparisons, it could be seen that although PM2.5 pollution has occurred in Long An province, the pollution level is still lower than that of HCMC and Hanoi Capital. Furthermore, because of the difference in population between provinces/cities is also another important factor in the difference in early mortality rates between areas. Long An province has a relatively smaller population (about 1.67 million people) than HCMC (around 8.59 million people) and Hanoi Capital (around 7.52 million people) (GSO 2019). As a result, the overall health burden from PM2.5 exposure is also generally low compared with these areas.
Economic Valuation Losses Assessment
From the input data presented above, the BenMAP-CE software was applied to quantify the economic benefits lost from the number of premature deaths associated with the estimated 95% CI due to short-term PM2.5 exposure. The quantification process is based on the estimated VSL value for Vietnam for 2018 of 4,788.95 million VND, equivalent to about 642 million USD (converted in 2018 US$). The calculation results show that the total value of economic damage causing short-term public health impacts (deaths) in the dry season in 2018 was approximately 62.020 (95% CI − 2.683; 89.605) billion VND, equivalent to approximately 8.308 (95% CI − 0.359; 12.004) million USD (Fig. 8). Compared with the value of gross domestic product (GRDP) of Long An Province in 2018 of 110.077 trillion VND (Department of Statistics Ho Chi Minh City 2019), the total value of economic loss accounted for approximately 0.0563% of the total value of Provincial GRDP. In general, economic loss levels in this study are about 48.9 times lower than HCMC’s total losses in 2018 due to exposure to PM2.5 pollution (Bui and Nguyen, 2022).

Quantification of monthly economic losses due to 24-h average PM2.5 pollution in the 2018 dry season (January – April) in Long An province
The total number of premature deaths due to respiratory diseases caused a loss of approximately 37.545 (95% CI 5.133; 33.965) billion VND, equivalent to roughly 5.030 (95% CI 0.688; 4.550) million USD (about 60.54% of the total value of economic cost losses), whereas the total number of premature deaths due to cardiovascular and other circulatory diseases caused economic losses of 7.327 (95% CI − 0.866; 15.022) billion VND, equivalent to about 0.982 (95% CI -0.116; 2.012) million USD (around 11.81% of total valuation losses), and 17.148 (95% CI -6.950; 40.619) billion VND, equivalent to about 2.297 (95% CI -0.931; 5.441) million USD (accounting for 27.65%), respectively. However, when considering the total economic loss for each month in the dry season in 2018, the value of economic losses is in the order of January > April > February > March. Specifically, the total economic loss is in the order January > April > February > March. The estimated total number of premature deaths from all causes for each month was as follows: 22.486 (95% CI -0.984; 32.425) billion VND, equivalent to 3.012 (95% CI -0.132; 4.344) million USD, in January 2018; 13.121 (95% CI -0.563; 18.986) billion VND, equivalent to 1.758 (95% CI -0.075; 2.543) million USD, in February 2018; 12.935 (95% CI -0.555; 18.709) billion VND, equivalent to 1.733 (95% CI -0.074; 2.506) million USD, in March 2018; and 13.478 (95% CI -0.580; 19.485) billion VND, equivalent to 1.806 (95% CI -0.078; 2.610) million USD, in April 2018.
Uncertainty Analysis
The input data in this study included data on air quality (average 24-h PM2.5 concentration), exposed population, C-R functions, and corresponding β coefficients from the epidemiology of the studies. Each type of model input data has errors that can affect the final calculation results to different degrees. The results of the estimated population size exposure were obtained from reliable local data sources: the Long An Provincial Statistical Yearbook 2020 and the Health Statistical Yearbook 2017–2020. Therefore, the results on health damage basically depends on the choice of C-R functions and coefficient β. Currently in Vietnam, there have not been any quantitative studies on the relationship between air pollution and health traits, especially epidemiological studies on the short-term relationship between PM2.5 and health impact on premature deaths in provinces. Therefore, in this study, β coefficients and C-R functions from recent studies in cities of neighbouring countries were used. This is one of the main factors that can lead to errors in the calculated results because the coefficients β and the C-R functions have obvious differences in the data of the evaluation area (results of the regression function estimation). However, during the calculation and evaluation, the mean values and 95% confidence intervals (CIs) of health losses were considered and used to reflect the range of error.
Conclusion
The research results showed that the daily mean PM2.5 concentration in Long An had complicated changes in the 2018 dry season, ranging from 47.48 to 106.33 μg/m3, exceeding the NAAQS by 1.07 to 2.44 times and leading to health impacts and economic losses. The results obtained were as follows:
First, human health effects were quantified for the 2018 dry season. PM2.5 pollution caused health damage to the study area, estimated at 12.9 (95% CI -0.6; 18.7) premature deaths (all causes) per 100,000 population, of which 7.8 (95% CI 1.1; 7.1), 1.5 (95% CI -0.2; 3.1), and 3.6 (95% CI -1.5; 8.5) cases per 100,000 population were due to RDs, CVDs, and CSDs.
Second, the total value of economic losses related to daily exposure to PM2.5 concentrations during the study period reached 62.0 (95% CI -2.7; 89.6) billion VND, equivalent to 8.3 (95% CI -0.4; 12.0) million USD.
Third, a modeling framework for rapidly quantifying human health damage caused by exposure to short-term PM2.5 pollution is suitable for the proposed study area. These results could be a solid basis for further development, contributing to the construction and development of data sources for effective air environment management in Long An.
In low- and middle-income countries in Asia and Africa, socio-economic development is remarkably dependent on fossil fuels. Therefore, dwellers in these countries invariably face higher risks of premature mortality due to outdoor PM2.5 pollution-related diseases. Due to a lack of ambient air quality monitoring data, local authorities and environmental managers have encountered many difficulties in assessing PM2.5 pollution status, determining pollution causes, estimating impacts on public health attributed to PM2.5 exposure, and proposing effective mitigation measures. This study has proposed an appropriate implementation framework based on simulations by the coupled WRF/CMAQ, public health impact, and rapid quantification models of economic losses. This framework could be applied in these countries under conditions of limited measurement data to support the analysis and quantitative assessment of the factors that contribute to PM2.5 pollution and their impact on local socio-economic through the implementation of numerical simulations. Furthermore, based on these assessment results, technical and non-technical measures to control and mitigate both primary and secondary PM2.5 could be proposed to be conducted efficiently and cost-effectively.
Availability of Data and Materials
We declare that all data relating to this manuscript are truthful and we will gladly share it with any interested readers or at the request of the editor board.
References
Bayat R, Ashrafi K, Shafiepour Motlagh M et al (2019) Health impact and related cost of ambient air pollution in Tehran. Environ Res. https://doi.org/10.1016/j.envres.2019.108547
Borge R, Lumbreras J, Pérez J et al (2014) Emission inventories and modeling requirements for the development of air quality plans. Application to Madrid (Spain). Sci Total Environ 466–467:809–819. https://doi.org/10.1016/j.scitotenv.2013.07.093
Bui LT, Nguyen PH (2023) Evaluation of the annual economic costs associated with PM2.5-based health damage: a case study in Ho Chi Minh City, Vietnam. Air Quality, Atmos Health 16:415–435. https://doi.org/10.1007/s11869-022-01282-0
Bui LT, Nguyen PH, Nguyen DCM (2020) Model for assessing health damage from air pollution in quarrying area: case study at Tan Uyen quarry, Ho Chi Minh megapolis, Vietnam. Heliyon 6(9):105045. https://doi.org/10.1016/j.heliyon.2020.e05045
Bui LT, Nguyen PH, My Nguyen DC (2021) Linking air quality, health, and economic effect models for use in air pollution epidemiology studies with uncertain factors. Atmos Pollut Res 12(7):101118. https://doi.org/10.1016/j.apr.2021.101118
Bui QT, Nguyen DL, Bui TH (2022) Seasonal characteristics of atmospheric PM2.5 in an urban area of Vietnam and the influence of regional fire activities. Atmosphere. https://doi.org/10.3390/atmos13111911
Burnett RT, Arden Pope C, Ezzati M et al (2014) An integrated risk function for estimating the global burden of disease attributable to ambient fine particulate matter exposure. Environ Health Perspect 122(4):397–403. https://doi.org/10.1289/ehp.1307049
Byun D, Schere KL (2006) Review of the governing equations, computational algorithms, and other components of the models-3 Community Multiscale Air Quality (CMAQ) modeling system. Appl Mech Rev 59(1–6):51–76. https://doi.org/10.1115/1.2128636
Cai J, Peng C, Yu S et al (2019) Association between PM25 exposure and all-cause, non-accidental, accidental, different respiratory diseases, sex and age mortality in Shenzhen, China. Int J Environ Res Public Health. https://doi.org/10.3390/ijerph16030401
Chen D, Liu X, Lang J et al (2017a) Estimating the contribution of regional transport to PM2.5 air pollution in a rural area on the North China Plain. Sci Total Environ 583:280–291. https://doi.org/10.1016/j.scitotenv.2017.01.066
Chen L, Shi M, Gao S et al (2017b) Assessment of population exposure to PM2.5 for mortality in China and its public health benefit based on BenMAP. Environ Pollut 221:311–317. https://doi.org/10.1016/j.envpol.2016.11.080
Chen C, Zhu P, Lan L et al (2018) Short-term exposures to PM2.5 and cause-specific mortality of cardiovascular health in China. Environ Res 161(7):188–194. https://doi.org/10.1016/j.envres.2017.10.046
Chen L, Zhu J, Liao H, Yang Y, Yue X (2020a) Meteorological influences on PM2.5 and O3 trends and associated health burden since Chinas clean air actions. Sci Total Environ 744(219):140837. https://doi.org/10.1016/j.scitotenv.2020.140837
Chen Z, Chen D, Zhao C et al (2020b) Influence of meteorological conditions on PM2.5 concentrations across China: a review of methodology and mechanism. Environ Int 139:105558. https://doi.org/10.1016/j.envint.2020.105558
Cohen AJ, Brauer M, Burnett R et al (2017) Estimates and 25-year trends of the global burden of disease attributable to ambient air pollution: an analysis of data from the Global Burden of Diseases Study 2015. The Lancet 389(10082):1907–1918. https://doi.org/10.1016/S0140-6736(17)30505-6
Dang TN, Thanh NNN, Vien NT et al (2021) Mortality and economic burden of PM2.5 on cardiovascular disease in Ho Chi Minh City in 2018. Vietnam J Prevent Med 31(6):9–18. https://doi.org/10.51403/0868-2836/2021/369
Department of Statistics Ho Chi Minh City (2019) The Economic of Ho Chi Minh City and Key Economic Region of South Vietnam. In General Statistics Office 2(1). Ho Chi Minh City, Vietnam
Ding D, Zhu Y, Jang C et al (2016) Evaluation of health benefit using BenMAP-CE with an integrated scheme of model and monitor data during Guangzhou Asian Games. J Environ Sci (China) 42:9–18. https://doi.org/10.1016/j.jes.2015.06.003
Eder B, Yu S (2006) A performance evaluation of the 2004 release of Models-3 CMAQ. Atmos Environ 40(26):4811–4824. https://doi.org/10.1016/j.atmosenv.2005.08.045
Emery C, Liu Z, Russell AG, Odman MT, Yarwood G, Kumar N (2017) Recommendations on statistics and benchmarks to assess photochemical model performance. J Air Waste Manag Assoc 67(5):582–598. https://doi.org/10.1080/10962247.2016.1265027
Fan P, Ouyang Z, Nguyen DD, Nguyen TTH, Park H, Chen J (2019) Uranization, economic development, environmental and social changes in transitional economies: Vietnam after Doimoi. Landsc Urban Plan 187:145–155. https://doi.org/10.1016/j.landurbplan.2018.10.014
Fann N, Coffman E, Timin B, Kelly JT (2018) The estimated change in the level and distribution of PM2.5-attributable health impacts in the United States: 2005–2014. Environ Res 167:506–514. https://doi.org/10.1016/j.envres.2018.08.018
Ferreira TM, Forti MC, de Freitas CU, Nascimento FP, Junger WL, Gouveia N (2016) Effects of particulate matter and its chemical constituents on elderly hospital admissions due to circulatory and respiratory diseases. Int J Environ Res Public Health 13(10):1–11. https://doi.org/10.3390/ijerph13100947
Forouzanfar MH, Afshin A, Alexander LT et al (2016) Global, regional, and national comparative risk assessment of 79 behavioural, environmental and occupational, and metabolic risks or clusters of risks, 1990–2015: a systematic analysis for the Global Burden of Disease Study 2015. The Lancet 388(10053):1659–1724. https://doi.org/10.1016/S0140-6736(16)31679-8
Gao X, Koutrakis P, Coull B et al (2021) Short-term exposure to PM25 components and renal health: findings from the Veterans Affairs Normative Aging Study. J Hazardous Mater 420(38):126557. https://doi.org/10.1016/j.jhazmat.2021.126557
Gehrig R, Buchmann B (2003) Characterising seasonal variations and spatial distribution of ambient PM10 and PM2.5 concentrations based on long-term Swiss monitoring data. Atmos Environ 37(19):2571–2580. https://doi.org/10.1016/S1352-2310(03)00221-8
GSO (2019) Statistical Yearbook of Vietnam 2018 (The General Statistics Office (ed.)). The Statistical Publishing House, Hanoi Capital, Vietnam
Guan Y, Kang L, Wang Y, Zhang NN, Ju MT (2019) Health loss attributed to PM2.5 pollution in China’s cities: economic impact, annual change and reduction potential. J Clean Prod 217:284–294. https://doi.org/10.1016/j.jclepro.2019.01.284
Ha Chi NN, Kim Oanh NT (2021) Photochemical smog modeling of PM2.5 for assessment of associated health impacts in crowded urban area of Southeast Asia. Environ Technol Innovat 21:101241. https://doi.org/10.1016/j.eti.2020.101241
Hammitt JK, Robinson LA (2011) The income elasticity of the value per statistical life: transferring estimates between high and low income populations. J Benefit-Cost Anal 2(1):1–29. https://doi.org/10.2202/2152-2812.1009
Harrison RM, Laxen D, Moorcroft S, Laxen K (2012) Processes affecting concentrations of fine particulate matter (PM2.5) in the UK atmosphere. Atmos Environ 46:115–124. https://doi.org/10.1016/j.atmosenv.2011.10.028
Hien TT, Chi NDT, Nguyen NT, Vinh LX, Takenaka N, Huy DH (2019) Current status of fine particulate matter (PM2.5) in Vietnam’s most populous city, Ho Chi Minh City. Aerosol Air Qual Res 19(10):2239–2251. https://doi.org/10.4209/aaqr.2018.12.0471
Hoek G, Krishnan RM, Beelen R et al (2013) Long-term air pollution exposure and cardio-respiratory mortality: a review. Environ Health: A Global Access Sci Source. https://doi.org/10.1186/1476-069X-12-43
Hu J, Wu L, Zheng B et al (2015) Source contributions and regional transport of primary particulate matter in China. Environ Pollut 207:31–42. https://doi.org/10.1016/j.envpol.2015.08.037
Huang W, Cao J, Tao Y et al (2012) Seasonal variation of chemical species associated with short-term mortality effects of PM2.5 in Xi’an, a central city in China. Am J Epidemiol 175(6):556–566. https://doi.org/10.1093/aje/kwr342
Huy DH, Chi NDT, Phu NLS, Hien TT (2018) Fine particulate matter (PM2.5) in Ho Chi Minh City: Analysis of the status and the temporal variation based on the continuous data from 2013–2017. Sci Technol Dev J Nat Sci 2(5):130–137
ICD-10 (2016) International statistical classification of diseases and related health problems 10th revision. Geneva, Switzerland. http://apps.who.int/classifications/icd10/browse/%0A2016/en
IQAir (2020) 2019 World air quality report–region and City PM2.5 Ranking. Goldach, Switzerland. https://www.iqair.com/world-most-polluted-cities/world-air-quality-report-2019-en.pdf
Johnson RJ, Rolfe J, Windle J, Benner J (2015) The economics of non-market goods and resources benefit transfer of environmental and resource values. Benefit Transf Environ Resource Values. https://doi.org/10.1007/978-94-017-9930-0
Kampa M, Castanas E (2008) Human health effects of air pollution. Environ Pollut 151(2):362–367. https://doi.org/10.1016/j.envpol.2007.06.012
Kan H, London SJ, Chen G et al (2007) Differentiating the effects of fine and coarse particles on daily mortality in Shanghai China. Environ Int 33(3):376–384. https://doi.org/10.1016/j.envint.2006.12.001
Ke L, Zhang Y, Fu Y, Ma X, Di Q (2022) Short-term PM2.5 exposure and cognitive function: Association and Neurophysiological Mechanisms. SSRN Electronic J 170:107593. https://doi.org/10.2139/ssrn.4129729
Khanh PN (2020) Improving the growth quality of the Southern key economic region from an economic perspective. Ho Chi Minh City Open University. J Sci 14(3):84–105. https://doi.org/10.46223/hcmcoujs.econ.vi.14.3.479.2019
Khanh UL, Nguyen PH, Bui LT (2022) Risk assessment of hospital admission due to all–cause respiratory and cardiovascular diseases attributed to ground-level O3 short-term exposure in Dong Nai Province Vietnam. J Hydrometeorol 742:1–18. https://doi.org/10.36335/VNJHM.2022(742).1-18
Kim D, Kim J, Jeong J, Choi M (2019) Estimation of health benefits from air quality improvement using the MODIS AOD dataset in Seoul, Korea. Environ Res 173:452–461. https://doi.org/10.1016/j.envres.2019.03.042
Landrigan PJ, Fuller R, Acosta NJR et al (2018) The Lancet Commission on pollution and health. The Lancet 391(10119):462–512. https://doi.org/10.1016/S0140-6736(17)32345-0
Lang J, Zhou Y, Chen D et al (2017) Investigating the contribution of shipping emissions to atmospheric PM2.5 using a combined source apportionment approach. Environ Pollut 229:557–566. https://doi.org/10.1016/j.envpol.2017.06.087
Lelieveld J, Evans JS, Fnais M, Giannadaki D, Pozzer A (2015) The contribution of outdoor air pollution sources to premature mortality on a global scale. Nature 525(7569):367–371. https://doi.org/10.1038/nature15371
Levy JI, Hanna SR (2011) Spatial and temporal variability in urban fine particulate matter concentrations. Environ Pollut 159(8–9):2009–2015. https://doi.org/10.1016/j.envpol.2010.11.013
Li T, Guo Y, Liu Y et al (2019) Estimating mortality burden attributable to short-term PM2.5 exposure: A national observational study in China. Environ Int 125:245–251. https://doi.org/10.1016/j.envint.2019.01.073
Linh Nguyen TN, Pimonsree S, Prueksakorn K, Bich Thao PT, Vongruang P (2022) Public health and economic impact assessment of PM25 from open biomass burning over countries in mainland Southeast Asia during the smog episode. Atmos Pollut Res 13(6):101418. https://doi.org/10.1016/j.apr.2022.101418
Long An DNRE (2020) Report on environmental status of Long An province in the period 2016–2020. Tan An City, Long An Province, Vietnam
Long An Provincial Statistics Office (2021) Statistical Yearbook of Long An Province 2020. Tan An City, Long An Province, Vietnam
Lu F, Xu D, Cheng Y et al (2015) Systematic review and meta-analysis of the adverse health effects of ambient PM2.5 and PM10 pollution in the Chinese population. Environ Res 136:196–204. https://doi.org/10.1016/j.envres.2014.06.029
Lu X, Lin C, Li W et al (2019) Analysis of the adverse health effects of PM2.5 from 2001 to 2017 in China and the role of urbanization in aggravating the health burden. Sci Total Environ 652:683–695. https://doi.org/10.1016/j.scitotenv.2018.10.140
Luecken DJ, Yarwood G, Hutzell WT (2019) Multipollutant modeling of ozone, reactive nitrogen and HAPs across the continental US with CMAQ-CB6. Atmos Environ 201:62–72. https://doi.org/10.1016/j.atmosenv.2018.11.060
Luong LMT, Phung D, Sly PD, Morawska L, Thai PK (2017) The association between particulate air pollution and respiratory admissions among young children in Hanoi, Vietnam. Sci Total Environ 578:249–255. https://doi.org/10.1016/j.scitotenv.2016.08.012
Luong LTM, Dang TN, Thanh Huong NT et al (2020) Particulate air pollution in Ho Chi Minh city and risk of hospital admission for acute lower respiratory infection (ALRI) among young children. Environ Pollut 257:113424. https://doi.org/10.1016/j.envpol.2019.113424
Malesky EJ, Tuan DA, Thach PN et al (2020) The Vietnam Provincial Competitiveness Index Measuring, PCI 2020—Measuring economic governance for business development. Hanoi Capital, Vietnam
Ministry of Health (2019) The Health Statistics Yearbook 2018. Hanoi Capital, Vietnam
Morris RE, Mc Nally DE, Tesche TW, Tonnesen G, Boylan JW, Brewer P (2005) Preliminary evaluation of the Community Multiscale Air Quality Model for 2002 over the Southeastern United States. J Air Waste Manag Assoc 55(11):1694–1708. https://doi.org/10.1080/10473289.2005.10464765
Narain U, Sall C (2016) Methodology for valuing the health impacts of air pollution. D.C., USA, Washington
Nascimento AP, Santos JM, Mill JG et al (2017) Association between the concentration of fine particles in the atmosphere and acute respiratory diseases in children. Rev Saude Publica 51(1):1–10. https://doi.org/10.1590/S1518-8787.2017051006523
Nhung NTT, Long TK, Linh BN, Vos T, Huong NT, Anh ND (2013) Estimation of Vietnam National Burden of Disease 2008. Asia Pac J Public Health 26(5):527–535. https://doi.org/10.1177/1010539513510556
Nhung NTT, Schindler C, Dien TM, Probst-Hensch N, Perez L, Künzli N (2018) Acute effects of ambient air pollution on lower respiratory infections in Hanoi children: an eight-year time series study. Environ Int 110:139–148. https://doi.org/10.1016/j.envint.2017.10.024
Nhung NTT, Schindler C, Dien TM, Probst-Hensch N, Künzli N (2019) Association of ambient air pollution with lengths of hospital stay for Hanoi children with acute lower-respiratory infection, 2007–2016. Environ Pollut 247:752–762. https://doi.org/10.1016/j.envpol.2019.01.115
Nhung NTT, Duc VT, Ngoc VD, Dien TM, Hoang LT, Ha TTT, Khue PM, Truong NX, Thanh NTN, Jegasothy E, Marks GB, Morgan G (2022a) Mortality benefits of reduction fine particulate matter in Vietnam, 2019. Front Public Health 10:1056370. https://doi.org/10.3389/fpubh.2022.1056370
Nhung NTT, Jegasothy E, Ngan NTK, Truong NX, Thanh NTN, Marks GB, Morgan GG (2022b) Mortality burden due to exposure to outdoor fine particulate matter in Hanoi, Vietnam: Health Impact Assessment. Int J Public Health 67:1604331. https://doi.org/10.3389/ijph.2022.1604331
OECD (2012) Mortality risk valuation in environment, health and transport policies. Paris, France. https://doi.org/10.1787/9789264130807-en
Orellano P, Reynoso J, Quaranta N, Bardach A, Ciapponi A (2020) Short-term exposure to particulate matter (PM10 and PM2.5), nitrogen dioxide (NO2), and ozone (O3) and all-cause and cause-specific mortality: Systematic review and meta-analysis. Environ Int 142:105876. https://doi.org/10.1016/j.envint.2020.105876
Persson U, Norinder A, Hjalte K, Gralén K (2001) The value of a statistical life in transport: findings from a new contingent valuation study in Sweden. J Risk Uncertain 23(2):121–134. https://doi.org/10.1023/A:1011180018244
Pitiranggon M, Johnson S, Haney J, Eisl H, Ito K (2021) Long-term trends in local and transported PM2.5 pollution in New York City. Atmospheric Environment 248. https://doi.org/10.1016/j.atmosenv.2021.118238
Qu Y, Pan Y, Niu H et al (2018) Short-term effects of fine particulate matter on non-accidental and circulatory diseases mortality: A time series study among the elder in Changchun. PLoS ONE 13(12):1–12. https://doi.org/10.1371/journal.pone.0209793
Quan M, Shiqiu Z (2015) Assessment of the trend of heavy PM2.5 pollution days and economic loss of health effects during 2001–2013. Acta Scientiarum Naturalium Universitatis Pekinensis 51(4):694–706. https://doi.org/10.13209/j.0479-8023.2015.074
Ring AM, Canty TP, Anderson DC et al (2018) Evaluating commercial marine emissions and their role in air quality policy using observations and the CMAQ model. Atmospheric Environment 173:96–107. https://doi.org/10.1016/j.atmosenv.2017.10.037
Sacks JD, Lloyd JM, Zhu Y et al (2018) The environmental benefits mapping and analysis program–community edition (BenMAP–CE): a tool to estimate the health and economic benefits of reducing air pollution. Environ Model Softw 104(2):118–129. https://doi.org/10.1016/j.envsoft.2018.02.009
Shang Y, Sun Z, Cao J et al (2013) Systematic review of Chinese studies of short-term exposure to air pollution and daily mortality. Environ Int 54:100–111. https://doi.org/10.1016/j.envint.2013.01.010
Skamarock WC, Klemp JB, Dudhi J et al (2008) A description of the advanced research WRF Version 3. Technical Report, June, 113. Colorado, USA. https://doi.org/10.5065/D6DZ069T
Stanaway JD, Afshin A, Gakidou E et al (2018) The Lancet 392(10159):1923–1994. https://doi.org/10.1016/S0140-6736(18)32225-6
Sui X, Zhang J, Zhang Q (2013) The short-term effect of PM2.5/O3 on daily mortality from 2013 to 2018 in Hefei, China. Environ Geochem Health 43(1):153–169. https://doi.org/10.1007/s10653-020-00689-x
Thu NTA, Blume L, Addison E, Franielczyk K (2018) Air quality in Vietnam in 2017. In Air Quality Report–GreenID (Issue 2). Hanoi Capital, Vietnam
Thuy NTT, Dung NT, Sekiguchi K et al (2018) Mass concentrations and Carbonaceous compositions of PM0.1, PM2.5, and PM10 at urban locations in Hanoi, Vietnam. Aerosol and Air Quality Research 18(7):1591–1605. https://doi.org/10.4209/aaqr.2017.11.0502
Toledo T, Albuquerque DA, Andrade MDF et al (2018) WRF-SMOKE-CMAQ modeling system for air quality evaluation in São Paulo megacity with a 2008 experimental campaign data. Environ Sci Pollut Res 25:36555–36569
Vien NT, Thanh NNN, Dung PHT et al (2021) PM2.5 increased respiratory mortality in Ho Chi Minh city: a multi-source data study. J Med Res 142(6):108–118. https://doi.org/10.52852/tcncyh.v142i6.197
Vietnam VCCI (2021) The provincial competitiveness index. The Provincial Competitiveness Index Portal of Vietnam. Hanoi Capital, Vietnam. https://pcivietnam.vn/en
Viscusi WK, Aldy JE (2003) The value of a statistical life: a critical review of market estimates throughout the world. J Risk Uncertain 27(1):5–76. https://doi.org/10.1023/A:1025598106257
Vu HNK, Ha QP, Nguyen DH, Nguyen TTT, Nguyen TT, Nguyen TTH, Tran ND, Ho BQ (2020) Poor air quality and its association with mortality in Ho Chi Minh city: Case study. Atmosphere 11(7):1–20. https://doi.org/10.3390/atmos11070750
Wang J, Wang S, Voorhees AS, Zhao B et al (2015a) Assessment of short-term PM2.5-related mortality due to different emission sources in the Yangtze River Delta. China Atmos Environ 123:440–448. https://doi.org/10.1016/j.atmosenv.2015.05.060
Wang Y, Chen C, Wang P et al (2015b) Experimental investigation on indoor/outdoor PM2.5 concentrations of an office building located in Guangzhou. Proc Eng 121:333–340. https://doi.org/10.1016/j.proeng.2015.08.1076
Xie Y, Dai H, Dong H et al (2016) Economic impacts from PM2.5 pollution-related health effects in China: a provincial-level analysis. Environ Sci Technol 50(9):4836–4843. https://doi.org/10.1021/acs.est.5b05576
Xing X, Liu F, Yang X et al (2021) Declines in heart rate variability associated with short-term PM2.5 exposure were modified by blood pressure control and treatment: a multi-city panel study in China. Environ Pollut 287:117572. https://doi.org/10.1016/j.envpol.2021.117572
Yin H, Pizzol M, Xu L (2017a) External costs of PM2.5 pollution in Beijing, China: uncertainty analysis of multiple health impacts and costs. Environ Pollut 226:356–369. https://doi.org/10.1016/j.envpol.2017.02.029
Yin P, Chen R, Wang L et al (2017b) Ambient ozone pollution and daily mortality: a nationwide study in 272 Chinese cities. Environ Health Perspect 125(11):1–7. https://doi.org/10.1289/EHP1849
Zhang W, Hai S, Zhao Y et al (2021) Numerical modeling of regional transport of PM2.5 during a severe pollution event in the Beijing–Tianjin–Hebei region in November 2015. Atmos Environ. https://doi.org/10.1016/j.atmosenv.2021.118393
Acknowledgements
The authors acknowledge the support of time and facilities from Ho Chi Minh City University of Technology (HCMUT), VNU-HCM for this study.
Funding
We acknowledge the support of time and facilities from Ho Chi Minh City University of Technology (HCMUT), VNU-HCM for this study.
Author information
Authors and Affiliations
Contributions
Long Ta Bui: Conceptualization, Funding acquisition, Investigation, Project administration, Resources, Supervision, Methodology, Models, writing—original draft, writing—review\& editing. Han Thi Ngoc Lai: Data analysis, Formal analysis. Phong Hoang Nguyen: Models, Validation, GIS.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Ethical Approval
The manuscript is not submitted to more than one journal for simultaneous consideration.The manuscript is original and not have been published elsewhere in any form or language (partially or in full), unless the new work concerns an expansion of previous work. The manuscript is not split up into several parts to increase the quantity of submissions and submitted to various journals or to one journal over time (i.e. ‘salami-slicing/publishing’). Results are presented clearly, honestly, and without fabrication, falsification or inappropriate data manipulation. We adhere to discipline-specific rules for acquiring, selecting and processing data. We have provided all data and proper mentions of other works.
Consent to Participate
I consent to participate publish my manuscript entitled “Benefits of short-term premature mortality reduction attributed to PM2.5 pollution: A case study in Long An province, Vietnam” to the Archives of Environmental Contamination and Toxicology (AECT).
Consent to Publish
I consent to publish my manuscript entitled “Benefits of short-term premature mortality reduction attributed to PM2.5 pollution: A case study in Long An province, Vietnam” to the Archives of Environmental Contamination and Toxicology (AECT).
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Bui, L.T., Lai, H.T.N. & Nguyen, P.H. Benefits of Short-term Premature Mortality Reduction Attributed to PM2.5 Pollution: A Case Study in Long an Province, Vietnam. Arch Environ Contam Toxicol 85, 245–262 (2023). https://doi.org/10.1007/s00244-023-01012-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00244-023-01012-2