
Abstract
Introduction
Obstructive sleep apnea (OSA) is a chronic disease with a high populational prevalence that is characterized as airway closure during sleep. Treatment is multidisciplinary and varies according to each case. Continuous positive airway pressure (CPAP), oral appliances, and surgery are the primary therapeutic options. Non-invasive conservative treatments such as sleep hygiene, positional therapy, physical exercises, and weight loss aim to reduce the worsening of the disease while being complementary to the invasive primary treatment.
Objective
To analyze the impact of non-invasive conservative therapies on the clinical manifestations of OSA syndrome (OSA), compared with other interventions.
Method
This was a systematic review with meta-analysis. The searches were performed without filters for the time period, type of publication, or language. Randomized clinical trials on subjects over 18 years of age diagnosed with untreated OSA were included. Responses to non-invasive conservative treatment were compared with responses to the primary intervention. Primary outcomes were assessed using the Epworth Sleepiness Scale and/or Functional Outcomes of Sleep Questionnaire (FOSQ).
Results
A total of eight studies were included in the review. The heterogeneity of the effect was estimated at 89.77%. Six studies compared conservative treatment with CPAP, one with oral appliances, and one with oropharyngeal exercises. Using the Epworth Sleepiness Scale measurements, the standardized difference in the estimated means, based on the random-effects model, was 0.457 (95% CI (1.082 to 0.169)) and the mean result did not differ significantly from zero (z = 1.43; p = 0.153). The conservative therapies assessed in this study improved the subjective quality of sleep, although the post-treatment ESE scores did not show significant results. The reduction in AHI and better outcomes in the evaluated domains, as well as in cognition and mood, were superior in the groups that received CPAP and IOD.
Conclusion
The most commonly used treatments of choice for OSA are invasive, including the use of CPAP, oral appliances, and surgeries, being the most utilized options. This study demonstrated that non-invasive conservative treatments, such as sleep hygiene, yield results as effective as invasive treatments. Further studies are needed to confirm this result and to predict whether invasive treatment can be used as the primary treatment or only as a supplement.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Obstructive sleep apnea (OSA) is a condition characterized by repetitive pharyngeal collapses during sleep, which results in fragmentation and desaturation of sleep and sympathetic surges. It affects 2 to 14% of the adult population, provokes excessive daytime sleepiness [1, 2], and increases the risk of severe diseases that could overload healthcare systems and worsen quality of life [2,3,4].
Treatments for OSA are multidisciplinary and vary according to the severity of the case. Continuous positive airway pressure (CPAP) is an effective type of treatment that improves clinical symptoms and reduces the apnea–hypopnea index (AHI) [5]. However, adherence to CPAP treatment is an important problem that needs to be considered [3,4,5]. Oral devices for advancing the mandible and retaining the tongue present satisfactory responses for controlling mild OSA [6, 7], although the results are inferior to those from CPAP [8]. Surgical procedures are applicable for correcting anatomical alterations and have a good cost–benefit relationship for patients with severe apnea who cannot tolerate CPAP [3, 9]. In comparison with CPAP and oral devices, orthographic surgery to advance the maxilla and mandible is considered to be the most invasive type of treatment [10].
Simple interventions such as sleep hygiene, adjustment of body position during sleep, weight loss, physical exercise, and lifestyle change [11,12,13,14] are used as conservative treatment with the aim of minimizing and/or delaying the worsening of the disease. In addition, conservative treatments involve the reduction of the apnea–hypopnea index and sleep fragmentation, lifestyle changes, diminution of risk factors, elimination of snoring, and reduction of daytime sleepiness and fatigue [15, 16].
Studies have shown that there are relationships between weight loss and reduction of respiratory events during sleep [14], between alcohol intake and increased incidence of obstructive apnea [17], and between sleep deprivation/fragmentation and greater collapsibility of the upper airways [18]. Conservative treatments favor overall health, improved respiratory abnormalities, and, consequently, improved sleep quality and clinical manifestations [11, 19]. They have also been recommended as a complementary therapy in cases in which CPAP, oral devices, or surgery is used [8]. Sleep hygiene integrated with the treatment options favors the organization of the sleep routine and helps in rehabilitation and adherence to treatments [20, 21]. These are simple measures, but managing them requires considerable clinical skill [22, 23].
There is a shortage of data in the literature correlating sleep hygiene with clinical improvement of OSA. These good habits are recommended for diminishing daytime sleepiness and depression and for improving quality of life, independent of any sleep disorder [12, 14, 20]. Positional devices are simple public utility measures that can be used in combination with or separately from other treatment options and can also be chosen as therapy for individuals who cannot tolerate CPAP or for low-income individuals [23,24,25].
Objectives
The aim of this review was to compare and analyze the impact of conservative treatments such as sleep hygiene, weight loss, positional therapy, and/or physical exercise on the clinical manifestations of OSA, in comparison with other interventions.
Methods
Design
This study consisted of a systematic review of the literature. The registration in Prospective Register of Systematic Reviews (PROSPERO) was requested twice: in November 2020 and in February 2021. We received the number 209699 as provisional. However, the team did not verify eligibility because they focused their efforts on COVID-19 records throughout 2021, the period during which this review was proceeding to be finalized. It followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines.
Search and study selection criteria
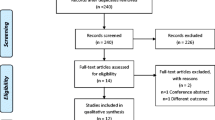
The search for studies was conducted by a non-author colleague, comprehensively among published papers that met the eligibility criteria of this study. The following electronic databases were examined: PubMed, PubMed Central, VBS (Lilacs, Medline), Cochrane, Scopus, Embase, Web of Science, and EBSCOhost. The search strategies were personalized for each database and involved the use of keywords relating to the population and intervention. No additional filters for time of publication or language were used (Fig. 1).

Search strategies
The guidelines represented by the acronym PICO (population, intervention, comparison, outcome) were used in elaborating the present review. The population was formed by adults over the age of 18 years of both sexes with an untreated previous diagnosis of OSA syndrome in accordance with the standardized definitions of the American Academy of Sleep Medicine (AASM) [26]. The trials included used either or both of the following measurement instruments: the Epworth Sleepiness Scale (ESS), which assesses excessive daytime sleepiness due to OSA; and the Functional Outcomes of Sleep Questionnaire (FOSQ), which assesses the impact of sleepiness on daily activities. Studies in which conservative treatment was compared with another type of intervention were also included. The type of study considered was restricted to randomized controlled trials, and these needed to present results in a form that was usable for meta-analysis, including the availability of unadjusted means and standard deviations (SD) or 95% confidence intervals. The inclusion and exclusion criteria used are detailed in Table 1. The present review sought to investigate and answer the following question: in patients with OSAS, what is the effect of conservative treatment on clinical manifestations, in comparison with other interventions?
A total of seven studies were included in the meta-analysis. Among these, one study allocated three groups to intervention, and the use of CPAP, intraoral devices (IOD), and conservative therapy was compared, and another study divided the participants into hypertensive and non-hypertensive groups.
The analysis of these seven studies was conducted using the standardized difference in the means as the outcome measurement. A random-effects model was fitted to the data. The degree of heterogeneity (tau2) was estimated using a limited maximum likelihood estimator. In addition to estimating tau2, Cochran’s Q test for heterogeneity and the I2 statistic were reported. Correlation classification and regression tests using the standard error of the observed result as a predictor were implemented to assess the asymmetry of funnel plots. The Jamovi 1.6.16 software was used.
Results
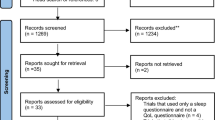
The data set that formed the input to screening was finalized as 1579 references. Within the computerized screening tool, 496 studies were excluded because they were either duplicates or systematic reviews. The remaining studies formed the input to a selection process according to the article title and abstract, which was conducted independently by two authors of this review. Any divergences in this selection were resolved by a third member of the study group. Following this, a complete analysis of the text of 28 studies was conducted blindly by three authors, and any divergences were resolved by reaching a consensus. As shown in Fig. 2, three studies were excluded because their analyses were not conducted using the ESS and/or FOSQ, eight because they presented insufficient data, five because they did not have a comparison group, three because they were follow-up studies, and one because it was a protocol. Although contacts were made with study authors to request further data, no responses were obtained. In the end, a total of eight articles were included in the present review for meta-analysis.

Flow diagram
Risk-of-bias analysis
The Cochrane Collaboration tool was used to assess the risk of bias for each randomized controlled trial, in seven categories (Fig. 3). Domain 3 (blinding of the participants and professional personnel) was not applicable as a significant risk of bias given that it was not possible to blind either of the parties involved for the type of intervention received. The risk of bias for each study was considered low when the required information was presented in the article or when the methodological quality pointed towards low risk. Three studies showed unclear risk in domain 1 (random sequence generation), four in domain 2 (allocation concealment), five in domain 3 (blinding of participants and researchers), and five in domain 4 (verification of results). Situations of the absence of information on allocation and blinding were considered to present an unclear risk of bias. No risk of bias was considered to have had an impact on the results from the meta-analysis.

Risk-of-bias analysis
Data collection process
In all the studies, polysomnography examinations were conducted over an entire night in order to diagnose OSA, and sleep parameters (AHI) were reported based on the standardized definitions of the American Academy of Sleep Medicine. The experimental groups of conservative therapies were compared with the use of CPAP, intraoral devices, and oropharyngeal exercises.
Study characteristics
The characteristics of the studies included in the meta-analysis are described in Table 2. These eight studies had a total of 671 participants with OSA, which was predominantly mild to moderate and/or moderate to severe, with a wide range of adult ages. Not all the studies specified the percentages of men and women, and thus, it was not possible to calculate means according to sex. Six studies made comparisons with the use of CPAP, one with the use of an intraoral device, and one with oropharyngeal exercises. One study integrated the experimental intervention with conservative treatment consisting of the use of a nasal dilator with the placebo effect, and for this reason, it was considered that this study fulfilled the inclusion criteria. Moreover, although the presence of OSA plus associated diseases was an exclusion criterion, it was decided to include a study in which the results were separated into groups of hypertensive and non-hypertensive participants.
Synthesis of results and meta-analysis
Table 3 summarizes the scores from the FOSQ applied before and after the intervention in two studies. Figure 4 shows the standardized mean differences from the ESS, which ranged from − 2.3234 to 0.5873. Most of these estimates were negative (67%).

Forest plot. Results between 0 and − 3 show that the interventions using CPAP and IOD were better than conservative treatment
The standardized mean difference estimated based on the random-effects model was 0.457 (95% confidence interval (CI), 1.082 to 0.169). Therefore, the mean result did not differ significantly from zero (z = 1.43; p = 0.153). In the Q test on the random-effects model, the true results seemed to be heterogenous (Q (8) = 65.559; p < 0.001; tau2 = 0.7959; I2 = 89.77%). The 95% CI for the true results was − 2.3136 to 1.400. Therefore, although the mean result was estimated as negative, the true result in some studies may in fact have been positive.
The classification correlation of the Begg-Mazumbar test (p = 0.919) and the Egger regression test (p = 0.722) indicated that there was no asymmetry in the funnel plot (Fig. 5). Studentized residuals and Cook distances were used to examine whether the studies might have been discrepant and/or influenced by the model. The studentized examination on the residuals showed that the study by Ballester et al. (1999) had a value greater than ± 2.8070 and may have been a potential outlier in the context of this model. According to the Cook distances, this study could be considered excessively influential. Therefore, it was decided to exclude Ballester (1999) and redo the meta-analysis.

Funnel plot
Discussion
This was the first meta-analysis to evaluate the impact of conservative treatment consisting of sleep hygiene, weight loss, positional therapy, and physical exercise on the clinical manifestations of OSA. Although there is evidence showing that treatment with CPAP is effective, no study has compared subgroups of different severities of OSA, a point that was previously identified by Sánchez (2008). The heterogeneity of the severity of this disease was one of the limitations of the present review. The clarity regarding CPAP titration was not achieved. Regarding patient tolerance, only those who completed the research without major discomfort were included in the final results.
The first review addressing this topic was not concluded due to a lack of published trials [12]. A bibliographic survey on randomized controlled trials that was published in 2008 investigated the effectiveness of CPAP in relation to daytime sleepiness, depression, and cognitive functions among patients who received CPAP, compared with more conservative measures [27]. However, the impact of these therapies was not quantified, and this formed the main objective of the present review.
Among the studies included in this review, only two of them assessed the impact of OSA on daily activities using the FOSQ tool. Monasterio (2001) showed that the group that received CPAP achieved a slight improvement after the intervention. Benoist (2016) found that there was a minimal change in the group that received conservative treatment, while the IOD group remained unchanged. In both of these studies, the changes observed were not clinically relevant. However, the reasons for this result were not explored by the authors.
In the analysis of the studies included in this meta-analysis, four of them showed results ranging between positive and negative, while in three, the results of conservative treatment were inferior. The reason for this discrepancy is not clear, since the only methodological characteristic widely prevalent in most studies was the combination of CPAP with conservative treatment. In the treatment of obstructive sleep apnea, the literature shows favorable outcomes for CPAP therapy and oral appliances, while the results for conservative treatment are less significant. However, the statistical analysis of this current review indicates that CPAP therapy, IOD, and oropharyngeal exercises do not show superior results compared to conservative treatment.
The heterogeneity of effect, which was estimated to be 89.77%, came from the difference in the procedures used in the studies that were included. The factors that may have contributed to this difference in our analyses were disparities in the total sample size, age group studied, severity of apnea, and type of intervention. One of the limitations of the review was the lack of homogeneity in the study data, which hindered a more detailed analysis of subgroups. This issue underscores the need for future studies to address these risk factors separately, enabling the acquisition of more concrete data. Another important factor to be raised concerns the length of follow-up which was between 2 and 6 months; i.e., each group had a different amount of time within which to adapt to and consolidate the proposed treatment. Furthermore, in four studies, the intervention in the comparison group was combined with guidance about sleep hygiene, weight loss, and/or physical activity.
The conservative therapies consisting of guidance about sleep hygiene, weight loss, positional therapy, and physical activity improved the subjective quality of sleep, but the ESS scores post-treatment were not statistically significant. The reduction in the AHI was greater in the groups that received CPAP and IOD. Previous studies demonstrated the efficacy of CPAP for reducing excessive daytime sleepiness, one of the main symptoms relating to OSA, through ESS scores and the objective multiple sleep latency test (MSLT) [27,28,29,30]. However, Zhao (2017) showed that conservative measures have important clinical implications in apnea treatments, even if the ESS score remains unchanged [31], and that finding was confirmed in the present review. Although daytime sleepiness is the main complaint among patients with OSA, it may be a marker for other sleep-related issues [32]. Moreover, even though CPAP is more effective for reducing respiratory disorders, oral devices present better adherence [33].
Sleep hygiene
Positive-pressure interventions in the airways presented better results in the domains evaluated in all the studies that compared conservative treatment with CPAP. Sleep hygiene did not show any significant reduction in the AHI or in OSA symptoms. However, it was unanimously concluded that conservative treatment can be the first approach and/or a resource associated with any therapeutic option [23, 34, 35]. More recent studies have shown that the daytime sleepiness that impacts the quality of life of people with OSA was strongly related to poor sleep hygiene among the individuals investigated [20, 36, 37]. In addition to presenting a positive correlation with patients’ subjective symptoms, good sleep hygiene may be related to good general quality of sleep, even if to a lesser degree than other interventions addressed in this review [38].
Redline (1999) was the first study to investigate and compare types of nonsurgical treatment for mild to moderate OSA. The results from that study showed that the impact of CPAP was significantly greater with regard to wellbeing, mood, and functional status than that of sleep hygiene advice. Lam (2006) compared CPAP, IOD, and sleep hygiene advice, three types of nonsurgical treatment that are commonly used for OSA. The ESS score decreased significantly in all three groups but the results for the CPAP group were superior despite being inconsistent in milder cases. A study conducted in 2019 contradicted that finding, through affirming that patients with mild OSA feel the benefit from regular use of CPAP, and suggested that further studies should be conducted to assess whether other therapies might be as effective as CPAP in that population [38]. Redline and Lam showed that the group that received sleep hygiene advice did not achieve improvements in sleep parameters and health-related quality of life [34, 39]. These results were also confirmed through the study by Ballester (1999), even though the ESS score diminished in both groups: the improvement in the domains evaluated was greater in the group that received CPAP plus conservative treatment, including in the cases of mild apnea [40].
Physical exercises and weight loss
Torres-Castro (2019) and Benoist (2016) can be highlighted among the studies because they did not include CPAP in any intervention or control group. Torres-Castro [41] explored the impact of physical activity plus sleep hygiene plus diet in group 1, and in their group 2, used the same interventions plus oropharyngeal exercises. The AHI did not differ between the groups, but after dividing the subjects according to age, those under 60 years of age showed a significant reduction after the intervention, while the older participants presented worsened sleep. It has been shown in the literature that physical activity reduces the severity of OSA, improves sleep efficiency, and diminishes daytime sleepiness with minimal alterations to body weight [42, 43].
Cipriano et al. compared CPAP with physical training and divided their two groups into hypertensive and non-hypertensive individuals. Their findings showed that there was no significant difference in daytime sleepiness between the groups, and they explained this in terms of the short duration of the treatment [44]. Studies indicate that more than 50% of moderate to severe OSA cases are related to obesity [45]. In these circumstances, lifestyle changes such as physical exercise and diet can favor significant improvements. A study from 2022 showed that these habits significantly reduced the AHI, with 15% of the observed group achieving complete remission of OSA and 45% not requiring CPAP [46]. According to Gambino and colleagues (2022), even if the expected effects do not meet the estimates, weight loss and physical activity should always be recommended to obese patients with OSA. [47]
Positional therapy
Benoist [48] analyzed the efficacy of positional therapy in comparison with the use of an oral device and observed that these treatments were equally effective for reducing the AHI. However, these authors left open the need for further studies combining these two therapies, with the suggestion that non-supine OSA could potentially be eliminated. Regarding adherence, positional therapy was better because it did not present side effects. According to the literature, the better the adherence is, the greater the efficacy of the treatment will be [49,50,51]. Although its effect is smaller than CPAP, the emergence of technological devices is very promising, as they have shown good effectiveness, sparked interest among CPAP-intolerant individuals, and increased long-term adherence [52].
Impact on cognition and mood
Two studies investigated the impact of interventions on daytime functioning and cognition. Ballester reported that there were improvements in daytime functioning, energy, and emotional reactions in the group that received CPAP [53]. Dalmases found that elderly people with severe OSA, over 65 years of age, presented cognitive impairment that mainly affected tasks requiring attention. These difficulties could be resolved through CPAP, which improved the functioning of the frontal lobe, but no improvement was seen through conservative therapy [54]. Efforts to elucidate the impact of OSA on cognition have been made in studies in the literature. It has been shown that patients with OSA have problems with attention and declining short- and long-term memory [55, 56], complaints relating to emotional control and motivation [57], and problems regarding executive functions and the ability to learn new things. It has also been shown that individuals with apnea present significantly worse performance in verbal memory tests [58, 59], resolution of problems and judgment [60], and flexibility and strategic planning [61].
In addition to surveying cognitive impairment, studies have addressed mood changes among people with OSA. These individuals have shown a high prevalence of depression and anxiety, even in cases of mild OSA [31, 62, 63]. A study conducted in 2004 reported that more than 40% of the patients with apnea presented clinically significant depression [64]. These data correlate with findings from other clinical studies in which a high prevalence of depression and anxiety among individuals with OSA was identified [65, 66].
Conclusion
The most commonly used treatments of choice for OSA are invasive, including the use of CPAP, oral appliances, and surgeries, being the most utilized options. This study demonstrated that non-invasive conservative treatments, such as sleep hygiene, yield results as effective as invasive treatments. Further studies are needed to confirm this result and to predict whether invasive treatment can be used as the primary treatment or only as a supplement.
Data availability
All data on the measured ecosystem variables indicating ecosystem functions that support the findings of this study are included within this paper and its Supplementary Information files.
References
Semelka M, Jonathan W, Floyd R (2016) Diagnosis and treatment of obstructive sleep apnea in adults. Am Fam Physician Pennsylvania Am Fam Physician 94(5):355–360
Ye L et al (2015) Spousal involvement and CPAP adherence: a dyadic perspective. Sleep Med Rev 19:67–74. https://doi.org/10.1016/j.smrv.2014.04.005
Tan KB, Toh ST, Guilleminault C, Holty JE (2015) A cost-effectiveness analysis of surgery for middle-aged men with severe obstructive sleep apnea intolerant of CPAP. J Clin Sleep Med 11(5):525–535
Chai-Coetzer CL, Luo YM, Antic NA, Zhang XL, Chen BY, He QY, Heeley E, Huang SG, Anderson C, Zhong NS, McEvoy RD (2013) Predictors of long-term adherence to continuous positive airway pressure therapy in patients with obstructive sleep apnea and cardiovascular disease in the SAVE study. Sleep 36(12):1929–1937
Avlonitou E, Kapsimalis F, Varouchakis G, Vardavas CI, Behrakis P (2012) Adherence to CPAP therapy improves quality of life and reduces symptoms among obstructive sleep apnea syndrome patients. Sleep Breath 16(2):563–569. https://doi.org/10.1007/s11325-011-0543-8
Hoffstein V (2007) Review of oral appliances for treatment of sleep-disordered breathing. Sleep Breath 11(1):1–22
Millman RP, Rosenberg CL, Carlisle CC, Kramer NR, Kahn DM, Bonitati AE (1998) The efficacy of oral appliances in the treatment of persistent sleep apnea after uvulopalatopharyngoplasty. Chest 113(4):992–996
Freedman N (2010) Treatment of obstructive sleep apnea syndrome. Clin Chest Med 31:187–201. https://doi.org/10.1016/j.ccm.2010.02.012
Holty J-E, Guilleminault C (2010) Surgical options for the treatment of obstructive sleep apnea. Med Clin N Am 94:479–515. https://doi.org/10.1016/j.mcna.2010.02.001
Prinsell JR (1999) Maxillomandibular advancement surgery in a site-specific treatment approach for obstructive sleep apnea in 50 consecutive patients. Chest 116(6):1519–1529
Baranwal N, Phoebe KY, Siegel NS (2023) Sleep physiology, pathophysiology, and sleep hygiene. Prog Cardiovasc Dis 77:59–69. https://doi.org/10.1016/j.pcad.2023.02.005
Shneerson J, Wright J (2001) Lifestyle modification for obstructive sleep apnea. Cochrane Database Syst Rev 1:CD002875. https://doi.org/10.1002/14651858.CD002875
Oksenberg A, Gadoth N, Töyräs J, Leppänen T (2020) Prevalence and characteristics of positional obstructive sleep apnea (POSA) in patients with severe OSA. Sleep Breath 24(2):551–559. https://doi.org/10.1007/s11325-019-01897-1
Smith PL, Gold AR, Meyers DA, Haponik EF, Bleecker ER (1985) Weight loss in mildly to moderately obese patients with obstructive sleep apnea. Ann Intern Med 103:850–855
Young T, Skatrud J, Peppard PE (2004) Risk factors for obstructive sleep apnea in adults. JAMA 291(16):2013–2016. https://doi.org/10.1001/jama.291.16.2013
Young T, Peppard PE, Gottlieb DJ (2002) Epidemiology of obstructive sleep apnea: a population health perspective. Am J Respir Crit Care Med 165(9):1217–1239. https://doi.org/10.1164/rccm.2109080
Issa FG, Sullivan CE (1982) Alcohol, snoring and sleep apnea. J Neurol Neurosurg Psychiatry 45:353–359
Series F, Roy N, Marc I (1994) Effects of sleep deprivation and sleep fragmentation on upper airway collapsibility in normal subjects. Am J Respir Crit Care Med 150:481–485
Brown FC, Buboltz WC Jr, Soper B (2002) Relationship of sleep hygiene awareness, sleep hygiene practices and sleep quality in university students. Behav Med 28(1):33–38. https://doi.org/10.1080/08964280209596396
Kitamura T, Miyazaki S, Koizumi H, Takeuchi S, Tabata T, Suzuki H (2016) Sleep hygiene education for patients with obstructive sleep apnea. Sleep Biol Rhythm 14:101–106
Victor LD (2004) Treatment of obstructive sleep apnea in primary care. Am Fam Physician 69(3):561–568
Peter HJ (1992) Sleep hygiene, relaxation therapy, and cognitive interventions. In: Hauri PJ (ed) Case studies in insomnia. Plenum, New York, NY, pp 65–84
Jackson M, Collins A, Berlowitz D, Howard M, O’Donoghue F, Barnes M (2015) Efficacy of sleep position modification to treat positional obstructive sleep apnea. Sleep Med 16:545–552. https://doi.org/10.1016/j.sleep.2015.01.008. (Elsivier)
A Review by, Veasey SC, Guilleminault C, Strohl KP et al (2006) Medical therapy for obstructive sleep apnea: a review by the medical therapy for obstructive sleep apnea task force of the standards of practice committee of the American Academy of Sleep Medicine. Sleep 29(8):1036–1044
Qureshi A, Lee-Chiong TL Jr (2005) Medical treatment of obstructive sleep apnea. Semin Respir Crit Care Med 26:1
American Academy of Sleep Medicine (2014) International classification of sleep disorders, 3a edn. American Academy of Sleep Medicine, Darien, IL
Sánchez AI, Martínez P, Miró E, Bardwell WA, Buela-Casal G (2009) CPAP and behavioral therapies in patients with obstructive sleep apnea: effects on daytime sleepiness, mood, and cognitive function. Sleep Med Rev 13(3):223-e 33. https://doi.org/10.1016/j.smrv.2008.07.002
Engleman HM, Martin SE, Deary IJ, Douglas NJ (1994) Effect of continuous positive airway pressure treatment on daytime function in sleep apnoea/hypopnoea syndrome. Lancet 343:572–575
Engleman HM, Martin SE, Kingshott RN, Mackay TW, Deary IJ, Douglas NJ (1998) Randomised placebo controlled trial of daytime function after continuous positive airway pressure (CPAP) therapy for the sleep apnoea/hypopnoea syndrome. Thorax 53:341–345
Lojander J, Maasilta P, Partinen M, Brander PE, Salmi T, Lehtonen H (1996) Nasal- CPAP, surgery, and conservative management for treatment of obstructive sleep apnea syndrome A randomized study. Chest 110:114–119
Zhao YY, Wang R, Gleason KJ, Lewis EF, Quan SF, Toth CM, Morrical M, Rueschman M, Weng J, Ware JH, Mittleman MA (2017) Effect of continuous positive airway pressure treatment on health-related quality of life and sleepiness in high cardiovascular risk individuals with sleep apnea: Best Apnea Interventions for Research (BestAIR) Trial. Sleep 40(4):zsx040. https://doi.org/10.1093/sleep/zsx040
Barbé F, Durán-Cantolla J, Capote F et al (2010) Long-term effect of continuous positive airway pressure in hypertensive patients with sleep apnea. Am J Respir Crit Care Med 181:718–726. https://doi.org/10.1164/rccm.200901-0050OC
Giles TL, Lasserson TJ, Smith BJ, White J, Wright J, Cates CJ (1998) Continuous positive airways pressure for obstructive sleep apnoea in adults. Cochrane Database Syst Rev 2:CD001106. https://doi.org/10.1002/14651858.CD001106
Redline S, Adams N, Strauss ME, Roebuck T, Winters M, Rosenberg C (1998) Improvement of mild sleep-disordered breathing with CPAP compared with conservative therapy. AM J Respir Crit Care Med 157:858–865
Monasterio C, Vidal S, Duran J et al (2001) Effectiveness of continuous positive airway pressure in mild sleep apnea–hypopnea syndrome. Am J Respir Crit Care Med 164:939–943
Lee S-A, Paek J-H, Han S-H (2015) Sleep hygiene and its association with daytime sleepiness, depressive symptoms, and quality of life in patients with mild obstructive sleep apnea. J Neurol Sci 359:445–449. https://doi.org/10.1016/j.jns.2015.10.017
Jung SY, Kim H, Min JY, Hwang KJ, Kim SW (2019) Sleep hygiene-related conditions in patients with mild to moderate obstructive sleep apnea. Auris Nasus Larynx 46:95–100. https://doi.org/10.1016/j.anl.2018.06.003. (Elsivier)
Wimms AJ, Kelly JL, Turnbull CD et al (2019) Continuous positive airway pressure versus standard care for the treatment of people with mild obstructive sleep apnoea (MERGE): a multicentre, randomised controlled trial. Lancet Respir Med. https://doi.org/10.1016/S2213-2600(19)30402-3
Lam B, Sam K, Mok WY, Cheung MT, Fong DY, Lam JC, Lam DC, Yam LY, Mary SM (2007) Randomised study of three non-surgical treatments in mild to moderate obstructive sleep apnea. Thorax 62:354–359. https://doi.org/10.1136/thx.2006.063644
Ballester E, Badia JR, Hernández L, Carrasco E, de Pablo J (1999) Consol Fornas, Robert Rodriguez-Roisin, and Josep M. Montserrat. Evidence of the effectiveness of continuous positive airway pressure in the treatment of sleep apnea/hypopnea syndrome. Am J Respir Crit Care Med 159:495–501
Torres-Castro R, Vilaró J, Martí JD et al (2019) Effects of a combined community exercise program in obstructive sleep apnea syndrome: a randomized clinical trial. J Clin Med 8:361. https://doi.org/10.3390/jcm8030361
Iftikhar IH, Kline CE, Youngstedt SD (2014) Effects of exercise training on sleep apnea: a meta-analysis. Lung 192:175–184
Mendelson M, Bailly S, Marillier M, Flore P, Borel JC et al (2018) Obstructive sleep apnea syndrome, objectively measured physical activity and exercise training interventions: a systematic review and meta-analysis. Front Neurol 9:73. https://doi.org/10.3389/fneur.2018.00073
Cipriano LHC, Borges YG, Mill JG, Mauad H, Martins de Araujo MT, Gouvea SA (2021) Effects of short-term aerobic training versus CPAP therapy on heart rate variability in moderate to severe OSA patients. Soc Psychophysiological Res Psychophysiol 58:e13771. https://doi.org/10.1111/psyp.13771
Young T, Peppard PE, Taheri S (1985) Excess weight and sleep-disordered breathing. J Appl Physiol 99(4):1592–9. https://doi.org/10.1152/japplphysiol.00587.2005
Carneiro-Barrera A, Amaro-Gahete FJ, Guillén-Riquelme A, Jurado-Fasoli L, Sáez-Roca G, Martín-Carrasco C, Buela-Casal G, Ruiz JR (2022) Effect of an interdisciplinary weight loss and lifestyle intervention on obstructive sleep apnea severity: the INTERAPNEA randomized clinical trial. JAMA Netw Open 5(4):e228212. https://doi.org/10.1001/jamanetworkopen.2022.8212
Gambino F, Zammuto MM, Virzì A, Conti G, Bonsignore MR (2022) Treatment options in obstructive sleep apnea. Intern Emerg Med 17(4):971–978. https://doi.org/10.1007/s11739-022-02983-1
Benoist L, de Ruiter M, de Lange J, de Vries N (2017) A randomized, controlled trial of positional therapy versus oral appliance therapy for position-dependent sleep apnea. Sleep Med 34:109–117. https://doi.org/10.1016/j.sleep.2017.01.024
Kribbs NB, Pack AI, Kline LR et al (1993) Objective measurement of patterns of nasal CPAP use by patients with obstructive sleep apnea. Am Rev Respir Dis 147:887–895
Pepin JL, Krieger J, Rodenstein D et al (1999) Effective compliance during the first 3 months of continuous positive airway pressure. A European prospective study of 121 patients. Am J Respir Crit Care Med 160:1124–9
Engleman HM, Wild MR (2003) Improving CPAP use by patients with the sleep apnoea/hypopnoea syndrome (SAHS). Sleep Med Rev 7:81–99
Yingjuan M, Siang WH, Leong Alvin TK, Poh HP (2020Jun) Positional therapy for positional obstructive sleep apnea. Sleep Med Clin 15(2):261–275. https://doi.org/10.1016/j.jsmc.2020.02.012
Dalmases M, Solé-Padullés C, Torres M et al (2015) Effect of CPAP on cognition, brain function, and structure among elderly patients with OSA - a randomized pilot study. Chest 148(5):1214–1223 (ClinicalTrials.gov; No.: NCT01826032)
Daurat A, Huet N, Tiberge M (2010) Metamemory beliefs and episodic memory in obstructive sleep apnea syndrome. Psychol Rep 107:289–302
Bédard M, Montplaisir J, Richer F, Rouleau I, Malo J (1991) Obstructive sleep apnea syndrome: pathogenesis of neuropsychological deficits. J Clin Exp Neuropsychol 13:950–964
Chen CW, Yang CM, Chen NH (2012) Objective versus subjective cognitive functioning in patients with obstructive sleep apnea. Open Sleep J 5:33–42
Salorio CF, White DA, Piccirillo J, Duntley SP, Uhles ML (2002) Learning, memory, and executive control in individuals with obstructive sleep apnea syndrome. J Clin Exp Neuropsychol 24(1):93–100. https://doi.org/10.1076/jcen.24.1.93.973
Kielb SA, Ancoli-Israel S, Rebok GW, Spira AP (2012) Cognition in obstructive sleep apnea-hypopnea syndrome (OSAS): current clinical knowledge and the impact of treatment. Neuromol Med 4(3). https://doi.org/10.1007/s12017-012-8182-1
Alvarez JA, Emory E (2006) Executive function and the frontal lobes: a meta-analytic review. Neuropsychol Rev 16:17–42
Saunamäki T, Himanen SL, Polo O, Jehkonen M (2009) Executive dysfunction in patients with obstructive sleep apnea syndrome. Eur Neurol 62:237–242
Vaessen Tim JÁ, Overeem S, Sitskoorn MM (2015) Cognitive complaints in obstructive sleep apnea. Sleep Med Rev 19:51–58. https://doi.org/10.1016/j.smrv.2014.03.008
Barnes M, Houston D, Worsnop J et al (2002) A randomised controlled trial of continuous positive airway pressure in mild obstructive sleep apnea. Am J Respir Crit Care Med 165(773–80):39
Barnes M, McEvoy RD, Banks S, Tarquinio N, Murray CG, Vowles N et al (2004) Efficacy of positive airway pressure and oral appliance in mild to moderate obstructive sleep apnea. Am J Respir Crit Care Med 170:656–664
Doherty LS, Kiely JL, Lawless G, McNicholas WT (2003) Impact of nasal continuous positive airway pressure therapy on the quality of life of bed partners of patients with obstructive sleep apnea syndrome. Chest 124(2209–14):63
Akashiba T, Kawahara S, Akahoshi T et al (2002) Relationship between quality of life and mood or depression in patients with severe obstructive sleep apnea syndrome. Chest 122:861–865
Borak J, Cieslicki JK, Koziej M, Matuszewski A, Zielinski J (1996) Effects of CPAP treatment on psychological status in patients with severe obstructive sleep apnoea. J Sleep Res 5(123–7):22
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Ethical approval
For this type of study, formal consent is not required.
Conflict of interest
The authors declare no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Costa, I.O.M., Cunha, M.O., Bussi, M.T. et al. Impacts of conservative treatment on the clinical manifestations of obstructive sleep apnea—systematic review and meta-analysis. Sleep Breath 28, 1563–1574 (2024). https://doi.org/10.1007/s11325-024-03034-z
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11325-024-03034-z