
Abstract
Purpose
Recent advancements in elastography techniques, specifically supersonic shearwave elastography (SWE), have enabled non-invasive assessment of muscle stiffness. However, there is limited research on the immediate and short-term effects of eccentric exercise-induced muscle damage (EIMD) in well-trained individuals. This study aimed to follow up on the effects of eccentric training on the biceps brachialis stiffness by supersonic shearwave imaging (SSI) as well as the soreness and elbow flexion maximal voluntary isometric contraction (MVIC), immediately post-intervention, at 10 min, 48 h, and 96 h in well-trained men.
Methods
Thirteen well-trained males participated in the study. Baseline measurements of elastography images, MVIC of the elbow flexors, and muscle soreness were obtained. The participants performed an eccentric exercise protocol (4 sets X 10 repetitions) on the dynamometer isokinetic and elastography measurements were repeated immediately post-exercise, at 10 min, 48 h, and 96 h.
Results
Significant reductions in stiffness (measured by shear modulus (µ)) were observed immediately and at 10 min post-exercise. MVIC exhibited significant reductions immediately after, 10 min, and 48 h compared to baseline measurements. Muscle soreness peaked at 48 h, persisting until 96 h.
Conclusions
The BB stiffness and MVIC reduction immediately post-eccentric exercise in well-trained men, suggest the potential involvement of mechanical stress and sarcomere rupture. Trained individuals may exhibit a distinct response to EIMD compared to untrained individuals, highlighting the applicability of elastography in monitoring acute biomechanical changes following high-intensity exercise.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Muscle damage from eccentric exercise, common in activities like weightlifting, running, and downhill motion [1,2,3], involves lengthening muscle fibers under high force, causing mechanical stress and cell disruption [4,5,6]. The exercise-induced muscle damage (EIMD) has been extensively studied through functional parameter analysis, impacting performance and daily activities via altered muscle soreness, weakness, and range of motion [7]. Despite its recent application in muscles and tendons, few studies analyzed tissue mechanical properties using elastography to monitor stiffness after the EIMD [8].
The Supersonic Shearwave Imaging (SSI) elastography presents clinical potential as a precise, non-invasive, real-time, in vivo for assessing muscle stiffness post-intervention. Its effectiveness in capturing immediate and long-term changes in stiffness after the intervention makes it essential in clinical practice (For reviews see [8,9,10]). The SSI technique operates in two primary modes: the pushing mode utilizes high-intensity acoustic radiation forces directed at various tissue depths, inducing transverse waves within the tissue. The propagation speed of these shear waves (cs) is then rapidly captured through imaging mode. Under the assumption of tissue isotropy and pure elasticity, the shear modulus (μ) can be estimated as μ = ρ*cs2 (ρ = 1010 kg/m3), considered the biological medium density [11, 12].
In recent years, the assessment of muscle damage using SSI has been applied to monitoring EIMD caused by eccentric contraction in young and healthy individuals. With this technique, Lacourpaille et al. [13, 14], analyzed the biceps brachialis (BB) muscle of healthy untrained individuals at different time points and muscle lengths after EIMD. Significant increases in µ of the BB were observed one-hour post-eccentric exercise with the elbow joint angles at both 110° and 160° [13]. Additionally, Lacourpauille et al. [14] found a similar increase in µ after 30 min when the elbow joint was positioned at 160°. The shorter measured time point after the exercise was 30 min and the peak torque was not measured as the functional measure [14]. The authors suggest that the mechanisms of the increase in stiffness after 30 min or 1 h remain unknown, though they propose that the increase in shear modulus occurs due to perturbations in calcium homeostasis and disturbances in fluid homeostasis within resting muscles, triggered by the damage process.
The shear modulus behavior immediately after damage induction was found only in one study, which investigated the quadriceps muscles of healthy, untrained individuals [15]. Following eccentric exercise, a significant increase in µ (shear modulus) was observed in the rectus femoris (RF) with the knee flexed at 90°, while no changes were noticed in the vastus medialis (VM) and vastus lateralis (VL). In contrast, when the knee was positioned at 30° and 60°, a slight yet statistically significant reduction of approximately 10% was observed solely in the µ of the VL. They suggested that the EIMD can affect synergic muscles differently and the muscle architecture could explain the differences among them. Although prior studies have explored the shear modulus behavior immediately after damage induction in quadriceps muscles of healthy, untrained individuals, with notable findings in muscle response [15], there appears to be a gap in the literature concerning immediate changes in BB muscle stiffness following EIMD induction in well-trained individuals, as well as the assessment of the functional parameter of peak torque.
The inflammatory processes and the formation of muscle edema that appear later seem to be more evident in untrained individuals, as they are not adapted to receive overload stimuli, becoming more susceptible to EIMD due to eccentric exercise [16]. Hence, it's unclear whether changes in BB stiffness in trained individuals exhibit different behavior compared to untrained subjects, either in temporal evolution or intensity, given that these individuals already present morphological and neural adaptations, including alterations in muscle architecture, musculotendinous stiffness, myotendinous unit recruitment, neuromuscular inhibition, and motor unit synchronization [17,18,19,20].
Therefore, the study aims to follow up on the effects of eccentric training on the biceps brachialis stiffness and soreness as well as the elbow flexion maximal voluntary isometric contraction (MVIC), immediately post-intervention, at 10 min, 48 h, and 96 h in well-trained men.
Methods
Participants
In this study, we recruited 13 male participants who met the inclusion criteria of being healthy and having at least 2 years of experience in resistance training (well-trained), while not having any experience with purely eccentric training. The sample was obtained by convenience among students from the Federal University of Rio de Janeiro. As exclusion criteria, individuals with the following characteristics were excluded: (a) those with a history of upper limb injury of any kind within the past 12 months; (b) positive PAR-Q; (c) individuals using ergogenic (included: steroidal-analgesics) resources that may influence the results; and (d) individuals who engaged in purely eccentric training in the past six months. The mean and standard deviation for age, body mass, and height were 27.43 ± 4.19 years, 80.35 ± 2.26 kg, and 176.33 ± 3.19 cm, respectively. During the study, participants were instructed to abstain from any type of vigorous physical exercise or activities (including periodized strength training, physical activities in general and sports) and cautioned against undergoing any treatments, including massage, stretching, or cryotherapy, on the exercised muscles. Moreover, participants were requested not to ingest caffeine, alcohol, and analgesics. Previously the study, all participants signed the informed consent form, which was approved by the Ethics Committee of Clementino Fraga Filho University Hospital (n° 3.031.279). This study was performed in line with the principles of the Declaration of Helsinki.
Experimental design of the study
The experimental protocol involved three visits to the Biomechanics Laboratory. During the initial visit, volunteers underwent a Physical Activity Readiness Questionnaire (PAR-Q), anamnesis to assess their suitability for participation, and the collection of anthropometric data. Subsequently, baseline data were collected for the dependent variables, including two elastographic images of the BB muscle, assessments of muscle soreness, maximal voluntary isometric contraction (MVIC) of the elbow flexors, and eccentric exercise-induced muscle damage. The elastography images, muscle soreness, and MVC measurements were then repeated immediately after the eccentric exercise, as well as at 10 min, 48 h, and 96 h.
Data acquisition
Maximal voluntary isometric contraction
To assess the isometric elbow flexion torque of the non-dominant limb produced by the individuals and its variation throughout the study, the isokinetic dynamometer (Biodex 4 System Pro—Biodex Medical Systems Inc, New York, USA) was used. The participants were positioned in the equipment chair with the hip flexed at 85° and the pelvis immobilized by straps, a cushioned support was used to position the evaluated arm, which remained at an angle of 0° abduction and 45° shoulder flexion [7]. The radioulnar joint was positioned in complete supination, enabling the participant to firmly hold the dynamometer lever arm where the force was applied. The dynamometer rotation axis was aligned with the non-dominant limb elbow joint axis (lateral epicondyle).
The tested limb was assessed by the equipment itself and participants received standardized verbal stimuli to perform the task with maximum effort in all procedures [21]. To ensure that the positioning of each participant was reproduced throughout the study, the following measures were recorded and replicated: dynamometer height; distance from the backrest, chair rotation, and lever arm length. Two maximal voluntary isometric contractions (MVICs) in elbow flexion were acquired for the non-dominant limb during five seconds, with at least a 2-min rest period between them. The peak torque was considered the higher value between the two trials [7].
Muscle soreness
The delayed-onset muscle soreness (DOMS) was measured using a visual analog scale, in which an adapted scale figure, with numbers ranging from 0 to 10, where 0 represents “no discomfort” and 10 represents “worst possible discomfort”. The discomfort was induced through a passive stretching of the trained muscle group, while the participant remained positioned in the BIODEX and was questioned about the level of discomfort after a flexion (140°) and extension (0°) of the elbow [21].
Elastographic images
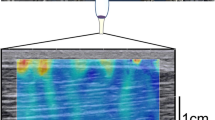
The acquisition of elastographic images was conducted on the non-dominant limb using the AIXPLORER equipment (v.11 Supersonic Image, Aix-en-Provence, France), equipped with a 40 mm linear transducer that operates at a frequency of 10–2 MHz. For the elastography settings, the preset used was MSK, with an opacity of 40%, gain of 90%, SWE opt. setting in penetration mode and the SWE box with dimensions of 1cmX1cm. Acoustic coupling gel (Ultrex gel; Farmativa Indústria e Comercio Ltda, Rio de Janeiro, Brazil) was applied to the skin surface to ensure proper contact. To minimize potential errors in the image acquisition process, the participant's skin was marked with a demographic pen to indicate the precise location where the transducer should be positioned.
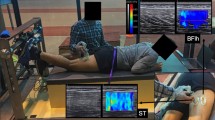
The participants were seated on the Biodex isokinetic dynamometer (Biodex 4 System Pro Medical System Inc, New York, USA) with their elbows flexed at 90°. A mark was made between the acromion angle and the interarticular line of the elbow to denote the exact location for the proximal insertion of the BB. The proximal and distal regions of the BB muscle were delimited by marking a line at 50% between the biceps brachialis insertion and interarticular lines of the elbow, located using B-mode ultrasound. After marking, an experienced evaluator (with over 2 years of experience using the technique) positioned the transducer longitudinally at 90° to the skin, with its lower transducer, with its lower edge on the marked line to capture two images (Fig. 1). Initially, the B-mode image was verified, after by activation of the elastographic mode, which featured a square-shaped mapping area. The preset used was MSK, with a scale ranging from 0 to 300 kPa (color variation from blue, green, red). To stabilize the color mapping and freeze the images, a wait time of 10 s was allowed.

Elastographic images of the BB before eccentric intervention, after, 10 min, 48 h, and 96 h
For data analysis, the images were exported in DICOM format, and the µ values were calculated using a custom Matlab R2015a routine (MathWorks, Natick, MA, USA). A circular region of interest (ROI), 1 cm diameter, at the center of the mapping area was used to measure the µ for the BB. The µ value was considered the mean of the two images.
Eccentric intervention
The exercise intervention consisted of eccentric elbow flexion contractions performed using a dynamometer, with participants seated in the same position as described for the MVIC tests. Each subject completed four sets of 10 repetitions of eccentric contractions, with an angular velocity of 30°/s and a two-minute rest interval between sets [22]. Following each eccentric phase, the elbow joint was passively returned to its initial position. The range of motion utilized ranged from 90° of elbow flexion to full extension of the elbow joint.
Statistical analysis
We conducted a Shapiro–Wilk test to assess the normal distribution of all parameters. For the analysis of torque, we applied repeated measures ANOVA to examine differences at multiple time points, including baseline, immediately after exercise, 10 min, 48 h, and 96 h post-exercise. Subsequently, we performed Tukey's post hoc test to identify any statistically significant differences. For parameters that did not meet the assumptions of normality, such as μ and muscle soreness, we employed non-parametric repeated measures ANOVA (Friedman test). The post hoc analysis for these variables was conducted using Dunn's post hoc test, comparing measurements at baseline, immediately after exercise (after), 10 min, 48 h, and 96 h post-exercise. Statistical significance was set at 5% (p < 0.05), and all data analyses were carried out using the statistical software package Statistica (Statsoft, Inc., Tulsa, OK, USA).
To assess the reliability of the elastographic images, the intraclass correlation coefficient (ICC) was calculated using SPSS 20 (IBM SPSS Statistics Viewer, Armonk, NY, USA). Based on the 95% confident interval, ICC values were interpreted as follows: below 0.49 as poor, 0.5 to 0.75 as moderate, 0.75 to 0.90 as good, and 0.90 to 1.00 as excellent reliability [23].
Results
As for the intra-rater reliability of shear modulus, the ICC ranged from 0.844 to 0.961, classified as good [23]. Statistically significant reductions in μ data were noted when comparing the baseline to both the after-exercise measurement (p = 0.002) and the 10-min measurement (p = 0.002) (Fig. 2). The mean and standard deviation (std) of shear modulus were: baseline 4.61 ± 1.89 kPa; immediately: 2.79 ± 0.60 kPa; 10 min after: 2.90 ± 0.89 kPa; 48 h: 3.86 ± 1.65 kPa and 96 h: 3.37 ± 0.81 kPa.

Shear modulus of the Biceps Brachii data expressed by mean and standard deviation. * for p < 0.05 to Baseline
The torque exhibited statistically significant reductions immediately after (p < 0.001—mean and std immediately: 50.91 ± 15.78 Nm;), at 10 min (p < 0.001—mean and std 10 min: 55.92 ± 14.67 Nm), and at 48 h (p = 0.010—mean and std 48 h: 69.53 ± 20.34 Nm) compared to baseline measurements (80.03 ± 18.86 Nm). Furthermore, when comparing the post-exercise measurements to those at 48 h, significant differences were evident (p < 0.001), and these differences persisted at 96 h (p < 0.001- mean and std 96 h: 74.35 ± 17.35 Nm). Notably, at the 10-min measurement, statistical differences when comparing the 48-h (p = 0.002) and 96-h (p < 0.001) measurements. Additionally, a significant difference was observed between the 48-h and 96-h measurements (p = 0.014) (Fig. 3).

Torque data expressed by mean and standard deviation. * for p < 0.05 to baseline; † for p < 0.05 to after; ‡ for p < 0.05 to 10 min; and # for p < 0.05 to 48 h
Statistically, differences in Muscle Soreness were detected between the 48-h and baseline measurements (p < 0.001), as well as between the after-exercise (p = 0.047) and the 10-min (p = 0.018) in comparison to the baseline. Furthermore, significant differences were observed between the baseline and the 96-h measurement (p < 0.001) (Fig. 4). The mean and standard deviation of muscle soreness were: baseline: 0.85 ± 1.70; immediately: 2.54 ± 1.9; 10 min after: 2.35 ± 2.0; 48 h: 6.66 ± 2.1 and 96 h: 5 ± 2.59.

Muscle Soreness data expressed by mean and standard deviation. * for p < 0.05 to Baseline; †for p < 0.05 to after; ‡ for p < 0.05 to 10 min
Discussion
The best of our knowledge, this is first study to examine the effects of eccentric elbow flexion training on biceps brachialis stiffness, muscle soreness, and MVIC over 96 h in well-trained men. The µ of the BB showed a significant reduction immediately and 10 min after four sets of 10 eccentric repetitions for the elbow flexors. These findings align with the observed variations in the functional parameter, peak torque. According to Paulsen et al. [24], the eccentric exercise protocol for trained individuals effectively induced moderate DOMS, resulting in significant alterations in both maximum torque and perceived discomfort.
The reliability of the shear elastic modulus of biceps brachii muscle was considered excellent (values greater than 0.90) and good (values ranging: 0.75–0.9), in accordance with the literature [23]. The examiner was highly trained, to prevent skin surface compression, which is directly related to changes in the shear modulus, the images were acquired along the longitudinal fibers, following literature recommendations [25].
The distinctive feature of the current study, in comparison to previous ones, was the assessment of tissue stiffness in trained men immediately following the eccentric intervention, as well as 10 min afterward. The rupture of desmin, which plays a role in transmitting tension from the contractile elements and directly affects tension transfer within the membrane, is one possible mechanism to explain this stiffness reduction [14, 26].
An additional aspect to consider, regarding the significant reduction in biceps brachialis stiffness after exercise, is the increased blood circulation in the region following a high-intensity exercise involving a substantial volume of repetitions. A recent review study [25] emphasizes the importance of acknowledging that this factor could impact elastography measurements by reducing their values. However, the current literature lacks comprehensive information, such as the variation range or correction factor, to standardize how blood flow might affect stiffness values. Consequently, further investigations are warranted to understand the effect of blood flow in using this technique, especially in cohorts comprising both trained and untrained individuals.
Similarly, the influence of increased muscle temperature resulting from the high exercise volume may have affected the mechanical properties of the tissue, particularly the stiffness of the medium [27]. Fifteen minutes after cyclic eccentric damage of extensor digitorum longus and tibialis anterior mouse fibers, a disruption of the membranes causes loss of the cytoskeletal protein, desmin [28], which could potentially explain the stiffness reduction immediately after EIMD.
The literature indicates that leukocytes are regulated in response to tissue degradation levels, such that when intracellular damage is extensive, a significant accumulation of leukocytes occurs in the damaged tissue to restore intracellular calcium homeostasis. However, sarcomere rupture may occur without a significant leukocyte accumulation [29,30,31]. Therefore, we suggest that the reduction in tissue stiffness in trained individuals may be explained by the rupture of passive sarcomere elements and the cytoskeleton due to mechanical stresses imposed by eccentric exercise to induce DOMS, without an immediate significant accumulation of intracellular fluids. These fluids may potentially contribute to tissue stiffness increase at a later stage32.
Only two studies examining the behavior of µ in the biceps brachii (BB) were identified. When µ in the BB was analyzed with the elbow at 70° of elbow flexion (180° = full extension), no significant changes were observed for untrained individuals at 1 h, 48 h, and 21 days after damage induction [13], and after 30 min [14]. However, when the elbow was positioned at 160° of extension, BB µ exhibited a significant increase at one hour, 48 h, and 21 days [13], and a similar pattern was observed after 30 min in the study by Lacourpaille et al. [14]. These authors [13, 14] report that the mechanisms involved in justifying the µ increase are not yet fully established. Still, they suggest that this increase may be associated with the rapid disruption of calcium homeostasis, increased intramuscular fluid, and the initiation of edema formation, as measurements were not taken immediately after exercise, allowing time for the onset of the inflammatory process. Regarding the increase in µ only for joint amplitudes with the muscle in a more elongated position, the authors propose that this increase may reflect the heightened sensitivity of muscle fibers to Ca2+. Methodological differences in image acquisition time and joint position may account for the discrepancies in the results found in the present study.
The loss of voluntary force production capacity is the primary functional variable studied in EIMD [4, 33]. Regardless of the sample characteristics, this response to EIMD is consistently observed and was no different in the current study, with a reduction of approximately 40% immediately after the intervention and 35% 10 min later. These findings align with the study conducted by Newton et al. [16] for elbow flexors, however, the same effect cannot be observed for other exercises, such as bench press, for example with approximately 18% of reduction on horizontal adduction peak torque [18]. Recognizing that the reduction in force production capacity in trained men is not related only to the neural factors [34], it is believed that the failure in the coupling of cross-bridges is the primary contributor to force depression, in conjunction with other structural disorganization following tissue injury [35].
The DOMS peaked at 48 h, displaying significant differences compared to the baseline measurement until 96 h. Specifically for trained individuals, these findings align with existing literature on trained individuals subjected to the EIMD regardless of the muscle group involved, such as for horizontal shoulder adductors [17, 18] and elbow flexors [16]. DOMS is widely accepted to be a consequence of physical damage to muscle tissue that initiates subsequent inflammatory processes [22]. The EIMD triggers the sensitization process in the connective tissue surrounding the muscles, in which pain nociceptors are activated through bradykinin B2 and inflammatory cytokines (COX-2) [36].
Because the trained sample participating in the present study is accustomed to conventional resistance exercise, it appears that this long-term activity may lead to a protective mechanism against muscle damage induced by eccentric intervention for elbow flexors similar to the second bout effect observed in untrained individuals [16]. As such, the immediate and 10-min post-intervention decrease in muscle stiffness (µ) responses may be associated with the individuals' training level, distinct from the sample used by Lacourpaille et al. [14] 30 min after eccentric intervention.
The primary focus of this study was to assess the usefulness of elastography in analyzing post-high-intensity exercise effects, considering in the subjects' training level and the technique's capacity to monitor the transient exercise-induced injury process. However, the current investigation exhibits some limitations deserving careful attention, such as the absence of commonly utilized markers in the assessment of EIMD, including blood markers, swelling, range of motion [37] and the immediate post-exercise assessment of blood flow. Additionally, it is imperative to highlight the non-generalizability of this study's outcomes to other muscle groups. Notably, existing literature extensively documents the heightened vulnerability of arm muscles to muscle damage compared to their lower limb counterparts [38].
Conclusion
This study presents the immediate and short-term implications of eccentric exercise-induced muscle damage (EIMD) on biceps brachialis stiffness using elastography, alongside assessments of muscle soreness and maximum voluntary isometric contraction (MVIC) in well-trained individuals. The observed substantial reductions in torque and muscle stiffness immediately and 10 min post-exercise point towards the potential involvement of mechanical stress, sarcomere and cytoskeletal rupture. Notably, the absence of significant intracellular fluid accumulation in this early phase of EIMD unveils a distinct response pattern in trained individuals when compared to results in the literature with untrained voluntary. These findings emphasize the application of elastography in the follow-up of the acute biomechanical changes following high-intensity exercise, shedding light on potential adaptations in tissue response among trained subjects. Moreover, further studies are needed to analyze different groups with varying training levels and different muscle groups with distinct muscular architecture, enabling future clinical application of SSI elastography technique in evaluating training periods or rehabilitation after injuries. As SSI technique can provide precise insights into muscle stiffness and tissue adaptations in response to training and intense exercise, it can assist in planning training programs and rehabilitation after injuries.
Data and materials availability
The data that support the findings of this study are available from the corresponding author upon reasonable request.
References
Withee ED, Tippens KM, Dehen R, Tibbitts D, Hanes D, Zwickey H (2017) Effects of Methylsulfonylmethane (MSM) on exercise-induced oxidative stress, muscle damage, and pain following a half-marathon: A double-blind, randomized, placebo-controlled trial. J Int Soc Sports Nutr 14(1):1–11. https://doi.org/10.1186/s12970-017-0181-z
Matta TTD, Pereira WCDA, Radaelli R, Pinto RS, Oliveira LFD (2018) Texture analysis of ultrasound images is a sensitive method to follow-up muscle damage induced by eccentric exercise. Clin Physiol Funct Imaging 38(3):477–482. https://doi.org/10.1111/cpf.12441
Peake JM, Suzuki K, Wilson G, Hordern M, Nosaka K, MacKinnon L et al (2005) Exercise-induced muscle damage, plasma cytokines, and markers of neutrophil activation. Med Sci Sports Exerc 37(5):737–745. https://doi.org/10.1249/01.mss.0000161804.05399.3b
Hyldahl RD, Hubal MJ (2014) Lengthening our perspective: Morphological, cellular, and molecular responses to eccentric exercise. Muscle Nerve 49(2):155–170. https://doi.org/10.1002/mus.24077
Lieber RL, Fridén J (1999) Mechanisms of muscle injury after eccentric contraction. J Sci Med Sport 2(3):253–265. https://doi.org/10.1016/s1440-2440(99)80177-7
Clarkson PM, Sayers SP (1999) Etiology of exercise-induced muscle damage. Can J Appl Physiol 24(3):234–248. https://doi.org/10.1139/h99-020
Matta TT, Pinto RO, Leitão BFM, de Oliveira LF (2019) Non-uniformity of elbow flexors damage induced by an eccentric protocol in untrained men. J Sport Sci Med 18(2):233
Ličen U, Kozinc Ž (2022) Using shear-wave elastography to assess exercise-induced muscle damage: a review. Sensors (Basel) 22(19):7574. https://doi.org/10.3390/s22197574
Lima KMM, Costa Jr JFS, Pereira de WCA, De Oliveira LF. (2018) Assessment of the mechanical properties of the muscle-tendon unit by supersonic shear wave imaging elastography: a review. Ultrasonography 37(1):3–15. https://doi.org/10.14366/usg.17017
Miller T, Bello UM, Tsang CSL, Winser SJ, Ying MTC, Pang MYC (2023) Using ultrasound elastography to assess non-invasive, non-pharmacological interventions for musculoskeletal stiffness: a systematic review and meta-analysis. Disabil Rehabil 5:1–15. https://doi.org/10.1080/09638288.2023.2252744
Shiina T (2013) JSUM ultrasound elastography practice guidelines: basics and terminology. J Med Ultrason 40(4):309–323. https://doi.org/10.1007/s10396-013-0490-z
Gennisson JL, Deffieux T, Fink M, Tanter M (2013) Ultrasound elastography: principles and techniques. Diagn Interv Imaging 94(5):487–495. https://doi.org/10.1016/j.diii.2013.01.022
Lacourpaille L, Nordez A, Hug F, Couturier A, Dibie C, Guilhem G (2014) Time-course effect of exercise-induced muscle damage on localized muscle mechanical properties assessed using elastography. Acta Physiol 211(1):135–146. https://doi.org/10.1111/apha.12272
Lacourpaille L, Nordez A, Hug F, Doguet V, Andrade R, Guilhem G (2017) Early detection of exercise-induced muscle damage using elastography. Eur J Appl Physiol 117(10):2047–2056. https://doi.org/10.1007/s00421-017-3695-9
Xu J, Fu SN, Zhou D, Huang C, Hug F (2019) Relationship between pre-exercise muscle stiffness and muscle damage induced by eccentric exercise. Eur J Sport Sci [Internet] 19(4):508–516. https://doi.org/10.1080/17461391.2018.1535625
Newton MJ, Morgan GT, Chapman DW, Nosaka KK (2008) Trained and untrained men. J Strength Cond Res 22(2):597–607. https://doi.org/10.1519/JSC.0b013e3181660003
Meneghel A, Verlengia R, Criso AH, Aoki MS, Nosaka K, Mota GR, Lopes CR (2014) Muscle damage of resistance-trained men after two bouts of eccentric bench press exercise. J Strength Cond Res 28(10):2961–2966. https://doi.org/10.1519/JSC.0000000000000494
Ferreira DV, Ferreira-Ju´nior, JB, Soares, SRS, Cadore, EL, Izquierdo, M, Brown, LE, and Bottaro, M. (2017) Chest press exercises with different stability requirements result in similar muscle dam- age recovery in resistance trained men. J Strength Cond Res 31(1):71–79. https://doi.org/10.1519/JSC.0000000000001453
Matta TT, de Salles BF, Spinetti J, Simão R, Oliveira LF (2010) Specific tension index of elbow flexors in trained and untrained men. Rev Bras Cineantropometria e Desempenho Hum 12(1):62–67
Suchomel TJ, Nimphius S, Bellon CR, Stone MH (2018) The importance of muscular strength: training considerations. Sport Med [Internet] 48(4):765–785. https://doi.org/10.1007/s40279-018-0862-z
Chen HL, Nosaka K, Chen TC (2012) Muscle damage protection by low-intensity eccentric contractions remains for 2 weeks but not 3 weeks. Eur J Appl Physiol 112(2):555–565. https://doi.org/10.1007/s00421-011-1999-8
Chan R, Newton M, Nosaka K (2012) Effects of set-repetition configuration in eccentric exercise on muscle damage and the repeated bout effect. Eur J Appl Physiol 112(7):2653–2661. https://doi.org/10.1007/s00421-011-2247-y
Koo TK, Li MY (2016) A guideline of selecting and reporting intraclass correlation coefficients for reliability research. J Chiropr Med 15(2):155–163. https://doi.org/10.1016/j.jcm.2016.02.012
Paulsen G, Mikkelsen UR, Raastad T, Peake JM (2012) Leucocytes, cytokines and satellite cells: what role do they play in muscle damage and regeneration following eccentric exercise? Exerc Immunol Rev 18:42–97
Zhu J, Qiu L, Ta D et al (2024) Chinese ultrasound doctors association guideline on operational standards for 2-D shear wave elastography examination of musculoskeletal tissues. Ultrasound Med Biol 50(2):175–183. https://doi.org/10.1016/j.ultrasmedbio.2023.10.005
Capetanaki Y, Bloch RJ, Kouloumenta A, Mavroidis M, Psarras S (2007) Muscle intermediate filaments and their links to membranes and membranous organelles. Exp Cell Res 313(10):2063–2076. https://doi.org/10.1016/j.yexcr.2007.03.033
Sapin-De Brosses E, Gennisson JL, Pernot M, Fink M, Tanter M (2010) Temperature dependence of the shear modulus of soft tissues assessed by ultrasound. Phys Med Biol 55(6):1701–1718. https://doi.org/10.1088/0031-9155/55/6/011
Lieber RL, Thornell LE, Fridén J (1996) Muscle cytoskeletal disruption occurs within the first 15 min of cyclic eccentric contraction. J Appl Physiol 80(1):278–284. https://doi.org/10.1152/jappl.1996.80.1.278
Dehne N, Kerkweg U, Flohé SB, Brüne B, Fandrey J (2011) Activation of hypoxia-inducible factor 1 in skeletal muscle cells after exposure to damaged muscle cell debris. Shock 35(6):632–638. https://doi.org/10.1097/SHK.0b013e3182111f3d
Frangogiannis NG (2008) The immune system and cardiac repair. Pharmacol Res 58(2):88–111. https://doi.org/10.1016/j.phrs.2008.06.007
Féasson L, Stockholm D, Freyssenet D, Richard I, Duguez S, Beckmann JS et al (2002) Molecular adaptations of neuromuscular disease-associated proteins in response to eccentric exercise in human skeletal muscle. J Physiol 543(1):297–306. https://doi.org/10.1113/jphysiol.2002.018689
McKune AJ, Semple SJ, Peters-Futre EM (2012) Acute exercise-induced muscle injury. Biol Sport 29(1):3–10. https://doi.org/10.5604/20831862.978976
Kuipers H (1994) Exercise-induced muscle damage. Int J Sports Med 15(3):132–135. https://doi.org/10.1055/s-2007-1021034
Ye X, Beck TW, Wages NP (2015) Reduced susceptibility to eccentric exercise-induced muscle damage in resistance-trained men is not linked to resistance training-related neural adaptations. Biol Sport 32(3):199–205. https://doi.org/10.5604/20831862.1150301
Warren GL, Ingalls CP, Lowe DA, Armstrong RB (2002) What mechanisms contribute to the strength loss that occurs during and in the recovery from skeletal muscle injury? J Orthop Sports Phys Ther 32(2):58–64. https://doi.org/10.2519/jospt.2002.32.2.58
Peake JM, Neubauer O, Gatta PAD, Nosaka K (2017) Muscle damage and inflammation during recovery from exercise. J Appl Physiol 22(3):559–570. https://doi.org/10.1152/japplphysiol.00971.2016
Boyd L, Deakin GB, Devantier-Thomas B, Singh U, Doma K (2023) The effects of pre-conditioning on exercise-induced muscle damage: a systematic review and Meta-analysis. Sport Med 53(8):1537–1557. https://doi.org/10.1007/s40279-023-01839-8
Chen TC, Lin KY, Chen HL, Lin MJ, Nosaka K (2011) Comparison in eccentric exercise-induced muscle damage among four limb muscles. Eur J Appl Physiol 111(2):211–223. https://doi.org/10.1007/s00421-010-1648-7
Acknowledgements
The authors acknowledge the financial support of the Brazilian Research agencies FAPERJ (Grant n° E-26/202955/2017) and FINEP (Grant n°. 01.23.4567.89). Author Maria Clara A. Brandão has received research support from CNPq.
Author information
Authors and Affiliations
Contributions
All authors contributed to the study conception and design. Material preparation, data collection and analysis were performed by Maria Clara A. Brandão and Lino de Azevedo Matias. The first draft of the manuscript was written by Thiago Torres da Matta. The second draft of the manuscript was written by Maria Clara A. Brandão and Liliam Fernandes de Oliveira. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare no conflict of interest.
Ethical approval
This study was performed in line with the principles of the Declaration of Helsinki. Approval by the Ethics Committee of Clementino Fraga Filho University Hospital (n° 3.031.279).
Consent to publish
All volunteers authorized the publication of the results.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Brandão, M.C.A., Matias, L.A., da Matta, T.T. et al. Biceps brachii elastography in well-trained men post eccentric exercise-induced muscle damage. J Ultrasound (2024). https://doi.org/10.1007/s40477-024-00886-9
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s40477-024-00886-9