
Abstract
Background
Hypoxia induces vascular endothelial injuries; however, the mechanisms involved and effects of interventions remain unclear.
Objective
Investigate the inflammatory response and oxidative stress in co-cultured neutrophils and vascular endothelial cells, apoptotic changes in endothelial cells, and effects of the antioxidant, Tempol, or the NF-êB inflammatory channel blocker, pyrrolidine dithiocarbamate (PDTC), upon endothelial cells under conditions of intermittent and/or continuous hypoxic exposure.
Methods
Polymorphonuclear neutrophils co-cultured with human umbilical vein endothelial cells were subjected to the following conditions: intermittent normoxia (IN), intermittent hypoxia (IH), continuous hypoxia (CH), intermittent with continuous hypoxia (OS), OS+Tempol (OS+T), or OS+PDTC (OS+P) for 2, 5, or 8 h. Inflammatory factors, TNF-α and IL-6, the adhesion molecule, ICAM-1, CAT activity, and MDA concentrations in supernatants from the co-culture as well as pro- (Bak) and anti- (Bcl-xl) apoptotic gene expression levels in the endothelial cells were determined.
Results
Inflammatory factors, adhesion molecules, oxidative stress, and apoptosis genes in all groups showed significant, time-dependent increases as compared with the IN group. TNF-α, IL-6, ICAM-1, and MDA levels in the OS group were increased, while CAT was decreased as compared with that observed in the IH, CH, OS+T, and OS+P groups. Bcl-x1 expression and Bcl-x1/BAK ratios were decreased and BAX increased in the OS versus IH, CH, OS+T, or OS+P groups. Both pro- and anti-apoptotic proteins showed time-dependent increases, while the Bcl-x1/BAK ratio decreased over these times. Tempol and PDTC partially prevented these effects.
Conclusion
Inflammation, oxidative stress, and apoptosis are all involved in vascular endothelial injury induced by OS. Anti-inflammatory and anti-oxidative interventions can partially improve effects of OS.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Obstructive sleep apnea (OSA) and chronic obstructive pulmonary disease (COPD) are the two most common chronic respiratory diseases, and their coexistence is referred to as respiratory overlap syndrome [1]. While it is known that vascular endothelial injuries are present in COPD and OSA patients, endothelial dysfunction is more serious in overlap syndrome patients and is related to the severity of the disease [2]. It has been reported that patients with overlap syndrome have higher rates of cardiovascular events and mortality compared with patients with COPD or OSA alone [3, 4]. The incidence of overlap syndrome is about 1% in people over 40 years of age [5]. With such a high incidence involving a large patient population, it is critical to conduct more in-depth and comprehensive investigations on the mechanisms of this condition. Studies on overlap syndrome have mainly focused on the clinical and epidemiological aspects, with few directed at examining the pathological mechanisms, especially at the cellular level. The goals of this study were to investigate (1) the interactions between neutrophils and vascular endothelial cells under conditions of intermittent and/or continuous hypoxic exposure, (2) the underlying mechanisms as related with abnormal apoptosis of endothelial cells, and (3) the potential intervention strategies for the treatment of overlap syndrome. The findings from this study provide important new theoretical and experimental evidence for understanding the pathogenesis and potential for development of intervention strategies for overlap syndrome patients complicated with cardiovascular disease.
Vascular endothelial cells play an important role in ensuring a normal function of blood vessels. Under normal conditions, endothelial cells are in an inactive state, which enables them to resist the aggregation and adhesion of circulating blood cells. In this inactive state, the expression of adhesion molecules within neutrophils and endothelial cells remains at basal levels. However, hypoxia can produce a dysfunction of vascular endothelial cells, which can further exacerbate cardiovascular and cerebrovascular diseases and systemic damage [6]. Cell interactions play an important role in this process of vascular endothelial cell injury, especially with regard to the interaction among the inflammatory cells, polymorphonuclear neutrophils (PMN), and vascular endothelial cells, which represent key components of endothelial cell injury. For example, Kent et al. [7] reported that intermittent hypoxia activates PMN, which increases reactive oxygen species (ROS) production and enhances the adhesion of PMN to vascular endothelial cells. Intermittent hypoxia also activates endothelial cells and promotes the activation of inflammatory pathways of pro-inflammatory factors, inflammatory chemokines, and adhesion molecules, which further promotes PMN adherence to endothelial cells. In addition, PMN releases inflammatory cytokines, proteolytic enzymes, and leukotrienes, and increases ROS production within vascular endothelial cells, thus accelerating cell injury and apoptosis. Hypoxia also increases the expression of ICAM-1, which mediates the migration of PMN to endothelial cells, thus inhibiting PMN apoptosis [8]. Therefore, it is believed that the longer PMN remains active at the site of inflammation, the greater the number of harmful substances that can be produced, which then enhances the inflammatory response and damage to vascular endothelial cells. Endothelial cell damage may also result from multiple factors like an unbalanced oxidation/antioxidation state and contact/adherence of inflammatory factor-induced endothelial cell damage to endothelial cells as well as the activation of various transcription factors.
We hypothesized that interactive effects may exist between PMN and vascular endothelial cells under conditions of hypoxia to produce endothelial cell damage resulting from mechanisms involving inflammation and oxidative stress. As overlap syndrome involves both intermittent and persistent hypoxia, it seems likely that endothelial cell injury would be worse under hypoxia mode conditions consisting of an intermittent+continuous exposure to hypoxia. To test this hypothesis, in the current study, we assessed responses of inflammatory factors and oxidative stress, as well as expression levels of apoptosis-related proteins, under different conditions of hypoxia in co-cultured endothelial cells and neutrophils. In addition, to investigate whether anti-inflammatory and antioxidant agents can delay the apoptosis in endothelial cells and protect vascular endothelium cells, we tested the effects of anti-oxidation and anti-inflammatory interventions, as achieved by treating these co-cultures with the antioxidant, Tempol (4-hydroxy-2,2,6,6-tetramethylpiperidine), or NF-κB inflammatory channel blocker, pyrrolidine dithiocarbamate (PDTC). Results from this study provide some new and important information on the mechanisms of pathogenesis and potential interventions for overlap syndrome patients complicated with cardiovascular disease.
Materials and methods
Cell preparation
Extraction of PMN
Healthy adult volunteers, who were seen for a physical examination at the Tianjin Third Central Hospital - Branch Hospital, were recruited for this study. Informed consents were obtained from all healthy volunteers. The following conditions were criteria for exclusion from this study: (1) previous history of respiratory, cardiovascular, or nervous system diseases, or any organic diseases such as liver or kidney disease; (2) patients with the potential for COPD as determined through reviewing their medical history, physical examination results, chest X-ray, and pulmonary function tests; and (3) self-reported history of sleep snoring, apnea, or sleepiness during the daytime. A peripheral venous blood sample (40 ml) was drawn from the volunteers after they had fasted for at least 8 h. A two-layer Ficoll-Histopaque density gradient centrifugation (Histopaque 1.077 and 1.119, Sigma-Aldrich) was used to separate PMN from blood samples. The PMN purity was greater than 96%, and the survival rate, as determined by trypan blue staining, was greater than 99%. PMN cells were resuspended in RPMI-1640 medium for further experimentation.
Preparation of human vascular endothelial cells
In this study, a human umbilical vein endothelial cell line EA.hy926 was produced by hybridizing human umbilical vein endothelial cells (HUVEC) with the epithelial cell line a549. The cryopreserved human umbilical vein endothelial cells were first resuscitated in a water bath followed by placement in a flask containing RPMI-1640 medium (Gibco, USA) with 10% fetal bovine serum (FCS), 100 U/mL penicillin, and 100 μg/mL streptomycin. Cells were cultured in a 5% CO2 and 37 °C incubator with saturated humidity. After two to three passages, cells in the logarithmic growth phase were collected, washed in PBS buffer, and digested with 2.5 g/L trypsin and 2 g/L EDTA (Gibco, USA). The cells were arranged into a single cell suspension with use of a pipette. The cell concentration was then adjusted to 3 × 106/ml with RPMI-1640 medium containing 10% FCS. The cell suspension was inoculated in a 6-well plate with 1 ml/well followed by incubation for 48 h at 37 °C, 5% CO2 in the incubator with saturated humidity. After cells adhered to the flask wall, a serum-free medium (pH 7.4) was used to rinse and change the medium to the serum-free medium (1 ml/well).
Co-culture of PMN and endothelial cells
Purified PMN were resuspended in RPMI-1640 medium at a cell concentration of 1 × 106/ml and then added to the endothelial cell culture plate with 1 ml PMN cell suspension/well. The ratio of PMN to endothelial cells was 10:1. Co-cultured cells in the 6-well culture plates were then placed in the incubator for 4 h at 37 °C and 5% CO2. The cells were subsequently grouped (six culture plates per group) for further experimentation. After the groups were exposed to the various treatment conditions described below, the supernatant was collected, cells were washed with PBS, and the adherent endothelial cells were collected. The supernatant and endothelial cells were frozen at − 80 °C for further experiments. The experiments were repeated six times.
Experimental design and methods
Exposure device
The Visual C language programming program (owned and operated by the Department of Respiratory Diseases of the Tianjin Medical University General Hospital) was used in the respiratory simulation system 1.0 (Copyright: Feng Jing, Tianjin, China, 2005). With this device, it was possible to control the intermittent hypoxia/reoxygenation cycle times. The predesigned program in the microcontroller chips controlled the solid-state relay and indirectly controlled the on/off of the solenoid valve, thus controlling the onset and offset of premixed gas flow. The cell culture chamber was designed and manufactured at the Tianjin Medical University General Hospital. The culture chamber was maintained at 37 °C, with a humidity ranging from 45 to 70% and a sterile environment using a thermostat, a heating humidifier, and a microporous membrane.
Experimental groups
Extracted PMN cells were co-cultured with endothelial cells and exposed to hypoxia for 2, 5, or 8 h. For each time period, cells were treated with different oxygen supply conditions and were divided into the following groups: (1) intermittent normoxia (IN), (2) intermittent hypoxia (IH), (3) continuous hypoxia (CH), (4) intermittent and continuous hypoxia (OS), (5) OS+the antioxidant, Tempol (1 × 10−6 mol/L, Sigma-Aldrich, OS+T), and (6) OS+the NF-κB inflammatory channel blocker, PDTC (10 μmol/L, Sigma-Aldrich, OS+P). Cells in the IN group served as the control group and were exposed to 21% O2 for 15 s and then continued with the 21% O2 for 3 min 45 s (i.e., a total of 4 min). Cells in the IH group were exposed to 1.5% O2 for 15 s and then 21% O2 for 3 min 45 s. Cells in the CH group were exposed to 10% O2 for the entire 4 min period. Cells in the OS group were exposed to 1.5% O2 for 15 s and then 10% O2 for 3 min 45 s. The self-made cell culture chamber capacity was 1.8 L, elution flow rate was 0.083 L/s, and the measured elution time was approximately 30 s. All groups of cells were washed for 30 s before exposure periods and were incubated under 5% CO2. Cells exposed to hypoxia for 2, 5, or 8 h indicate the specific oxygen supply conditions that were applied in the cells for 24, 60, and 96 cycles, respectively, with 5 min for each cycle (4 min for oxygen exposure and 2 × 30 s for the washing period). This hypoxia gas exposure device has been shown to effectively induce hypoxia within a variety of cell culture hypoxic exposure models. In this way, the conditions produced in this model are similar and of relevance to the pathophysiology present at the systemic and cellular levels of this disease [9].
Test indicators
The inflammatory factors IL-6 and TNF-α and adhesive molecule, ICAM-1, were determined in the extracted supernatant with use of the double-antibody sandwich enzyme-linked immunosorbent assay (ELISA) (USA R&D Systems, Inc.) according to the kit instructions. The activity of catalase (CAT) and the concentration of malondialdehyde (MDA) were determined with the use of the chemical reagent method (Nanjing Jiancheng Bioengineering Research Institute) according to the kit instructions.
Real-time quantitative PCR (qRT-PCR) was used to assess gene expression of the pro-apoptotic gene, Bak, and anti-apoptotic gene, Bcl-xl, in endothelial cells. Extracted endothelial cells were removed from the − 80 °C freezer, and after being dissolved, the total RNA was extracted using TRIzol according to the kit instructions (Invitrogen, USA). RNA concentration was determined with use of Thermo NanoDrop2000. Total RNA (200 ng) was subjected to reverse transcription reaction using M-MLV reverse transcriptase (Promega Leiden, USA). The reverse transcription product was used as a template and SYBR Green I (AMBION, USA) as a fluorescent dye to perform real-time fluorescent quantitative PCR. Primer sequences for Bak were the following: forward 5′-CCCAGGACACAGAGGAGGTTT-3′ and reverse 5′-GCCTCCTGTTCCTGCTGATG-3′. The amplified fragment length was 65 bp. Primer sequences for Bcl-xl were the following: forward 5′-TGCGTGGAAAGCGTAGACAA-3′ and reverse 5′ -ATTCAGGTAAGTGGCCATCCAA-3′. The amplified fragment length was 75 bp. Primer sequences for GAPDH were the following: forward 5′-AACAGCCTCAAGATCATCAGCA-3′ and reverse 5′-CATGAGTCCTTCCACGATACCA-3′. The amplified fragment length was 102 bp.
Statistical analysis
Data were expressed as mean ± standard deviation. Comparisons among groups were performed using one-way analysis of variance, while those between two groups with use of t tests using SPSS19.0 software. A P = 0.05 was required for results to be considered as statistically significant.
Results
Comparisons of inflammatory factors and adhesion molecules in the supernatant
Within the 2-h hypoxic exposure groups, levels of the inflammatory factors TNF-α and IL-6 and adhesion molecule, ICAM-1, were all significantly increased as compared with those in the IN group (P < 0.05; Fig. 1). Significantly increased levels of TNF-α, IL-6, and ICAM-1 were present in the OS group as compared with those observed in the IH and CH groups (P < 0.05). The antioxidant, Tempol, or the NF-êB inflammatory channel blocker, PDTC (OS+T and OS+P group), significantly reduced the levels of TNF-α, IL-6, and ICAM-1 induced by OS exposure (P < 0.05). TNF-α, IL-6, and ICAM-1 levels in the IH group, while increased as compared with that of the CH group, failed to achieve a statistically significant difference. Similar trends were observed in the 5-h and 8-h exposure groups, with the exception that the overall levels of TNF-α, IL-6, and ICAM-1 were increased with these extended exposure times. Tempol or PDTC treatment significantly reduced the levels of TNF-α, IL-6, and ICAM-1 induced by OS exposure as determined at 5 h or 8 h after hypoxic exposure (P < 0.05). Levels of TNF-α, IL-6, and ICAM-1 in the IH, CH, OS, OS+T, and OS+P groups at 8 h after hypoxic exposure were significantly greater than that obtained after 2 h of exposure (P < 0.05). These results suggest that inflammatory responses represent a major factor underlying time-dependent OS-induced cell damage. Anti-inflammatory and anti-oxidative intervention significantly reduced this hypoxia-induced damage.

Levels of TNF-α (a), IL-6 (b), and ICAM-1 (c) as a function of different conditions and exposure times of hypoxia. a-P < 0.05, aa-P < 0.01 compared with IN; b-P < 0.05, bb-P < 0.01 compared with IH; c-P < 0.05, cc-P < 0.01 compared with CH; d-P < 0.05, dd-P < 0.01 compared with OS; f-P < 0.05, ff-P < 0.01 compared with 2 h; g-P < 0.05, gg-P < 0.01 compared with 5 h
Comparison of oxidative stress markers in the supernatant
Within the 2-h hypoxic exposure groups, CAT activity was significantly decreased, and MDA concentrations significantly increased in the CH, IH, and OS groups as compared with that in the IN group (P < 0.05; Fig. 2). CAT activity in the OS group was significantly decreased as compared with that in the IH and CH groups (P < 0.05). Tempol or PDTC treatment significantly inhibited the reduction of CAT activity induced by OS (P < 0.05). MDA concentrations in the OS group were significantly increased as compared with that in the IH and CH groups (P < 0.05). Tempol or PDTC treatment significantly reduced the increases in MDA concentration induced by OS (P < 0.05). Compared with the CH group, CAT activity in the IH group was decreased and MDA concentrations increased. Within the 5-h and 8-h exposure groups, CAT activity and MDA concentration changes showed a similar trend as that obtained with the 2-h exposure groups; however, these longer exposure times resulted in overall higher levels of MDA and lower levels of CAT. Tempol or PDTC treatment significantly inhibited OS effects on CAT activity and MDA concentrations after OS exposure for 5 h or 8 h (P < 0.05). At the 8-h exposure time period, the CAT activity and MDA concentrations in the IH, CH, and OS groups were significantly different from that obtained in the 2-h exposure group (P < 0.05). CAT activity and MDA concentrations in the OS+T and OS+P groups were similar between 8 h and 2 h of hypoxic exposures. These findings suggest that the OS group exhibited a severe, time-dependent oxidative stress response as compared to the other groups. Anti-inflammatory (Tempol) or anti-oxidation (PDTC) intervention significantly alleviated these oxidative stress responses.

Levels of CAT activity (a) and MDA concentrations (b) as a function of different conditions and exposure times of hypoxia. a-P < 0.05, aa-P < 0.01 compared with IN; b-P < 0.05, bb-P < 0.01 compared with CH; c-P < 0.05, cc-P < 0.01 compared with IH; d-P < 0.05, dd-P < 0.01 compared with OS; f-P < 0.05, ff-P < 0.01 compared with 2 h; g-P < 0.05, gg-P < 0.01 compared with 5 h
Comparison of apoptosis gene expression levels in endothelial cells
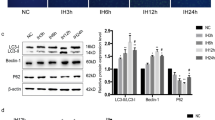
Within the 2-h hypoxic exposure groups, BAK levels were significantly increased, and Bcl-x1 and Bcl-x1/BAK significantly decreased in all groups as compared with those obtained in the IN group (P < 0.05; Fig. 3). Expression levels of the anti-apoptotic genes, Bcl-x1 and Bcl-x1/BAK, were decreased in the OS versus that observed in the IH and CH groups (P < 0.05). The Bcl-x1 gene expression and Bcl-x1/BAK were increased in Tempol- or PDTC-treated OS groups as compared to that in the OS group (P < 0.05). Expression levels of the pro-apoptotic gene, BAK, were increased in the OS as compared to those in the IH and CH groups (P < 0.05). Tempol or PDTC treatment inhibited the increase in BAK gene expression induced by OS (P < 0.05). As compared with the CH group, expression levels of anti-apoptotic genes were decreased, and pro-apoptotic genes increased in the IH group. Results obtained with the 5-h and 8-h exposure groups, including OS groups with Tempol or PDTC treatment, were similar to those of 2-h exposure group. However, again, with these prolonged hypoxia exposure times, these expressions of both pro- and anti-apoptotic genes showed accentuated responses. These reactions were found to be significantly improved with anti-inflammatory (Tempol) or anti-oxidation (PDTC) interventions (P < 0.05). These results indicate that pro-apoptotic genes appear to play a more predominate role in exerting the effects observed versus that of anti-apoptotic genes. Moreover, the significant differences obtained between the 8-h versus 2-h exposure times for both the IH and OS groups (P < 0.05) suggest that the apoptosis within endothelial cells of OS group was more prevalent and time-dependent.

Expressions of BAK (a), Bcl-xl (b), and Bcl-xl/BAK (c) as a function of different conditions and exposure times of hypoxia. a-P < 0.05, aa-P < 0.01 compared with IN; b-P < 0.05, bb-P < 0.01 compared with CH; c-P < 0.05, cc-P < 0.01 compared with IH; d-P < 0.05, dd-P < 0.01 compared with OS; f-P < 0.05, ff-P < 0.01 compared with 2 h; g-P < 0.05, gg-P < 0.01 compared with 5 h
Discussion
A common pathophysiological process in COPD and OSA is hypoxia. While COPD is mainly associated chronic hypoxia, OSA mainly involves intermittent hypoxia. The oxidation and activation/dysfunction of leukocytes resulting from OSA and COPD can trigger a systemic inflammatory response and increase the level of inflammatory factors within the body, eventually inducing a progression to overlap syndrome [10]. It has been reported that NF-κB signaling pathways are preferentially activated during intermittent hypoxia, while HIF-1 is preferentially activated in persistent hypoxia [11]. When the intermittent is accompanied with continuous hypoxic exposure, the downstream gene for NF-κB and a target gene of HIF-1 express a substantial number of inflammatory factors [12]. These inflammatory factors include TNF-α, IL-6, IL-8, and ICAM-1. Such a plethora of inflammatory factors can synergize or produce additive effects, thus resulting in more severe endothelial damage following OS exposure as compared to that resulting from IH and CH. Consistently, our results show that the inflammatory factors IL-6, TNF-α, and adhesion molecule ICAM-1 were increased in the OS versus the IH and CH exposure groups, suggesting that OS hypoxia exposure induces a more severe inflammatory response. In this way, IL-6, TNF-α, and ICAM-1, as well as other inflammatory factors, may be involved in vascular endothelial injury under OS hypoxia exposure, eventually leading to systemic multi-system damage in overlap syndrome patients.
Another important factor involved with vascular endothelial injury induced by hypoxia is oxidative stress. It is well-known that oxidative stress is a major cause of vascular endothelial injury. The increase of oxidative stress in OSA patients mainly occurs during the re-oxygenation phase. Increased ROS can result from either direct effects of oxidative stress or through lipid peroxidation products activating nuclear factor-kappa B (NF-κB), which can then increase levels of downstream inflammatory cytokine targets of NF-κB (e.g., IL-6, IL-8, TNF-α) and adhesion molecules (ICAM-1, VCAM-1) [13]. Increased activity of pro-inflammatory cytokines and adhesion molecules leads to delayed apoptosis of PMN, accelerated apoptosis of endothelial cells, and ultimately vascular endothelial inflammation [14, 15]. The oxidative stress observed in COPD patients includes increased oxides, decreased oxidative damage repair capacity, and reduced oxide active media clearance [16]. Inflammatory cells such as PMN, macrophages, and eosinophils are important sources of oxide production [17]. Therefore, an essential component of systemic oxidative stress and inflammation resulting from COPD involves an activation of circulating pro-inflammatory cells, such as PMN, and macrophages. Activated inflammatory cells release increased levels of endogenous oxides [18]. Thus, as demonstrated within our current study, we propose that the OS mode of hypoxic exposure can be a significant factor in endothelial damage. In this way, the combination of intermittent and continuous hypoxia may lead to more severe inflammation and oxidative stress, delayed PMN apoptosis, and endothelial damage. Oxidative stress can be reflected by several markers. The lipid peroxidation product, MDA, can indirectly reflect levels of cellular oxidative stress levels, while CAT catalytically decomposes hydrogen peroxide to protect cells from oxidative stress damage caused by ROS. In this study, we show that the OS group had lower levels of CAT activity and higher levels of MDA concentrations as compared with that of the IH or CH groups, indicating that more oxidative stress would be present in the OS group.
Results obtained from a rat model of OS as induced by IH and smoke exposure revealed that a greater degree of systemic inflammation and oxidative stress was detected as compared with that observed in IH-exposed rats or the rat model of emphysema induced by smoke exposure, suggesting the presence of an additive effect [19]. Consistently, our current findings show that, at the cellular level, maximal inflammatory injury and oxidative stress occur in the OS group, as well as more severe damage to endothelial cells, effects which are time-dependent. Therefore, it appears that the interaction between neutrophil and endothelial cells can induce the inflammation and oxidative stress involved in vascular endothelial cell injury resulting from OS hypoxia.
It has been well established that the Bcl-2 gene family is involved in apoptosis [20]. Bcl-xl and bak, which belong to the Bcl-2 family, are widely expressed in various tissues within the human body. Bcl-x1 inhibits apoptosis by forming a heterodimer with bak, and the ratio of these two genes determines whether cells will undergo apoptosis or not. OSA patients have significantly increased densities of serum endothelial cell apoptosis, and hypoxia plays an important role in mediating this endothelial apoptosis [21]. Hypoxia is also associated with abnormal endothelial vasodilation and initiates atherosclerosis [21]. The accelerated and time-dependent apoptosis seen in endothelial cells in response to OS hypoxia within our current experiment suggest that apoptotic genes play an important role in the pathogenesis of vascular endothelial cell injury induced by OS hypoxia.
Tempol is a superoxide dismutase mimetic that directly scavenges oxygen radicals. Accordingly, it can alleviate ischemia-reperfusion injury of tissues and organs and inhibit the oxidative damage of inflammatory responses. In specific, Tempol reduces damage resulting from exogenous ROS within cultured cells and ischemia-reperfusion injury within the brain and liver [22, 23]. It has been reported that in animal models, tempol can partially protect cardiovascular dysfunction resulting from overlap syndrome [24]. Here, we show that the antioxidant, Tempol, was effective in diminishing oxidative stress damage and improving endothelial function by scavenging ROS. We also tested the effects of PDTC, a metal chelating agent with anti-inflammatory effects. PDTC can inhibit the phosphorylation and degradation of IκB by affecting the production of pro-inflammatory cytokines, which further inhibits the activation and function of NF-κB [25]. Inhibition of NF-κB expression can partially inhibit inflammatory responses [26]. Our current results show that the levels of inflammatory factors, oxidative stress, and apoptosis gene expression were all improved in the OS+T and OS+P as compared to the OS group. These findings indicate that anti-inflammatory and anti-oxidative treatment can partially inhibit inflammation and oxidation and endothelial cell apoptosis, thereby slowing vascular endothelial injury. Accordingly, our findings may provide a new and important theoretical basis for the clinical application of anti-inflammatory or anti-oxidant treatment of cardiovascular complications resulting from overlap syndrome.
In summary, neutrophil and vascular endothelial cell interactions resulting from OS hypoxia can increase pro-inflammatory cytokines, aggravate inflammatory responses, and oxidative stress, thereby accelerating vascular endothelial cell apoptosis. In this way, inflammatory responses, oxidative stress, and apoptotic genes are all involved in vascular endothelial injury induced by OS, which represents the pathogenesis of overlapping syndromes complicated with cardiovascular disease. While application of anti-inflammatory and antioxidant interventions cannot completely reverse this endothelial cell damage, these treatments can partially reduce inflammatory responses, regulate the oxidation/antioxidant imbalance, and reduce the apoptosis of vascular endothelial cells.
References
Ganga HV, Nair SU, Puppala VK, Miller WL (2013) Risk of new-onset atrial fibrillation in elderly patients with the overlap syndrome: a retrospective cohort study. J Geriatr Cardiol 10:129–134
Thomashow MA, Shimbo D, Parikh MA, Hoffman EA, Vogel-Claussen J, Hueper K, Fu J, Liu CY, Bluemke DA, Ventetuolo CE, Doyle MF, Barr RG (2013) Endothelial microparticles in mild chronic obstructive pulmonary disease and emphysema. The multi-ethnic study of atherosclerosis chronic obstructive pulmonary disease study. Am J Respir Crit Care Med 188:60–68
Papachatzakis I, Velentza L, Zarogoulidis P, Kallianos A, Trakada G (2018) Comorbidities in coexisting chronic obstructive pulmonary disease and obstructive sleep apnea- overlap syndrome. Eur Rev Med Pharmacol Sci 22(13):4325–4331
Kendzerska T, Leung RS, Aaron SD, Ayas N, Sandoz JS, Gershon AS (2019) Cardiovascular outcomes and all-cause mortality in patients with obstructive sleep apnea and chronic obstructive pulmonary disease (overlap syndrome). Ann Am Thorac Soc 16(1):71–81
Tang SF, Wang X, Zhang Y, Hou J, Ji L, Wang ML, Huang R (2015) Analysis of high alert medication knowledge of medical staff in Tianjin: a convenient sampling survey in China. J Huazhong Univ Sci Technolog Med Sci 35:176–182
Foster GE, Poulin MJ, Hanly PJ (2007) Intermittent hypoxia and vascular function: implications for obstructive sleep apnoea. Exp Physiol 92:51–65
Kent BD, Ryan S, McNicholas WT (2011) Obstructive sleep apnea and inflammation: relationship to cardiovascular co-morbidity. Respir Physiol Neurobiol 178:475–481
Hu M, Lin X, Du Q, Miller EJ, Wang P, Simms HH (2005) Regulation of polymorphonuclear leukocyte apoptosis: role of lung endothelium-epithelium bilayer transmigration. Am J Physiol Lung Cell Mol Physiol 288:L266–L274
Feng J, Chen B, Guo M, Cao J, Zhao H, Liang D (2006) A novel system for the simulation of various intermittent hypoxia modes. J Tianjin Med Univ 12(4):509–515
McNicholas WT (2009) Chronic obstructive pulmonary disease and obstructive sleep apnea: overlaps in pathophysiology, systemic inflammation, and cardiovascular disease. Am J Respir Crit Care Med 180:692–700
Ryan S, Taylor CT, McNicholas WT (2005) Selective activation of inflammatory pathways by intermittent hypoxia in obstructive sleep apnea syndrome. Circulation 112:2660–2667
Leroy V, De Seigneux S, Agassiz V, Hasler U, Rafestin-Oblin ME, Vinciguerra M et al (2009) Aldosterone activates NF-kappaB in the collecting duct. J Am Soc Nephrol 20:131–144
Li S, Qian XH, Zhou W, Zhang Y, Feng J, Wan NS et al (2011) Time-dependent inflammatory factor production and NFkappaB activation in a rodent model of intermittent hypoxia. Swiss Med Wkly w13309:141
Jurado-Gamez B, Bujalance Cabrera C, Caballero Ballesteros L, Marin Hinojosa C, Munoz Cabrera L, Perez-Jimenez F et al (2012) Association of cellular adhesion molecules and oxidative stress with endothelial function in obstructive sleep apnea. Intern Med 51:363–368
Lurie A (2011) Endothelial dysfunction in adults with obstructive sleep apnea. Adv Cardiol 46:139–170
Yao H, Rahman I (2011) Current concepts on oxidative/carbonyl stress, inflammation and epigenetics in pathogenesis of chronic obstructive pulmonary disease. Toxicol Appl Pharmacol 254:72–85
Wang ZL (2010) Evolving role of systemic inflammation in comorbidities of chronic obstructive pulmonary disease. Chin Med J 123:3467–3478
Rahman I (2003) Oxidative stress, chromatin remodeling and gene transcription in inflammation and chronic lung diseases. J Biochem Mol Biol 36:95–109
Li C, Yang X, Feng J, Lei P, Wang Y (2015) Proinflammatory and prothrombotic status in emphysematous rats exposed to intermittent hypoxia. Int J Clin Exp Pathol 8:374–383
Korsmeyer SJ (1992) Bcl-2 initiates a new category of oncogenes: regulators of cell death. Blood 80:879–886
Grebe M, Eisele HJ, Weissmann N, Schaefer C, Tillmanns H, Seeger W, Schulz R (2006) Antioxidant vitamin C improves endothelial function in obstructive sleep apnea. Am J Respir Crit Care Med 173:897–901
Kato N, Yanaka K, Hyodo K, Homma K, Nagase S, Nose T (2003) Stable nitroxide Tempol ameliorates brain injury by inhibiting lipid peroxidation in a rat model of transient focal cerebral ischemia. Brain Res 979:188–193
Sepodes B, Maio R, Pinto R, Marques C, Mendes-do-Vale J, McDonald MC et al (2004) Tempol, an intracelullar free radical scavenger, reduces liver injury in hepatic ischemia-reperfusion in the rat. Transplant Proc 36:849–853
Zhao H, Zhao Y, Li X, Xu L, Jiang F, Hou W, Dong L, Cao J (2018) Effects of antioxidant tempol on systematic inflammation and endothelial apoptosis in emphysematous rats exposed to intermittent hypoxia. Yonsei Med J 59(9):1079–1087
Liu LN, Wang S, Wu YJ, Guo Y, Tian YM, Wang Q et al (2017) Association of NF-κB and its downstream pathway with acute radiation-induced myocardial fibrosis in rats. Chin J Radiat Oncol 26:453–458
Ben-Neriah Y, Karin M (2011) Inflammation meets cancer, with NF-kappaB as the matchmaker. Nat Immunol 12:715–723
Funding
This study was funded by the National Natural Science Foundation of China (grant number 81670084).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Xiao, F., Li, X., Wang, J. et al. Mechanisms of vascular endothelial cell injury in response to intermittent and/or continuous hypoxia exposure and protective effects of anti-inflammatory and anti-oxidant agents. Sleep Breath 23, 515–522 (2019). https://doi.org/10.1007/s11325-019-01803-9
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11325-019-01803-9