
Abstract
Purpose
The aim of this investigation was to evaluate the effects of local cryotherapy on the recovery from symptoms of exercise-induced muscle damage (EIMD) on biceps brachii.
Methods
Nineteen untrained women performed an eccentric protocol of damage induction (2 sets of 10 repetitions) in both arms after the baseline data collection. The cryotherapy was applied for 20 min, twice per day, for 4 days following the eccentric exercise. Randomly, one of the subject’s arms was assigned as intervention, and received cryotherapy, the opposite arm served as control. As muscle damage indirect markers, we collected muscle thickness, and echo intensity, delayed onset muscle soreness, and peak torque at baseline (PRE), and at 24, 48, 72, and 96 h.
Results
Muscle thickness at PRE was significantly lower than all time points in both experimental and control arms. Echo intensity at PRE was significantly lower than 24, 48, and 72 h in the experimental arm, and significantly lower than all time points in the control arm. Muscle soreness assessed by flexion–extension, and by self-palpation of both the experimental and the control arms significantly increased compared to the PRE value at 24, 48, and 72 h. Peak Torque of both experimental and control arm was significantly lower than all time points after EIMD. None of the muscle damage indirect markers showed any significant difference between arms at any moment (p > 0.05).
Conclusion
The results demonstrated that the protocol of cryotherapy utilized in the present study was not effective in enhancing the recovery from EIMD in untrained women.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Cryotherapy is commonly utilized in the musculoskeletal system as a therapeutic resource [1, 2]. Previous studies have shown that cryotherapy provides an analgesic effect and helps to decrease muscle spasms [3, 4]. Furthermore, cold therapy promotes structural and functional restoration by reducing blood flow, tissue temperature, and metabolism, limiting edema formation [5, 6]. More recently, cryotherapy has been extensively utilized to attenuate symptoms of exercise-induced muscle damage (EIMD) such as delayed onset muscle soreness (DOMS) and decreased strength [7,8,9]. However, it remains unclear whether cryotherapy is effective in easing such symptoms.
The most remarkable indirect marker of EIMD is DOMS that is usually measured with Visual Analog Scale (VAS) [10]. Even though it is an important assessment tool, its results may be very subjective. To obtain more tangible information about EIMD, ultrasonography (US) has been a common approach in this field [10,11,12]. This non-invasive and easily accessible tool enables the extraction of accurate information about edema formation (muscle thickness-MT) and inflammatory cell infiltration (echo intensity-EI), which may contribute to better understand the influence of cryotherapy on symptoms of EIMD.
The literature has been trying to elucidate the role of cryotherapy on symptoms of EIMD [13, 14]. Pointon et al. [13] examined the effects of local cold therapy on recovery from the effects of EIMD on the knee extensor muscles. Results demonstrated that cryotherapy was not effective in reducing indices of EIMD. Another previous study [14] compared the effects of local cryotherapy and a topical menthol-based analgesic on the recovery from DOMS and decreased strength of elbow flexors. The authors observed that menthol-based topical analgesic showed a tendency to be more effective than local cryotherapy in easing symptoms of EIMD.
Cryotherapy was ineffective in both above-mentioned studies. However, both of them presented limitations. Pointon et al. [13] used a small sample (10 athletes). Additionally, another factor that may have influenced the results is that the authors evaluated knee extensors, which is a muscle group more resistant to EIMD when compared to both knee flexors and elbow flexors [15]. Johar et al. [14] recruited male and female participants that respond differently to EIMD [16, 17], and performed a single session of ice at 48 h after the muscle damage protocol, which does not seem to be sufficient to accelerate the recovery [18,19,20]. Oakley et al. [20] have demonstrated that a higher rate of ice application contributes to decrease muscle soreness following eccentric exercise. A single application of ice may not be sufficient to decrease the conductivity of pain receptors [21].
That said, it seems reasonable to assume that gender [16, 17], physical conditioning level [22], and time of application of ice [20] can affect muscular response to EIMD. Therefore, it would be valuable to analyze the influence of a proper rate of ice application in a more homogeneous sample to better understand the effects of cryotherapy on symptoms of EIMD. Moreover, the utilization of an assessment tool as US would contribute to clarify the real influence of cryotherapy on EIMD.
Hence, the aim of the current study was to evaluate the effects of local cryotherapy utilizing a proper frequency of application on echo intensity, muscle thickness, and other indirect markers of EIMD (DOMS, and peak torque) on young women’s biceps brachii after a bout of eccentric exercise.
Methods
Study design
The study required the participants to visit the laboratory five times. On day one, the participants performed the eccentric protocol of damage induction (EPDI) on an isokinetic dynamometer. The EPDI was composed by 2 sets of 10 maximal eccentric contractions of elbow flexors at the angular velocity of 30°/s. Before (PRE), 24, 48, 72 and 96 h (h) after the protocol, measures of muscle thickness (MT), echo intensity (EI), DOMS, and peak torque (PT) were taken from the dominant and non-dominant elbow flexors. Twenty minutes of local cryotherapy was applied on the intervention arm, twice per day for four days following the EPDI, with an interval of 6–7 h between the sessions. The first session was always carried out immediately after evaluations.
Participants
Nineteen young women (21.6 ± 2.0 years old; 60.3 ± 10.9 kg; 162.1 ± 5.8 cm) who had not performed systematic strength training or any other type of activity involving the upper limbs in the last year were recruited for the study. An untrained population was chosen because of their greater tendency to develop symptoms of EIMD [22]. Also, we opted to recruit participants of only one sex to avoid any differences in responses to EIMD related to gender that might exist. The participants were free from any musculoskeletal disorders, and they were not taking any medication or dietary supplements. Both arms underwent the eccentric protocol of damage induction. The arm that would receive the treatment was chosen randomly. The randomization was carried out using an opaque envelope containing 20 cards, 10 cards for dominant arm, and 10 cards for non-dominant arm. The participants were instructed to pick a card from the envelope before the first test. The card would establish which of the subjects’ arms would receive the therapy. Ten subjects applied the cryotherapy on the non-dominant arm, and nine subjects applied it on the dominant arm. We decided to randomize the arms once the dominant arm might respond differently due to its higher participation in daily activities. Before participation, each volunteer read and signed a detailed informed consent. The informed consent was approved by the University Institutional Review Board, and described the study and its potential risks and benefits. The participants were oriented not to perform any vigorous physical activities or unaccustomed exercises during the experimental period.
Eccentric protocol of damage induction
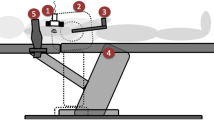
The tests were carried out on a Scott bench (preacher curl, Sculptor, Porto Alegre, Brazil), using isokinetic contractions on a Cybex Norm isokinetic dynamometer (Ronkonkoma, NY, USA), calibrated according to the manufacturer’s instructions. Before the maximal eccentric protocol, the subject performed 15 concentric submaximal (minimum force necessary to move the elbow adapter) repetitions of elbow flexion/extension as familiarization and warm-up. The eccentric protocol consisted of 2 sets of 10 maximal eccentric contractions at 0.52 rad/s (30°/s) of velocity of unilateral elbow flexion, with a 30-s rest interval between sets, and it was performed in both arms. The range of motion of the exercise was 0°–100° (0° = full elbow extension). Throughout the tests, participants were given verbal encouragement by the researcher, who administered all tests.
Cryotherapy
Cryotherapy sessions were conducted twice a day, only in the experimental arm. An ice bag with 500 g of ice was placed over the biceps brachii area (8 cm above the elbow joint) and tied with a viscoelastic bandage. The sessions lasted 20 min each. This amount of sessions was chosen because it was a number that would be doable for the participants without significantly interfere with their daily routine. The first cryotherapy session occurred immediately after the evaluations on all days, and the second session was unsupervised and occurred 6–7 h after the first application. We called the participants to remind them about the ice application, and they were strongly advised to let the researchers know if there were any problems during the application, which would cause the exclusion of the subject from the study. The skin temperature was measured using a laser thermometer (Raytek, Minitemp) 8 cm above the elbow joint. The skin temperature of the participants’ arm decreased from 28 to 18 °C on average during the local cryotherapy application.
Ultrasonography images
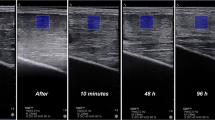
The MT and EI were assessed by US according to the methodology used in previous studies in our laboratory [11, 12]. The images were obtained by B-mode ultrasonography (Nemio XG ultrasound, Toshiba, Japan) 8 cm above the elbow joint [10] using a high-resolution linear array probe (38 mm) with 7.5 MHz. During image acquisition, the participants remained supine with the tested arm extended and relaxed. To obtain the US images, the examiner placed the probe perpendicular to the evaluated muscle on a marked site on the biceps brachii 8 cm above the elbow joint. A water-based gel was used to promote acoustic contact without causing excessive probe pressure on the skin during imaging acquisition. The coefficient of variation was 4.2%, and the baseline test–retest ICC was 0.94. The same image used to assess MT was used to measure the EI. The EI of the biceps brachii muscles was determined using a 1-cm2 region of interest (ROI = 1 × 1 = 1-cm2), based on a grayscale histogram (0: black, 255: white). The EI was quantified using the Image-J software (version 1.37, National Institutes of Health, Bethesda, MD. USA). A trained investigator with experience and publications in the field [12, 23] performed all analyses of MT and EI, and he was blind to the arm that was receiving cryotherapy.
Muscle soreness
The DOMS was evaluated using a well-established methodology [10]. The participants were asked to indicate their level of muscle soreness on a 100-mm visual analog scale (0 mm = “‘no pain”’ and 100 mm = “extreme pain”), after a full range of elbow flexion and extension movement. We also requested the participants to assess their muscle soreness by self-palpation of the biceps brachii.
Peak torque
The isometric PT was tested on an isokinetic dynamometer (Cybex NORM dynamometer, Ronkonkoma, NY, USA), which was calibrated before the tests according to the manufacturer’s instructions. The participants were seated with their elbow on a Scott bench (preacher curl, Sculptor, Porto Alegre, Brazil) and aligned with the axis of the adapted dynamometer lever arm. The test consisted of three 5-s maximal isometric voluntary contractions at 60° of elbow flexion (0° = full elbow extension), with 3 min of recovery between each effort. The elbow adapter length was adjusted for each subject, and the participants were instructed to keep their non-tested arm on the Scott bench. The greatest PT among three isometric voluntary contractions, provided by Humac 2009 software version 12.17.0 (Humac, Stoughton, MA, USA), was used for analyses.
Statistical analysis
All values are reported as mean ± SD. The Shapiro–Wilk test was used to test the normality of the outcome distribution. The ANOVA test using 2 × 5 [arm (experimental and control) × time (pre, 24, 48, 72, and 96 h)] was used for comparisons. When ANOVA showed a significant main effect, the post hoc Tukey test was used to detect differences between bouts. The level of significance was set at 0.05. All analyses were performed with the software SPSS 13.0 (IBM, Somers, NY, USA).
Results
There were no significant differences between experimental and control arms for none of EIMD indirect markers analyzed (Table 1).
Ultrasonography images
The MT was significantly higher than the PRE value (p ≤ 0.05) in both the experimental arm (24 h = 3.6%; 48 h = 1.9%; 72 h = 1.3% 96 h = 1.6%) and the control arm (24 h = 2.37%; 48 h = 4.74%; 72 h = 6.10%; and 96 h = 3.72%) at all time points (Fig. 1).

Muscle thickness of the biceps brachii across time for both arms; *significant difference compared to PRE (p < 0.05)
The EI was significantly higher than the PRE value (p ≤ 0.05) at 24, 48, and 72 h in the experimental arm (24 h = 5.65; 48 h = 6.11%; 72 h = 9.96%), and at all time points in the control arm (24 h = 13.4%; 48 h = 14.2%; 72 h = 13.9%; 96 h = 16.7%) (Fig. 2).

Echo intensity of the biceps brachii across time for both arms; *significant difference compared to PRE (p < 0.05)
Muscle soreness
The DOMS assessed by flexion–extension, and by self-palpation of both the experimental and the control arms significantly increased (p ≤ 0.05) compared to the PRE value at 24, 48, and 72 h (Fig. 3a, b).

Muscle soreness across time for both arms: a flexion–extension (f-e) and b palpation (palp). *Significant difference compared to PRE (p < 0.05)
Torque peak
The PT of the both experimental and control arms at all time points after the EPDI was significantly lower (p ≤ 0.05) compared to the PRE value (Fig. 4).

Peak torque across time for both arms. *Significant difference compared to PRE (p < 0.05)
Discussion
The present study evaluated the effects of local cryotherapy using a proper frequency of application (twice per day) on the recovery from symptoms of EIMD on biceps brachii after an acute bout of eccentric exercise. The exercise protocol carried out was sufficient to provoke significant post-exercise alterations in all indirect markers of EIMD analyzed: MT, EI, DOMS, and muscle strength. The main finding of this investigation was that 20 min of local cryotherapy applied twice per day for 4 days is not effective in accelerating muscle recovery after EIMD.
Ultrasonography images have been used in recent years as reproductive indirect markers of muscle damage [12, 23, 24]. Regarding muscle damage over time, the present study is in line with previous studies [15, 25] that have found significant changes in both MT and EI from the PRE moment until 96 h after EPDI. An increase in MT and EI in the days after eccentric exercise has been demonstrated to be highly associated with signs of inflammation response such as edema formation [26]. Inflammation is essential for the adaptation of skeletal muscle after exercise because it is during the inflammation that the damaged tissue is eliminated and regeneration takes place [27]. However, this process might take a considerable amount of time to recover, which will affect muscular performance. Alternatives to accelerate this process have been investigated.
Cryotherapy is known for helping to control the symptoms related to the inflammation process after muscle trauma (injury) such as edema and pain [28]. Since muscle regeneration responses to both muscle injury and muscle damage are quite similar [28], cryotherapy has been used in an attempt to accelerate the inflammatory process related to muscle damage after strenuous exercise. Nevertheless, a recent study [29] showed that local cryotherapy delayed the release of inflammatory cytokines (TNF-α and IL-6) after EIMD, which may have delayed the recovery process. This information suggests that local cryotherapy may not be the most appropriate alternative to accelerate the natural inflammation response to muscle damage.
The muscle soreness peak occurred 48 h after EPDI which is in line with other studies [10, 12]. Regarding DOMS, there was no significant difference over time between the experimental and control arm in none of the muscle soreness measures. Similar results were found in the study by Johar et al. [14] that concluded that local cryotherapy was less effective in relieving DOMS after EIMD in the elbow flexors compared to a topical menthol-base analgesic. Likewise, Pointon et al. [13] evaluated the effects of a single session of local cryotherapy applied with ice cuffs for the recovery from DOMS in the knee extensors. The results showed improvement on muscle pain (assessed by algometry). However, according to the authors, such response was most likely due a perceptual or placebo effect, since all other indirect markers analyzed, including muscle soreness, showed no significant differences between intervention and control groups, supporting the results of the present study.
The diminished ability to produce strength after eccentric contractions is one of the most used and most reproducible indirect markers of muscle damage in humans [30]. In the current study, reduced muscle strength was identified over time in all periods following the EPDI in both arms. Furthermore, both strength loss and strength recovery were very similar during the study period in both arms, evidencing no effect of local cryotherapy. The present study has not shown positive results of cryotherapy on the recovery of strength loss in the days following EIMD. However, there is some evidence [7, 9] that cold therapy may help to diminish the deleterious effects of EIMD on muscle strength. The discrepancy in the findings may be related to differences in muscle damage protocols performed (e.g., multi-joint vs. single-joint; upper limb vs. lower limb; the number of repetitions), which influences muscle response to exercise [13, 31].
Limitations
A point that should be highlighted as a limitation of the current study refers to the home ice application. Even though the participants were advised to inform the researchers about any problems involving the ice application, we did not have complete control over it. Another factor that must be included as a limitation is the lack of control of the subjects’ menstrual cycle. The individuals’ estrogen concentration may have varied among the participants. Previous findings suggest that estrogen has a protective function in the muscle cell membrane after EIMD [32]. Therefore, different stages within the menstrual cycle may have influenced the magnitude of damage generated by the EPDI.
Conclusion
In conclusion, the present results showed that the application of local cryotherapy performed 20 min twice a day for 4 days was not effective in reducing symptoms of EIMD. Thus far, local cryotherapy does not seem to be the most appropriate technique to be performed in order to accelerate the recovery from EIMD. Further investigations could invest in more frequent applications in an attempt to establish whether cold therapy is worth using to ease symptoms of EIMD.
References
Bleakley CM, Bieuzen F, Davison GW, Costello JT (2014) Whole-body cryotherapy: empirical evidence and theoretical perspectives. Open Access J Sport Med 5:25–36. doi:10.2147/OAJSM.S41655
Martin SS, Spindler KP, Tarter JW et al (2001) Cryotherapy: an effective modality for decreasing intraarticular temperature after knee arthroscopy. Am J Sports Med 29:288–291
Swenson C, Sward L, Karlsson J (1996) Cryotherapy in sports medicine. Scand J Med Sci Sports 6:193–200. doi:10.1111/j.1600-0838.1996.tb00090.x
Wilcock IM, Cronin JB, Hing WA (2006) Physiological response to water immersion: a method for sport recovery? Sport Med 36:747–765. doi:10.2165/00007256-200636090-00003
Karunakara RG, Lephart SM, Pincivero DM (1999) Changes in forearm blood flow during single and intermittent cold application. J Orthop Sport Phys Ther 29:177–180. doi:10.2519/jospt.1999.29.3.177
Glenn RE, Spindler KP, Warren TA et al (2004) Cryotherapy decreases intraarticular temperature after ACL reconstruction. Clin Orthop Relat Res 2:268–272. doi:10.1097/01.blo.0000126302.41711.eb
Ascensão A, Leite M, Rebelo AN et al (2011) Effects of cold water immersion on the recovery of physical performance and muscle damage following a one-off soccer match. J Sports Sci 29:217–225. doi:10.1080/02640414.2010.526132
Eston R, Peters D (1999) Effects of cold water immersion on the symptoms of exercise-induced muscle damage. J Sports Sci 17:231–238. doi:10.1080/026404199366136
Minett GM, Duffield R, Billaut F et al (2014) Cold-water immersion decreases cerebral oxygenation but improves recovery after intermittent-sprint exercise in the heat. Scand J Med Sci Sport 24:656–666. doi:10.1111/sms.12060
Chen TC, Chen HL, Lin MJ et al (2010) Potent protective effect conferred by four bouts of low-intensity eccentric exercise. Med Sci Sports Exerc 42:1004–1012. doi:10.1249/MSS.0b013e3181c0a818
Flores DF, Gentil P, Brown LE et al (2011) Dissociated time course of recovery between genders after resistance exercise. J Strength Cond Res 25:3039–3044. doi:10.1519/JSC.0b013e318212dea4
Radaelli R, Bottaro M, Wilhelm EN et al (2012) Time course of strength and echo intensity recovery after resistance exercise in women. J Strength Cond Res 26:2577–2584. doi:10.1519/JSC.0b013e31823dae96
Pointon M, Duffield R, Cannon J, Marino FE (2011) Cold application for neuromuscular recovery following intense lower-body exercise. Eur J Appl Physiol 111:2977–2986. doi:10.1007/s00421-011-1924-1
Johar P, Grover V, Topp R, Behm DG (2012) A comparison of topical menthol to ice on pain, evoked tetanic and voluntary force during delayed onset muscle soreness. Int J Sports Phys Ther 7:314–322
Chen TC, Lin KY, Chen HL et al (2011) Comparison in eccentric exercise-induced muscle damage among four limb muscles. Eur J Appl Physiol 111:211–223. doi:10.1007/s00421-010-1648-7
MacIntyre DL, Reid WD, Lyster DM, McKenzie DC (2000) Different effects of strenuous eccentric exercise on the accumulation of neutrophils in muscle in women and men. Eur J Appl Physiol 81:47–53. doi:10.1007/PL00013796
Stupka N, Lowther S, Chorneyko K et al (2000) Gender differences in muscle inflammation after eccentric exercise. J Appl Physiol 89:2325–2332
Barnett A (2006) Using recovery modalities between training sessions in elite athletes: does it help? Sport Med 36:781–796. doi:10.2165/00007256-200636090-00005
Howatson G, Gaze D, Van Someren KA (2005) The efficacy of ice massage in the treatment of exercise-induced muscle damage. Scand J Med Sci Sport 15:416–422. doi:10.1111/j.1600-0838.2005.00437.x
Oakley ET, Pardeiro RB, Powell JW, Millar AL (2013) The effects of multiple daily applications of ice to the hamstrings on biochemical measures, signs, and symptoms associated with exercise-induced muscle damage. J Strength Cond Res 27:2743–2751. doi:10.1519/JSC.0b013e31828830df
Kowal MA (1983) Review of physiological effects of cryotherapy. J Orthop Sports Phys Ther 5:66–73. doi:10.2519/jospt.1983.5.2.66
Newton MJ, Morgan GT, Chapman DW, Nosaka KK (2008) Comparison of responses to strenuous eccentric exercise of the elbow flexors between resistance-trained and untrained men. J Strength Cond Res 22:597–607. doi:10.1519/JSC.0b013e3181660003
Radaelli R, Bottaro M, Wagner DR et al (2014) Men and women experience similar muscle damage after traditional resistance training protocol. Isokinet Exerc Sci 22:47–54. doi:10.3233/IES-130519
Pinto RS, Gomes N, Radaelli R et al (2012) Effect of range of motion on muscle strength and thickness. J Strength Cond Res 26:2140–2145. doi:10.1519/JSC.0b013e31823a3b15
Nosaka K, Newton M (2002) Difference in the magnitude of muscle damage between maximal and submaximal eccentric loading. J Strength Cond Res 16:202–208. doi:10.1519/1533-4287(2002)016<0202:DITMOM>2.0.CO;2
Fujikake T, Hart R, Nosaka K (2009) Changes in B-mode ultrasound echo intensity following injection of bupivacaine hydrochloride to rat hind limb muscles in relation to histologic changes. Ultrasound Med Biol 35:687–696. doi:10.1016/j.ultrasmedbio.2008.10.008
Tidball JG, Villalta SA (2010) Regulatory interactions between muscle and the immune system during muscle regeneration. Am J Physiol Regul Integr Comp Physiol 298:R1173–R1187. doi:10.1152/ajpregu.00735.2009
Urso ML (2013) Anti-inflammatory interventions and skeletal muscle injury: benefit or detriment? J Appl Physiol 115:920–928. doi:10.1152/japplphysiol.00036.2013
Tseng C-Y, Lee J-P, Tsai Y-S et al (2013) Topical cooling (icing) delays recovery from eccentric exercise-induced muscle damage. J Strength Cond Res 27:1354–1361. doi:10.1519/JSC.0b013e318267a22c
Cheung K, Hume PA, Maxwell L (2003) Delayed onset muscle soreness: treatment strategies and performance factors. Sport Med 33:145–164. doi:10.2165/00007256-200333020-00005
Saka T, Akova B, Yazici Z et al (2009) Difference in the magnitude of muscle damage between elbow flexors and Knee extensors eccentric exercises. J Sport Sci Med 8:107–115
Enns DL, Tiidus PM (2010) The influence of estrogen on skeletal muscle: sex matters. Sport Med 40:41–58. doi:10.2165/11319760-000000000-00000
Acknowledgements
The authors thank the National Counsel of Technological and Scientific Development for the scientific initiation scholarship.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
All procedures of the present study were approved by the Federal University of Rio Grande do Sul Review Board, and they were performed in accordance with the ethical standards of the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Rights and permissions
About this article

Cite this article
Lima, C.S., Medeiros, D.M., Prado, L.R. et al. Local cryotherapy is ineffective in accelerating recovery from exercise-induced muscle damage on biceps brachii. Sport Sci Health 13, 287–293 (2017). https://doi.org/10.1007/s11332-017-0355-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11332-017-0355-8