
Abstract
Background
Obstructive sleep apnea (OSA) has been demonstrated to be associated with an increase of oxidative stress. However, whether circulating malondialdehyde (MDA), a widely used biomarker of oxidative stress, could be reduced by the treatment of OSA by continuous positive airway pressure (CPAP) is debated. The present meta-analysis was performed to determine the effect of CPAP treatment on circulating MDA among patients with OSA.
Methods
A systematic search of PubMed, Embase, and Web of Science was performed for literature covering the period between 1967 and August 2019. Standardized mean difference (SMD) was calculated to estimate the treatment effects of pre- and post-CPAP therapy.
Results
A total of 10 studies with 220 patients were included in this meta-analysis. A significant decrease in circulating MDA was observed after CPAP treatment (SMD = 1.164, 95% CI = 0.443 to 1.885, z = 3.16, p = 0.002) in OSA patients. Subgroup analyses revealed that CPAP therapy was associated with a significant decrease of circulating MDA in elder (SMD = 1.629, 95% CI = 0.265 to 2.994, z = 2.34, p = 0.019), more obese patients (SMD = 0.954, 95% CI = 0.435 to 1.473, z = 3.61, p = 0.000), more severe OSA patients (SMD = 0.879, 95% CI = 0.421 to 1.336, z = 3.76, p = 0.000), patients with therapeutic duration ≥ 3 months (SMD = 1.867, 95% CI = 0.563 to 3.172, z = 2.80, p = 0.005), and patients with good compliance (SMD = 1.004, 95% CI = 0.703 to 1.305, z = 6.54, p = 0.000).
Conclusions
This meta-analysis suggested that CPAP therapy exerted significant lowering effects on circulating MDA, especially in elder, more obese, and more severe OSA patients and patients with good compliance as well as longer duration of CPAP application.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Obstructive sleep apnea (OSA) is the most common form of breathing-related sleep disorder, which is characterized by recurrent episodes of partial or complete upper airway obstruction during sleep leading to chronic intermittent hypoxia (CIH). Accumulating evidence reveals that OSA is a significant risk factor for adverse health outcomes including hypertension, cardiovascular disease, metabolic disorders, cognitive impairment, and reduced quality of life. It is suggested that these comorbidities associated with OSA are largely mediated through oxidative stress [1].
It is well documented that OSA-related multiple cycles of hypoxia/reoxygenation result in the formation of reactive oxygen species and induce oxidative stress, which is known to be mechanistic facilitators of cardiovascular diseases and other disorders [2]. Lipid peroxidation represents a direct consequence of oxidative stress and the main cause of oxidative damage [3]. Among the aldehydes produced by lipid peroxidation, malondialdehyde (MDA) and 4-hydroxynonenal (HNE) have received the most attention. MDA is formed by the polyunsaturated fatty acids in the biofilm, which initiate lipid peroxidation after being attacked by oxygen free radicals. It has been demonstrated that MDA is the most abundant aldehyde generated during lipid peroxidation, where 4-HNE generation only amounts to 10% that of MDA [4]. Since MDA is produced at high levels during lipid peroxidation, it is commonly used as a measure of oxidative stress [5]. MDA has been extensively studied in biological and medical sciences due to its reactivity with biological molecules and connection to various diseases [6]. Previous studies have investigated the systemic oxidative stress status in OSA patients by the use of circulating MDA [7, 8].
Continuous positive airway pressure (CPAP), as the golden standard in current management of OSA patients, has been demonstrated to result in significant clinical benefits [9]. However, the impact of CPAP therapy on oxidative stress biomarker, namely MDA, remains unclear. To our knowledge, no meta-analysis has determined the effect of CPAP treatment on serum/plasma MDA levels among OSA patients. Therefore, in the present meta-analysis, we quantitatively evaluated the effect of CPAP therapy on circulating MDA among OSA patients.
Material and methods
This meta-analysis was reported in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-analysis (PRISMA) Statement for the conduct of meta-analyses of intervention studies [10].
Search strategy
A computerized search was carried out on the following databases covering the period between 1967 and August 2019: Web of Science, PubMed, and Embase. We used the following search terms; “sleep disordered breathing or sleep apnea” and “CPAP or continuous positive airway pressure”, in combination with “malondialdehyde or MDA”. Furthermore, we searched the reference lists of review articles and selected articles.
Study selection
Studies were considered eligible for inclusion if they fulfilled the predetermined criteria: (1) subjects were adults (age ≥ 18 years) with newly diagnosed OSA; (2) the intervention was an application of CPAP; (3) the value of serum or plasma MDA needed to be reported pre- and post-CPAP therapy; (4) the study provided sufficient data for analysis including continuous data reported as means with standard deviations/standard errors, or median and interquartile range and sample size. Two investigators identified eligible studies independently. If there was any disagreement, it was resolved by consensus with a third investigator.
Editorials, letters, case reports, reviews, and abstracts without original data were excluded. Animal studies were also excluded. Studies were deemed ineligible if it(1) is a non-English article and (2) has assessment of MDA in low-density lipoprotein (LDL) or erythrocytes. The study with the largest population was included if multiple studies reported outcomes on the same patient group.
Data extraction
Two of the authors extracted data from eligible studies using a standardized form independently. The following information was extracted from each paper: first author, publication year, place of the study, total sample size, sex distribution, inclusion criteria, therapy duration, mean daily CPAP usage time, CPAP average weekly use, patients’ characteristics, study design, pre-CPAP MDA concentrations, and post-CPAP MDA concentrations.
Statistical analysis
We performed statistical analyses with Stata software (v12.0; Stata Corp, College Station, TX, USA). Medians and interquartile ranges were converted to means and standard deviations according to Wan et al. [11]. Standardized mean difference (SMD) was used to generate forest plots of continuous data and to evaluate differences in MDA levels before and after CPAP therapy. The statistical significance of SMD was analyzed by the z test, and p < 0.05 was deemed statistically significant. Q statistic was used to test the heterogeneity of SMD across studies (significance level at p < 0.10). The I2 statistic was also calculated to measure inconsistency across studies quantitatively. Statistical heterogeneity was defined as an I2 statistic value ≥ 50%. If significant heterogeneity was observed, we used a random effect model, otherwise we used a fixed-effect model. We conducted sensitive and subgroup analyses to explore the possible sources of heterogeneity in treatment effect. Begg’s correlation and Egger’s regression were used for assessing publication bias. All statistical tests were two-sided.
Results
Literature search
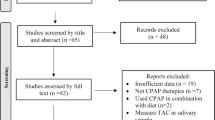
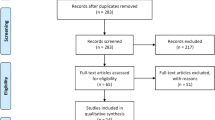
A total of 38 initially identified studies were excluded after the first screening because of duplicates. The majority of the remaining studies were also excluded, mainly because they were either in abstract or letter format, review, irrelevant, not in English, or animal studies. A flow chart showing the study selection was showed in Fig. 1.

Flow diagram of study selection. MDA, malondialdehyde; LDL, low-density lipoprotein
Characteristics of the studies
A total of 10 studies (11 cohorts) were found eligible for inclusion for meta-analysis based on the set criteria. These studies involved 220 subjects. Of them, 2 were randomized clinical trials (RCTs) [12, 13] and 8 were observational studies [14,15,16,17,18,19,20,21]. One study reported results separately for good (≥ 4 h/night) compliance group and poor (< 4 h/night) compliance group [14]. Table 1 summarized the characteristics of the 10 included studies and the patients’ characteristics.
Pool analysis
Substantial heterogeneity between studies was detected (I2 = 91.0%, p = 0.000). Thus, a random effect model was used for the pooled analysis. Overall, pooled results showed that a significant decrease in serum or plasma MDA was observed after CPAP treatment (SMD = 1.164, 95% CI = 0.443 to 1.885, z = 3.16, p = 0.002). The forest plot for MDA concentrations in OSA patients between pre-CPAP treatment and post-CPAP treatment was shown in Fig. 2.

Forest plot for the change in circulating MDA before and after CPAP treatment. MDA, malondialdehyde; CPAP, continuous positive airway pressure; SMD, standardized mean difference; CI, confidence interval
Sensitivity and subgroup analyses
Sensitivity analyses were performed in order to explore the possible sources of heterogeneity. The results showed that no individual studies significantly affected the pooled results, indicating a statistically robust result (Fig. 3). Subgroup analyses revealed that CPAP therapy resulted in a significant decrease of circulating MDA in elder (≥ 50 years) (SMD = 1.629, 95% CI = 0.265 to 2.994, z = 2.34, p = 0.019), more obese patients(BMI ≥ 30)(SMD = 0.954, 95% CI = 0.435 to 1.473, z = 3.61, p = 0.000), more severe OSA patients (AHI ≥ 50 events/h) (SMD = 0.879, 95% CI = 0.421 to 1.336, z = 3.76, p = 0.000), patients with therapeutic duration ≥ 3 months (SMD = 1.867, 95% CI = 0.563 to 3.172, z = 2.80, p = 0.005), and patients with good compliance (≥ 4 h/night) (SMD = 1.004, 95% CI = 0.703 to 1.305, z = 6.54, p = 0.000). However, CPAP has no effect on circulating MDA in OSA patients with age < 50 years, BMI < 30, AHI < 50, follow time < 3 months, and poor compliance(< 4 h/night). The differences in sample size and racial differences did not influence CPAP efficacy. Table 2 showed the detailed results of the subgroup analyses.

Sensitivity analysis of the included studies. CI, confidence interval
Publication bias
No statistical significance of publication bias was indicated by the results of Begg’s tests (z = 0.93, p = 0.350) and Egger’s tests (t = 1.88, p = 0.093) in the present meta-analysis (Fig. 4). Furthermore, trim-and-fill method suggested that no study needed to be statistically corrected for funnel plot asymmetry.

Funnel plots for assessing publication bias of studies included. SE, standard error; SMD = standardized mean difference
Discussion
The present meta-analysis aimed to assess the effects of CPAP therapy on circulating MDA among OSA patients. We chose this marker because it is a widely studied oxidative stress biomarker and may closely link OSA with various complications. The findings of the study demonstrated that CPAP treatment might be effective in decreasing circulating MDA in patients with OSA. Furthermore, subgroup analyses revealed that CPAP was more effective in decreasing circulating MDA in OSA patients in elder, more obese, and more severe OSA patients, and patients with good compliance as well as therapeutic period ≥ 3 months.
MDA, an important endogenous product of lipid peroxidation, was shown to be elevated in OSA patients in previous studies. Jordan et al. [7] reported that the plasma MDA was positively associated with the duration of sleeping time less than 85% and 90% O2 saturations. Another study found that MDA levels were higher in the moderate and severe OSA group than the healthy subjects after comparing 25 OSA patients with 24 healthy male subjects [8]. A recent study also found that the mean MDA concentrations in patients with higher AHI values were also higher than those in patients with lower AHI. Higher predominance of apnea in patients with similar AHI values, longer mean apnea durations, O2 saturation dips to < 90%, and higher ODI values predicted higher plasma MDA concentrations [22]. This has been further supported by animal experiments. An animal study showed that mice were subjected to CIH or intermittent air (IA) for 12 h a day and fed either a high-fat (HF) or a control diet (CD) for 6 weeks. MDA levels were significantly higher in the CDIH group than that in the CDIA group; the increase in MDA levels was more pronounced in the HFIH group [23]. Oxidative stress and systemic inflammation are found to be fundamental mechanisms in the pathophysiology of atherosclerosis and cardiovascular morbidity and other disorders in OSA. Moreover, higher MDA levels in ischemic stroke patients were suggested to be associated with poor functional outcome and early mortality [24, 25]. However, the effect of CPAP on circulating MDA among OSA patients remains unclear.
It is widely accepted that CPAP therapy could eliminate respiratory disturbances, reduce the AHI, and reverse IH. The formation of reactive oxygen species and oxidative stress is caused by OSA-related multiple cycles of hypoxia/reoxygenation. Thus, it is reasonable to speculate that CPAP therapy could decrease circulating MDA in OSA patients. This was further confirmed by the results of the present meta-analysis. Further subgroup analyses suggested that CPAP was more effective in elder, more severe OSA, more obese patients, patients with therapeutic period ≥3 months, and patients with good compliance. While this positive result was not observed in patients with age < 50 years, BMI < 30, AHI < 50, follow time < 3 months, or poor compliance. The results indicated that the efficacy of CPAP therapy was influenced by the baseline condition of patients, CPAP therapy duration, and therapy compliance. Our previous studies also supported this conclusion [26, 27]. This result allows us to predict responses to CPAP treatments and choose the patients with specific OSA phenotypes who can benefit more from CPAP therapy to initiate CPAP therapy. It is valuable to perform precision treatment on patients with OSA, and more research and data are needed to deepen our understandings of the disease and possible new methods of precision treatment.
In the present meta-analysis, the cutoff value for AHI in the subgroup analysis was set as 50. The mean AHI value of most included studies was higher than 30, so it is unsuitable to choose 30, a cutoff value currently used to define severe OSA. The evidence from previous meta-analysis demonstrated that the effect of CPAP therapy was influenced by baseline severity of OSA grouped by AHI ≤ 50 and > 50 [28]. Based on the above two reasons, we set the cutoff value for AHI in the subgroup analysis as 50. Some studies used 35 as the cutoff value for BMI in the subgroup analysis when evaluating the effect of CPAP therapy [29], while several studies used 30 as the cutoff value [28]. Considering the majority of population in our study was Asian, who seemed to be less obese, hence, we chose 30 as the cutoff value for BMI in subgroup analysis.
To the best of our knowledge, this was the first meta-analysis to access the impact of OSA treatment with CPAP therapy on circulating MDA among OSA patients. However, a few caveats are needed to be noted when interpreting the findings from present meta-analysis. First, significant heterogeneity was observed in our meta-analysis, but no consistent determinant was identified. Second, the sample size of the included study was relatively small. Third, the proportion of male patients of the present meta-analysis was significantly high; therefore, it should be cautious to interpret the results when it is generalizable to female patients. Fourth, most of the included studies were observational rather than RCTs. Fifth, most of the studies used TBARS (thiobarbituric acid reactive substances) to measure MDA; however, HPLC, LC-MS/MS, and GC-MS methods have been shown to be specific and more sensitive than the batch TBARS assays. In addition, AASM criteria for apnea and/or hypopnea have changed during the last two decades. The included studies using different published standard definitions led to differences in AHI. This may have implications for disease identification, severity grading. Finally, only English language studies were included, which may cause some publication biases.
Conclusions
This meta-analysis suggested that in OSA patients, CPAP therapy exerted significant lowering effects on circulating MDA, especially in elder, more obese, and more severe OSA patients, patients with good compliance as well as longer duration of CPAP application. Thus, it could be speculated that CPAP treatment could improve systemic oxidative stress status in OSA patients, which may be one mechanism by which CPAP treatment exerts significant clinical benefits. Furthermore, the circulating MDA might be considered a useful tool in assessing the efficacy of CPAP treatment in reducing OSA-related complication risk in patients.
References
Lavie L (2009) Oxidative stress--a unifying paradigm in obstructive sleep apnea and comorbidities. Prog Cardiovasc Dis 51:303–312
Lavie L (2003) Obstructive sleep apnoea syndrome--an oxidative stress disorder. Sleep Med Rev 7:35–51
Niki E (2009) Lipid peroxidation: physiological levels and dual biological effects. Free Radic Biol Med 47:469–484
Esterbauer H, Zollner H (1989) Methods for determination of aldehydic lipid peroxidation products. Free Radic Biol Med 7:197–203
Ayala A, Munoz MF, Arguelles S (2014) Lipid peroxidation: production, metabolism, and signaling mechanisms of malondialdehyde and 4-hydroxy-2-nonenal. Oxidative Med Cell Longev 2014:360438
Janero DR (1990) Malondialdehyde and thiobarbituric acid-reactivity as diagnostic indices of lipid peroxidation and peroxidative tissue injury. Free Radic Biol Med 9:515–540
Jordan W, Cohrs S, Degner D, Meier A, Rodenbeck A, Mayer G, Pilz J, Ruther E, Kornhuber J, Bleich S (2006) Evaluation of oxidative stress measurements in obstructive sleep apnea syndrome. J Neural Transm 113:239–254
Vatansever E, Surmen-Gur E, Ursavas A, Karadag M (2011) Obstructive sleep apnea causes oxidative damage to plasma lipids and proteins and decreases adiponectin levels. Sleep Breath 15:275–282
Cao MT, Sternbach JM, Guilleminault C (2017) Continuous positive airway pressure therapy in obstuctive sleep apnea: benefits and alternatives. Expert Rev Respir Med 11:259–272
Moher D, Liberati A, Tetzlaff J, Altman DG (2009) Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med 6:e1000097
Wan X, Wang W, Liu J, Tong T (2014) Estimating the sample mean and standard deviation from the sample size, median, range and/or interquartile range. BMC Med Res Methodol 14:135
Dal-Fabbro C, Garbuio S, D'Almeida V, Cintra FD, Tufik S, Bittencourt L (2014) Mandibular advancement device and CPAP upon cardiovascular parameters in OSA. Sleep Breath 18:749–759
Wu K, Su X, Li G, Zhang N (2016) Antioxidant carbocysteine treatment in obstructive sleep apnea syndrome: a randomized clinical trial. PLoS One 11:e0148519
Dorkova Z, Petrasova D, Molcanyiova A, Popovnakova M, Tkacova R (2008) Effects of continuous positive airway pressure on cardiovascular risk profile in patients with severe obstructive sleep apnea and metabolic syndrome. Chest 134:686–692
Ye LA, Ma GH, Chen L, Li M, Liu JL, Yang K, Li QY, Li N, Wan HY (2010) Quantification of circulating cell-free DNA in the serum of patients with obstructive sleep apnea-hypopnea syndrome. Lung 188:469–474
Jurado-Gamez B, Fernandez-Marin MC, Gomez-Chaparro JL, Munoz-Cabrera L, Lopez-Barea J, Perez-Jimenez F, Lopez-Miranda J (2011) Relationship of oxidative stress and endothelial dysfunction in sleep apnoea. Eur Respir J 37:873–879
Alzoghaibi MA, Bahammam AS (2012) The effect of one night of continuous positive airway pressure therapy on oxidative stress and antioxidant defense in hypertensive patients with severe obstructive sleep apnea. Sleep Breath 16:499–504
Yagihara F, Lucchesi LM, D'Almeida V, de Mello MT, Tufik S, Bittencourt LRA (2012) Oxidative stress and quality of life in elderly patients with obstructive sleep apnea syndrome: are there differences after six months of continuous positive airway pressure treatment? Clinics 67:565–571
Tichanon P, Wilaiwan K, Sopida S, Orapin P, Watchara B, Banjamas I (2016) Effect of continuous positive airway pressure on airway inflammation and oxidative stress in patients with obstructive sleep apnea. Can Respir J 2016:3107324
Wang XT, Zhao G, Tu L, Yue ZY, Liu ZH, Han J, Gao K, Zhou XC, Xu S, Li JF (2019) Continuous positive airway pressure effectively alleviates arrhythmias in patients with obstructive sleep apnea: possible relationship with counteracting oxidative stress. Curr Med Sci 39:52–58
Lavie L, Vishnevsky A, Lavie P (2004) Evidence for lipid peroxidation in obstructive sleep apnea. Sleep 27:123–128
Savas O, Suslu AE, Lay I, Ozer S (2019) Assessment of the relationship between polysomnography parameters and plasma malondialdehyde levels in patients with obstructive sleep apnea. Eur Arch Otorhinolaryngol 276:3533–3538
Badran M, Golbidi S, Devlin A, Ayas N, Laher I (2014) Chronic intermittent hypoxia causes endothelial dysfunction in a mouse model of diet-induced obesity. Sleep Med 15:596–602
Lorente L, Martin MM, Abreu-Gonzalez P, Ramos L, Argueso M, Sole-Violan J, Riano-Ruiz M, Jimenez A (2015) Serum malondialdehyde levels in patients with malignant middle cerebral artery infarction are associated with mortality. PLoS One 10:e0125893
Polidori MC, Cherubini A, Stahl W, Senin U, Sies H, Mecocci P (2002) Plasma carotenoid and malondialdehyde levels in ischemic stroke patients: relationship to early outcome. Free Radic Res 36:265–268
Chen LD, Lin L, Ou YW, Wu Z, Cai ZM, Wang TZ, Liu JN (2017) Effect of positive airway pressure on glomerular filtration rate in patients with sleep-disordered breathing: a meta-analysis. Sleep Breath 21:53–59
Chen LD, Lin L, Zhang LJ, Zeng HX, Wu QY, Hu MF, Xie JJ, Liu JN (2018) Effect of continuous positive airway pressure on liver enzymes in obstructive sleep apnea: a meta-analysis. Clin Respir J 12:373–381
Chen X, Niu X, Xiao Y, Dong J, Zhang R, Lu M, Kong W (2014) Effect of continuous positive airway pressure on homocysteine levels in patients with obstructive sleep apnea: a meta-analysis. Sleep Breath 18:687–694
Guo Y, Pan L, Ren D, Xie X (2013) Impact of continuous positive airway pressure on C-reactive protein in patients with obstructive sleep apnea: a meta-analysis. Sleep Breath 17:495–503
Funding
This work was supported by the National Natural Science Foundation of China (81870074 and 81900088) and Startup Fund for scientific research from Fujian Medical University (2017XQ1117).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflicts of interest.
Ethics approval and consent to participate
All analyses were based on previous published studies, thus no ethical approval and patient consent are required.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Chen, Q., Chen, LD., Chen, MX. et al. The effect of continuous positive airway pressure on circulating malondialdehyde among obstructive sleep apnea patients: a meta-analysis. Sleep Breath 24, 1407–1415 (2020). https://doi.org/10.1007/s11325-019-01998-x
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11325-019-01998-x