
Abstract
Objectives
The sella turcica is an important component situated in the mid-third of the cranial fossa. Knowledge about its normal morphologies and dimensions may play a crucial role in diagnosing underlying pathologies. The present study aimed to analyze the principal morphological shapes of the sella turcica, measure its linear dimensions, and determine whether any correlations exist between its dimensions and body mass index (BMI) in subjects in a North Indian population.
Methods
The study was conducted on 100 subjects (50 men; 50 women) who underwent cone-beam computed tomography scans at our Oral Medicine and Radiology Department. The subjects had an age range of 20–60 years. The morphology of the sella turcica was examined according to age and various measurements were taken to determine its size. Possible correlations between the dimensions of the sella turcica and BMI were evaluated by statistical analysis.
Results
In the present study, 69% of the subjects had a normal morphology. No uniform increases in length, width, and depth of the sella turcica were observed with aging. When Pearson correlation coefficients were calculated, no strong correlations were found between the dimensions of the sella turcica and BMI. A mild correlation was seen between the length and width of the sella turcica.
Conclusion
No significant correlations were found between the dimensions of the sella turcica and BMI in the present study. These findings may have arisen through the small sample size, and thus further studies with larger groups of subjects are warranted.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The name “sella turcica” is derived from a Latin word meaning “Turkish chair” and describes a saddle-shaped depression [1]. The sphenoid bone is situated between the frontal, temporal, and occipital bones at the base of the skull. It comprises a central body with paired greater and lesser wings that spread laterally and two pterygoid plates at the junctions of the body and the greater wing. The central part of the middle cranial fossa is formed by the body of the sphenoid bone [2]. The sella turcica is positioned in a depression lying on the intracranial surface of the body of the sphenoid bone that is bounded by the tuberculum sella and dorsum sella anteroposteriorly. Two anterior and two posterior clinoid processes project over the pituitary fossa [3, 4]. The anterior clinoid processes are formed by medial and anterior prolongations of the lesser wing of the sphenoid bone, and the terminations of the dorsum sella are present in the form of posterior clinoid processes [5]. The fossa has a unique relationship with the enveloped pituitary gland. There are reports of a larger sella turcica in a hyperfunctioning pituitary gland and a smaller sella turcica in a hypofunctioning pituitary gland [6, 7]. A theory that the pituitary can serve as a functional matrix for the sella turcica can be based on these findings, because increased growth of the sella turcica must follow increased growth of the pituitary gland. The pituitary is a master gland that secretes hormones including prolactin, growth hormones, and adrenocorticotrophic hormone. These hormones affect the growth and development of individuals. With this background, we hypothesize that there may be correlations between the size of the sella turcica and body mass index (BMI). The sella turcica is usually well demarcated by a thin dense white curve on lateral cephalograms, and is readily traceable for metric analysis, making it as an outstanding source of information for identification of pathologies related to the pituitary gland [8]. Furthermore, the sella turcica is quite stable because its morphology does not show much variation after 12 years of age [9]. Clinicians should be well acquainted with the normal radiographic anatomy and morphologic variability of this area, to distinguish and investigate aberrations that may reflect pathological conditions. Thus, any data obtained regarding these aspects will be very useful for detecting abnormalities in this anatomic area. Most studies related to sella turcica shapes and morphometric analyses have been performed with the aim of creating a baseline database containing computed tomography (CT) images and lateral cephalograms.
The aims of the present study were to analyze the predominant morphological shape of the sella turcica, measure its linear dimensions, and determine whether any correlations exist between its dimensions and BMI in subjects in a North Indian population.
Materials and methods
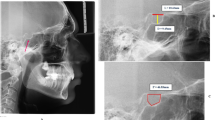
This was a prospective study conducted on 100 subjects (50 men, 50 women) who underwent cone-beam CT scans at our Oral Medicine and Radiology Department. All procedures were carried out in accordance with the ethical standards of the Helsinki Declaration of 1964 and later versions. Informed consent was obtained from all patients for being included in the study. All patients were referred for CBCT scans to evaluate other pathologies, including dental implant surgery, tumors, cysts, and embedded teeth. The scans were carried out using an Orthophos SL 3D CBCT machine (Sirona Dental Systems GmbH, Bensheim, Germany; effective radiation dose: 68–1073 µSv) with the patient’s Frankfort plane parallel to the floor. All images were evaluated in a darkened quiet room with dual monitors (S2240L; Dell, Round Rock, TX, USA; resolution: 1920 × 1080). Each viewing session was limited to 30 min. Care was taken to ensure that 24 h elapsed between sessions. For intraexaminer calibration and determination of the reliability and reproducibility of sella turcica measurements, the images were evaluated by the same observer for a second time after 2 weeks. The subjects were divided into five different groups according to age. To determine the variation in sella turcica shapes, the different morphological appearances were described as normal, irregular, oblique, pyramidal, and double-contoured (Fig. 1). The normal form of the sella turcica was defined as saddle-shaped. All morphometric measurements were performed using three parameters on the sagittal section closest to the mid-sagittal section. The morphometric parameters were (Fig. 2): sella length (SL), the length was measured as the distance from the tuberculum sella to the tip of the dorsum sella; sella width (SW), the anteroposterior width was measured as a line drawn from the tuberculum sella to the furthest point on the posterior inner wall of the fossa; sella depth (SD), the depth was measured perpendicular from the above line to the deepest point on the floor. BMI was defined as weight in kilograms divided by square of the height in meters (kg/m2).

Various shapes of the sella turcica

Morphometric measurements of the sella turcica
The obtained data were evaluated using Statistical Package for the Social Sciences software (version 20.0; IBM Corp., Armonk, NY, USA). Descriptive data were presented as mean ± standard deviation. An independent-samples t test was used for paired groups when comparing parametric values. Correlation analyses among the groups were performed using Pearson’s correlation test. Statistical significance in intergroup comparisons was set at p < 0.05.
Results
The subjects included in the study had an age range of 20–60 years, with a mean age of 40 years. The results for the intraclass correlation coefficient (ICC) reflected the reliability of the intraobserver ratings, and indicated that the observer provided similar ratings in the repeated observations for each measurement. The ICC scores for the measurements for SL, SW, and SD were 0.96, 0.95, and 0.97, respectively. The morphology of the sella turcica appeared to be normal in the majority of subjects (69%), regardless of sex and age. An oblique-shaped sella turcica was found in 14%, a double-contoured sella turcica was present in 9%, and a pyramidal and irregular-shaped sella turcica was observed in 4% (Table 1). The morphological measurements are shown in Table 2. The mean SL was 9.29 ± 1.37 mm in males, 9.02 ± 1.26 mm in females, and 9.15 ± 1.31 mm in the total population. The mean SW was 9.73 ± 1.29 mm in males, 9.35 ± 1.43 mm in females, and 9.54 ± 1.37 mm in the total population. The mean SD was 8.39 ± 1.19 mm in males and 7.81 ± 1.15 mm in females, and 8.10 ± 1.20 mm in the total population. No uniform increases in SL, SW, and SD were observed with aging (Table 3). SL and SW did not differ significantly between males and females, but a significant difference was seen in SD (p < 0.05; Table 2). When the Pearson correlation coefficients were calculated, no strong correlations were found between the dimensions of the sella turcica and BMI (Table 4). A mild correlation was seen between SL and SW (Table 4).
Discussion
The sella turcica is a vital component of the middle cranial fossa. Knowledge about its normal sizes and shapes can help clinicians to identify aberrations and sometimes detect underlying pathologies [10, 11]. The present study was designed to provide novel insights into the morphometric characteristics of the sella turcica, which can be highly variable among different populations. In 1922 study by Gordon and Bell [12], the sella turcica was classified into circular, oval, and flattened or saucer shaped. According to the study, a circular or oval-shaped sella turcica was the most prevailing morphology in the sample, but as the shapes were quite general and broadly classified, it was difficult to place some cases into one of the three categories. In the present study, five different types of sella turcica shape were described (normal, irregular, pyramidal, double-contoured, oblique), with the outcome that approximately 69% of subjects had a normal-shaped sella turcica and 31% had various aberrations. These findings are consistent with those reported by Axelsson et al. [13]. Alkofide [14] described that a normal-shaped sella turcica was observed in almost 67% of subjects, and found no significant correlations with sex, age, and skeletal type. Similar results were reported by Kiran et al. [8] and Shah et al. [15], wherein 70 and 66% of subjects had a normal-shaped sella turcica, respectively. Nagaraj et al. [16] found morphological variations of the sella turcica in 53.5% of their study population, which was not consistent with the present study.
Statistical analysis of sella turcica sizes have been documented in the literature, with typical size ranges of 4–12 mm for the vertical dimension and 5–16 mm for the anteroposterior dimension [17]. When the linear dimensions of length, depth, and width of the sella turcica in the present study were compared with other investigations [13, 18], differences between the measurements were noted. A microsurgical anatomical study on 250 sphenoidal blocks obtained from cadavers of different ages was performed by Quaknine and Hardy [18], who concluded that the average length of the sella turcica was 12 mm, the anteroposterior diameter (width) was 8 mm, and the average height (depth) was 6 mm. When compared with the present findings, their mean dimensions for width and depth were smaller and that for length was larger than those in our North Indian population. These differences could be due to the differences in sample sizes and age groups included in the studies. Choi et al. [19] concluded that the linear dimensions of the sella turcica showed a positive linear tendency until 25 years of age, with no significant increases in sella turcica size after 26 years of age. In our study, no linear increases in SL and SW were seen, but an increase was observed in SD. The size of the sella turcica was also examined longitudinally by Axelsson et al. [13], who evaluated a Norwegian population with an age range of 6–21 years. Their results demonstrated that the length remained almost constant throughout the observation period, while the depth and diameter increased with age.
No significant differences with sex were found in the present study in terms of sella turcica size. Similar findings were described by Israel [20], who concluded that the sella turcica sizes in young adult males and females were almost the same. According to the results of Shah et al. [15], no significant differences in sella turcica sizes were found between males and females or among different skeletal types.
No strong correlations were observed between the dimensions of the sella turcica and BMI of our subjects. No similar studies comparing these factors in North Indian populations were found in the literature, and thus further studies need to be conducted regarding this aspect.
In conclusion, the present study is the first of its kind in a North Indian population and is a useful initiative to use the sella turcica for identification of underlying pathologies of the pituitary gland and to examine whether any correlations are present between the dimensions of the sella turcica and BMI. Previous reports support evidence of a larger sella turcica in a hyperfunctioning pituitary gland and a smaller sella turcica in a hypofunctioning pituitary gland, suggesting the possibility that the pituitary gland acts as a functional matrix for the sella turcica. In our study, no significant correlations were found between the dimensions of the sella turcica and BMI which may be due to the small sample size. It should also be noted that the morphometry of the sella turcica and the BMI of subjects vary with ethnic backgrounds, evolutionary changes, growth hormone disturbances, and genetic influences. Hence, similar studies on larger scales need to be carried out in other regions to confirm the present findings.
References
Tekiner H, Acer N, Kelestimur F. Sella turcica: an anatomical, endocrinological, and historical perspective. Pituitary. 2015;18:575–8.
Kolagi S, Herur A, Patil G, Rairam GB. Complete sella turcica bridges prevalence and dimensions. J Anat Soc India. 2011;60:22–5.
Jones RM, Faqir A, Millett DT, Moos KF, McHugh S. Bridging and dimensions of sella turcica in subjects treated by surgical-orthodontic means or orthodontics only. Angle Orthod. 2005;75:714–8.
Pisaneschi M, Kapoor G. Imaging the sella and parasellar region. Neuroimaging Clin N Am. 2005;15:203–19.
Chauhan P, Kalra S, Mongia SM, Ali S, Anurag A. Morphometric analysis of sella turcica in North Indian population: a radiological study. Int J Res Med Sci. 2014;2:521–6.
Anandhi KS, Kumar AS, Kumari MCI. Abnormal small sella—a case report. J Anat Soc India. 2009;58:13–5.
Keleştimur F. Sheehan’s syndrome. Pituitary. 2003;6:181–8.
Kiran CS, Ramaswamy P, Santosh N, Smitha B, Satish A. Radio-morphometric analysis of sella turcica in the South Indian Population: a digital cephalometric study. Arab J Forensic Sci Forensic Med. 2017:517–23.
Norton LA, Melsen B. Functional appliances. In: Melsen B, editor. Current controversies in orthodontics. Chicago: Quintessence Publishing; 1991. pp. 103–30.
Chen JK, Tang JF, Du LS, Li H. Radiologic analysis of 540 normal Chinese sella turcica. Chin Med J (Engl). 1986;99:479–84.
Lang J. Structure and postnatal organization of heretofore uninvestigated and infrequent ossifications of the sella turcica region. Acta Anat (Basel). 1977;99:121–39.
Gordon MB, Bell AL. A roentgenographic study of the sella turcica in normal children. N Y State J Med. 1922;22:54–9.
Axelsson S, Storhaug K, Kjær I. Post-natal size and morphology of the sella turcica. Longitudinal cephalometric standards for Norwegians between 6 and 21 years of age. Eur J Orthod. 2004;26:597–604.
Alkofide EA. The shape and size of the sella turcica in skeletal class I, class II and class III Saudi subjects. Eur J Orthod. 2007;29:457–63.
Shah AM, Bashir U, Ilyas T. The shape and size of the sella turcica in skeletal class I, II, and III in patients presenting at Islamic International Dental Hospital, Islamabad. Pak Oral Dent J. 2011;31:104–10.
Nagaraj T, et al. The size and morphology of sella turcica: a lateral cephalometric study. J Med Radiol Pathol Surg. 2015;1:3–7.
Silverman FN. Roentgen standards fo-size of the pituitary fossa from infancy through adolescence. Am J Roentgenol Radium Ther Nucl Med. 1957;78:451–60.
Quaknine GE, Hardy J. Microsurgical anatomy of the pituitary gland and the pituitary gland and the sellar region. 1. The pituitary gland. Am Surg. 1987;53:285–90.
Choi WJ, Hwang EH, Lee SE. The study of shape and size of normal sella turcica in cephalometric radiographs. Korean J Oral Maxillofac Radiol. 2001;31:43–9.
Israel H. Continuing growth in sella turcica with age. Am J Roentgenol Radium Ther Nuclear Med. 1970;108:516–27.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
Vidisha Gargi, Sasankoti Mohan Ravi Prakash, K. Nagaraju, Sangeeta Malik, Sumit Goel, and Swati Gupta declare that they have no conflict of interest.
Human rights statement and informed consent
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1964 and later versions. Informed consent was obtained from all patients for being included in the study.
Rights and permissions
About this article

Cite this article
Gargi, V., Ravi Prakash, S.M., Nagaraju, K. et al. Radiological analysis of the sella turcica and its correlations with body mass index in a North Indian population. Oral Radiol 35, 184–188 (2019). https://doi.org/10.1007/s11282-018-0337-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11282-018-0337-9