
Abstract
Introduction
Oral microflora is a well-orchestrated and acts as a sequential defense mechanism for any infection related to oral disease. Chronic periodontitis is a disease of a microbial challenge to symbiosis and homeostasis. Periodontal surgery is the most promising cure with repair process during periodontal regeneration. It has an encouraging outcome in terms of early recovery biomarkers.
Objective
Saliva of periodontal surgery subjects with the chronic periodontitis have been evaluated by 1H NMR spectroscopy in search of possible early metabolic differences that could be obtained in order to see the eradication of disease which favours the symbiotic condition.
Method
The study employed 1H NMR spectroscopy on 176 human saliva samples in search of distinctive differences and their spectral data were further subjected to multivariate and quantitative analysis.
Result
The 1H NMR study of periodontal surgery samples shows clear demarcation and profound metabolic differences when compared with the diseased condition. Several metabolites such as lactate, ethanol, succinate, and glutamate were found to be of higher significance in periodontal surgery in contrast to chronic periodontitis subjects. The PLS-DA model of the studied group resulted in R2 of 0.83 and Q2 of 0.70.
Conclusion
Significant metabolites could be considered as early repair markers for chronic periodontitis disease as they are being restored to achieve symbiosis. The study, therefore, concluded the early recovery process of the diseased subjects with the restoration of possible metabolomic profile similar to the healthy controls.
Graphic abstract

Similar content being viewed by others


Avoid common mistakes on your manuscript.
1 Introduction
Salivary microbiome infers the symbiosis between human health and microbiota. Many factors that influence this dynamic ratio of symbiosis i.e. smoking, tobacco consumptions, food habits, reactive oxygen species (ROS) generation and many more factors that disturbs the microbiota leading to the deterioration of oral biofilm which refers to the condition defined as dysbiosis (Kilian et al. 2016). Perturbation or dysbiosis indicate pathological consequences such as chronic periodontitis, gingivitis, dental plaque, tooth decay, etc. Roughly 108 microbes constitute per ml of saliva, which shows the great diversity and functionality of this biofluid (Marsh et al. 2016). Introduction of microbial diseases to Human Microbiome project [Human Oral Microbiome Database (HOMD)] which establishes the fact that microbial association with humans has a great impact with respect to a healthy life.
Chronic periodontitis is a diseased state which faces with a microbial challenge that penetrates the host defense system, connective tissue detachment followed by alveolar bone resorption and thus results in tooth decay (Page and Kornman 1997). In chronic periodontitis, gram-negative bacteria generally establish a connection via epithelium to connective tissue and releases their active metabolites as Lipopolysaccharides (LPS), fatty acid, N-formyl-methionylleucyl-phenylalanine (FMLP), etc. It further prompts the host defense system to release various cytokines including Matrix metalloproteinases(MMPs), prostaglandins and Tumor Necrosis Factor- α (TNF-α) (Kornman et al. 1997). These effector molecules move through junctional epithelium which results in Extra Cellular Matrix (ECM) destruction accompanied by neutrophils activation including stimulation of endothelial cells and extravasation of leukocytes. These processes activate macrophages along with MMPs in action, thus launching an inflammatory response with triggering of complement cascade locally. Macrophage secretary products act as a chemoattractant and are responsible for capitalizing its own numbers. Initiation of the collagen degradation majorly by MMPs (Referred to as Endopeptidases sometimes) and collagenase production that favors the ECM degradation (Reynolds and Meikle 1997). Extensive collagenase activity was identified on larger amounts in chronic periodontitis patients as compared to healthy fellows particularly in Gingival crevicular fluid (GCF). Majorly, there are two types of cell in jaw bone named as osteoblast and osteoclast. Osteoblast has a major function of synthesis and mineralization while osteoclast does resorption by performing demineralization. Their activities are tightly regulated by hormones and factors that are locally involved are Interleukins, Interferon, TNF-α, Prostaglandins, Platelet-derived growth factor (PDGF) and Transforming growth factor β-1 (TGF-β1), etc. (Foresta et al. 1984). Both the cells perform their function on a regular basis of time span i.e. from 25 to 30 years of age. Thereafter, constant decreases in the bone mass start for both the genders but male are more prone to it. Our recent study had already demonstrated distinct salivary metabolic perturbations in chronic periodontitis when compared with healthy controls (Singh et al. 2017). At last stage of chronic periodontitis, crestal alveolar bone starts disappearing followed by osteoclast recruitment and activation sequestering the crestal bone resorption thus resulting in a loss of anchorage along with cementum resorption and finally concluding the process of tooth loss (Page and Schroeder 1976).
The ultimate aim for periodontal surgical treatment is to stop recurrence of the disease and to restore the healthy structure and function of tooth periodontium. Several antibiotics, locally administered antimicrobial agents and medically tested mouth wash as suggested by the clinicians often lead to dysbiotic conditions which have always been a challenge for an ultimate cure (Mombelli 2018). Periodontal wound repair and healing normally take place after periodontal surgery in diseased subjects. A fibrin clot formation between the root and flap surface initiates the healing process, which often supports a route for cellular movements. Fibrin clot needs further stabilization as many mechanical forces are likely to disturb it until new collagen tissue replaces it successfully (Susin et al. 2015). Later, gingival connective and epithelium tissues come into the picture which has a powerful mechanism of regeneration that precedes the repair events in a sequential manner (Melcher 1976). Since this study is the extended work of our earlier published research article (Singh et al. 2017) regarding the comparative study between healthy controls and chronic periodontitis patients to find distinctive metabolic differences. Hence the current study prompted us further to evaluate the role of saliva metabolomics using 1H NMR spectroscopy for observing possible metabolic recovery between earlier chronic periodontitis subjects (please refer to the Supplementary Figure S-7) after their periodontal surgery. Secondly, to evaluate the extent of metabolic recovery along with pathway analysis of statistically significant metabolites when compared to healthy subjects in order to see the reversal of the disease that progresses towards a symbiotic condition which could indicate the stage of improvement. Eventually, periodontal surgery attempts to establish a symbiotic environment from the very beginning, which starts from the adherence of early colonizers to till colony stabilization by late colonizers to support the overall structure of biofilm. Many microbial species may vary a lot depending on the individual’s own habit, oral hygiene and other influential factors (smoking, chewing tobacco, etc.). Therefore, we aim to focus on the early repair process, where metabolomics helps us to find a way on the level of metabolites, whereas classical approaches will take much longer duration.
2 Material and method/experimental section
2.1 Subjects and sample collection
The study involves a collection of 176 human saliva samples, chronic periodontal subjects (n = 62), further subjected to periodontal surgery (n = 62) and healthy controls (n = 52) mentioned in Table S-1. Saliva was collected in a sterile container (containing 2.0 mg of Sodium Azide) for 10 min of time duration in early morning hours without any oral refraining activity (Brushing, gargling, chewing, etc.). Patient consents were taken well before the study and were fully briefed about the investigation purpose. Samples were snap frozen in liquid nitrogen immediately after expectoration and later kept at − 80 °C till further processing of samples. TSP (Trimethylsilyl propionate) was used as an internal standard for all saliva samples. According to the Gardner et al. 2018, the use of TSP as an internal standard has a significant impact on the condition where the buffer is not being used with saliva samples. Notably, TSP is known to bind protein which results in line broadening of signals obtained, but this happens more in plasma rather than in saliva, which has very low protein content. The saliva samples were collected after 21 days of periodontal surgery (Kaner et al. 2017). The study was ethically approved by the committee (Ethical approval No. - B-07: CBMR/EMP/IEC/3/26-02-2011).
2.2 Sample preparation and acquisition
Sample preparation and acquisition was performed in a similar way as mentioned in our earlier study (Singh et al. 2017). Samples were taken out of − 80 °C and thawed at room temperature and were further subjected to centrifugation at 5000×g for a duration of 30 min. The supernatant of the amount of 300 µl was isolated from each sample and was mixed with an equal amount (300 µl) of sodium phosphate buffer in 5 mm standard NMR tube (Wilmad Glass USA) and sample homogeneity was maintained by vortexing it for 30 s. Samples were subjected to NMR experiments by using spectrometer equipped with a 5 mm Triple resonance inverse (TCI)1H/13C/15N cryoprobe with a Z-shielded gradient and standard vertical bore, operating at a proton frequency of 800.21 MHz (18.8 T) of Bruker Biospin Avance III 800 MHz NMR (Bruker, GmBH).
2.3 NMR experimental conditions
The 1H NMR spectra were recorded of all 176 human saliva samples were recorded at 300 K with 128 scans and 4 dummy scans with water presaturation using Carr-Purcell-Meiboom-Gill (CPMG) pulse sequence with the following experimental parameters: spectral width of 12,019 Hz, time domain data points of 64 K, relaxation delay 4.0 s, 128 scans with 4 dummy scans, with a total recording time of approximately 15 min. CPMG pulse sequence with water suppression [PRESET − 90° − (δ − 180° − δ) n − Aq] with an echo time of 300 µs was performed. 1D NOESY pulse sequence was also recorded with a total acquisition time of 12 min 54 s per sample. To confirm the assignments, two-dimensional 1H–1H homonuclear correlation spectroscopy (COSY) and 1H–13C heteronuclear single quantum correlation spectroscopy (HSQC) were performed using Bruker’s standard pulse program library [for details please refer (Singh et al. 2017)]. In order to minimize quantification error using short recycle delay of all the metabolites by CPMG NMR spectral data, relaxation correction factors have to be incorporated while performing the quantification of metabolites (Bharti and Roy 2012). Since the commercial Chenomx Software (Chenomx Inc.) is designed to perform precise quantification by utilizing their calibrated internal standard (TMSP) at different field strengths (Chenomx 2015) using CPMG spectra with 4 s recycle delay, we have followed the identical pattern and it has also been validated in a recent NMR methodology study on saliva samples (Gardner et al. 2018).
2.4 Statistical analysis (data reduction and pattern recognition)
Phase, baseline corrected and calibrated CPMG NMR spectra were employed in multivariate analysis. The spectral region was reduced with a specific region in chemical shift after removing water region 5.15 to 4.49. Binning and other removal of discrete regions were exactly performed as mentioned in our previous research article (Singh et al. 2017). The resulting data matrices having normalized integral values were exported into Microsoft Office Excel 2007 (Microsoft Corporation, USA). These were further imported to ‘The Unscrambler X’ Software package (Version 10.0.1, Camo USA, Norway) for multivariate principal component analysis (PCA) and partial least square discriminant analysis (PLS-DA). PCA and PLS-DA were performed on matrices of spectra from periodontal Surgery subject (n = 62), chronic periodontal case subject (n = 62) and healthy controls (n = 52) for comparing their metabolic profiles. In PCA and PLS-DA, full cross-validation using leave-one-out were applied for avoiding the overfitting of the mathematical model. VIP score analysis was performed by Metaboanalyst (version 4.0) for further confirmation of the results.
3 Results
3.1 Metabolic profile of Saliva samples
The 1H NMR spectra from periodontal surgery, periodontal case (chronic periodontitis) subjects and healthy controls (n = 176) were further analyzed for characterizing the metabolites as reported in literature (Aimetti et al. 2012), (Dame et al. 2015), The assignment of metabolites were further reinstated as reported in the Biological Magnetic Resonance Bank (BMRB, www.bmrb.wisc.edu), (Markley et al. 2007) Human Metabolome Data Base (HMDB, www.hmdb.ca), (Wishart et al. 2009) (Supplementary Table S-4) and Chenomx version 8.1(Chenomx Inc.). A representative class of 1H NMR-spectra obtained from periodontal surgery, periodontal case and healthy subjects are presented in Fig. 1.

Typical 800 MHz comparative 1H-NMR spectra of saliva samples of a healthy, b chronic periodontitis and c periodontal surgery subjects were recorded at 300 K
In the above comparative spectra, we can easily identify the differences, which were further illustrated by their metabolomic signatures (please refer supplementary Fig S-1 for more information). Figs S-1 and S-3 represents some inter-individual variability with respect to lactate within the periodontal surgery group and this may likely to happen as few subjects are still in the process of improvement after surgery as reflected in the multivariate analysis. Periodontal surgery spectra represent an improved metabolic profile when compared to periodontal case, while with healthy controls, the more refined and prominent profile was observed due to their surgical indisposition.
3.2 Multivariate analysis of the periodontal case and periodontal surgery subjects (group 1)
Multivariate analysis was performed for periodontal cases and periodontal surgery subjects as presented in Fig. 2a, b; 3D scatter plot shows a clear demarcation between the groups in supervised PLS-DA analysis, which indicates comparatively different metabolomic status with R2 and Q2 of 0.83 and 0.70 respectively.

a 3D PCA and b 3D PLS-DA plot describing the difference between periodontal case and periodontal surgery subjects. c A 3D PCA and d 3D PLS-DA plot displaying the pattern between healthy control and periodontal surgery subjects
3.3 Multivariate analysis of healthy control and periodontal surgery subjects (group 2)
Multivariate analysis was performed for healthy controls and periodontal surgery subjects as demonstrated in Fig. 2c, d showing PCA and further PLS-DA 3D scatter plot analysis. In PCA, insignificant group separation observed, however in the supervised PLS-DA scattered score plot, surgical and control subjects has subtle differences as few surgical subjects are falling apart from control ones. This acquired character reflect supreme oral hygiene due to surgical indisposition with low goodness of fit (R2) and predictive ability (Q2). This explains that groups are poorly separated which points out towards similar metabolomic profile. While multivariate analysis with healthy ones and chronic periodontitis patients were found to be well separated as demonstrated in our earlier study (Singh et al. 2017). The multivariate analysis of all three groups as shown in Fig. 3 also strengthens the fact that periodontal surgery subjects in the PCA score plot is showing similar distribution pattern when compared against controls along with fewer towards the disease subjects. This indicates the improvement observed after periodontal surgery. Figure 2c is also depicting similar pattern as demonstrated in the PCA score plot.

a 3D PCA and b PLS-DA plot depicting the stage of improvement and orchestration among healthy control, periodontal case and periodontal surgery subjects
3.4 Pathway impact and VIP score analysis of group 1 subjects
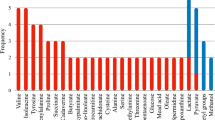
VIP score and pathway impact analysis were further executed for data enrichment using Metaboanalyst (version 4.0) software along with SPSS (SPSS Inc., Version 21) software for independent student t test between the periodontal case and periodontal surgery subjects (Supplementary Fig S-3). All significant metabolites analyzed through VIP score of 2 and above are portrayed in Fig. 4b; listing glutamate (2.09 ppm) followed by ethane sulfonate (1.25 ppm), fucose (1.19 ppm), lactate (4.15 ppm), ethanol (3.67 ppm), succinate (2.41 ppm), proline (1.99 ppm) and pyruvate (2.39 ppm), were found to be lower in periodontal surgery subjects. The pathway analysis (Fig. 4a) reflected alanine, aspartate and glutamate metabolism which impacted the most, followed by glycolysis/gluconeogenesis, butanoate metabolism, arginine and proline metabolism, citrate metabolism, and pyruvate metabolism are also presented in Supplementary Table S-2.

a Pathway impact analysis and b VIP score plot between the periodontal case and periodontal surgery subjects. c Pathway impact analysis and d VIP score plot between healthy control and periodontal surgery subjects
3.5 Pathway impact and VIP score analysis of group 2 subjects
In this group, the VIP score analysis did not display a string of significance but depicted a mixture of responses as few are associated with controls and rest favoured the surgical condition (Fig. 4d). Ethane sulfonate (1.25 ppm), ethanol (1.19 ppm), lactate (4.15 ppm) and isoleucine (1.27 ppm) are highly significant in healthy control subjects. Whereas, propionate (1.07 ppm), glycine (3.57 ppm), alanine (3.77 ppm), leucine (3.83 ppm) and succinate (2.41 ppm) favors the periodontal surgery subjects, while glutamate (2.09 ppm) appeared in both the subjects. This mixed responses where only half of the metabolites were found to be statistically significant (Supplementary Table S-3), indicating the alanine, aspartate and glutamate metabolism playing major roles in the pathway impact analysis as indicated in Fig. 4c. The Table S-3 which again consolidates the fact that even though major confounders were reported between controls vs periodontal surgery subjects, half of them were found not to be statistically significant and states that these metabolites followed the similar pattern. Due to low goodness of fit (R2) and predictive ability (Q2) of groups, separation could be considered as indiscrete.
4 Discussion
The larger population in developing countries ignore periodontitis which may arise due to the lack of pain and sometimes bleeding gums until it has reached a chronic stage. This results in dragging the severe clinically detectable diseased subjects to the dentist. Recently, an epidemiological study was conducted on Indian population regarding periodontitis and has been found that public to dentist ratio is 200,000:1 especially in rural areas, which is quite alarming (Chandra et al. 2016). Perceptible observation, pocket declination, probe bleeding measurement and severity of attachment loss is the most recommended procedure opted by the dental practitioner for identification of chronic periodontitis. Salivary diagnostic tests are available for the periodontitis but they are unable to predict the duration and commencement of the disease affair (Kim et al. 2013).
Well-Orchestrated events define the entire repair process after periodontal surgery which takes almost about 3 weeks that begins with fibrin clot formation. This fibrin-rich complex renders more strength and avoids any wound dehiscence followed by local recruitment of leucocytes and neutrophils in close vicinity of the fibrin clot along with the active proliferation of mesenchymal, periodontal ligament and bone lining cells in the same niche. Bone lining cells thus moves to the margins and secretory osteoblasts are employed to nurture the local environment with a copious amount of collagen, referred as osteoid that overlays the foundation of the fresh periodontium (Susin et al. 2015). Sometimes enamel matrix derivative (EMD) is also dispensed in the local area for profound healing and effective regeneration accelerates in the hard and soft tissues (Andrei et al. 2017).
Reduced levels of glutamate, succinate, fucose, proline, and ethanol in group 1 could be useful in distinguishing and diagnosing the improvement in the repair process with respect to the diseased condition (García-Villaescusa et al. 2018). Improving levels of pyruvate, lactate also states similar consequences (Aimetti et al. 2012). Glutamate is a principal metabolite as it has a pivotal role in transamination reaction that further upregulates in proteolysis and gets accelerated in chronic periodontitis during collagen destruction (Higham and Edgar 1989). In group 2, several metabolites having minor significance are succinate, propionate, leucine, isoleucine, and glycine, with subtle differences within the group, also consolidates the above findings. This indicates the metabolic shifting of periodontal surgery subjects towards healthy controls as the surgical subjects were found to have a similar metabolomic pattern when compared with healthy controls (Singh et al. 2017)). Thus, it supports the periodontal repair mediating the genesis of the recovery process.
Chronic periodontitis is characterized as a bacterial disease with heavy loads of inflammation and acid stress which can be predicted in the proposed pathway (Fig. 5). Multiple metabolic processes during chronic periodontitis include significant metabolites that have been upregulated and its improvement was observed after periodontal surgery (Supplementary Table S-2) are summarized as Fig. 5. Microbial recruitment starts with primary adherence of early colonizers bridged by mid and successively attended by late colonizers (Kolenbrander and London 1993). The bacterial population inducts different ways of attaining energy for their metabolic needs. The metabolic shift is the main cause of the disease as a number of different bacteria metabolize the host-derived products in a different manner depending on their metabolic needs. They can be saccharolytic, asaccharolytic and proteolytic in nature, thus influencing the microbial ecosystem by the product they impart in the niche. Oral microflora also generates VSCs (Volatile Sulfur compounds) which are toxic in nature and are responsible for oral malodor (Ratcliff and Johnson 1999). Majority of oral malodor comes from foul smell generated by VSCs. VSCs comprises of Hydrogen Sulfide (H2S), Methyl mercaptan, dimethyl sulfide (CH3SCH3) and dimethyl disulfide (CH3SSCH3). Host tissues are required to generate VSCs which often involves protein putrefaction (Fosdick and Piez 1953) and metabolism of sulfur-containing amino acids such as cysteine and methionine (van der Ploeg et al. 2001). Ethane sulfonate observed in this study also favours cysteine metabolism (Kertesz 2000).

Proposed metabolic pathways for early repair in chronic periodontitis
Streptococcus and Actinomyces species are saccharolytic in nature and metabolizes carbohydrate through the glycolytic pathway leading to the formation of anaerobic products i.e. lactate, formate, acetate, and succinate. Porphyromonas gingivalis, Eubacterium saburreum, Campylobacter, Fusobacterium nucleatum, and Prevotella intermedia are asaccharolytic or proteolytic in nature (Takahashi and Yamada 2000). They both require dipeptide or amino acids for nutrition and impart their role in amino acid metabolism, which often plays an important role in the increased inflammatory and immune response by compromising the complement cascade proteins and degrading the blood-clotting cascade. Porphyromonas gingivalis has two arginine- and lysine-specific cysteine proteases termed as gingipains. While P. intermedia has active cysteine protease known as Interpain ‘A’ which degrades the majority of the proteins including major carrier protein albumin etc. (Takahashi 2005). Few gram-negative bacteria i.e. Fusobacterium spp. also generates short chain fatty acids like acetate, propionate, isovalerate, and lactate which plays a key role in chronic periodontitis leading to host cell dysfunction and compromised immunity (Gharbia and Shah 1991).
Periodontal surgery subjects demonstrated the restoration of glutamate, lactate, ethanol, and succinate as shown in Fig. 5. Whereas, proline was found to be significantly reduced in post-surgical subjects (Supplementary Table S-2). Therefore, it serves as an important metabolite which supports the degradation of proline-rich salivary proteins in chronic periodontitis. Ethane sulfonate mostly imparts in VSCs production and oral malodor. It may get controlled later by establishing a symbiotic population and thus not reflecting its effectiveness in early repair process (Supplementary Table S-2). The above-mentioned metabolites can be considered as early repair markers for post-surgical cases as they are getting restored towards healthy controls (Singh et al. 2017). Surgery also lowers the rate of normal aerobic fermentation, which is characteristic of healthy subjects. Surgical subjects projected very high levels of maltose and glucose present in the representative spectra and same also has been provided in the Supplementary Fig S-1 that includes comparative spectra between periodontitis vs periodontal surgery subjects. This explains the shifting of the proteolytic, gram-negative and majorly anaerobic microbial population (commonly described as dysbiosis) to fermentative, gram-positive and facultative population, a condition is known as symbiosis (Takahashi 2005). Fermentative metabolism which includes an adequate amount of sugars is an indicator of healthy microflora as projected in healthy control subjects. Few post-surgery cases which are still in the process of improvement might lack some of the healthy metabolic signatures when compared to the other post-surgery subjects who had responded well in our study. Such post-surgical patients can upgrade their metabolic status by maintaining better oral hygiene and preventive care as advised by dental professionals.
Outmost aim of periodontal surgery is to rehabilitate the symbiotic microbial population in order to provide effective resistance against microflora that perturbs homeostasis and shifts the microbial population towards dysbiosis resulting in massive inflammation, malodor and tissue destabilization. It has been observed that we were unable to find marked differences between healthy controls and periodontal surgery subjects. This may arise due to a reason that both of the group share common metabolic features and hence we cannot demarcate between this two metabolomically. This may be considered as a limiting factor associated in our study and can be further explored by incorporating a larger cohort of the study subjects.
5 Conclusion
Healthy microflora plays an important role in our digestion as well, where saliva plays a primary step in the process and probably initiates the start of a healthy day. The microbial association with humans are now offering new insights for future research as mostly immunity comes from the gut as 90% serotonin synthesized by microbes in the gut and not from the brain (O’mahony et al. 2015). Periodontal ligament (PDL) which supports the tooth structure as the tensile cable that connects the cementum and alveolar bone. Cells which synthesizes PDL largely referred to as PDL Fibroblasts (PDLFs). PDLFs produces collagen which strengthens PDL and helps majorly in repair and regeneration of the periodontal ligament. PDL stem cell activity in the local environment plays a crucial role as they are more tolerant to mechanical stress in healthy condition than in periodontitis (Chukkapalli and Lele 2018). Periodontal regeneration is a sequential procedure and a matter of enhanced public awareness to avoid any wound dehiscence and stay away from any further infection. This study may help to demarcate the differences between diseased and post-surgical subjects with early repair biomarkers and dental professionals can easily monitor the progress within a short span of time. Therefore, more diversified research is required in the area of oral health in order to gain in-depth knowledge regarding healthy oral microflora, which could be redefined in terms of geographical distribution, eating habits and oral hygiene.
6 Supporting information
Table S-1 for demographic distribution of study subjects and Table S-2, Table S-3 for a p-value of both the group-1 and group-2 metabolites along with Table S-4 for list of identified metabolites along with their HMDB id. Figure S-1 for more detailed information regarding comparison among the metabolic profile of studied subjects and Figure S-2 to S-6 were provided for more detailed statistical analysis. Figure S-7 refers to PCA and PLS-DA analysis between control (healthy) and case (chronic periodontitis) group. Binned excel data for saliva samples of all groups, chronic periodontitis, and periodontal surgery subjects, healthy and periodontal surgery subjects. Quantified excel data for all groups.
Abbreviations
- CPMG:
-
Carr-purcell-meiboom-gill
- NMR:
-
Nuclear magnetic resonance
- NOESY:
-
Nuclear overhauser effect spectroscopy
- PCA:
-
Principal component analysis
- PLS-DA:
-
Partial least square discriminant analysis
- SD:
-
Standard deviation
- SPSS:
-
Statistical package for social science
- TSP:
-
Trimethylsilyl propionate
- VIP:
-
Variables importance in projection
- ROC:
-
Receiver operating characteristic curve
References
Aimetti, M., Cacciatore, S., Graziano, A., & Tenori, L. (2012). Metabonomic analysis of saliva reveals generalized chronic periodontitis signature. Metabolomics, 8(3), 465–474.
Andrei, M., Dinischiotu, A., Didilescu, A. C., Ionita, D., & Demetrescu, I. (2017). Periodontal materials and cell biology for guided tissue and bone regeneration. Annals of Anatomy-Anatomischer Anzeiger, 216, 164–169.
Bharti, S. K., & Roy, R. (2012). Quantitative 1H NMR spectroscopy. TrAC, Trends in Analytical Chemistry, 35, 5–26.
Chandra, A., Yadav, O. P., Narula, S., & Dutta, A. (2016). Epidemiology of periodontal diseases in Indian population since last decade. Journal of International Society of Preventive & Community Dentistry, 6(2), 91.
Chenomx, N. M. R. (2015). Suite. Edmonton: Chenomx Inc.
Chukkapalli, S. S., & Lele, T. P. (2018). Periodontal cell mechanotransduction. Open Biology, 8(9), 180053.
Dame, Z. T., Aziat, F., Mandal, R., Krishnamurthy, R., Bouatra, S., Borzouie, S., et al. (2015). The human saliva metabolome. Metabolomics, 11(6), 1864–1883.
Foresta, C., Ruzza, G., Mioni, R., Guarneri, G., Gribaldo, R., Meneghello, A., et al. (1984). Osteoporosis and decline of gonadal function in the elderly male. Hormones, 19(1), 18–22.
Fosdick, L., & Piez, K. (1953). Chemical studies in periodontal disease: X. Paper chromatographic investigation of the putrefaction associated with periodontitis. Journal of Dental Research, 32(1), 87–100.
García-Villaescusa, A., Morales-Tatay, J. M., Monleón-Salvadó, D., González-Darder, J. M., Bellot-Arcis, C., & Almerich-Silla, J. M. (2018). Using NMR in saliva to identify possible biomarkers of glioblastoma and chronic periodontitis. PLoS ONE, 13(2), e0188710.
Gardner, A., Parkes, H. G., Carpenter, G. H., & So, P.-W. (2018). Developing and standardizing a protocol for quantitative proton nuclear magnetic resonance (1H NMR) spectroscopy of saliva. Journal of Proteome Research, 17(4), 1521–1531.
Gharbia, S. E., & Shah, H. N. (1991). Pathways of glutamate catabolism among Fusobacterium species. Microbiology, 137(5), 1201–1206.
Higham, S., & Edgar, W. (1989). Effects of Parafilm® and cheese chewing on human dental plaque pH and metabolism. Caries Research, 23(1), 42–48.
Kaner, D., Soudan, M., Zhao, H., Gaßmann, G., Schönhauser, A., & Friedmann, A. (2017). Early healing events after periodontal surgery: Observations on soft tissue healing, microcirculation, and wound fluid cytokine levels. International Journal of Molecular Sciences, 18(2), 283.
Kertesz, M. A. (2000). Riding the sulfur cycle–metabolism of sulfonates and sulfate esters in Gram-negative bacteria. FEMS Microbiology Reviews, 24(2), 135–175.
Kilian, M., Chapple, I. L. C., Hannig, M., Marsh, P. D., Meuric, V., Pedersen, A. M. L., et al. (2016). The oral microbiome–an update for oral healthcare professionals. British Dental Journal, 221(10), 657.
Kim, J. J., Kim, C. J., & Camargo, P. M. (2013). Salivary biomarkers in the diagnosis of periodontal diseases. Journal of the California Dental Association, 41(2), 119.
Kolenbrander, P. E., & London, J. (1993). Adhere today, here tomorrow: Oral bacterial adherence. Journal of Bacteriology, 175(11), 3247.
Kornman, K. S., Page, R. C., & Tonetti, M. S. (1997). The host response to the microbial challenge in periodontitis: Assembling the players. Periodontology, 14(1), 33–53.
Markley, J. L., Anderson, M. E., Cui, Q., Eghbalnia, H. R., Lewis, I. A., Hegeman, A. D., et al. (2007). New bioinformatics resources for metabolomics. Biocomputing, 2007, 157–168.
Marsh, P. D., Do, T., Beighton, D., & Devine, D. A. (2016). Influence of saliva on the oral microbiota. Periodontology, 70(1), 80–92.
Melcher, A. (1976). On the repair potential of periodontal tissues. Journal of Periodontology, 47(5), 256–260.
Mombelli, A. (2018). Microbial colonization of the periodontal pocket and its significance for periodontal therapy. Periodontology, 76(1), 85–96.
Omahony, S., Clarke, G., Borre, Y., Dinan, T., & Cryan, J. (2015). Serotonin, tryptophan metabolism and the brain-gut-microbiome axis. Behavioural Brain Research, 277, 32–48.
Page, R. C., & Kornman, K. S. (1997). The pathogenesis of human periodontitis: An introduction. Periodontology, 14(1), 9–11.
Page, R. C., & Schroeder, H. E. (1976). Pathogenesis of inflammatory periodontal disease. A summary of current work. Laboratory Investigation: A Journal of Technical Methods and Pathology, 34(3), 235–249.
Ratcliff, P. A., & Johnson, P. W. (1999). The relationship between oral malodor, gingivitis, and periodontitis. A review. Journal of Periodontology, 70(5), 485–489.
Reynolds, J. J., & Meikle, M. C. (1997). Mechanisms of connective tissue matrix destruction in periodontitis. Periodontology, 14(1), 144–157.
Singh, M. P., Saxena, M., Saimbi, C. S., Arif, J. M., & Roy, R. (2017). Metabolic profiling by 1H NMR spectroscopy of saliva shows clear distinction between control and diseased case of periodontitis. Metabolomics, 13(11), 137.
Susin, C., Fiorini, T., Lee, J., De Stefano, J. A., Dickinson, D. P., & Wikesjö, U. M. (2015). Wound healing following surgical and regenerative periodontal therapy. Periodontology, 68(1), 83–98.
Takahashi, N. (2005). Microbial ecosystem in the oral cavity: Metabolic diversity in an ecological niche and its relationship with oral diseases. International Congress Series. Amsterdam: Elsevier.
Takahashi, N., & Yamada, T. (2000). Pathways for amino acid metabolism by Prevotella intermedia and Prevotella nigrescens. Oral Microbiology and Immunology, 15(2), 96–102.
van der Ploeg, J. R., Eichhorn, E., & Leisinger, T. (2001). Sulfonate-sulfur metabolism and its regulation in Escherichia coli. Archives of Microbiology, 176(1–2), 1–8.
Wishart, D. S., Knox, C., Guo, A. C., Eisner, R., Young, N., Gautam, B., et al. (2009). HMDB: A knowledgebase for the human metabolome. Nucleic Acids Research, 37, D603.
Acknowledgements
The authors are thankful for the grant funded by ICMR, New Delhi (Budget Allotment letter no.-5/4/2-7-12-NCD-II). Manvendra Pratap Singh also expresses his gratitude for the award of the fellowship. Manuscript Communication Number: IU/R&D/2018-MCN000453.
Funding
The authors are thankful for the Grant funded by ICMR, New Delhi (Budget Allotment letter no.-5/4/2-7-12-NCD-II).
Author information
Authors and Affiliations
Contributions
MS, CSS, and RR designed the study. MPS has conducted the experiments. MPS, CSS and RR analyzed the data. The initial draft was written by MPS. CSS, MHS, and RR edited and revised the paper. Project administration of the study has carried under CSS and RR. All authors carefully read and agree to be accountable for all aspects of the work.
Corresponding authors
Ethics declarations
Conflict of interest
The authors have no potential conflict of interest. The disclosure of a potential conflict of interest in the prescribed format has been obtained from all the authors.
Ethical approval
The study was ethically approved and the work was performed in strict accordance with the guidelines of Institutional Ethical Committee of the institute. The selected patients were fully informed and their consents were taken well before the investigations (Ethical approval No.- B-07: CBMR/EMP/IEC/3/26-02-2011). The authors: Manvendra Pratap Singh, Mona Saxena, Charanjit S. Saimbi, Mohammed Haris Siddiqui, and Raja Roy are aware of ethical policy.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Singh, M.P., Saxena, M., Saimbi, C.S. et al. Post-periodontal surgery propounds early repair salivary biomarkers by 1H NMR based metabolomics. Metabolomics 15, 141 (2019). https://doi.org/10.1007/s11306-019-1593-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s11306-019-1593-3