
Abstract
While studies have demonstrated that air pollution can be catastrophic to the population’s health, few empirical studies are found in the economic literature because a considerable proportion of the evidence comes from epidemiological studies. Because of the crucial role of governance in the health community, good governance has been a contentious issue in public sector management in recent years. Therefore, the aim of this study is to examine the effects of air pollution and the role of governance on health outcomes. This study employed the generalized method of moment (GMM) estimation techniques to analyse panel data for 72 developing countries from 2010 to 2017. The empirical results confirm that higher PM2.5 and CO2 levels have a detrimental influence on life expectancy and healthy life expectancy, whereas the role of governance has a positive impact on life expectancy and healthy life expectancy. Furthermore, the findings show governance quality plays a role in moderating the negative effect of PM2.5 on health outcomes. The ongoing rise in air pollution has had a significant impact on the health of developing countries. It appears that governance quality has improved health outcomes. The findings have important policy implications, such that strengthening governance can reduce air pollution emissions in developing countries. However, to reduce the health effects of air pollution, developing countries must implement effective environmental development policies and track the implementation and enforcement of such policies.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
In developing countries, structural change in their economies has largely moved away from primary products towards manufacturing-based production, leading to high growth rates of their GDPs (McMillan et al. 2017; Collier and Venables 2007). Manufacturing intensification between many developing countries is an increasingly significant concern during the process of economic development. The manufacturing process is accompanied by significant increases in pollutant discharges, the depletion of a large amount of natural resources, tremendous increases in pollutant discharge, damage to ecosystem sustainability, and severe effects on human health (Zafar et al. 2019; Wang et al. 2018). Notably, air pollution is an important issue that has been shown to be worse in rapidly developing countries than in wealthy or very poor nations. The influence of disclosure on air pollution is far larger in such countries, in which population growth (nearly 70% of the global population resides in middle-income countries), urbanisation, and accelerated industrialisation lead to reduced environmental quality (Mannucci and Franchini 2017; Pena and Rollins 2017; Sultana et al. 2022).
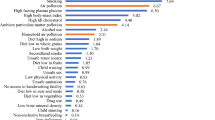
Based on the Global Burden of Disease (GBD) project, air pollution is presently considered among the world’s leading risk factors for death. A growing body of literature has verified the negative association between air pollution and health effects. Exposure to polluted air increases the frequency of various types of diseases that lead to a higher incidence of mortality (Ahmad et al. 2021a, b; Yu et al. 2020) and lower life expectancy (Qi et al. 2020; Urhie et al. 2020). While air pollution in high-income countries has decreased dramatically, the World Health Organisation (WHO) reported that it still accounted for some 4.9 million fatalities in 2017, mainly in low- and middle-income countries, where air pollution has risen in the last 25 years (Boogaard et al. 2019). Poor air quality is thus unavoidable in many developing countries, and it can have various health repercussions, including increased disability and a shorter lifespan (Anser et al. 2020; Wang et al. 2019; Ebenstein et al. 2015). Therefore, it has become a priority for developing countries to rectify air pollution to address the concerns regarding its adverse effects on health and the quality of life.
Notwithstanding, many experts agree that good governance practises in decision-making may be the best way to resolve the increasingly visible risks to health from air pollution by framing effective policy mechanisms and implementing appropriate strategies (Kim and Wang 2019; Dash et al. 2020). Ahmad et al. (2021a, b) proposed that governments should considerably reduce the detrimental impact of air pollution on mortality. This study is similar, albeit healthy life expectancy is used to proxy health outcomes instead of adult mortality rates. Despite their importance, mortality indicators provide decision-makers with limited and insensitive information on general population health (Stiefel et al. 2010; Jagger 2015). Healthy life expectancy (also known as disability-free life expectancy), which integrates mortality and morbidity information, has attained importance as a population health measurement. Thus, the degree to which improving the quality of life keeps pace with the rise in life expectancy is a significant health policy issue in many countries.
This study contributes to the following dimensions in the current literature. First, this issue is examined by including finer air pollution sources, particulate matter (PM2.5), in exploring better health outcomes, namely healthy life expectancy. This provides a more inclusive measure of population health, including the morbidity and mortality associated with non-fatal health outcomes. PM2.5, on the other hand, is the local air pollutant that poses a more serious health risk than other types of contaminants. Second, this study also considers the role of governance in moderating air pollution’s negative effects on better health outcomes in developing countries. A governance quality index was constructed from six individual Worldwide Governance Indicators (WGI) from the World Bank to measure the overall quality of a country’s governance quality. Such an index can be useful for evaluating the broader governance dimensions that contain extended information and provide valuable insights into cross-country patterns. Thus, understanding good governance and its relevant role is crucial for developing countries when seeking to improve health during periods of economic growth and environmental problems.
Literature review
The interaction between socio-economic elements—such as the environment and health outcomes—has provided beneficial insights for scholars and policymakers. As a result, the literature explores the relationship between air pollution, governance, and health impacts to enable better comprehension of the function of this link in previous investigations.
Air pollution and health effects
Ambient air pollution has been reported as a contributing cause of non-communicable diseases and associated deaths, accounting for 40% of all pollution-related deaths or approximately 3.4 million annual deaths (Fuller et al. 2019). Among the pollutants, particulate matter (PM10 and PM2.5) has a more substantial health effect than other contaminants (Yap et al. 2019; Kim et al. 2018). Notably, due to its smaller size, PM2.5 was more closely correlated with chronic diseases. This pollutant is more likely to enter the lungs and even the bloodstream, producing further negative health effects (Wu et al. 2020; Schwartz et al. 2018; Fann et al. 2017). The dominance of PM2.5 risk was recorded in a study conducted by Hadei et al. (2017) in Iran, in which the total number of deaths related to PM2.5 was 4336, while those related to PM10, O3, NO2, and SO2 were 4192, 1363, 2830, and 1216 over 3 years (2013 to 2016), respectively. Similarly, considerable numbers of deaths owing to PM2.5 have been reported in India (Balakrishnan et al. 2019), Iran (Bayat et al. 2019), and the USA (Bennett et al. 2019). Comparing different global risk factors shows that ambient air pollution (PM2.5) is a leading cause of excess mortality and loss of life expectancy, mainly through cardiovascular diseases (Lelieveld et al. 2020).
Apte et al. (2018) reported that PM2.5 exposure was estimated to reduce the average global life expectancy by nearly 1 year, with declines of 1.2 to 1.9 years in contaminated countries of Asia and Africa when using the Global Burden of Disease project. The results of Hill et al. (2019) across multiple life expectancy models reported that greater PM2.5 levels of exposure tend to lower the average life expectancy. Similarly, Chen et al. (2019) showed that citizens residing in areas with greater levels of PM2.5 displayed significantly contracted life expectancy, whereby escalation in PM2.5 was related to a deterioration in life expectancy of 0.3 years among adults. De Keijzer (2017) found that the increase of PM2.5 and other air concentrations (PM10, NO2 and O3) resulted in a loss of life in Spain. Bennett et al. (2019) found that current PM2.5 levels correlated with impacts on mortality and loss of life expectancy, with more significant implications in lower-income counties and those with higher poverty rates. Fotourehchi (2015) found that PM10 and CO2 negatively affected life expectancy and positively affected infant mortality. Moreover, studies have revealed that life expectancy decreased with higher CO2 emissions (Anser et al. 2020; Urhie et al. 2020; Ahmad and Zhao 2018).
Despite the emerging concerns about air pollution and its health outcomes, most accessible studies emphasising mortality and life expectancy are found outside the economic literature (De Keijzer 2017; Bennett et al. 2019; Urhie et al. 2020), in which less attention has been devoted to healthy life expectancy. Life expectancy and mortality rate were essentially chosen not because they were the very best indicators, but because they are accessible ways to find measurements across many years for most countries and they are reliable in assessing health outcomes (Beltrán-Sánchez et al. 2015). Healthy life expectancy, on the other hand, provides a relatively more extensive measure of population health, which is sensitive to changes in health across the population and allows for the morbidity related to non-fatal health effects and mortality (Stiefel et al. 2010; Jagger and Robine 2011).
Studies on this include the works by Gangadharan and Valenzuela (2001), Wen and Gu (2012), Bardi and Perini (2013), and Grigoli and Kapsoli (2018). Gangadharan and Valenzuela (2001) reported the significant negative effect of the environmental stress variable on healthy life expectancy from 1997 to 1999, despite a data limitation. Wen and Gu (2012) analysed the relationships between the Air Pollution Index and health outcomes using datasets from a nationwide comprehensive longitudinal survey undertaken across China. According to the findings, acquaintance with air pollutants was linked to a drop in life expectancy and health expectancy. Bardi and Perini (2013) observed that one possible cause of the drop in healthy life expectancy could be a connection with climate change, which caused a heatwave in Europe. Data on healthy life expectancy can be gathered by querying people directly, although this assessment is more imprecise and subjective than determining the cause of death. Grigoli and Kapsoli (2018) found that access to sanitation facilities positively affects healthy life expectancy. As a result, further research and reports are needed that explore how relative air pollution risks link to healthy life expectancy.
Governance and health association
Governance is defined broadly as the act, process, or power of governing through good governance principles. This intuitive interpretation conceals the assertion that governance is a complicated matter with many varied aspects. Some people have used the term governance broadly to describe the entire spectrum of social, political, and institutional structures that have an impact on how the government operates, while others use it to describe primarily to state capability. Even more people have referred to it as a code phrase for government corruption and mismanagement (Quibria 2015). The most comprehensive and influential definition of governance is provided by Kaufmann et al. (2009) and the World Bank on WGI. According to the World Bank, governance is the process by which authority is used to manage a nation’s social and economic resources for development. Kaufmann et al. (2009) stated that governance includes the method by which governments are chosen, scrutinised, and replaced; the capability of the government to successfully develop and enforce effective laws and a nation’s institutions that control its residents’ economic and social interactions are respected by both its citizens and by the state. All of the previously described dimensions—political regime, state capability, and legal framework—are included in this concept.
Governance is thought to have a significant impact on population health. Regulating environmental and economic policies thru the long-term governance of ecology, economics, with public health allows for the quantification of the influence of governance on population health (Wang et al. 2018; Lisciandra and Migliardo 2017). Some of the interventions include developing and monitoring legislation for air pollution, raising taxes on and eliminating subsidies for sources of pollution, increasing the utilisation of clean energy, and placing limitations on the consumption of biomass fuels (Murukutla et al. 2017; Chatterjee 2016). All policy choices should result from a transparent, inclusive, and accountable decision-making procedures in a setting where good governance is practised. Aside from economic progress, good governance is thought to be essential for achieving positive social and development impacts by reducing newborn and maternal mortality, eradicating illiteracy, and eradicating poverty (Lemos and Agrawal 2006; Akan et al. 2022).
Batniji et al. (2014) claimed that the government’s effectiveness was a significant factor in reducing mortality, while the main obstacle to the population’s access to healthcare in Arab countries was political instability. Kim and Wang (2019) stated that government effectiveness positively influences life expectancy and has an adverse effect on infant death rates. Sirag et al. (2017) provided evidence that public healthcare financing is more effective in promoting the health of the population in countries where the standard of governance is relatively high, compared to countries where it is poor. Accordingly, Doucouliagos et al. (2019) found that these governance indicators significantly affect health aid efficacy in minimising mortality. Achim et al. (2019) presented strong evidence that the degree of corruption significantly influences physical health (represented by life expectancy and mortality rate) and mental health (represented as happiness), as well as economic development and cultural context moderation, in both high-income and low-income countries. Furthermore, greater corruption has a more significant impact on the population’s physical health in low-income countries than in high-income ones. Biadgilign et al. (2019) showed that regulatory quality, government effectiveness, and corruption control reduced childhood undernutrition. Furthermore, Ahmad et al. (2021b) discovered that regulating corruption appeared to attenuate the detrimental effects of PM2.5 on life expectancy.
Although good governance is extensively realised to be the potential factor leading to better-quality health outcomes, less effective governance can negatively affect health. Gupta (2000) observed that places with extensive corruption have high child and infant mortality rates. In all socio-economic groups along the lifecycle, relatively high corruption rates were found to correlate with self-reported poor general health among both men and women in 20 African countries (Witvliet et al. 2013). Ahmad and Hasan (2016) demonstrated that higher corruption threatens health status development in Malaysia over the long term. Also, corruption was found to reduce the effectiveness of public health spending on mortality, as indicated by Mhango and Chirwa (2018).
On the other hand, a large number of studies have explored the interaction between public health expenditure and governance quality to assess the influence on health (Sirag et al. 2017; Doucouliagos et al. 2019; Kim and Wang 2019). Only Aliyu and Ismail (2016) and Ahmad et al. (2021a, b) investigated the health effects of the interaction between governance quality and air pollution. Lower adult mortality rates are associated with improved governance quality, according to Ahmad et al. (2021a, b), whereas stronger government efficiency is linked to lower infant mortality rates, according to Aliyu and Ismail (2016). Shortcomings in these issues warrant more empirical work in the field, as this would potentially affect pollution regulations and the efficient procurement of healthcare services.
Data and methodology
Data description
Due to the data availability, this study used data collected annually from 2010 to 2017. Three data sources were used. First, the average life expectancy at birth, PM2.5 (fine particulate matter in micrograms per cubic metre), CO2 emissions (metric tons per capita), national income per capita (GDP per capita), public health expenditure (% of GDP), and school enrolment figures were gathered from the World Bank (World Development Indicators). Second, the data for governance quality were collected from the WGI database, which comprises six aggregate indicators and was constructed by the World Bank. The six measures are voice and accountability, government effectiveness, the rule of law, regulation quality, political stability, and corruption control, each of which defines different aspects of a country’s quality of governance. All the government quality indicators are scaled from − 2.5 to + 2.5, whereby higher values show better quality and vice versa. Lastly, data on healthy life expectancy were collected from the Global Burden of Disease database developed by the Institute for Health Metrics and Evaluation (IHME).
Econometric models
For this study, econometric models following Aliyu and Ismail (2016) and Ahmad et al. (2021a) were formulated:
where H is the dependent variable that refers to the health outcomes proxy by life expectancy (LE) and healthy life expectancy (HLE). LE is a metric that determines the average estimated number of years of life that will remain at a given age. This measure is usually used to estimate the average lifespan, whereby improved life expectancy at birth is generally regarded as a sign of a population’s better health condition. This rise is usually linked to the decline in infectious disease mortality. The increased importance of chronic diseases as the leading cause of death, however, suggests that life expectancy is no longer adequate when quantifying health. Hence, HLE estimates the sum of healthy years an individual is predicted to live at birth by deducting the years of ill health included in the overall life expectancy. Good health is the most crucial aspect of healthcare, and healthy life expectancy is an insightful and meaningful measurement that incorporates the span and quality of life that represents fuller lives in good health. lPOL represents the indicators for air pollution, namely particulate matter (PM2.5) and carbon dioxide emissions (CO2). The size of the particulate matter plays a significant role in environmental health risks. The aerodynamic diameter categorises particulate matter by classifying particles below 10 μm in diameter as thoracic particles PM10, whereas particles below 2.5 μm in diameter are known as fine particles PM2.5 (Brown et al. 2013). PM10 particles penetrate deep into the respiratory system when inhaled, while finer particles (PM2.5) enter the lungs, pass into the bloodstream, and are brought into other bodily organs. PM2.5 may, therefore, be more detrimental to human health than larger particles. Also, due to the growing danger of global warming, CO2 poses significant challenges to healthy living. It has a significant relationship with rising human mortality and other life-threatening diseases.
The analyses also involve several control variables, including GDP per capita, public health expenditure, and population education status, consistent with previous studies measuring air pollution and health effects. lY refers to GDP per capita and indicates the importance of income in improving health status; it can, for instance, provide better housing, sanitation and nutrition to a country’s people (Cutler et al. 2006). Public health spending is represented by lPHS, which is commonly correlated with improved health outcomes as it offers greater access to healthcare and facilities. lEDU reflects the population’s education level, which affects health and social well-being because better-informed people are more likely to understand nutrition, hygiene, health services, and standard disease prevention measures (Balan 2016). In addition, μ denotes country-specific effects, while ε represents an error term. The subscripts i and t denote cross-sectional countries and time (year), respectively. The lagged dependent variable (\({H}_{it-1}\)) indicates the dynamic effect, whereby the likelihood of health status is conditional on the value of this same variable from the preceding year. The coefficient should be below 1 because of the variable’s statistically significant persistence.
Furthermore, there are compelling grounds for assuming that better health status is positively related to more outstanding governance quality (Witvliet et al. 2013; Batniji et al. 2014). Therefore, Eq. 1 was extended as follows:
GQI measures the quality of governance, combining six governance indicators into one overall index. The six dimensions were assumed to represent relatively significant aspects of the quality of governance. The governance quality index applies principal component analysis (PCA)Footnote 1 to measure the indicator weights within a component. This method introduced a multidimensional weighted index from all the variables to represent the governance quality. Also, it makes it more convenient for the general public to recognise and compare across different countries, a composite index indicator that incorporates multiple correlated indicators.
On the other hand, various studies have shown that governance may have a moderating impact, implying that governance affects other system processes or mechanisms that enhance health (Farag et al. 2013; Kim and Wang 2019). Based on the impacts of governance quality on the provision of healthcare services, including government attempts to resolve environmental problems, the interaction terms were estimated in the following regression equation:
Governance represents its role in the public sector in providing healthcare services, including protection against environmental pollution. Thus, in the moderation analyses, the interaction term (\(l{\mathrm{POL}}_{it}{*\mathrm{GQI}}_{it}\)) was employed to formally determine whether the relationship between air pollution and health outcomes differs as a function of the quality of governance. In other words, the interaction terms were employed to examine whether governance quality played a moderating role by influencing the effectiveness of a government in containing the adverse effects of air pollution on health outcomes.
Methodology
The dynamic panel models in the above Eqs. 1, 2, and 3 contain statistical problems that make the conventional panel estimation methods inappropriate and biased, including the pooled OLS, fixed-effect, and random-effect estimation methods. Since the lag term in the dependent variables \(\left({H}_{it-1}\right)\) can be associated with the error term\((\mathrm{cov}\left({H}_{it-1}, {\varepsilon }_{it}\right) \ne 0)\), the conventional OLS estimate would be biased even if there was no serial association in the error term\(({\varepsilon }_{it})\). Besides that, for the estimator of fixed effects, while the individual-level effects \({(\mu }_{i})\) were omitted from the intra-group data that deviated from individual means, there may still have been a correlation between \({(H}_{it-1}-\overline{{H }_{it-1}} )\) and \({(\varepsilon }_{it}-\overline{{\varepsilon }_{it}} ).\) For the estimator of generalized least squares (GLS), which was achieved through the estimation of the random effects, even once the variables had been quasi-centralised, the estimation findings would also be biased because of the correlation between \({(H}_{it-1}-\theta \overline{{H }_{it-1}} )\) and \({(\varepsilon }_{it}-\theta \overline{{\varepsilon }_{it}} ).\) Furthermore, generalized method of moment (GMM) controls for country-specific effects that cannot use country-specific dummies because of the dynamic structure of the regression equation. It also mitigates the simultaneity bias created by the chance that some of the explanatory variables are endogenous.
To address these problems, this analysis used the GMM estimation introduced by Arellano and Bond (1991). This estimator was created for small T and large N panel situations in which one left-side variable is dynamic (based on prior realisations) and explanatory variables were not solely exogenous (Baltagi 2013; Roodman 2009). GMM estimators resolve such econometric problems by utilising lagged observations within the explanatory variables as instruments. In particular, the first-differenced GMM estimators and the system GMM estimators are two forms of GMM estimation. The first-differenced GMM approach eliminates the country-specific effects or the time-invariant country-specific variable directly by taking the first differentiation. Later, in order to overcome the resulting correlation of lagged dependent variable and disturbance terms following the first differentiation, the instrumental variables are used to comply with the endogeneity issue of the regressors. Lagged explanatory variables are used by first-differenced GMM estimators as instrumental variables, assuming that the idiosyncratic error term is not serially associated and the explanatory indicators are weakly exogenous (Li et al. 2015). Even though the aforesaid difference estimator is able to control the country-specific effects and simultaneity bias, it does have significant limitations. Alonso-Borrego and Arellano (1999) and Blundell and Bond (1998) showed that while the explanatory variables were persistent, the lagged levels of the variables tended to be weak instruments and therefore possibly asymptotically resulted in bias parameter estimates across small samples and a greater variance.
Arellano and Bover (1995) and Blundell and Bond (1998) proposed the GMM system to rectify these issues. This estimator demonstrated that the system GMM estimator was able to lessen the biases and inaccuracy associated with the difference estimator. This estimator raises efficiency by utilising the lagged levels and also lagged differences. To cater to the correlations within the error terms and lagged dependent variables, as well as the inclusion of endogenous variables in both regressions, instrumental variables were then used. Since the instruments were not simple to define, the approach used internal instruments, notably instrumented lagged values of variables (Ibrahim and Law 2016). The level regression was instrumented by lagged first-differenced variables, while the first-differenced regression was instrumented to the lagged level variables. Unlike the first-differenced GMM, the GMM system integrates possible information within the level relationship and the relations between the levels and the first differences.
GMM estimators are generally related to one-step and two-step alternatives. The one-step estimator incorporates weighting matrices, which are independent of estimated parameters. The two-step GMM estimator utilises optimal weighting matrices, whereby the moment conditions are measured with a consistent estimate within their covariance matrix. This method makes the two-step estimator more efficient than the one-step estimator. Thus, the two-step system GMM estimator was employed in this analysis to produce more consistent and efficient parameter estimates. However, when adopting this estimation procedure, instrument proliferation or the issue of too many instruments may exist. With too many instruments, the GMM estimators may over-fit the endogenous variables and barely distinguish their exogenous components. The collapse of the lag length approach described by Roodman (2009) was used to address this problem, obtain improved results and achieve model fitness.
Two specification tests were performed to examine the estimation’s overall validity, namely the Hansen J-test of over-identifying restrictions and the AR(2) test of autocorrelation. The empirical moments contain zero expectations within the null joint validity with all the instruments, so the J statistic was dispersed as a chi-square of degrees of freedom equal to that of the degree of over-identification. The absence of error term auto-correlation within the equations above was supported when the errors of the first-differenced equations displayed a lack of autocorrelation at order 2. Thus, the failure to reject both the null of the J-test and that of the second-order serial correlation tests supported the model estimations.
Empirical results and discussion
The datasets of the descriptive statistics are reported in Table 1. The means, standard deviations (within countries, between countries, and overall), and minimum and maximum values are shown in the table. The discrepancies between the minimum and maximum values for life expectancy and healthy life expectancy were high, at almost 30 years, according to the table. Cote d’Ivoire and Swaziland had the lowest levels of life expectancies and healthy life expectancies, 50 years and 39 years, respectively. In contrast, Costa Rica recorded the highest level of life expectancy (80 years), while Colombia had the highest level of healthy life expectancy (70 years). The same discrepancies were observed in the PM2.5 variable results. The maximum concentration of PM2.5 was 97.4 µg/m3, whereas the lowest concentration was 10.5 µg/m3, as reported in India and Kiribati, respectively. As for the minimum and maximum per capita CO2 emissions, the values varied from 0.19 in Zambia to 16.07 in Kazakhstan. This is a plausible indication that air pollution could be a crucial factor in reducing health outcomes in developing countries. In addition, the levels of emissions and health indicators were generally better in sample countries with higher governance quality, which likely endorses the view that governance is essential to improving health and enhancing the enforcement of environmental regulations.
The empirical results are reported in Tables 2 and 3, and the analysis contains three parts. First, the findings from the basic regression of PM2.5 and health outcomes (columns 1 and 4 of Table 2) are followed by the inclusion of the governance quality index in the regression models (columns 2 and 5 of Table 2) and the models with the interaction terms (columns 3 and 6 of Table 2). The robustness of the estimated results for the relationship between PM2.5 and the governance quality index in terms of health outcomes was assessed by re-estimating the previous models using CO2 emissions as an air pollutant (Table 3). No issues with instrument validity and error autocorrelation were indicated in the diagnostic statistics. More specifically, we did not reject the null hypothesis from the Hansen test statistics that the instruments were valid. Moreover, the autocorrelation Arellano-Bond tests showed the absence of autocorrelation. Thus, it could be justified that the estimated models passed the diagnostic tests.
The estimation findings of models 1 and 4 (Table 2) indicated that PM2.5 significantly and negatively affected health outcomes across developing countries. PM2.5 had coefficients of − 0.125 and − 0.254 for life expectancy (LE) and healthy life expectancy (HLE), respectively. Total life expectancy reduced by about 0.01 years (nearly 0.2 months), while healthy life expectancy reduced by around 0.03 years (over 0.3 months), with a 10% increase in PM2.5 levels. The results imply that higher particulate air pollution levels are harmful to human health and potentially lead to the prevalence of illness. They cause a deterioration in overall health conditions by increasing disability (reducing healthy life) and reducing life duration. Thus, the evidence that lower health status is correlated with PM2.5 appears to support the epidemiological findings that air polluting particles can contribute to chronic disease-induced disability (Hendryx et al. 2019; Gurung et al. 2017).
Concerning the estimated effect of governance indicators, the estimation models include the governance quality index (GQI) in the models in columns (2) and (5). The estimation results show that governance quality had a positive effect on enhancing the population’s health condition. The governance effect ranges from 0.132 to 1.429. A unit increase in governance adds life expectancy and healthy life expectancy of between 0.1 and 1.4 years, respectively. Despite the variations throughout the explanatory variables’ estimated coefficients, they generally remained significant in both regressions performed. It is worth noting that the magnitude of the air pollution effect on life expectancy fell and the healthy life expectancy coefficient became insignificant when the governance role was considered. These findings suggest the need to use interactive terms that highlight the importance of governance in mitigating the adverse health effects of air pollution.
The regressions were modified with the insertion of the interaction terms to address the modifying impact of governance quality on air pollution (Eq. 3). The findings are broadly comparable to those of the regressions before the interaction terms’ inclusion (columns 3 and 6). The results of the interaction between levels of PM2.5 and the governance quality index brought positive signs for life expectancy (0.665) and healthy life expectancy (0.619). A one-unit increase in the governance measure reduced the effect of air pollution and lengthened life expectancy by 0.007 years and 0.006 years, respectively, on healthy life expectancy through these interaction terms. These results indicate that governance quality may be the solution that improves health, which is corroborated by Aliyu and Ismail (2016), Achim et al. (2019), and Kim and Wang (2019). They studied the impact of multiple individual components of governance quality on development outcomes, including health. However, the current study suggests that the Governance Quality Index can outweigh the adverse effects of air pollution because this specific dimension, as a benchmark of governance quality, does not comprehensively represent a country’s overall performance. The findings of Ahmad et al. (2021a, b) revealed the interactive terms of governance quality index and air pollution; however, the researchers focused only on mortality rates.
As a standard application of the robustness test, carbon dioxide emissions were considered to be the indicator that could evaluate the extent of air pollution when the regression of Eqs. 1, 2, and 3 were undertaken again. The findings are presented in Table 3. On the other hand, the estimated models passed both the Hansen J-test and AR(2) test, suggesting that the regression course’s instrument variables were effective and that second-order serial correlation did not affect the regression results. The regression results reported here are, therefore, reliable.
The results observed in the regression analysis of the alternative proxy variables did not affect the previous econometric results, i.e. CO2 exhibited a negative relationship with health outcomes across developing countries. Life expectancy and healthy life expectancy were − 0.06 and − 0.088, respectively (columns 1 and 4). Consistent with the PM2.5 findings, the CO2 effects were more pronounced on healthy life expectancy. Air pollution’s harmful effects might cause a population to suffer from disabilities for longer periods. Since an improved life expectancy is not inherently an indication of improved living conditions for the population, this possibility illustrates the importance of healthy life expectancy as a health measure. Thus, the probability of living longer may not mean a better quality of life, as the burden of ill health can accompany an increase in life expectancy. In addition, both the health indicators from PM2.5 exposure strongly exceeded the values of CO2 emissions, i.e. by order of magnitude. Therefore, fine particulate matter, PM2.5, could be considered a more critical health issue and more attempts should be made to monitor fine particulate emissions.
When the governance quality index was added to the estimation models (columns 2 and 5), the coefficients of CO2 consistently displayed negative signs. The governance quality index was found to affect health outcomes positively. However, none of the health outcomes were affected by the interaction between CO2 and the governance quality index. Due to the local effects of the PM2.5 pollutant, people feel susceptible to this air pollutant, making them increase their demands for improved air quality. Nations with better governance quality may create incentives to reduce local air pollution in response to their citizens’ rising environmental consciousness. However, to reduce global pollutants (e.g. CO2), governance constraint is important, and it requires international participants to devise effective policies that could curtail the detrimental effects.
Conclusion
The relationships between air pollution, governance quality, and health outcomes were analysed based on dynamic panel data from 72 developing countries between 2010 and 2017 using the GMM estimation. In general, both air pollutants were harmful to health, with the most significant risk to healthy life expectancy coming from PM2.5. Fine particulate matter has an apparent impact on human health relative to CO2. This pollutant is related to a wide variety of acute and chronic diseases, causing disability that contributes to ‘lost’ healthy years. Further analysis shows that the quality of governance unambiguously enhances well-being. The interactive term of PM2.5 and the quality of governance were significantly positive, suggesting that the relationship between governance and air pollution is mutually reinforcing; i.e. improving governance quality will further reduce air pollution and thus improve health outcomes.
According to this finding, if air pollution levels in developing world rose, it would be unable to improve production levels, which would result in lower productivity in the economy and health issues for the local population. This stresses the importance of local air pollution measures for enhancing urban air quality and embracing global climate change. This requires cooperation between the public, governing authorities, and health agencies to address this issue. The governance institutions should develop aggressive local pollution-control strategies that take into account the consequences of air quality on human health and ecosystems. The study indicated that fine particles are considerably more hazardous to human health, implying that action is required to establish atmospheric PM2.5 concentration guidelines for fine particle emission control. The governance role appears to be a necessary element in terms of compliance with effective pollution reduction measures, as well as tracking the implementation and enforcement of such measures. Where rules are well articulated and transparent, control procedures for PM2.5 levels can be easily applied and incentives can be generated for firms to use resources more efficiently. For instance, manufacturing industries that emitted more hazardous gases into the environment than allowed could face fines as a deterrent to others. With significant policy-driven improvements in air quality, air pollution may be significantly reduced. Thus, the study draws attention to the importance of setting air quality standards for air pollution control to safeguard human health. In addition, more efforts are required to raise public awareness about the potential dangers of air pollution. Health authorities could educate the public about the health benefits of clean air, such as fewer hospital stays and skipped days at school and work because of sickness. Public outreach activities, as well as a partnership with a variety of public and private institutions, will be critical in recognising the dangers of air pollution.
This study can be expanded in a number of ways, including by gathering more data over time on environmental variables as well as other variables that affect health status for various nations at various stages of development. Since this study is concerned with a variety of environmental and health indicators, acquiring data for all of these measures over a long period of time is rather difficult, which limits the purpose here. For example, the availability of data for the provision of public health spending and pollution indicator PM2.5 influenced the selection of both countries and the start time. However, this condition will gradually become better as data availability increases, and study into it may be promoted. The research can also be expanded by creating a single indication or index that captures the comprehensive standard of an environment state in a nation. According to the available literature, the quantity of study done utilising environmental indices to examine the consequence on health still seems to be limited. The analysis of environmental problems within a nation would benefit from such an index, which can also offer significant insights into cross-country patterns. Future index-based research should therefore take into account and compare with the current findings.
Data availability
The datasets used and analysed during the current study are available from the corresponding author on reasonable request.
References
Achim MV, Văidean VL & Borlea SN (2019) Corruption and health outcomes within an economic and cultural framework. Eur J Health Econ 1–13. https://doi.org/10.1007/s10198-019-01120-8
Ahamed MM, Mallick SK (2019) Is financial inclusion good for bank stability? International evidence. J Econ Behav Organ 157:403–427. https://doi.org/10.1016/j.jebo.2017.07.027
Ahmad R, Hasan J (2016) Public health expenditure, governance and health outcomes in Malaysia. J Ekonomi Malaysia 50(1):29–40. https://doi.org/10.17576/JEM-2016-5001-03
Ahmad M, Zhao ZY (2018) Empirics on linkages among industrialisation, urbanisation, energy consumption, CO2 emissions and economic growth: a heterogeneous panel study of China. Environ Sci Pollut Res 25(30):30617–30632. https://doi.org/10.1007/s11356-018-3054-3
Ahmad NA, Ismail NW, Ahmad Sidique SF, Mazlan NS (2021a) Air pollution effects on adult mortality rate in developing countries. Environ Sci Pollut Res 28(7):8709–8721. https://doi.org/10.1007/s11356-020-11191-3
Ahmad NA, Ismail NW, Tilde AY, Aliyu AJ (2021) Effects of air pollution and corruption control on life expectancy in middle-income countries. International Journal of Economics and Management 15(2):257–268. Retrieved January 20, 2021, from http://www.ijem.upm.edu.my/vol15no2/7.%20Effects%20of%20Air%20Pollution%20and%20Corruption%20Control.pdf
Akan T, Gündüz Hİ, Vanlı T, Zeren AB, Işık AH, Mashadihasanli T (2022) Why are some countries cleaner than others? New evidence from macroeconomic governance. Environ Dev Sustain 1–57. https://doi.org/10.1007/s10668-022-02298-3
Aliyu AJ, Ismail NW (2016) The effects of air pollution on human mortality: does gender difference matter in African countries? Environ Sci Pollut Res 23(21):21288–21298. https://doi.org/10.1007/s11356-016-7253-5
Alonso-Borrego C, Arellano M (1999) Symmetrically normalized instrumental-variable estimation using panel data. Journal of Business & Economic Statistics 17(1):36. https://doi.org/10.2307/1392237
Anser MK, Hanif I, Vo XV & Alharthi M (2020) The long-run and short-run influence of environmental pollution, energy consumption, and economic activities on health quality in emerging countries. Environ Sci Pollut Res 1–15. https://doi.org/10.1007/s11356-020-09348-1
Apte JS, Brauer M, Cohen AJ, Ezzati M, Pope III CA (2018) Ambient PM2.5 reduces global and regional life expectancy. Environ Sci Technol Lett 5(9):546–551. https://doi.org/10.1021/acs.estlett.8b00360
Arellano M, Bond S (1991) Some tests of specification for panel data: Monte Carlo evidence and an application to employment equations. Rev Econ Stud 58(2):277–297. https://doi.org/10.2307/2297968
Arellano M, Bover O (1995) Another look at the instrumental variable estimation of error-components models. J Econ 68(1):29–51. https://doi.org/10.1016/0304-4076(94)01642-D
Balakrishnan K, Dey S, Gupta T, Dhaliwal RS, Brauer M, Cohen A J, ..., & Sabde Y (2019). The impact of air pollution on deaths, disease burden, and life expectancy across the states of India: the Global Burden of Disease Study 2017. Lancet Planet Health 3(1):e26-e39. https://doi.org/10.1016/S2542-5196(18)30261-4
Balan F (2016) Environmental quality and its human health effects: a causal analysis for the EU-25. Int J Appl Econ 13(1):57–71
Bali TG, Brown SJ, Caglayan MO (2014) Macroeconomic risk and hedge fund returns. J Financ Econ 114(1):1–19. https://doi.org/10.1016/j.jfineco.2014.06.008
Baltagi BH (2013) Panel data forecasting. Handb Econ Forecast 2:995–1024. https://doi.org/10.1016/B978-0-444-62731-5.00018-X
Bardi U, Pierini V (2013) Declining trends of healthy life years expectancy (hlye) in europe. Retrieved January 20, 2021, from https://arxiv.org/pdf/1311.3799.pdf
Batniji, R., Khatib, L., Cammett, M., Sweet, J., Basu, S., Jamal, A., ... & Giacaman, R. (2014). Governance and health in the Arab world. The Lancet, 383(9914), 343–355. https://doi.org/10.1016/S0140-6736(13)62185-6
Bayat R, Ashrafi K, Motlagh MS, Hassanvand MS, Daroudi R, Fink G, Künzli N (2019) Health impact and related cost of ambient air pollution in Tehran. Environ Res 176:108547. https://doi.org/10.1016/j.envres.2019.108547
Beltrán-Sánchez H, Soneji S, Crimmins EM (2015) Past, present, and future of healthy life expectancy. Cold Spring Harb Perspect Med 5(11):a025957
Bennett J E, Tamura-Wicks H, Parks RM, Burnett RT, Pope III CA, Bechle MJ, ..., & Ezzati M (2019). Particulate matter air pollution and national and county life expectancy loss in the USA: a spatiotemporal analysis. PLoS Med 16(7):e1002856. https://doi.org/10.1371/journal.pmed.1002856
Biadgilign S, Ayenew HY, Shumetie A, Chitekwe S, Tolla A, Haile D, ..., & Gebre B (2019). Good governance, public health expenditures, urbanisation and child undernutrition Nexus in Ethiopia: an ecological analysis. BMC Health Serv Res 19(1):1-10https://doi.org/10.1186/s12913-018-3822-2
Blundell R, Bond S (1998) Initial conditions and moment restrictions in dynamic panel data models. J Econ 87(1):115–143. https://doi.org/10.1016/S0304-4076(98)00009-8
Boogaard H, Walker K, Cohen AJ (2019) Air pollution: the emergence of a major global health risk factor. Int Health 11(6):417–421. https://doi.org/10.1093/inthealth/ihz078
Brown JS, Gordon T, Price O, Asgharian B (2013) Thoracic and respirable particle definitions for human health risk assessment. Part Fibre Toxicol 10(1):12. https://doi.org/10.1186/1743-8977-10-12
Chatterjee P (2016) India takes steps to curb air pollution World Health Organization. Bullet World Health Organ 94(7):487
Chen CC, Chen PS, Yang CY (2019) Relationship between fine particulate air pollution exposure and human adult life expectancy in Taiwan. J Toxicol Environ Health A 82(14):826–832. https://doi.org/10.1080/15287394.2019.1658386
Collier P & Venables AJ (2007). Rethinking trade preferences to help diversify African exports. Policy Insight, 2. https://doi.org/10.1111/j.1467-9701.2007.01042.x
Cutler D, Deaton A, Lleras-Muney A (2006) The determinants of mortality. J Econ Perspect 20(3):97–120
Dash DP, Behera SR, Rao DT, Sethi N, Loganathan N (2020) Governance, urbanisation, and pollution: a cross-country analysis of global south region. Cogent Econ Finance 8(1):1742023. https://doi.org/10.1080/23322039.2020.1742023
De Keijzer C, Agis D, Ambrós A, Arévalo G, Baldasano JM, Bande S ... & Ghigo S (2017) The association of air pollution and greenness with mortality and life expectancy in Spain: a small-area study. Environ Int 99:170–176. https://doi.org/10.1016/j.envint.2016.11.009
Doucouliagos H, Hennessy J & Mallick D (2019). Health aid, governance and infant mortality. IZA Discussion Papers 12166, Institute of Labor Economics (IZA)
Ebenstein A, Fan M, Greenstone M, He G, Yin P, Zhou M (2015) Growth, pollution, and life expectancy: China from 1991–2012. Am Econ Rev 105(5):226–231. https://doi.org/10.1257/aer.p20151094
Fann N, Kim SY, Olives C, Sheppard L (2017) Estimated changes in life expectancy and adult mortality resulting from declining PM 2.5 exposures in the contiguous United States: 1980–2010. Environ Health Perspect 125(9):097003. https://doi.org/10.1289/EHP507
Farag M, Nandakumar AK, Wallack S, Hodgkin D, Gaumer G, Erbil C (2013) Health expenditures, health outcomes and the role of good governance. Int J Health Care Finance Econ 13(1):33–52. https://doi.org/10.1007/s10754-012-9120-3
Fotourehchi Z (2015) Health effects of air pollution: an empirical analysis for developing countries. Atmos Pollut Res 30:1–6. https://doi.org/10.1016/j.apr.2015.08.011
Fuller R, Sandilya K, Hanrahan D (2019) Pollution and health metrics: global, regional, and country analysis. Global Alliance on Health and Pollution. Retrieved February 6, 2021, from https://gahp.net/wpcontent/uploads/2019/12/PollutionandHealthMetrics-final-12_18_2019.pdf
Gangadharan L, Valenzuela MR (2001) Interrelationships between income, health and the environment: extending the Environmental Kuznets Curve hypothesis. Ecol Econ 36(3):513–531. https://doi.org/10.1016/S0921-8009(00)00250-0
Grigoli F, Kapsoli J (2018) Waste not, want not: the efficiency of health expenditure in emerging and developing economies. Rev Dev Econ 22(1):384–403. https://doi.org/10.5089/9781484364260.001
Gupta MS (2000).Corruption and the provision of health care and education services. Int Monet Fund. https://doi.org/10.5089/9781451853926.001
Gurung A, Son J-Y, Bell ML (2017) Particulate matter and risk of hospital admission in the Kathmandu Valley, Nepal: a case-crossover study. Am J Epidemiol 186(5):573–580. https://doi.org/10.1093/aje/kwx135
Hadei M, Hopke PK, Nazari SSH, Yarahmadi M, Shahsavani A, Alipour MR (2017) Estimation of mortality and hospital admissions attributed to criteria air pollutants in Tehran metropolis, Iran (2013–2016). Aerosol Air Qual Res 17(10):2474–2481. https://doi.org/10.4209/aaqr.2017.04.0128
Hendryx M, Luo J, Chojenta C, Byles JE (2019) Air pollution exposures from multiple point sources and risk of incident chronic obstructive pulmonary disease (COPD) and asthma. Environ Res 179:108783. https://doi.org/10.1016/j.envres.2019.108783
Hill TD, Jorgenson AK, Ore P, Balistreri KS, Clark B (2019) Air quality and life expectancy in the United States: an analysis of the moderating effect of income inequality. SSM Populat Health 7:100346. https://doi.org/10.1016/j.ssmph.2018.100346
Ibrahim MH, Law SH (2016) Institutional quality and CO2 emission–trade relations: evidence from Sub-Saharan Africa. S Afr J Econ 84(2):323–340. https://doi.org/10.1111/saje.12095
Jagger C (2015) Trends in life expectancy and healthy life expectancy. Future of an ageing population: evidence review. Foresight Government Office for Science, London Retrieved February 10, 2021, from https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/464275/gs-15-13-future-ageing-trends-life-expectancy-er12.pdf
Jagger C, Robine JM (2011) Healthy life expectancy. International handbook of adult mortality. Springer, Dordrecht, pp 551–568
Jones AM, Labeaga JM (2003) Individual heterogeneity and censoring in panel data estimates of tobacco expenditure. J Appl Economet 18(2):157–177
Kaufmann D, Kraay A, & Mastruzzi M (2009).Governance matters VIII: aggregate and individual governance indicators 1996-2008. The World Bank. https://doi.org/10.1596/1813-9450-4978
Kim S, Wang J (2019) Does quality of government matter in public health?: comparing the role of quality and quantity of government at the National Level. Sustainability 11(11):3229. https://doi.org/10.3390/su11113229
Kim D, Chen Z, Zhou LF, Huang SX (2018) Air pollutants and early origins of respiratory diseases. Chronic Dis Transl Med 4(2):75–94. https://doi.org/10.1016/j.cdtm.2018.03.003
Lelieveld J, Pozzer A, Pöschl U, Fnais M, Haines A & Münzel T (2020). Loss of life expectancy from air pollution compared to other risk factors: a worldwide perspective. Cardiovasc Res. https://doi.org/10.1093/cvr/cvaa025
Lemos MC, Agrawal A (2006) Environmental governance. Annu Rev Environ Resour 31(1):297–325
Levi M (2006) Presidential address: why we need a new theory of government. Perspect Polit 4(1):5–19. https://doi.org/10.1017/S1537592706060038
Li S, Zhang J, Ma Y (2015) Financial development, environmental quality and economic growth. Sustainability 7(7):9395–9416. https://doi.org/10.3390/su7079395
Lisciandra M, Migliardo C (2017) An empirical study of the impact of corruption on environmental performance: evidence from panel data. Environ Resource Econ 68(2):297–318. https://doi.org/10.1007/s10640-016-0019-1
Mannucci PM, Franchini M (2017) Health effects of ambient air pollution in developing countries. Int J Environ Res Public Health 14(9):1048. https://doi.org/10.3390/ijerph14091048
McMillan M, Rodrik D, Sepulveda C (2017). Structural change, fundamentals and growth: a framework and case studies (No. w23378). National Bureau of Economic Research. Retrieved February 7, 2021, from https://www.nber.org/system/files/working_papers/w23378/w23378.pdf
Mhango CT, Chirwa GC (2018) Government health expenditure and health outcomes in Malawi: does governance matter? J Public Adm Dev Altern (JPADA) 3(1–1):1–14
Murukutla N, Negi NS, Puri P, Mullin S, Onyon L (2017) Online media coverage of air pollution risks and current policies in India: a content analysis. WHO S-E Asia J Public Health 6(2):41–50
Pena MSB, Rollins A (2017) Environmental exposures and cardiovascular disease: a challenge for health and development in low-and middle-income countries. Cardiol Clin 35(1):71–86. https://doi.org/10.1016/j.ccl.2016.09.001
Qi J, Ruan Z, Qian Z, Yin P, Yang Y, Acharya BK ... & Lin H. (2020) Potential gains in life expectancy by attaining daily ambient fine particulate matter pollution standards in mainland China: a modeling study based on nationwide data. PLoS Med 17(1):e1003027. https://doi.org/10.1371/journal.pmed.1003027
Quibria MG (2015) Governance in developing Asia concepts measurements determinants and a paradox. In Governance in Developing Asia. Edward Elgar Publishing, Camberley, pp 17–48
Roodman D (2009) A note on the theme of too many instruments. Oxford Bull Econ Stat 71(1):135–158. https://doi.org/10.1111/j.1468-0084.2008.00542.x
Schwartz JD, Wang Y, Kloog I, Yitshak-Sade MA, Dominici F, Zanobetti A (2018) Estimating the effects of PM2.5 on life expectancy using causal modeling methods. Environ Health Perspect 126(12):127002. https://doi.org/10.1289/EHP3130
Sirag A, Nor NM, Abdullah NMR, Abd Ghani J (2017) Public health financing and infant mortality: does governance quality matter? Public Finance Manag 17(4):341–370
Stiefel MC, Perla RJ, Zell BL (2010) A healthy bottom line: healthy life expectancy as an outcome measure for health improvement efforts. Milbank Q 88(1):30–53. https://doi.org/10.1111/j.1468-0009.2010.00588.x
Sultana N, Rahman MM, Khanam R (2022) Environmental Kuznets curve and causal links between environmental degradation and selected socioeconomic indicators in Bangladesh. Environ Dev Sustain 24(4):5426–5450. https://doi.org/10.1007/s10668-021-01665-w
Urhie E, Afolabi A, Afolabi A, Matthew O, Osabohien R, Ewetan O (2020) Economic growth, air pollution and health outcomes in Nigeria: a moderated mediation model. Cogent Soc Sci 6(1):1719570. https://doi.org/10.1080/23311886.2020.1719570
Wang Z, Zhang B, Wang B (2018) The moderating role of corruption between economic growth and CO2 emissions: evidence from BRICS economies. Energy 148:506–513. https://doi.org/10.1016/j.energy.2018.01.167.10.1016/S2542-5196(18)30277-8
Wang Q, Wang J, Zhou J, Ban J, Li T (2019) Estimation of PM2· 5-associated disease burden in China in 2020 and 2030 using population and air quality scenarios: a modelling study. Lancet Planet Health 3(2):e71–e80. https://doi.org/10.1016/S2542-5196(18)30277-8
Wen M, Gu D (2012) Air pollution shortens life expectancy and health expectancy for older adults: the case of China. J Gerontol A: Biomed Sci Med Sci 67(11):1219–1229. https://doi.org/10.1093/gerona/gls094
Windmeijer F (2006) GMM for panel count data models. University of Bristol Economics Working Paper, (06–591). https://doi.org/10.2139/ssrn.936579
Witvliet MI, Kunst AE, Arah OA, Stronks K (2013) Sick regimes and sick people: a multilevel investigation of the population health consequences of perceived national corruption. Trop Med Int Health 18(10):1240–1247. https://doi.org/10.1111/tmi.12177
Wu Z, Chen X, Li G, Tian L, Wang Z, Xiong X, Yang C, Zhou Z, Pan X (2020) The impact of air pollution on attributable risks and economic costs of hospitalization for mental disorders. Retrieved January 18, 2021, from https://www.iza.org/publications/dp/12986/the-impact-of-air-pollution-on-attributable-risks-and-economic-costs-of-hospitalization-for-mental-disorders
Yap J, Ng Y, Yeo KK, Sahlén A, Lam CSP, Lee V, Ma S (2019) Particulate air pollution on cardiovascular mortality in the tropics: impact on the elderly. Environ Health 18(1):34. https://doi.org/10.1186/s12940-019-0476-4
Yu W, Guo Y, Shi L, Li S (2020) The association between long-term exposure to low-level PM2. 5 and mortality in the state of Queensland, Australia: a modelling study with the difference-in-differences approach. PLoS Med 17(6):e1003141. https://doi.org/10.1371/journal.pmed.1003141
Zafar MW, Saud S, Hou F (2019) The impact of globalization and financial development on environmental quality: evidence from selected countries in the Organization for Economic Co-operation and Development (OECD). Environ Sci Pollut Res 26(13):13246–13262. https://doi.org/10.1007/s11356-019-04761-7
Author information
Authors and Affiliations
Contributions
The study’s design and model specifications were made by Nor Asma Ahmad and Normaz Wana Ismail. Nor Asma Ahmad and Normaz Wana Ismail prepared the materials, collected the data, and analysed the results. Nor Asma Ahmad wrote the first version of the text, which was reviewed by Normaz Wana Ismail, Shaufique Fahmi Ahmad Sidique, and Nur Syazwani Mazlan. The final manuscript was read and accepted by Nor Asma Ahmad, Normaz Wana Ismail, Shaufique Fahmi Ahmad Sidique, and Nur Syazwani Mazlan.
Corresponding author
Ethics declarations
Ethics approval
Not applicable.
Consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Responsible Editor: Eyup Dogan
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Appendix
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Ahmad, N.A., Ismail, N.W., Sidique, S.F.A. et al. Air pollution, governance quality, and health outcomes: evidence from developing countries. Environ Sci Pollut Res 30, 41060–41072 (2023). https://doi.org/10.1007/s11356-023-25183-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11356-023-25183-6