
Abstract
Ambient air pollution had been shown strongly associated with cardiovascular diseases. However, the association between air pollution and myocardial infarction (MI) is inconsistent. In the present study, we conducted a time-series study to investigate the association between air pollution and MI. Daily air pollutants, weather data, and MI data were collected from January 2015 to December 2016 in Changzhou, China. Generalized linear model (GLM) was used to assess the immediate effects of air pollutants (PM2.5, PM10, NO2, SO2, and O3) on MI. We identified a total of 5545 cases for MI, and a 10-μg/m3 increment in concentrations of PM2.5 and PM10 was associated with respective increases of 1.636% (95% confidence interval [CI] 0.537–2.740%) and 0.805% (95% CI 0.037–1.574%) for daily MI with 2-day cumulative effects. The associations were more robust among males and in the warm season versus the cold one. No significant effect was found in SO2, NO2, or O3. This study suggested that short-term exposure to PM2.5 and PM10 was associated with the increased MI risks. Our results might be useful for the primary prevention of MI exacerbated by air pollutants.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Ambient air pollution, a heterogeneous group of particulate matters (PMs) and gaseous pollutants, represents a modifiable threat to human health (Chen et al. 2012; Gurung and Bell 2013) and has aroused general concern of the academia recently. Numerous epidemiological studies have demonstrated that exposure to air pollutants may increase the mortality, hospital admissions, and emergency visits for patients with cardiovascular diseases (Argacha et al. 2016; Nuvolone et al. 2011; Zhang et al. 2016). In specific, PMs with aerodynamic diameters < 10 μm (PM10) and < 2.5 (PM2.5) have been linked to deleterious effects on cardiovascular health. Transient elevations of PM2.5 and PM10 could increase the occurrence of ischemic heart disease hospital admissions, and moreover, increased cardiovascular mortality has also been associated with hourly peak PM2.5 concentration (Lin et al. 2017; Sohn et al. 2016; Stockfelt et al. 2017; Weber et al. 2016).
Myocardial infarction (MI), an acute and severe cardiovascular event, can cause damage to the heart and induce heart failure (Krumholz and Normand 2008). It is the leading cause of morbidity and mortality in Chinese populations (Zhou et al. 2016). MI caused more than 1 million deaths annually; this number in China will increase to 23 million by 2030 (Li et al. 2015; Yang et al. 2013). Without immediate medical attention, MI may result in a poor prognosis with nearly 25% dying within minutes and 40% within the first month (Ibanez et al. 2015). Due to the limitation in therapeutic regimen and the fatal outcomes, identifying modifiable risk factors for MI and taking effective countermeasures is of critical public health problem (Thiele et al. 2015). The previous studies indicated that diabetes, hypertension, obesity, smoking, high cholesterol levels, and physical inactivity contributed to MI (Mehta et al. 2015). Recently, MI was linked to air pollution (Roswall et al. 2017; Talbott et al. 2014). However, few studies, especially in China, have discussed the differences in the effects of the main air pollutants on MI risk.
With the rapid economic development that has occurred in the past years and as one of the most populous developing country, China is experiencing exacerbating air quality due to emissions from manufacturing industries, traffic, agriculture, and forest fires (Kan et al. 2009; Petaja et al. 2016; Rohde and Muller 2015). Changzhou is a prefecture-level city in southern Jiangsu province of China and locates on the southern bank of the Yangtze River. It is a part of the highly developed Yangtze Delta region of China extending from Shanghai going northwest, which now has more than 36 million inhabitants (Kerstens et al. 2009). The concentrations of PM2.5 and PM10 in Changzhou were higher than the national ambient air quality standard (35 μg/m3 for PM2.5 and 50 μg/m3 for PM10) (Li et al. 2008). Thus, Changzhou was chosen to study the effect of air pollutants on MI.
In this study, we performed an epidemiological time-series design to estimate the effect of main air pollutants on MI in Changzhou, China. In addition, the association of possible modifiers, including meteorological factors, demographic characteristics between air pollutants and MI were also evaluated. This work will help provide insights into the relationship between MI and air pollutants, especially particulate matters and implications for prevention of MI in Changzhou, China.
Methods
Data collection
Air pollution data, including PM10, PM2.5, nitrogen dioxide (NO2), sulfur dioxide (SO2), and ozone (O3), were obtained from the database of Changzhou Environmental Monitoring Center, from January 1, 2015 to December 31, 2016. This center established ten air quality monitoring stations in different administrative districts of Changzhou (Fig. 1). These stations are located away from major roads, industrial sources, buildings, or residential sources of emissions including coal, waste, or oil. Thus, the daily air pollution data collected from the monitoring stations can represent the background urban air pollution level. Furthermore, all the cases identified in this study resided less than 40 km from the nearest monitoring station, and it is appropriate to use the monitoring data to represent a good indicator of individual exposures (Dockery et al. 2005; Wellenius et al. 2012; Xie et al. 2015). Weather data regarding temperature (°C), wind speed (m/s), and relative humidity (%) were collected from Changzhou Meteorological Bureau and averaged daily.

Locations of air quality monitoring stations and weather monitoring station in Changzhou, 2015–2016
Daily MI data from January 1, 2015 to December 31, 2016 were obtained from the database of Changzhou Center for Disease Control and Prevention (CDC), which is a part of Changzhou-controlled network reporting system for chronic diseases. The data in this study were recorded according to The International Classification of Diseases, Revision 10 (ICD-10) and further categorized into acute myocardial infarction (I21) and subsequent myocardial infarction (I22). Daily MI counts were also classified by gender and age group (< 65, 66–85, and > 85 years old). Demographic data were collected from Changzhou Municipal Bureau of Statistics.
Statistical analysis
Daily MI counts, air pollutants concentrations, and meteorological data were linked by date for the subsequent time-series design, which was applied to explore the effects of each air pollutant on MI. Spearman’s correlation coefficient was used to determine the association between air pollutants and meteorological variables. To develop the basic model, the distribution pattern of daily MI numbers was investigated. Since the data followed a Poisson distribution, Poisson regression was applied in the generalized linear model (GLM) to analyze the effect of air pollutants on daily MI counts. To control the potential confounding effect, multivariable regression model was used, including the following: (1) a natural cubic smooth function of calendar time with three degrees of freedom (df) per year to exclude unmeasured long-term and seasonal trends; (2) natural smooth functions of the current day-to-day relative humidity (3 df) and average temperature (3 df) to control the weather confounding effects; (3) indicator variable was used for “day of the week (DOW)”. In addition, data with different modifiers stratified by sex and season (warm season as 1 May to 31 October and cold season as 1 November to 30 April) were also tested to separately analyze the effect of air pollutants on MI.
Moreover, a single-pollutant model was performed to explore the air pollution’s effects on MI with single-day lags (lag 0, 1, 2, 3, 4, 5, 6) and multiple-day lags (lag 0–1, 0–2, 0–3, 0–4, 0–5, 0–6). Two-pollutant model was developed to examine the stability of results. Smoothing function was applied to analyze the exposure-response relationship between the log-relative risk of daily MI numbers and air pollutant concentrations using a 0 df in single-pollutant model.
Statistical software R (version 3.2.3, R Foundation for Statistical Computing, Austria) was used for data analysis and result output. The baseline data were presented as mean ± standard deviation (SD) for continuous variables. All tests were two-sided, and P < 0.05 was considered as statistically significant.
Results
Descriptive analysis
Table 1 shows the basic demographic information of MI. There were 5545 MI cases recorded; of these, 63% were males and 81.1% were aged between 65 and 85. The daily average MI counts were 7.6 during study period (data not shown).
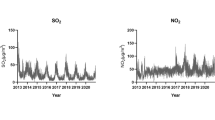
Table 2 reveals the summary statistics of daily air pollutants and weather conditions. The daily average concentrations for PM2.5, PM10, SO2, NO2, and O3 were 52.4, 86.0, 22.6, 38.9, and 90.2 μg/m3, respectively. The corresponding average concentrations of PM2.5 and PM10 in Changzhou were 2.1 and 1.6 times higher than the national ambient air quality standard (35 μg/m3 for PM2.5 and 50 μg/m3 for PM10). The daily temperature, wind speed, and relative humidity were 17.0 °C, 2.2 m/s, and 75.0%, respectively.
Table 3 illustrates the Spearman correlation coefficients among the air pollutants and weather conditions. They were positively correlated among five air pollutants, except O3. In addition, they were negatively correlated with temperature, wind speed, and humidity.
Estimated effects of air pollutants
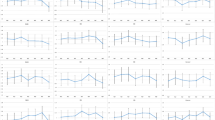
Figure 2 summarizes the estimated changes in daily MI counts associated with a 10-μg/m3 increase in air pollutant concentrations with different lag days in single-pollutant models. The cumulative effects of PM2.5 and PM10 were more significantly associated with percent increment in MI numbers than single day effects. And the highest association was identified for lag 0–1 (1.636%, 95%CI: 0.537–2.740%; 0.805%, 95%CI: 0.037–1.574%). Moreover, for lag 4, lag 0–5, lag 0–6, and lag 0–7, significantly negative associations were identified in 10-μg/m3 increase of SO2 and NO2. And no significant association was observed regarding O3 for any lag days. A 2-day moving average of the concentrations (lag 0–1 days) was used in the subsequent analysis.

Estimated changes with 95% confidence intervals in daily MI (myocardial infarction) percentage deviations (%) associated with an interquartile range increase in PM10, PM2.5, NO2, SO2, or O3 concentrations with different lag days in single-pollutant model
Figure 3 illustrates the concentration-response relationships of MI counts with air pollutants. The smoothing function curves for PM2.5 and PM10 were linear positive and flat at higher concentrations, whereas the curves for other pollutants were linear without statistic positive correlation.

The concentration-response curve of 2-day (lag 0–1) moving average air pollutants (df = 3) concentrations and MI counts in Changzhou, 2015–2016. Note: the X-axis is the 2-day (lag 0–1) moving air pollutants. Y-axis is the log relative risk (RR). The solid line represents the predicted log relative risk and the dotted lines represent the 95% CI
Table 4 shows the estimated changes in daily MI counts associated with a 10-μg/m3 increase in air pollutant concentrations modified by seasons (warm and cold period) and gender. The estimated effects of PM2.5 and PM10 were more pronounced in the warm season (2.296%, 95%CI: 0.671–3.929%; 1.135%, 95%CI: 0.004–2.269%) than that in the cold season. In addition, the association of PM2.5 and MI numbers in males (2.733%, 95%CI: 0.986–4.487%) was more pronounced than that in females and for PM10, though not statistically significant, the percentage increase was much higher in males than in females. No significant association was noted for other pollutants modified by seasons and gender.
The two-pollutant models were performed for lag 0–1 (Fig. 4). The effect estimate of all five pollutants did not change a lot in two-pollutant model. However, PM2.5 was dramatically robust when adjusted for PM10 and PM10 produced the lower effect estimates for MI after adjusting for PM2.5 than single-pollutant model.

Association between 10-μg/m3 increment in air pollutants (lag 0–1 day) and MI counts using single- and two-pollutant models in Changzhou, 2015–2016
Discussion
Our results described the short-term effects of air pollutant exposure on MI in Changzhou, China. To the best of our knowledge, in China, studies regarding the differences in the effects of the main air pollutants on MI counts are typically deficient. By identifying 5545 cases of MI in Changzhou, this study performed a comprehensive investigation on the association of exposure to main air pollutants with MI risk. In the present study, daily MI counts were found to tightly coincide with the elevation of PM2.5 and PM10 concentrations. Of note, the males had greater estimated MI risk than females and the effect of PM2.5 and PM10 in cold season has been attenuated than that in warm season. Moreover, SO2 and NO2 were found to be cardiovascular protective at seven cumulative days lag models (lag 0–7) and O3 levels showed no significant association with MI counts.
Exposure to PM2.5 and PM10 could induce the cardiovascular dysfunction of humans (McGuinn et al. 2017). For instance, numbers of MI admissions were statistically associated with higher PM2.5 levels in a case-crossover study performed in Taiwan (Tsai and Yang 2014). Moreover, a Shanghai study demonstrated that a 10-μg/m3 increment of PM2.5 or PM10 was associated with a 0.25 or 0.57% increase in the hospitalizations of ischemic heart disease, respectively (Xu et al. 2017). A meta-analysis of 31 studies conducted recently, which indicated that risk of PM2.5 (OR = 1.022) exposure was relatively greater than PM10 (OR = 1.005) (Luo et al. 2015). In the current study, a 10-μg/m3 increase in PM2.5 and PM10 concentrations increased the daily MI counts (1.636% for PM2.5 and 0.805% for PM10). In consistent with previous study (Zanobetti and Schwartz 2009), a cumulative effect of PM2.5 and PM10 (lag 0–1) on the short-term effect with MI was also identified. And it was plausible that PM2.5 was more deleterious to cardiovascular system than PM10. In addition, the risk estimates from single-pollutant models found that SO2 and NO2 could exert protective effect on risk of MI, which was in accordance with previous report (Wang et al. 2016). It was also reported that SO2 preconditioning could reduce MI injury in rats, and PI3K/Akt pathway was involved in the protective effects (Wang et al. 2011; Zhao et al. 2013). However, this should be interpreted with caution as limited study populations in this study. Further studies are required to explore the specific cardiovascular effects of SO2 and NO2.
The concentration-response relationship is important for assessment of the public health and determination of the adverse response pattern. In this study, the function curves for PM2.5/MI and PM10/MI were positive linear, with an estimated threshold of 100 μg/m3 for PM2.5 and 150 μg/m3 for PM10, respectively. The curves illustrated that the risks of the deterioration of MI could increase linearly corresponding to short-term increases in PM2.5 and PM10 levels, and specifically, a sharp increase in MI counts was associated with the increment in moderate PM2.5 (25 to 75 μg/m3) and PM10 (50 to 125 μg/m3) levels, suggesting that populations were more susceptible at that range.
Exploring the modifiers of the association between air pollution and MI is crucial to the primary prevention of MI (Dagres and Hindricks 2017). Males were found to have had greater estimated MI risk than females in this study, which was consistent with previous studies (Liu et al. 2017; Ye et al. 2001). A possible explanation for this observation may be that males are more likely to be exposed to air pollutants due to the higher rate of outdoor work and experience (Qiu et al. 2013). Furthermore, we found that the air pollutants (PM2.5 and PM10)-MI associations varied by season. Despite of the higher levels of air pollutants in cold season, PM2.5 and PM10 exhibited higher excess risk in the warm season. This was supported by Zanobetti but contrast to Kan and Chen’s work (Chen et al. 2015; Kan et al. 2008; Zanobetti and Schwartz 2006). The underlying reasons may be the different population exposure patterns, differences in population susceptibilities, and lifestyles (Qiu et al. 2013).
However, the association between air pollution and near-term risk of MI remains controversial. No associations were recognized between the risk for onset of MI and air pollutant exposure in a case-crossover design conducted in Stockholm (PM10, NO2, CO, or O3). Similarly, no significant associations between PM2.5, NO2, and CO and daily adults MI admissions were observed (Barnett et al. 2006; Berglind et al. 2010). However, a case-crossover study performed recently has demonstrated that per 5-μg/m3 increment in 3-day mean PM2.5 was associated with an increased risk of MI among elderly populations (Weichenthal et al. 2017). These differences might be attributed to the different levels of PM2.5 concentrations: Stockholm and Australia experience a lower level of particulate matters.
This study had several strengths. Firstly, our study consisted of a large sample size of 5545 cases for MI and there were no missing data on air quality and meteorological figures during the study period, allowing for sufficient statistical power to detect a significant association. Secondly, it was the first time to investigate the hazardous effects of air pollutants on MI in Changzhou, China. Thirdly, the air quality and meteorological data were obtained from reliable sources and the results were consisted with many other studies. Herein, our work still had several limitations. First, we relied on routine measurements from fixed-site monitoring stations without data like the distance from the monitoring stations to the individual’s residence and indoor exposure. Thus, the exact air pollutant exposure of individuals was unavailable. Second, individuals were recorded retrospectively from main hospitals in Changzhou, which may cause selection bias. Third, we obtained the data only from one city and the results were difficult to extrapolate.
In summary, we demonstrated that short-term exposure to PM2.5 and PM10 were associated with daily MI counts in China. We believe that these findings have implications related to local environmental health risk assessment and early warning. And further studies should be conducted to validate our findings.
References
Argacha JF, Collart P, Wauters A, Kayaert P, Lochy S, Schoors D, Sonck J, de Vos T, Forton M, Brasseur O, Beauloye C, Gevaert S, Evrard P, Coppieters Y, Sinnaeve P, Claeys MJ (2016) Air pollution and ST-elevation myocardial infarction: a case-crossover study of the Belgian STEMI registry 2009-2013. Int J Cardiol 223:300–305
Barnett AG, Williams GM, Schwartz J, Best TL, Neller AH, Petroeschevsky AL, Simpson RW (2006) The effects of air pollution on hospitalizations for cardiovascular disease in elderly people in Australian and New Zealand cities. Environ Health Persp 114:1018–1023
Berglind N, Ljungman P, Moller J, Hallqvist J, Nyberg F, Rosenqvist M, Pershagen G, Bellander T (2010) Air pollution exposure-a trigger for myocardial infarction? Int J Environ Res Public Health 7:1486–1499
Chen R, Huang W, Wong CM, Wang Z, Thach TQ, Chen B, Kan H, Group CC (2012) Short-term exposure to sulfur dioxide and daily mortality in 17 Chinese cities: the China air pollution and health effects study (CAPES). Environ Res 118:101–106
Chen YC, Weng YH, Chiu YW, Yang CY (2015) Short-term effects of coarse particulate matter on hospital admissions for cardiovascular diseases: a case-crossover study in a Tropical City. J Toxicol Environ Health A 78:1241–1253
Dagres N, Hindricks G (2017) Devices for management of sudden cardiac death: successes, challenges and perspectives. Int J Cardiol 237:34–37
Dockery DW, Luttmann-Gibson H, Rich DQ, Link MS, Mittleman MA, Gold DR, Koutrakis P, Schwartz JD, Verrier RL (2005) Association of air pollution with increased incidence of ventricular tachyarrhythmias recorded by implanted cardioverter defibrillators. Environ Health Persp 113:670–674
Gurung A, Bell ML (2013) The state of scientific evidence on air pollution and human health in Nepal. Environ Res 124:54–64
Ibanez B, Heusch G, Ovize M, Van de Werf F (2015) Evolving therapies for myocardial ischemia/reperfusion injury. J Am Coll Cardiol 65:1455–1471
Kan HD, London SJ, Chen GH, Zhang YH, Song GX, Zhao NQ, Jiang LL, Chen BH (2008) Season, sex, age, and education as modifiers of the effects of outdoor air pollution on daily mortality in shanghai, China: the public health and air pollution in Asia (PAPA) study. Environ Health Persp 116:1183–1188
Kan HD, Chen BH, Hong CJ (2009) Health impact of outdoor air pollution in China: current knowledge and future research needs. Environ Health Persp 117:A187–A187
Kerstens SM, de Mes TZ, Lue B (2009) Designing sustainable sanitation in urban planning proposed for Changzhou, China. Water Sci Technol 60:3165–3172
Krumholz HM, Normand SLT (2008) Public reporting of 30-day mortality for patients hospitalized with acute myocardial infarction and heart failure. Circulation 118:1394–1397
Li J, Li X, Wang Q, Hu S, Wang YF, Masoudi FA, Spertus JA, Krumholz HM, Jiang LX, Grp CPC (2015) ST-segment elevation myocardial infarction in China from 2001 to 2011 (the China PEACE-retrospective acute myocardial infarction study): a retrospective analysis of hospital data (retracted article. See vol. 385, pg. 402, 2015). Lancet 385:441–451
Li L, Chen CH, Huang C, Huang HY, Li ZP, Fu JS, Jang CJ, Streets DG (2008) Regional air pollution characteristics simulation of O3 and PM10 over Yangtze River Delta region. Huan jing ke xue 29:237–245
Lin HL, Liu T, Xiao JP, Zeng WL, Guo LC, Li X, Xu YJ, Zhang YH, Chang JJ, Vaughn MG, Qian ZM, Ma WJ (2017) Hourly peak PM2.5 concentration associated with increased cardiovascular mortality in Guangzhou, China. J Expo Sci Environ Epidemiol 27:333–338
Liu H, Tian Y, Xiang X, Sun K, Juan J, Song J, Cao Y, Xu B, Hu Y (2017) Air pollution and hospitalization for acute myocardial infarction in China. Am J Cardiol 120:753–758
Luo CM, Zhu XX, Yao CJ, Hou LJ, Zhang J, Cao JY, Wang AL (2015) Short-term exposure to particulate air pollution and risk of myocardial infarction: a systematic review and meta-analysis. Environ Sci Pollut Res 22:14651–14662
McGuinn LA, Ward-Caviness C, Neas LM, Schneider A, Di Q, Chudnovsky A, Schwartz J, Koutrakis P, Russell AG, Garcia V, Kraus WE, Hauser ER, Cascio W, Diaz-Sanchez D, Devlin RB (2017) Fine particulate matter and cardiovascular disease: comparison of assessment methods for long-term exposure. Environ Res 159:16–23
Mehta PK, Wei J, Wenger NK (2015) Ischemic heart disease in women: a focus on risk factors. Trends Cardiovas Med 25:140–151
Nuvolone D, Balzi D, Chini M, Scala D, Giovannini F, Barchielli A (2011) Short-term association between ambient air pollution and risk of hospitalization for acute myocardial infarction: results of the cardiovascular risk and air pollution in Tuscany (RISCAT) study. Am J Epidemiol 174:63–71
Petaja T, Jarvi L, Kerminen VM, Ding AJ, Sun JN, Nie W, Kujansuu J, Virkkula A, Yang XQ, Fu CB, Zilitinkevich S, Kulmala M (2016) Enhanced air pollution via aerosol-boundary layer feedback in China. Sci Rep 12:18998
Qiu H, Yu ITS, Wang XR, Tian LW, Tse LA, Wong TW (2013) Cool and dry weather enhances the effects of air pollution on emergency IHD hospital admissions. Int J Cardiol 168:500–505
Rohde RA, Muller RA (2015) Air pollution in China: mapping of concentrations and sources. PLoS One 10:e0135749
Roswall N, Raaschou-Nielsen O, Ketzel M, Gammelmark A, Overvad K, Olsen A, Sorensen M (2017) Long-term residential road traffic noise and NO2 exposure in relation to risk of incident myocardial infarction - a Danish cohort study. Environ Res 156:80–86
Sohn J, You SC, Cho J, Choi YJ, Joung B, Kim C (2016) Susceptibility to ambient particulate matter on emergency care utilization for ischemic heart disease in Seoul, Korea. Environ Sci Pollut Res 23:19432–19439
Stockfelt L, Andersson EM, Molnar P, Gidhagen L, Segersson D, Rosengren A, Barregard L, Sallsten G (2017) Long-term effects of total and source-specific particulate air pollution on incident cardiovascular disease in Gothenburg, Sweden. Environ Res 158:61–71
Talbott EO, Rager JR, Benson S, Brink LA, Bilonick RA, Wu C (2014) A case-crossover analysis of the impact of PM(2.5) on cardiovascular disease hospitalizations for selected CDC tracking states. Environ Res 134:455–465
Thiele H, Ohman EM, Desch S, Eitel I, de Waha S (2015) Management of cardiogenic shock. Eur Heart J 36:1223–1230
Tsai SS, Yang CY (2014) Fine particulate air pollution and hospital admissions for pneumonia in a Subtropical City: Taipei, Taiwan. J Toxicol Environ Health A 77:192–201
Wang XB, Huang XM, Ochs T, Li XY, Jin HF, Tang CS, Du JB (2011) Effect of sulfur dioxide preconditioning on rat myocardial ischemia/reperfusion injury by inducing endoplasmic reticulum stress. Basic Res Cardiol 106:865–878
Wang XD, Zhang XM, Zhuang SW, Luo Y, Kang S, Liu YL (2016) Short-term effects of air pollution on acute myocardial infarctions in shanghai, China, 2013-2014. J Geriatr Cardiol 13:132–137
Weber SA, Insaf TZ, Hall ES, Talbot TO, Huff AK (2016) Assessing the impact of fine particulate matter (PM2.5) on respiratory cardiovascular chronic diseases in the new York City metropolitan area using hierarchical Bayesian model estimates. Environ Res 151:399–409
Weichenthal S, Kulka R, Lavigne E, van Rijswijk D, Brauer M, Villeneuve PJ, Stieb D, Joseph L, Burnett RT (2017) Biomass burning as a source of ambient fine particulate air pollution and acute myocardial infarction. Epidemiology 28:329–337
Wellenius GA, Burger MR, Coull BA, Schwartz J, Suh HH, Koutrakis P, Schlaug G, Gold DR, Mittleman MA (2012) Ambient air pollution and the risk of acute ischemic stroke. Arch Intern Med 172:229–234
Xie W, Li G, Zhao D, Xie X, Wei Z, Wang W, Wang M, Li G, Liu W, Sun J, Jia Z, Zhang Q, Liu J (2015) Relationship between fine particulate air pollution and ischaemic heart disease morbidity and mortality. Heart 101:257–263
Xu AY, Mu Z, Jiang B, Wang W, Yu H, Zhang LJ, Li J (2017) Acute effects of particulate air pollution on ischemic heart disease hospitalizations in shanghai, China. Int J Environ Res Public Health 14:e168
Yang GH, Wang Y, Zeng YX, Gao GF, Liang XF, Zhou MG, Wan X, Yu SC, Jiang YH, Naghavi M, Vos T, Wang HD, Lopez AD, Murray CJL (2013) Rapid health transition in China, 1990-2010: findings from the global burden of disease study 2010. Lancet 381:1987–2015
Ye F, Piver WT, Ando M, Portier CJ (2001) Effects of temperature and air pollutants on cardiovascular and respiratory diseases for males and females older than 65 years of age in Tokyo, July and august 1980-1995. Environ Health Persp 109:355–359
Zanobetti A, Schwartz J (2006) Air pollution and emergency admissions in Boston, MA. J. Epidemiol Commun Health 60:890–895
Zanobetti A, Schwartz J (2009) The effect of fine and coarse particulate air pollution on mortality: a national analysis. Environ Health Perspect 117:898–903
Zhang Q, Qi WP, Yao W, Wang M, Chen YY, Zhou YJ (2016) Ambient particulate matter (PM2.5/PM10) exposure and emergency department visits for acute myocardial infarction in Chaoyang District, Beijing, China during 2014: a case-crossover study. J Epidemiol 26:538–545
Zhao MM, Yang JY, Wang XB, Tang CS, Du JB, Jin HF (2013) The PI3K/Akt pathway mediates the protection of SO(2) preconditioning against myocardial ischemia/reperfusion injury in rats. Acta Pharmacol Sin 34:501–506
Zhou MG, Wang H, Zhu J, Chen W, Wang L, Liu S, Li Y, Wang L, Liu Y, Yin P, Liu J, Yu S, Tan F, Barber RM, Coates MM, Dicker D, Fraser M, González-Medina D, Hamavid H, Hao Y, Hu G, Jiang G, Kan H, Lopez AD, Phillips MR, She J, Vos T, Wan X, Xu G, Yan LL, Yu C, Zhao Y, Zheng Y, Zou X, Naghavi M, Wang Y, Murray CJL, Yang G, Liang X (2016) Cause-specific mortality for 240 causes in China during 1990-2013: a systematic subnational analysis for the global burden of disease study 2013. Lancet 387:251–272
Acknowledgements
We thank the Changzhou Municipal Environmental Monitoring Center for providing the air pollution data and the Changzhou Municipal Meteorological Monitoring Center for providing the weather data.
Funding
This study was supported by the Natural Science Foundation of China (81502801), a project funded by the Priority Academic Program Development of Jiangsu Higher Education Institutions (2014), a collegiate Natural Science Foundations of Jiangsu province (16KJB330005), the science and technology support program funded by Changzhou Municipal Science and Technology Bureau (CE20145046), and the Science and Technique Foundation for Youths by Health and Family Planning Commission of Changzhou.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
The present study was approved by the Institutional Review Board of Changzhou Center for Disease Control and Prevention, and all procedures were in accordance with prevailing ethical principles.
Conflict of interest
The authors declare that they have no conflict of interest.
Additional information
Responsible editor: Philippe Garrigues
Rights and permissions
About this article

Cite this article
Yu, Y., Yao, S., Dong, H. et al. Short-term effects of ambient air pollutants and myocardial infarction in Changzhou, China. Environ Sci Pollut Res 25, 22285–22293 (2018). https://doi.org/10.1007/s11356-018-2250-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11356-018-2250-5