
Abstract
Urban areas under the influence of multi-industrial activities with arid and semi-arid environments witness the significant increase in environmental pollution especially in the water sector. The present study evaluated the water quality and associated health risk assessment through heavy metal pollution. Drinking (n = 48) and surface (n = 37) water samples were collected from semi-arid multi-industrial metropolis, Faisalabad, Pakistan. Physio-chemical and biological parameters and different metals (Al, As, Ba, Cd, Cr, Cu, Fe, Pb, Ni and Zn) were investigated using standard procedures and multivariate water quality assessments. Many physio-chemical and biological parameters and metals especially arsenic were exceeding the permissible limit of Punjab environmental quality standards and the World Health Organization. The results from water quality index showed that < 56% samples have poor, < 8% have very poor and < 6% have unsuitable water quality for drinking purposes. Water quality for the Gugera Branch Canal was found suitable with medium sodium (alkalinity) and salinity hazards, while it was found poor with magnesium absorption ratio. Hazard quotient (HQ) values for arsenic were found at the threshold level (HQ > 1) and carcinogenicity was found in case of arsenic and chromium (1 × 10−4) in adults and children. Semi-arid weather combined with different anthropogenic activities and unusual water features provoked metal contamination. Results of the present study can deliver basic information for effective management of water in the most populous and industrial areas.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Groundwater is the utmost valuable source for drinking which is extensively used in various parts of the world (Khanoranga and Khalid 2019). A worldwide challenge of water contamination has developed into a serious subject particularly with augmented urbanization (Titilawo et al. 2018; Ghorade et al. 2014; Li et al. 2014). It significantly impacts on water resource management by many ways including overexploitation, land-use change and adulteration (Grimm et al. 2008; Jia et al. 2013; Nawab et al. 2018; Vesali Naseh et al. 2018). The unrestrained urban and industrial wastewater release has substantial influence on the soil, plants and river and stream water quality (Qadir et al. 2007; Yousaf et al. 2016; Abbas et al. 2017; Mukatea et al. 2018), especially trace elements’ impact on human health and ecology (Xiao et al. 2019; Dong et al. 2017; Chowdhury et al. 2016; Zeng et al. 2015). High concentrations of metals including chromium, cadmium, lead and manganese are lethal for aquatic and human life especially causing breath shortening and different types of cancers (Muhammad et al. 2011; Khan et al. 2013b).
Existing water resources lead to insufficiency and deteriorating quality of freshwater which lead to serious water scarcity (Khair et al. 2012; Khan et al. 2013a; Hussain et al. 2017a, b; Khan et al. 2017; Ishaque and Shaikh 2017). Irrigation practices consume almost 70% of this water extraction (FAO 2013). Pakistan is ranked as the seventh highest region of the globe exposed to water scarcity. Farmers’ response to water scarcity insight also showed that it directly impacts on the economic sector. Farmers always practice numerous methods for adaptation of farming to climate change susceptibility in which water scarcity is a major concern (Tang et al. 2013; Fahad and Wang 2018).
Most of the developing countries including Pakistan, India, Africa and Bangladesh are using water with worsened quality due to man-made activities day by day (Chabukdhara et al. 2017; Li et al. 2017; Yousaf et al. 2016b). Pakistan is situated in southern Asia with arid to semi-arid climatic conditions in different areas. The large population is facing a lot of water-related problems due to urbanization (Azizullah et al. 2011). In Pakistan, water availability is continuously decreasing; it will further drop to 877 m3/annum which will shockingly decrease to 660 to 575 ft3 by year 2025 and 2050 respectively. In KPK <half of the six million population in different districts have no access to clean water due to high contamination of metals from adjacent sources (Khan et al. 2013a). In Baluchistan and Sindh, the groundwater table is reducing by 3.5 m, and soon, it will be entirely exhausted (Khanoranga and Khalid 2019; Van Steenbergen et al. 2015; Khair et al. 2015). Numerous researchers (Shakoor et al. 2018; Khalid et al. 2018; Daud et al. 2017) studied the water quality of different districts of Punjab including Sheikhupura (73%), Lahore (100%), Gujranwala (64%), Multan (94%), Kasur (100%) and Bahawalpur (88%) and found that the water quality of these districts exceeded the limit of arsenic in groundwater; diarrhoea was also observed due to the deteriorated water quality. Currently, arsenic is becoming the major pollutant in various surface and groundwater (Baig et al. 2010a; Arain et al. 2009; Fatmi et al. 2009; Farooqi et al. 2007). Faisalabad is recognised as a contaminated industrial (industries including textile, ice, pharmaceutical, flour, cotton, sugar and food) city because of insufficient treatment facilities and < 90% of samples were above the WHO limits with respect to K, Na, Cl, total dissolved solids (TDS) and SO4 (Daud et al. 2017).
Therefore, it is necessary to assess the concentration of different pollutants and their health risks in water. Globally, the use of different statistical analysis, indices and health risk assessment in different water bodies have been reported earlier (Avino et al. 2011; Wen et al. 2011; Escudero et al. 2010). Water quality index (WQI) proved an easy approach to measure quality of water in a quantitative way. It changes the concentration of pollutants to sub-indexes and then convert these into one numerical score, based on their quality (Fox 2014). It makes it easy to assess water quality for policymakers to comprehend the condition of a freshwater body or aquatic environment (Feng et al. 2015). Mostly, different multivariate and univariate statistical analyses which include principal component analysis and inter-metal correlation are used for analysing complex and huge data matrices. These methods have been used previously in numerous studies to investigate the contamination and health impacts (Wunderlin et al. 2001; Muhammad et al. 2011; Khan et al. 2013b).
The objective of the present study was to identify the quality and risk assessment from different surface and drinking water sources, through multivariate indexes and risk assessments in an industrial and populous city where there is no data available on these selected areas with quantification of pollution and health risk assessment in children and adults.
Methodology
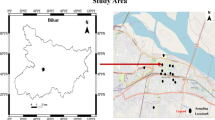
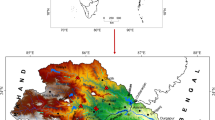
Study area
In Punjab, Faisalabad is accounted as the second mega metropolitan with a rising population. The accounted population of the city was 3.2 million in 2015 at 3.58% growth rate. It comprised of a 157-km2 area and is located at Rechna Doab (Awais et al. 2017). The intensity of rainfall was recorded at 408 mm per year. The highest temperature was recorded at 45 °C and the documented wind speed was 94 mph (Ali et al. 2017). Figure S1 shows the sample collection sites in Faisalabad city.
Sampling and laboratory analysis
Drinking water samples (n = 48) collected from tap water and hand pumps. Surface water samples (n = 37) collected from the Chenab river (n = 9) and canals (Jhang Branch Upper Canal n = 8, Rakh Branch Canal n = 9, Gugera Branch Canal n = 11) were collected from Faisalabad to identify the water quality for drinking and irrigation purposes. Samples were collected in pre-washed plastic bottles and brought to the laboratory for analysis of selected parameters including physical, chemical, biological and trace metal analyses according to the standard method of APHA (American Public Health Association) (2012) (Table S1 supplementary information).
Water quality index
Water quality index (WQI) was calculated by following different steps. WQI was firstly proposed by Horton (1965); later, it developed into different methods (Alobaidy et al. 2010). A total of 19 parameters were selected and were assigned their weight by considering previous studies. Dividing each assigned weight with the total assigned weight of all parameters gave the value of relative weight (RW) (Table 1). Qi was calculated by the following formula:
where Qi is the quality rating obtained from assigned weight, Ci is the concentration of parameters and Si is the standard value given by WHO.
To calculate the water quality index, the sub-indices (SIi) of every parameter were calculated prior. This value was used in calculating the quality index by the given formula
The classification of WQI, described by Goher et al. (2014), is as follows: a value 0 to 25 WQI was categorized as excellent water, between 26 and 50 is good, from 51 to 75 is poor, and between 56 to 100 is considered very poor, while above 100, water becomes unsuitable for drinking.
Water quality for irrigation
Surface water quality was evaluated by calculating the salinity hazard and sodium (alkalinity) hazard (SAR) and magnesium absorption ratio (MAR). Xiao et al. (2019) divided salinity hazard into four classes: if electrical conductivity is less than 250 μS/cm, it is considered low (C1); if the value lies between 250 and 750 μS/cm, it is considered as medium (C2); it is categorized as high if EC is found between 750 and 2250 μS/cm (C3); and it is considered very high if the value of EC is found above 2250 μS/cm (C4). Sodium (alkalinity) hazard (SAR) is categorised into four classes, as mentioned by Raju et al. (2011): (S1) low if the value of SAR is less than 10; (S2) medium if between 10 and 18; (S3) high if between 18 and 26; and (S4) considered very high if SAR is more than 26. SAR was calculated by using the following formula in which cation and anion concentration was taken in milliequivalents per liter:
Magnesium absorption ratio was also calculated by using the following formula (Obiefuna and Sheriff 2011):
The acceptable level for MAR is 50 meq/L; above this level, the water is considered unsuitable.
Health risk assessment
Non-carcinogenic risk assessment
There are three exposure routes of heavy metals in the human body including oral ingestion, dermal interaction and inhalation (Agency for Toxic Substances, Disease Registry (ASTDR) 2007). Average daily dose (ADD) was computed by using following formula
where C was the concentration of metals (mg/L), the water consumption rate (IR) was 2 L day−1 for adults and 0.63 L day−1 for children, the values 72 kg for adults and 15 kg for children were considered average body weight (BW) (Rehman et al. 2018), the frequency of exposure (EF) which was 350 days year−1, ED was the duration of exposure (70 years for adults and 6 years for children) (USEPA 2004) and the average time (AT) for adults 25,550 days and for children 2190 days were taken for non-carcinogenic risk assessment, while for carcinogenic risk, it was 25,550 days for both adult and children (USEPA 2014).
To evaluate non-carcinogenic risk value, the hazard quotient of average daily dose was calculated, which was assumed to be the threshold value. It was calculated by dividing the ADD with (RfD) oral reference dose (Table 2) (United State Environmental Protection Agency (USEPA) 1992).
Carcinogenic risk assessment
The probability of producing cancer risk is identified due to the presence of any metal. It was calculated by the multiplication of cancer slope factor (CSF) (Table 2) with lifetime average daily dose (LADD). Here, LADD was calculated with an AT value of 25,550 both in children and adults (USEPA 2014). Cancer risk is high with an at-risk value reaching 10−3 (Wei et al. 2015). Carcinogenic risk was evaluated only for As, Cr and Ni, due to accessibility of cancer slope factor values.
Principal component analysis (PCA) combined with cluster analysis (CA) were completed by Origin 2017 software, while R software was used for correlation matrix.
Results and Discussion
Overall physiognomies of water parameters
Drinking and surface water samples (n = 48, n = 37 respectively) from different locations were analysed for physicochemical and biological parameters and metal values. Average concentrations of all drinking and surface water parameters are shown in Table 3. Management of groundwater is significantly affected by these physicochemical parameters (Kattan 2018). Average concentrations of some physical parameters in drinking water include pH (6.93 ± 0.16), chloride (431.8 ± 343.8), TDS (1275.5 ± 773) and phosphate (0.22 ± 0.13), and in groundwater, turbidity (32.21 ± 18.95), electrical conductivity (297.08 ± 108.34) and F (3.49 ± 0.74) were higher than their permissible standard values. Increased value of pH in water may cause a decrease in the metal toxicity (Aktar et al. 2010). A high concentration of TDS in water is the root cause of sewage and industrial effluent discharge. (Phiri et al. 2005; Rim-Rukeh et al. 2006). More TDS increases the level of COD and BOD in water which ultimately impact on dissolve oxygen (DO) which contribute in gastro-intestinal irritation, alter taste and corrosion etc. (Patil et al. 2012; Mahananda et al. 2010). Increased concentration of chloride applies osmotic pressure in marine living organisms and change the taste of water, and also cause increased blood pressure and hypertension between individuals (Kattan 2018). Correlation matrix was measured in drinking and surface water parameters (Figure S2 and S3). In drinking water, calcium strongly correlates with sulphate, magnesium and hardness, sulphate with total dissolved solids while electrical conductivity with chloride and chloride with sodium and potassium has a strong correlation. This can be also supported by principal component analysis and cluster analysis in Figure 1a and 2a. In surface water samples COD has strong correlation with temperature, TDS, EC and NO2, Cl has significant correlation with DO and hardness while Fe was correlated with DO also shown their variance in principal component analysis and cluster analysis (Figs. 1b and 2b). Biological parameters including total coliform (114.1 ± 16.4) and E. coli (106.8 ± 12.7 and 479 ± 161) in drinking and surface water were many folds higher than WHO and PEQ permissible limits (0/100 mL). Drinking water is highly polluted with numerous anthropogenic activities in largely populated cities of Pakistan like Lahore, Rawalpindi, Karachi, Peshawar, Kasur, Faisalabad, Gujrat and Sialkot and cannot be suggested for human intake (Bhutta et al. 2002; Mumtaz et al. 2010; Azizullah et al. 2011). A was study conducted by PCRWR (2005) in metropolises of Pakistan and stated that 35% and 65% of groundwater samples were polluted with E. coli and total coliform, respectively, while surface water samples had 100% contamination of total coliform and E. coli. Another research was conducted by Khan et al. (2018) on bacterial contamination of the Swat river, Pakistan, and found high faecal contamination in surface water that could be credited to increasing urbanization at downstream, direct discharge of municipal effluents, excreta from human beings and agricultural runoffs which may spread possible health risks in the native communal. As (0.032 ± 0.03) and Ni (0.04 ± 0.03) were found higher in drinking water, while in surface water, As (0.013 ± 0.02) and Cr (0.24 ± 0.08) were higher than their permissible limits. The major cause of metal pollution is anthropogenic activity which decreases the water quality (Noreen et al. 2017). Ingestion of Ni-sulphate and Ni-chloride can be a reason of lethal cardiac capture and other major health complications (Muhammad et al. 2011). Karavoltsos et al. (2008) determined the value of nickel in surface water which exceeded 2.1% than Greece standards. In many national and international health and environmental organisations, it is admitted that arsenic is one of the highest cancer-causing and toxic pollutants which poses an extreme risk to the environmental and health (Rafiq et al. 2018). Arsenic exposure (acute and chronic) results in As-associated illness called arsenicosis and their adverse influences on health strongly depend on the dietary status of the exposed living being (Shahid et al. 2018). Arsenic in groundwater with a higher level was reported in many studies, which implicated geohydrological, biogeochemical and geothermal factors, telling arsenic is mobilised in aquifers by numerous arsenic-bearing oxides (Abbas et al. 2018; Mehmood et al. 2017; Shakoor et al. 2016; Brahman et al. 2013; Baig et al. 2010b; Singh 2006). This type of non-point sources of pollution could be accountable too for the high concentration of heavy metals in water, like deposition through the atmosphere becomes a reason for seepage of some heavy metals in different underground resources of water (Ali et al. 2017).

Principal component analysis for a drinking water and b surface water

Cluster analysis for a drinking water and b surface water samples
Table 4 presents the comparison of metal concentration in water with other national and international studies. Arsenic was found higher in the present study in comparison with others except Ghaderpoori et al.’s (2018) study in Iran and Kumari et al. (2017) study in India. Cadmium was found higher in Kohistan northern Pakistan (Muhammad et al. 2011), Peninsular Malaysia (Azrina et al. 2011) and Bangladesh (Rahman et al. 2016), while lower in all other studies especially in Swat and Quetta in Pakistan (Khan et al. 2013b; Khanoranga and Khalid 2019). Chromium was lower in South Africa as studied by Nuthunya et al. (2017) and higher in all other studies. Copper was higher in western Nigeria and Khorramabad, Iran (Ayandiran et al. 2018; Ghaderpoori et al. 2018), and lower in all other studies. Lead was found lower in the present study except in Peninsular Malaysia (Azrina et al. 2011). Nickel values were higher than those in Charsadda (Khan et al. 2013a), northern Pakistan (Muhammad et al. 2011), Chinese Loess Plateau (Xiao et al. 2019) and Malaysia (Azrina et al. 2011; Kato et al. 2010). Zinc values were found lower than those in northern Pakistan (Muhammad et al. 2011), western Nigeria (Ayandiran et al. 2018) and Iran (Ghaderpoori et al. 2018), and higher from those in India (Kumari et al. 2017). In the present study, all the samples were taken from residential areas, but due to massive industrialization and overpopulation, the underground water characteristics deteriorated with the passage of time (Noreen et al. 2017; Ali et al. 2017; Yamin et al. 2015). Overall concentration was found lower than those in other studies in Pakistan but higher than those in other different countries. Increased concentration of these heavy metals might be credited to anthropogenic activities mainly improper agriculture runoff (Kumari et al. 2017).
Assessment of Water pollution
Water quality index was determined for a comprehensive understanding about drinking water quality. WQI in all samples were ranged from 28 to119 with a mean value of 61.8 indicating poor water quality (Table 1). Out of 48 sites, three sites (6%) were identified as unsuitable water quality (>100 WQI) while 4 sites (8%) have very poor water quality ranged from 76 to 100 WQI and 27 sites (56%) have poor water quality with WQI < 50–75. All unsuitable water sites were located near the sewage drains which deteriorate the drinking water quality through seepage. A similar study was conducted by Xiao et al. (2019) and 3% of samples were found poor and 3% unsuitable for drinking purposes. Khanoranga and Khalid (2019) determined the ground water quality index of Baluchistan district and found that all selected sites were poor in quality for drinking purposes due to variations in some physicochemical parameters and the occurrence of several heavy metals from anthropogenic sources. Al-Mutairi et al. (2014) found that only 3.1% surface water samples had excellent WQI in 2010 which deteriorated after years of anthropogenic activity. Groundwater of Faisalabad is being contaminated by nearby industrial effluent and sewerage wastewater drains and showed a noteworthy increase by WHO drinking water standards (Yamin et al. 2015). Alobaidy et al. (2010) investigated WQI in Iraq and found that it was 75 in 2008 and increased to < 100 during 2009 which indicates that the preventive movements conducted by the establishments were not adequate to improve water quality.
In agricultural countries, water needs for irrigation are higher than those for domestic and drinking purposes. Numerous indices were developed for evaluating irrigation water quality from surface and groundwater sources, which were substantial methods and commonly used worldwide (Singh et al. 2018; Rana et al. 2018; Shooshtarian et al. 2018). Electrical conductivity and sodium absorption ratio were generally used reciprocally to determine the irrigation water quality (Awais et al. 2017). SAR was applied to river and canal water samples in China and found that the value of sodium (alkalinity) hazard ranged from 2.12 to 45.88 with average value 14.8 (Xiao et al. 2019). Out of 11, only 1 sample of the Gugera Branch Canal was found with S2 sodium (alkalinity) hazard with low salinity hazard and identified in zone C1–S2; two other sites also have medium salinity. Other sites including Chenab, Jhang and Rukh showed low SAR with low alkalinity hazard and were categorized in zones S1–C1 and S1–C2 (Fig. 3a). Magnesium absorption ratio (MAR) in all the sites were above 50 meq/L except for two sites of the Chenab river (Fig. 3b). Additionally, according to RSC values, 61.89% of samples were unfit for irrigation purposes in the study area. Crop yields were affected adversely with high magnesium contents as the soils become more saline (Obiefuna and Sheriff 2011). Rasool et al. (2016) evaluated the water quality for irrigation purposes and results of his study described that water quality was slightly appropriate at some points for irrigation purposes. Khanoranga and Khalid (2019) found that soil water availability was reduced by the high value of SAR which affected crop growth and lowered the major nutrient contents, i.e. calcium and magnesium. Water quality varied with average discharge also. The Jhang Branch Upper Canal discharge was 89 m3/s and 52 m3/s at the upstream end and downstream end, respectively. The Rakh Branch Canal discharge was 38 m3/s and 11 m3/s at the upstream end and downstream end, respectively. The Lower Gugera Branch Canal discharge was about 64 m3/s and 15 m3/s at the upstream end and downstream end, respectively. At the Chenab river, the minimum and maximum monthly average discharges were 51 m3/s in September and 1940 m3/s in July, respectively. Groundwater quality was investigated by Sarkar and Hassan (2006) for irrigation and detected that average water quality indices like pH, EC, SAR, MAR and TDS were in the permissible level for production of crops. A pictorial presentation of groundwater quality was presented by Raihan and Alam (2008) in the Sunamganj district and they found suitable water quality for irrigation. Obiefuna and Orazulike (2010) experimented on a similar study in the Yola area of Northeast Nigeria which also showed the ground water of that zone was appropriate for irrigation.

Water quality for irrigation purposes. a Sodium (alkalinity) and salinity hazard. b Magnesium absorption ratio
Health Risk Assessment
Hand pump and tap water are the major source of drinking water in Faisalabad. For drinking and surface water, average daily dose (ADD) and HQ (hazard quotient) indices were calculated for assessment of health risk of drinking and surface water in adults and children and were also calculated by other researchers like Kamunda et al. (2016) and Titilawo et al. (2018). Table 5 presents the mean value of ADD and HQ for non-carcinogenic and CAR for carcinogenic risk assessment in drinking and surface water respectively. The HQ values of arsenic (2.84E+00, 4.30E+00) in drinking water, while in surface water arsenic (1.15E+00, 1.75E+00) and chromium (2.13E+00, 3.22E+00) were very near to threshold limit (HQ > 1) both in adult and children respectively. The order of HQ in drinking water samples were As > Cu, Cd> Cr, Ni, Pb, Zn > Fe in adult and As> Cu, Cd, Zn> Ni, Cd, Pb> Fe in children. Whereas, in surface water were As, Cr> Al, C> Ba, Ni, Pb, Fe> Cu, Zn in adults and As, Cr> Al, Ba, Cd> Ni, Pb, Fe> Cu, Zn in children. Rehman et al. (2018) determined that, in children, the HQ values of cobalt, copper, cadmium and lead were higher than those of permissible limits in groundwater of Chitral, Pakistan. The result of the present study was similar to that of Kavcar et al. (2009). Muhammad et al. (2011) stated that the hazard quotient indices for metals indicated no risk to local inhabitants compared with those of earlier studies but the hazard quotient indices of Zn, Pb, Ni, Cu and Cd were inclined to be more than what Kavcar et al. (2009) reported in drinking water and what Lim et al. (2008) reported in surface water. Xiao et al. (2019) reported that the HQ > 1 in arsenic especially in children were higher than that in adults, indicating that in a similar environment, children are more susceptible than adults. The presence of arsenic in drinking water in the long run can cause possibly cancer-causing effects and skin lesions, hypertension, diabetes, neuropathy, etc. Coal mining/usage and the arid weather can also lead to arsenic pollution (He and Charlet 2013; Xiao et al. 2016). Titilawo et al. (2018) estimated the hazard index of river water which indicated that no non-carcinogenic consequence in the inhabitant would rise by metal exposure in his study area.
Hu et al. (2012) stated that the hazard is supposed to begin in humans if the value of cancer risk is greater than 1 × 10−4. In the present study, the values for cancer risk in drinking water was higher in As (1.28E−03) in adults, while in surface water samples, Cr was found higher (3.20E+00) than cancer the threshold limit (Table 5). Arsenic and chromium posed a high risk of carcinogenicity in adults while Nickel was also found very close to the tolerable value of carcinogenicity. Rehman et al. (2018) reported that CR above the range of carcinogenicity for these metals in the order cobalt > cadmium > chromium > nickel happened in adults and children. Cancer risk was applied in the northern side of Pakistan and resulted that 1 person in every 225,836 children and 314,206 adults might be at risk (Muhammad et al. 2011). Exposure of metal in drinking water may cause carcinogenic effects which can be lethal for the local community.
According to the results of the present study, drinking water quality was considered poor. This is correlated with health risk assessment. Poor drinking water quality leads to serious health risks in adults and children which can lead to carcinogenicity, especially in the presence of metals. The major source of contamination in water is heavy industries with no treatment facility and regular monitoring. A study conducted by Rehman et al. (2018) indicated that by consuming water for drinking and irrigation purposes, the inhabitants are more prone to different diseases including hypertension, stomach cancer, lung cancer, gastroenteritis, anaemia, cardiac arrest and intellectual disabilities in the area of industrial, agricultural and mining activities. As opposed to Aelion et al.’s (2008) report that city areas are extremely polluted, the suburban area might also pose metals of human-driven origin (using pesticide and industrial activities).
Conclusion
The present study thoroughly describes the water pollution and associated health risks in the metropolis industrial city of Pakistan. Most of the parameters including physico-chemical and biological and metals (chloride, total dissolved solids, bacteriological contamination, arsenic and nickel and chromium) exceeded the World Health Organization and Punjab environment quality standard permissible limits. WQI showed poor water quality in most of the sites where major industries occur and deteriorate water to the level where it can cause severe health hazards. The order for poor surface water quality in barrages and rivers was as follows: GBC >RBC >JBC > Chenab river, mainly depending on the average flow rate. Drinking water quality was found poor in more than 56% of samples due to major industrial pollution in the area. Irrigation water quality was medium in the case of sodium alkalinity hazard and high in the case of magnesium absorption. Non-carcinogenic and carcinogenic risk was found in children and adults for arsenic, both in drinking water and surface water. The values of hazard quotient (HQ) and CRA were more than the probable hazard which occurred in children and adults.
The industrial and domestic wastewater badly impacted on ground water quality and created an alarming situation for the local inhabitants’ health and environment. Preventive measures and monitoring are supposed to be compulsory to eliminate the health hazard in the local population. The study will be of benefit to the provision and implementation of proper monitoring and public policies in order to approve integrated and sustainable water development and to minimise the health hazards in the study area. The study is further recommended to evaluate the organic pollutants in this industrial area especially pesticides which can cause major health problems.
References
Abbas Q, Yousaf B, Liu G, Ali MU, Munir MAM, Zia-ur-Rehman M, Husain SA (2017) Evaluating the health risks of potentially toxic elements through wheat consumption in multi-industrial metropolis of Faisalabad, Pakistan. Environ Sci Pollut Res 24:26646–26657
Abbas G, Murtaza B, Bibi I, Shahid M, Niazi NK, Khan MI, Amjad M, Hussain M (2018) Arsenic uptake, toxicity, detoxification, and speciation in plants: physiological, biochemical, and molecular aspects. Int J EnvironRes Public Health 15:59
Aelion CM, Davis HT, McDermott S, Lawson AB (2008) Metal concentrations in rural topsoil in South Carolina: potential for human health impact. Sci Total Environ 402:149–156
Agency for Toxic Substances, Disease Registry (ASTDR) (2007) Toxicological profile for arsenic. U.S. Department of Health and Human Services, Atlanta, Georgia, pp. 2000
Aktar MW, Paramasivam M, Ganguly M, Purkait S, Sengupta D (2010) Assessment and occurrence of various heavy metals in surface water of Ganga river around Kolkata: a study for toxicity and ecological impact. EnvironMonit Assess 160(1-4):207–213
Ali J, Kazi TG, Tuzen M, Ullah N (2017) Evaluation of mercury and physicochemical parameters in different depths of aquifer water of Thar coal field, Pakistan. Environ Sci Pollut Res:1–10
Al-Mutairi N, Abahussain A, El-Battay A (2014) Application of water quality index to assess the environmental quality of Kuwait Bay. International Conference on Advances in Agricultural, Biological & Environmental Sciences (AABES-2014) Oct 15-16, 2014 Dubai (UAE)
Alobaidy AHM, Abid HS, Maulood BK (2010) Application of water quality index for assessment of Dokan lake ecosystem, Kurdistan region, Iraq. J Water Resour and Protec 2:792–798
APHA (American Public Health Association) (2012) Standard methods for the examination of water and waste Water, 17th edn. American Public Health Association, Washington DC
Arain MB, Kazi TG, Baig JA, Jamali MK, Afridi HI, Jalbani N, Sarfraz RA, Shah AQ, Kandhro GA (2009) Respiratory effects in people exposed to arsenic via the drinking water and tobacco smoking in southern part of Pakistan. Sci Total Environ 407:5524–5530
Arain MB, Ullah I, Niaz A, Shah N, Shah A, Hussain Z, Tariq M, Afridi HI, Baig JA, Kazi TG (2014) Evaluation of water quality parameters in drinking water of district Bannu, Pakistan: multivariate study. Sustain Water Qual Ecol 3-4:114–123
Arizhibowa F (2011) A human health risk assessment of heavy metal bioaccumulation in Nile tilapia Oreochromis niloticus from Lake Chivero, Zimbabwe. MSc thesis. University of Zimbabwe, Harare
Avino P, Capannesi G, Rosada A (2011) Ultra-trace nutritional and toxicological elements in Rome and Florence drinking waters determined by instrumental neutron activation analysis. Microchem J 97:144–153
Awais M, Arshad M, Shah SHH, Anwar-Ul-Haq M (2017) Evaluating groundwater quality for irrigated agriculture: spatio-temporal investigations using GIS and geostatistics in Punjab, Pakistan. Arab J Geosci 10(23):510
Ayandiran TA, Fawole OO, Dahunsi SO (2018) Water quality assessment of bitumen polluted Oluwa River, South Western Nigeria. Water Resour Indus 19:13–24
Azizullah A, Khattak MNK, Richter P, Hader DP (2011) Water pollution in Pakistan and its impact on public health – a review. Environ Int 37:479–497
Azrina A, Khoo HE, Idris MA, Amin I, Ramzan MR (2011) Major inorganic elements in tap water samples in Peninsular Malaysia. Malays J Nutr 17:271–276
Baig JA, Kazi TG, Shah AQ, Kandhro GA, Afridi HI, Arain MB, Jamali MK, Jalbani N (2010a) Speciation and evaluation of arsenic in surface and ground water samples: a multivariate case study. Ecotoxicol Environ Saf 73:914–923
Baig JA, Kazi TG, Shah AQ, Kandhro GA, Afridi HI, Khan S, Kolachi NF (2010b) Biosorption studies on powder of stem of Acacia nilotica: removal of arsenic from surface water. J Hazard Mater 178:941–948
Bhutta MN, Ramzan M, Hafeez CA, (2002) Ground water quality and availability in Pakistan. Islamabad, Pakistan: Pakistan Council for Research in Water Resources (PCRWR)
Bortey-Sam N, Nakayama SMM, Ikenaka Y, Akoto O, Baidoo E, Mizukawa H, Ishizuka M (2015) Health risk assessment of heavy metals and metalloid in drinking water from communities near gold mines in Tarkwa, Ghana. Environ Monit Assess 187:397
Brahman KD, Kazi TG, Afridi HI, Naseem S, Arain SS, Ullah N (2013) Evaluation of high levels of fluoride, arsenic species and other physicochemical parameters in underground water of two sub districts of Tharparkar, Pakistan: a multivariate study. Water Res 47:1005–1020
Chabukdhara M, Gupta SK, Kotecha Y, Nema AK (2017) Ground water quality in Ghaziabad district, Uttar Pradesh, India: multivariate and health risk assessment. Chemosphere 179:167–178
Chowdhury S, Jafar Mazumder MA, Al-Attas O, Husain T (2016) Heavy metals in drinking water: occurrences, implications, and future needs in developing countries. Sci Total Environ 569-570:476–488
Daud MK, Nafees M, Ali S, Rizawan M, Bajwa RA, Shakoor MB, Arshad MU, Chatha SAS, Deeba F, Murad W, Malook I, Zhu SJ (2017) Drinking water quality status and contamination in Pakistan. Biomed Res Int 2017:1–18. https://doi.org/10.1155/2017/7908183
Dong ZW, Qin DH, Qin X, Cui JY, Kang SC (2017) Changes in precipitating snow chemistry with seasonality in the remote Laohugou glacier basin, western Qilian Mountains. Environ Sci Pollut Res 24:11404–11414. https://doi.org/10.1007/s11356-017-8778-y
Escudero LA, Martinez LD, Salonia JA, Gasquez JA (2010) Determination of Zn(II) in natural waters by ICP-OES with on-line preconcentration using a simple solid phase extraction system. Microchem J 95:164–168
Fahad S, Wang J (2018) Farmers’ risk perception, vulnerability, and adaptation to climate change in rural Pakistan. Land Use Policy 79:301–309
FAO (2013) FAO statistical yearbook. World food and agriculture. Food and Agriculture Organization of the United Nations (FAO), Rome 978-92-5-107396-4
Farooqi A, Masuda H, Firdous N (2007) Toxic fluoride and arsenic contaminated groundwater in the Lahore and Kasur districts, Punjab, Pakistan and possible contaminant sources. J Environ Pollut 145:839–849
Fatmi Z, Azam I, Ahmed F, Kazi A, Gill AB, Kadir MM, Ahmed M, Ara N, Janjua NZ (2009) Core group for arsenic mitigation in Pakistan, health burden of skin lesions at low arsenic exposure through groundwater in Pakistan. Is river the source? Environ Res 109:575–581
Feng Y, Linga L, Yanfengb L, Youa Z, Musonga C, Xiganga X (2015) A dynamic water quality index model based on functional data analysis. Ecol Indic 57:249–258
Fox DR (2014) Probability weighted indices for improved ecosystem report card scoring. Environmetrics 25:351–360
Ghaderpoori M, kamarehie B, Jafari A, Ghaderpoury A, Karami M (2018) Heavy metals analysis and quality assessment in drinking water – Khorramabad city, Iran. Data in Brief 16:685–692
Ghorade IB, Lamture SV, Patil SS (2014) Assessment of heavy metal content in Godavari River water. Int J Res Appl Nat Soc Sci 2:23–26
Goher ME, Hassan AM, Abdel-Moniem IA, Fahmy AH, El-Sayed SM (2014) Evaluation of surface water quality and heavy metal indices of Ismailia Canal, Nile River, Egypt. Egypt J Aquat Res 40:225–233
Grimm NB, Faeth SH, Golubiewski NE, Redman CL, Wu J, Bai X, Briggs JM (2008) Global change and the ecology of cities. Science 319(5864):756–760
He J, Charlet L (2013) A review of arsenic presence in China drinking water. J Hydrol 492:79–88
Horton RK (1965) An index number system for rating water quality. J Water Pollut Control Fed 37(3):300–306
Hu X, Zhang Y, Ding Z, Wang T, Lian H, Sun Y, Wu J (2012) Bio accessibility and health risk of arsenic and heavy metals (Cd, Co, Cr, Cu, Ni, Pb, Zn and Mn) in TSP and PM2. 5 in Nanjing, China. Atmos Environ 57:146–152
Hussain Y, Ullah SF, Akhter G, Aslam AQ (2017a) Groundwater quality evaluation by electrical resistivity method for optimized tubewell sites election in an agostressed Thal Doab Aquifer in Pakistan. Model Earth. Sy. Env 3(1):15
Hussain Y, Ullah SF, Hussain MB, Aslam AQ, Akhter G, Martinez-Carvajal H, Cárdenas-Soto M (2017b) Modelling the vulnerability of groundwater to contamination in an unconfined alluvial aquifer in Pakistan. Environ Earth Sci 76(2):84
Ishaque, W., Shaikh, S., 2017. Water and energy security for Pakistan are prospective analysis. Grassroots 51(1)
Jia H, Yao H, Yu SL (2013) Advances in LID BMPs research and practices for urban runoff control in China. Front Environ Sci and Engin 7(5):709–720
Kamunda C, Mathuthu M, Madhuku M (2016) Health risk assessment of heavy metals in soils from Witwatersrand gold mining basin, South Africa. Int J Environ Res Public Health 13:663
Karavoltsos S, Sakellari A, Mihopoulos N, Dassenakis M, Scoullos M (2008) Evaluation of the quality of drinking water in regions of Greece. Desalination 224(1–3):317–329
Kato M, Onuma S, Katoa Y, Thangac ND, Yajima I, Hoque MZ et al (2010) Toxic elements in well water from Malaysia. Toxicol Environ Chem 92:1609–1612
Kattan Z (2018) Using hydrochemistry and environmental isotopes in the assessment of ground water quality in the Euphrates alluvial aquifer. Syria Environ Earth Sci 77(2):45
Kavcar P, Sofuoglu A, Sofuoglu SC (2009) A health risk assessment for exposure to trace metals via drinking water ingestion pathway. Int J Hyg Environ Health 212:216–227
Khair SM, Mushtaq S, Culas RJ, Hafeez M (2012) Groundwater markets under the water scarcity and declining water table conditions: the upland Balochistan Region of Pakistan. Agric Syst 107:21–32
Khair SM, Mushtaq S, Reardon-Smith K (2015) Groundwater governance in a water starved country: public policy, farmers’ perceptions, and drivers of tubewell adoption in Balochistan. Pakistan Ground Water 53(4):626–637
Khalid S, Murtaza B, Shaheen I, Ahmad I, Ullah MI, Abbas T, Rehman F, Ashraf MR, Khalid A, Abbas S, Imran M (2018) Assessment and public perception of drinking water quality and safety in district Vehari, Punjab, Pakistan. J Clean Prod 181:224–234
Khan S, Shahnaz M, Jehan N, Rehman S, Shah MT, Din I (2013a) Drinking water quality and human health risk in Charsadda district, Pakistan. J Clean Prod 60:93–101
Khan K, Lu Y, Khan H, Zakir S, Ihassanullah KS, Khan AA, Wei L, Wang T (2013b) Health risk associated with heavy metals in the drinking water of Swat, northern Pakistan. J Environ Sci 25(10):2003–2013
Khan A, Husain V, Bakhtiari AE, Khan H, Arsalan M (2017) Groundwater arsenic contamination in semi-urban areas of Tando Muhammad Khan District: a case study from deltaic flood plain of Sindh, Pakistan. Sust Environ 2(2):171
Khan K, Lu Y, Saeed MA, Bilal H, Sher H, Khan H, Ali J, Wang P, Uwizeyimana H, Baninla Y, Li Q, Liu Z, Nawab J, Zhou Y, Su C, Liang R (2018) Prevalent fecal contamination in drinking water resources and potential health risks in Swat, Pakistan. J Environ Sci 72:1–12
Khanoranga, Khalid S (2019) An assessment of groundwater quality for irrigation and drinking purposes around brick kilns in three districts of Balochistan province, Pakistan, through water quality index and multivariate statistical approaches. J Geochem Explor 197:14–26
Kubicz J, Pawełczyk A, Lochynski P (2018) Environmental health risk posed by contamination of the individual water wells. Chemosphere 208:247–256
Kumari B, Kumar V, Sinha AK, Ahsan J, Ghosh AK, Wang H, Deboeck G (2017) Toxicology of arsenic in fish and aquatic systems. Environ Chem Lett 15(1):43–64
Li J, Li FD, Liu Q, Zhang Y (2014) Trace metal in surface water and ground water and its transfer in a Yellow River alluvial fan: evidence from isotopes and hydrochemistry. Sci Total Environ 472:979–988
Li P, Tian R, Xue C, Wu J (2017) Progress, opportunities, and key fields for groundwater quality research under the impacts of human activities in China with a special focus on western China. Environ Sci Pollut Res 24(15):13224–13234
Lim HS, Lee JS, Chon HT, Sager M (2008) Heavy metal contamination and health risk assessment in the vicinity of the abandoned Songcheon Au–Ag mine in Korea. J Geochem Explor 96:223–230
Mahananda M, Mohanty B, Behera N (2010) Physico-chemical analysis of surface and ground water of Bargarh District, Orissa, India. Int J Res Rev Appl Sci 2:284–295
Mehmood T, Bibi I, Shahid M, Niazi NK, Murtaza B, Wang H, Ok YS, Sarkar B, Javed MT, Murtaza G (2017) Effect of compost addition on arsenic uptake, morphological and physiological attributes of maize plants grown in contrasting soils. J Geochem Explor 178:83–91
Muhammad S, Shah MT, Khan S (2011) Health risk assessment of heavy metals and their source apportionment in drinking water of Kohistan region, northern Pakistan. Microchem J 98:334–343
Mukatea S, Panaskara D, Wagha V, Muleyb A, Jangama C, Pawarc R (2018) Impact of anthropogenic inputs on water quality in Chincholi industrial area of Solapur, Maharashtra, India. Groundwater Sustain Develop 7:359–371
Mumtaz MW, Adnan A, Mukhtar H, Nawaz K, Raza A, Ahmad Z (2010) Estimation of bacteriological levels in surface water samples to evaluate their contamination profile. Environ Monit Assess Published online
Nawab J, Khan S, Xiaoping W, Rahman A, Ali H, Qamar Z, Khan A (2018) Spatial distribution of toxic metals in drinking water sources and their associated health risk in district buner, Northern Pakistan. Hum Ecol Risk Assess Int J 24(3):615–626
Noreen M, Shahid M, Iqbal M, Nisar J (2017) Measurement of cytotoxicity and heavy metal load in drains water receiving textile effluents and drinking water in vicinity of drains. Measurement 109:88–99
Nuthunya LN, Masheane ML, Malinga SP, Nxumalo EN, Mamba BB, Mhlanga SD (2017) Determination of toxic metals in drinking water sources in the Chief Albert Luthuli Local Municipality in Mpumalanga, South Africa. Phys Chem Earth 100:94–100
Obiefuna GI, Orazulike DM (2010) Assessment of groundwater quality of Yola area for irrigation purposes water resources. J Nigerian Assoc Hydrogeol 20(1):32–52
Obiefuna GI, Sheriff A (2011) Assessment of Shallow Ground Water Quality of Pindiga Gombe Area, Yola Area, NE, Nigeria for Irrigation and Domestic Purposes. Research Journal of Environmental and Earth Sciences 3(2):131–141
Patil PN, Sawant DV, Deshmukh R (2012) Physico-chemical parameters for testing of water—a review. Int J Environ 3:1194
PCRWR (2005) Annual Report 2005–2006, part 2. Islamabad, Pakistan: Pakistan Council for Research in Water Resources PCRWR; 2008a. Available at http://www.pcrwr.gov.pk/Annual%20Reports/New%20Annual%20Repot%202005-06_2.pdf. Accessed 12 Sep 2018
Phiri O, Mumba P, Moyo BHZ, Kadewa W (2005) Assessment of the impact of industrial effluents on water quality of receiving Rivers in urban areas of Malawi. Int J Environ Sci Technol 2(3):237–244
Qadir M, Malik NR, Husain ZS (2007) Spatio-temporal variations in water quality of Nullah Aik-tributary of the river Chenab, Pakistan. Environ Monit Assess 140:43–59
Rafiq M, Shahid M, Shamshad S, Khalid S, Niazi NK, Abbas G, Saeed MF, Ali M, Murtaza B (2018) A comparative study to evaluate efficiency of EDTA and calcium in alleviating arsenic toxicity to germinating and young Vicia faba L. seedlings. J Soils Sediments 18:2271–2281
Rahman MM, Islam MA, Khan MB (2016) Status of heavy metal pollution of water and fishes in Balu and Brahmaputra rivers. Progress Agric 27(4):444–452
Raihan F, Alam JB (2008) Assessment of groundwater quality in sunamganj Bangladesh Iranian. J Environ Health Sci Eng 6(3):155–166
Raju NJ, Shukla UK, Ram P (2011) Hydrogeochemistry for the assessment of groundwater quality in Varanasi: a fast-urbanizing center in Uttar Pradesh, India. Environ Monit Assess 173:279–300
Rana R, Ganguly R, Gupta AK (2018) Indexing method for assessment of pollution potential of leachate from non-engineered landfill sites and its effect on groundwater quality. Environ Monit Assess 190(1):46
Rasool A, Farooqi A, Masood S, Hussain K (2016) Arsenic in groundwater and its health risk assessment in drinking water of Mailsi, Punjab, Pakistan. Hum Ecol Risk Assess 22(1):187–202
Rehman I, Ishaq M, Ali L, Khan S, Ahmad I, Din I, Ullah H (2018) Enrichment, spatial distribution of potential ecological and human health risk assessment via toxic metals in soil and surface water ingestion in the vicinity of Sewakht mines, district Chitral, Northern Pakistan. Ecotoxicol Environ Saf 154:127–136
Rim-Rukeh A, Ikhifa OG, Okokoyo AP (2006) Effects of agricultural activities on the water quality of Orogodo River, Agbor Nigeria. J Appl Sci Res 2(5):256–259
Sarkar AA, Hassan AA (2006) Water quality assessment of a groundwater basin in Bangladesh for irrigation use. Pak J Biol Sci 9(9):1677–1684
Shahid M, Niazi NK, Dumat C, Naidu R, Khalid S, Rahman MM, Bibi I (2018) A meta-analysis of the distribution, sources and health risks of arsenic-contaminated groundwater in Pakistan. Environ Pollut 242:307–319
Shakoor MB, Niazi NK, Bibi I, Murtaza G, Kunhikrishnan A, Seshadri B, Shahid M, Ali S, Bolan NS, Ok YS (2016) Remediation of arsenic contaminated water using agricultural wastes as biosorbents. Crit Rev Environ Sci Technol 46:467–499
Shakoor A, Khan ZM, Farid HU, Sultan M, Khan AA, Ahmad I, Azmat M (2018) Groundwater vulnerability mapping in Faisalabad district using GIS based drastic model. MATEC web of conferences 246. https://doi.org/10.1051/matecconf/20182460100
Shooshtarian MR, Dehghani M, Margherita F, Gea OC, Mortezazadeh S (2018) Land use change and conversion effects on groundwater quality trends: an integration of land change modeler in GIS and a new ground water quality index developed by fuzzy multi-criteria group decision-making models. Food Chem Toxicol 114:204–214
Singh AK (2006) Chemistry of arsenic in groundwater of Gangese–Brahmaputra river basin. Curr Sci 91:599–606
Singh PK, Panigrahy BP, Verma P, Kumar B (2018) Evaluation of the surface water quality index of Jharia coal mining region and its management of surface water resources. Environ Pollut:429–437
Tang J, Folmer H, Xue J (2013) Estimation of awareness and perception of water scarcity among farmers in the Guanzhong Plain, China, by means of a structural equation model. J Environ Manag 126:55–62
Titilawo Y, Adeniji A, Adeniyi M, Okoh A (2018) Determination of levels of some metal contaminants in the freshwater environments of Osun State, Southwest Nigeria: a risk assessment approach to predict health threat. Chemosphere 211:834–843
United State Environmental Protection Agency (USEPA) (1992) Guidelines for exposure assessment Fed Regist 57 (104), 22888-22938, 1992
USEPA (2004) Risk assessment guidance for superfund volume 1. Human health evaluation. Manual (Part E, Supplemental guidance for dermal risk assessment). EPA/540/ R/99/005 Office of Superfund Remediation and Technology Innovation; U.S. Environmental Protection Agency, Washington, DC
USEPA (2014) Child-specific exposure scenarios examples. EPA/600/R-14/217F National Center for Environmental Assessment, Office of Research and Development, U.S. Environmental Protection Agency, Washington, DC 20460. www.epa.gov/ncea. Accessed 12 Sep 2018
Van Steenbergen F, Kaisarani AB, Khan NU, Gohar MS (2015) A case of groundwater depletion in Balochistan, Pakistan: enter into the void. J Hydrol 4:36–47
Vesali Naseh MR, Noori R, Berndtsson R, Adamowski J, Sadatipour E (2018) Groundwater pollution sources apportionment in the Ghaen Plain, Iran. Int J Environ Res Public Health 15(1):172
Wei H, Le Z, Shuxian L, Dan W, Xiaojun L, Lan J, Xiping M (2015) Health risk assessment of heavy metals and polycyclic aromatic hydrocarbons in soil at coke oven gas plants. Environ Eng Manag J 14:487–496
Wen X, Yang Q, Yan Z, Deng Q (2011) Determination of cadmium and copper in water and food samples by dispersive liquid–liquid microextraction combined with UV–vis spectrophotometry. Microchem J 97:249–254
Wunderlin DA, Diaz MP, Ame MV, Pesce SF, Hued AC, Bistoni MA (2001) Pattern recognition techniques for the evaluation of spatial and temporal variations in water quality. A case study: Suquia river basin (Cordoba, Argentina). Water Res 35:2881–2894
Xiao J, Jin ZD, Zhang F (2016) Spatial characteristics and controlling factors of chemical weathering of loess in the dry season in the middle Loess Plateau, China. Hydrol Process 30:4855–4869
Xiao J, Wangb L, Denga L, Jina Z (2019) Characteristics, sources, water quality and health risk assessment of trace elements in river water and well water in the Chinese Loess Plateau. Sci Total Environ 650:2004–2012
Yamin M, Nasir A, Sultan M, Ismail WIW, Shamshiri R, Akhbar FN (2015) Impact of sewage and industrial effluents on water quality in Faisalabad, Pakistan. Adv Environ Biol 9(18):53–58
Yousaf B, Amina, Liu G, Wang R, Imtiaz M, Rizwan MS, Zia-ur-Rehman M, Qadir A, Si Y (2016) The importance of evaluating metal exposure and predicting human health risks in urban-periurban environments influenced by emerging industry. Chemosphere. 150:79–89
Yousaf B, Liu G, Wang R, Imtiaz M, Zia-ur-Rehman, Munir MAM, Niu Z (2016b) Bioavailability evaluation, uptake of heavy metals and potential health risks via dietary exposure in urban-industrial areas. Environ Sci Pollut Res 23:22443–22453
Zeng XX, Liu YG, You SH, Zeng GM, Tan XF, Hu XJ, Hu X, Huang L, Li F (2015) Spatial distribution, health risk assessment and statistical source identification of the trace elements in surface water from the Xiang Jiang River, China. Environ Sci Pollut Res 22:9400–9412
Zhang T, Ruan J, Zhang B, Lu S, Gao C, Huang L, Bai X, Xie L, Gui M, Qiu R (2019) Heavy metals in human urine, foods and drinking water from an e-waste dismantling area: identification of exposure sources and metal-induced health risk. Ecotoxicol Environ Saf 169:707–713
Acknowledgments
The Chinese Academy of Science (CAS) is greatly acknowledged for providing the CAS-Young Scientist Award (2018FYB0002). We also greatly appreciate the efforts of Dr Habib Ullah, Dr Muhammad Ubaid Ali and Dr Qumber Abbas for the improvement of the manuscript.
Funding
This study was financially supported by the Fundamental Research Funds for the Central Universities (WK2080000103) and the China Postdoctoral Science foundation (2018M632552).
Author information
Authors and Affiliations
Corresponding author
Additional information
Responsible editor: Philippe Garrigues
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
ESM 1
(DOCX 662 kb)
Rights and permissions
About this article

Cite this article
Mahfooz, Y., Yasar, A., Sohail, M.T. et al. Investigating the drinking and surface water quality and associated health risks in a semi-arid multi-industrial metropolis (Faisalabad), Pakistan. Environ Sci Pollut Res 26, 20853–20865 (2019). https://doi.org/10.1007/s11356-019-05367-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11356-019-05367-9