
Abstract
Objectives
This study was performed to assess the morphological appearance, incidence of bridging, and linear dimensions of the sella turcica (ST) in Bosnian and Iraqi subjects, and to identify associations of sex, age, and racial group with the size of the ST.
Methods
The digital standardised lateral cephalograms of 360 Bosnian and Iraqi patients (116 female, 64 male; age range 8–28 years) were retrospectively analysed. The following ST-related parameters were analysed on the lateral cephalograms: sella morphology, sella bridging, and sella size. The data were correlated with sex, age, and race.
Results
The ST exhibited a normal morphology in most subjects of both races (86.7%). The frequency of partial bridging was found in 38.9 and 37.2% of Bosnian and Iraqi subjects, respectively. A significant correlation was detected between the length of the ST and sex in both the Bosnian and Iraqi subjects (p < 0.05). A direct correlation was present between patient age and the size of the ST in both races at the 0.01 and 0.001 levels for depth, length, and diameter. When race was compared with sella size, a significant difference was found in the length and depth of the ST (p < 0.001).
Conclusions
Similarities were found between Bosnian and Iraqi subjects in the morphology, incidence of bridging, and linear dimensions of the ST. Length was the only parameter significantly associated with sex, age, and racial group. These findings could be used as reference standards for studying the ST in both races.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Several anatomical landmarks on lateral cephalometric radiographs have been established as reference points during tracing to measure and position the mandible and maxilla either in relation to the cranial base or in relation to each other. These landmarks serve as a diagnostic tool during evaluation of orthodontic treatment outcomes [1, 2]. The sella turcica (ST) is an important saddle-shaped anatomical structure on the lateral cephalometric radiograph [3]. The sella point, which is located in the middle of the ST, is one of the most commonly used cranial landmarks for cephalometric tracing. The ST possesses the anterior and posterior clinoid processes [4] and central hypophyseal fossa, situated in the superior part of the sphenoid bone. The deepest part of the ST houses the hypophysis (pituitary gland) in the cranial base [1, 5, 6]. On a lateral skull radiograph, the ST exhibits a varied anatomical structure with respect to size and shape and has been classified into three types: round, oval, and flat. Round and oval STs are the most common types [2, 7]. Various methods to measure the size of the ST on radiographs have been suggested [8,9,10]. The sella bridge or calcification of the interclinoid ligament is a fused bony structure that forms as a result of abnormal development in the anterior, middle, and posterior clinoid processes [4, 11]. An altered ST morphology, or ST bridging (STB), is present in some patients with severe craniofacial deviations, congenital malformations, spina bifida [12], dental anomalies, and other disorders and syndromes or is considered a normal variant of the ST [13].
Various authors have studied the shape and size of the ST in the populations in their own countries [1, 4, 14,15,16]. However, variations in the ST dimensions among the Bosnian and Iraqi populations have not been investigated. Therefore, this study was performed to elucidate the morphological appearance, incidence of STB, and linear dimensions of the ST in Bosnian and Iraqi subjects and identify any possible associations of sex, age, and racial group with the size of the ST. The null hypothesis was that association exists between the linear dimensions of the ST and sex, age, or racial group.
Subjects and methods
The study group comprised 360 subjects, among whom 116 were female and 64 were male from each racial group. The selection of all subjects was based on the inclusion and exclusion criteria described below.
The data were divided into two groups according to the subjects’ age: 8–14 and 15–28 years. The mean age in each of these age groups in both races is presented in Table 1. The selection criteria for these age groups were based on previous studies showing no significant change in the morphology of the ST after 12 years of age. Girls have finished their pubertal development by roughly 15 years of age; the size of the ST in young adult men and women is reportedly almost the same except during pregnancy [1, 7, 15].
Study data were gathered at two different geographic locations: Banja Luka and Sulaimani cites. Banja Luka is the largest city located in the northwestern part of Bosnia and Herzegovina [17]. Sulaimani city is located in northeast Iraq, and most of the population is of Kurdish origin [18]. The details of the study subjects, the data collection sites, and the instruments used for cephalometric radiographs are presented in Table 2.
All cephalometric radiographs were reviewed and measured by the principal author. Digital lateral cephalograms with records from the Bosnian and Iraqi subjects were collected electronically. Radiographs are now commonplace, and referrals, along with photographs, are being increasingly communicated via email [19, 20].
Inclusion and exclusion criteria
The inclusion criteria were a clinically healthy status, no severe malformations, and treatment by orthodontics alone without surgical intervention if class III malocclusion was present. The exclusion criteria were cleft lip and palate, craniofacial syndromes, trauma, multi-reagent chemotherapy, and poor-quality images [13].
Size of the ST
The linear dimensions of the ST were measured using a digitising WinCeph® version 8.0 software (Rise Corporation, Sendai, Japan) according to the method described by Silverman [21]. Radiographs were of good quality and clearly showed the ST anatomy. The imaging analysis software was calibrated to account for any differences in magnification due to radiographic technique and/or use of the cephalostat. A bone filtre was applied for improved contrast and more accurate location of structures. Four landmark points of the ST were carefully placed: the tuberculum sella (anterior point of the contour of the ST), the dorsum sella (furthest point on the posterior wall of the ST), the sella floor (deepest point on the base of the pituitary fossa), and the posterior clinoid (most anterior point of the posterior clinoid process).
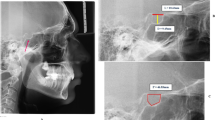
The software calibrated linear measurements of the sella length and interclinoid distance, indicating the distance between the tuberculum sella and dorsum sella as well as the position, diameter, and depth of the diaphragm sellae as shown in Fig. 1.

Normal sella turcica morphology and reference lines used for measuring sella size. TS tuberculum sella, DS dorsum sella, BPF base of the pituitary fossa, black line length of sella, dashed line diameter of sella, dotted line depth of sella, line a sella length/interclinoid distance, line b diameter of diaphragm sellae, line c depth of diaphragm sellae
Shape of the ST
The morphology of the ST was classified into three groups: U shape (dorsum and tubercle of the ST are at the same height), J shape (ST tubercle is at a lower position in relation to the dorsum), and flat shape (ST depth is minimal) [7, 22].
STB
STB was classified as no calcification, partial calcification, and complete calcification according to previously applied criteria [13, 23]. Partial calcification includes extension but no fusing of the anterior and posterior clinoid processes. Full bridging was defined as radiographically visible fusion (ribbon-like fusion) of the anterior and posterior structures of the ST.
Reliability of measurements
To reduce bias due to intra-examiner variability, 40 lateral cephalometric radiographs were randomly selected (20 from each racial group) and re-evaluated by the same operator 4 weeks after the initial analysis. The intraclass correlation coefficient (ICC) was used in this study. The ICC estimates and their 95% confidence intervals were calculated using SPSS v.20.0 (IBM Corp., Armonk, NY, USA) based on a mean-rating, consistency, two-way mixed-effects model. The ICC is a widely used index of measurement reliability to evaluate the reproducibility of the readings [24].
Statistical analyses
The statistical software SPSS v.20.0 (IBM Corp.) was used for statistical analysis of the data. Descriptive statistics such as mean values and standard deviations were generated for every parameter. The Welch unequal variance t test was used to compare the mean differences in ST measurements between sexes and between the different age groups. The effects of race, sex, and age on the dimensions of the ST were evaluated using multiple linear regression models. The significance level was calculated at the p < 0.05 level.
Results
The reliability statistics for the ST length, depth, and diameter in Bosnian subjects were 0.98, 0.98, and 0.96, respectively. The reliability statistics for Iraqi length, depth, and diameter in Iraqi subjects were 0.99, 0.92, and 0.92, respectively. These results indicate excellent reproducibility of the remeasured radiographs. Based on the 95% confidence interval of the ICC estimate, values of < 0.50, 0.50–0.75, 0.75–0.90, and > 0.90 were indicative of poor, moderate, good, and excellent reliability, respectively [24].
Shape of the ST
Three different shapes of the ST were observed: U, J, and flat shapes. Most of the Bosnian and Iraqi subjects showed a U-shaped morphology of the ST (86.7%). A small proportion of Bosnian and Iraqi patients had a flat or shallow ST (1.1 and 3.9%, respectively) (Table 3).
Assessment of STB in the study groups showed three distinct types: no STB, partial STB, and full STB. The incidence of no STB in the Bosnian and Iraqi subjects was 53.9 and 57.2%, respectively. The incidence of partial STB in the Bosnian and Iraqi subjects was 38.9 and 37.2%, respectively. Finally, full STB occurred more frequently in the Bosnian subjects (7.2%) than Iraqi subjects (5.6%), as shown in Table 3.
Size of the ST
Sex was significantly related to the length of the ST in both study groups (p < 0.05) (Table 4).
The ST linear dimensions by age group are shown in Table 5. A statistically significant association was found between the size of the ST and age in both the Bosnian (p < 0.01) and Iraqi patients (p < 0.001).
Table 6 shows the results of one-way analysis of variance for the effects of race on sella length, depth, and diameter in the Bosnian and Iraqi subjects irrespective of age or sex. Sella length and depth were significant in both races, and the difference was highly significant (p < 0.001). Multiple linear regression models were applied to investigate the associations between linear measures of ST (length, depth, and diameter) and race, adjusted for patients’ sex and age. The results showed that after the adjustment, the associations between length and all factors were statistically significant. The depth and diameter were significantly associated with sex and age, respectively (Table 7).
Discussion
This retrospective study was performed to reveal the morphological appearance, incidence of bridging, and linear dimensions of the ST in Bosnian and Iraqi subjects and identify any possible associations of sex, age, or race with the size of the ST. A study of this type does not appear to have been performed previously.
Cephalometric morphometric studies of the ST have long been performed by many researchers, but they have mainly been restricted to one population [1, 14,15,16, 25]. In the present study, Bosnian and Iraqi subjects were selected and compared. The radiographic diagnosis of the shape of the ST was performed according to the criteria established in the literature and classified into three morphological variations: U, J, and flat [1, 7, 22, 26]. A greater frequency of a U- and J-shaped ST has been described in normal patients [7, 22, 26]. The results of the present study showed that the frequency of a U-shaped ST was identical in the Bosnian and Iraqi patients (86.7%). It seems that a flat-shaped ST is less likely to occur in both races compared with previous studies [7, 22, 26]. The flat type is reportedly the least frequent [27].
Knowledge of the prevalence of STB is essential in the prognosis of surgical procedures of the ST. There is a clear tendency toward a greater frequency of partial bridging in Bosnian and Iraqi patients with no clinical manifestations. Partial bridging was found to occur in 13.6% of Peruvian patients [23]; this is a markedly lower incidence than in Bosnian (38.9%) and Iraqi subjects (37.2%). The highest incidence of partial bridging was recorded in patients from Texas (38.4%) [28]. The occurrence of STB is also possible in healthy populations, with a range of 1.75–22.00% reported in anatomical and radiographic studies [15, 27, 29,30,31]. The frequency of full STB observed in our study was 7.2 and 5.6% in the Bosnian and Iraqi subjects, respectively. The highest incidence of full STB was recorded in Anatolian subjects (34.17%) [11]. No STB was found in Bangladeshi subjects [31]. A higher percentage of STB was reported in medically compromised patients and those with tooth anomalies [12, 23]. STB was present in 18.6% of patients with severe craniofacial disorders, 13.0% of those with Williams syndrome [32], 7.3% of those undergoing orthodontic treatment, and 16.7% of those undergoing surgical orthodontic treatment [33]; a range of 0.7–43.3% was observed in patients with skeletal class I, II, and III malocclusion [1, 15, 23]. The effect of STB on the pituitary gland is not known [12].
Selected radiographs were classified according to the two populations in this study to determine the association between the size of the ST and sex. A statistically significant difference was detected between males and females in the length of the ST in each study group. The current study outcome is not consistent with previous studies performed in Iraqi [7], Saudi Arabian [1], Pakistani [14], Iranian [15], Nigerian [34, 35], Malaysian [22], Maharashtrian [36], Indian [16], and Bangladeshi [31] populations, among which no notable associations were found between sex and ST length, depth, or diameter. When our study sample was compared with an Iraqi sample in another study by Hasan et al. [7], the sella length was the only variable found to be significantly different between the sexes, being larger in males in the present study. This discrepancy can be attributed to factors such as ethnicity, the use of different landmarks and radiographic techniques, and the degree of radiographic enlargement. A study in Greece showed that the anterior sella height was larger in males than in females [25].
Statistically significant correlations were found between the dimensions of the ST and age groups. The ST was consistently larger in older than younger subjects. This result is in agreement with previously reported studies showing a direct and significant correlation between advanced age and the length, depth, and diameter of the ST [1, 16, 22, 27]. One study of Iranian subjects showed that the length and depth were not affected by age, while the diameter was significantly correlated with increasing age [15]. In contrast to our findings, previous measurements in Iraqi subjects showed no significant differences in linear dimensions between the older and younger age groups [7]. This may be attributed to the same reasons explained earlier.
Significant differences were found between the two racial groups and the length and depth of the ST (Table 6). To date, no evidence has been found associating race with the linear dimensions of the ST. Comparisons between the two groups were made using regression analyses. Length is generally seen as a factor strongly related to race, sex, and age. Sex was significantly related to length and depth, while age was significantly related to length and diameter (p < 0.001). The present findings seem to be consistent with other studies, which showed that age was significantly related to the change in the length and diameter when comparing skeletal classifications and linear dimensions of the ST [1]. However, in a study conducted by Valizadeh et al. [15], the associations of sex and age with the size of the ST were not statistically significant.
We also compared our findings with the current global data regarding the ST size (Table 8) [1, 4, 7, 14,15,16, 22, 25, 26, 31, 35]. The linear dimensions in 180 subjects in each racial group in our study were lower than those in Saudi Arabian [1] and Pakistani [14] subjects. Iranian [15] and Turkish [4] subjects showed a greater depth and diameter than in our subjects, and the largest sella length was recorded among Nigerian patients [35]. It might be helpful to assess these linear dimensions and morphological shapes of the ST in other populations.
Measurement of the ST and examination of its morphology are vital for evaluation of pituitary gland pathology. The sella shape and size may be used as reference standards for Bosnian and Iraqi subjects, particularly those of the Kurdish ethnic group, when studying ST morphology.
Within the limitations of the current study, the following conclusions can be drawn. The most striking observation was that similarities were present between the Bosnian and Iraqi subjects in morphology, the incidence of bridging, and the linear dimensions of the ST. The length and depth of the ST were significantly associated with race. The length of the ST is the only parameter significantly associated with race, sex, and age, justifying rejection of the null hypothesis. The associations among these factors should be investigated in future studies.
References
Alkofide EA. The shape and size of the sella turcica in skeletal class I, class II, and class III Saudi subjects. Eur J Orthod. 2007;29(5):457–63.
Tekiner H, Acer N, Kelestimur F. Sella turcica: an anatomical, endocrinological, and historical perspective. Pituitary. 2015;18(4):575–8.
Neha SM, Shetty VS, Shetty S. Sella size and jaw bases—is there a correlation? Cont Clin Dent. 2016;7(1):61–6.
Marsan G, Oztas E. Incidence of bridging and dimensions of sella turcica in class I and III Turkish adult female patients. World J Orthod. 2009;10(2):99–103.
Norton N. Netter’s head and neck anatomy for dentistry. Philadelphia: Elsevier Saunders; 2011.
Iván E, Pérez I, Allison K, Chávez A, Ponce D. Frequency of sella turcica bridge and clinoid enlargement in lateral cephalometric plain film radiography from Peruvians. Int J Morphol. 2013;31(2):373–7.
Hasan HA, Alam MK, Abdullah YJ, Nakano J, Yusa T, Yusof A, et al. 3DCT morphometric analysis of sella turcica in Iraqi population. J Hard Tissue Biol. 2016;25(3):227–32.
Abdel-Kader HM. Sella turcica bridges in orthodontic and orthognathic surgery patients. A retrospective cephalometric study. Au Orthod J. 2007;23(1):30–5.
Keats T, Lusted L. Atlas of roentgenographic measurement. St. Louis: Mosby; 1990.
Friedland B, Meazzini MC. Incidental finding of an enlarged sella turcica on a lateral cephalogram. Am J Orthod Dentofac Orthop. 1996;110(5):508–12.
Peker T, Anil A, Gulekon N, Turgut HB, Pelin C, Karakose M. The incidence and types of sella and sphenopetrous bridges. Neuro Rev. 2006;29(3):219–23.
Becktor JP, Einersen S, Kjaer I. A sella turcica bridge in subjects with severe craniofacial deviations. Eur J Orthod. 2000;22(1):69–74.
Leonardi R, Barbato E, Vichi M, Caltabiano M. A sella turcica bridge in subjects with dental anomalies. Eur J Orthod. 2006;28(6):580–5.
Shah AM, Bashir U, Ilyas T. The shape and size of the sella turcica in skeletal class I, II and III in patients presenting at Islamic International Dental Hospital, Islamabad. Pakistan Oral Dent J. 2011;31(1):104–10.
Valizadeh S, Shahbeig S, Mohseni S, Azimi F, Bakhshandeh H. Correlation of shape and size of sella turcica with the type of facial skeletal class in an Iranian group. Iranian J Radiol. 2015;12(3):e16059.
Sathyanarayana H, Kailasam V, Chitharanjan A. The size and morphology of sella turcica in different skeletal patterns among South Indian population: a lateral cephalometric study. J In Orthod Soc. 2013;47(4):266–71.
Hussein S, Noori A. Prevalence of oral mucosal changes among 13 year old children in Sulaimani city, Iraq. Sulaimani Dent J. 2014;1:5–9.
Lakic B, Racic M, Vulic D. Retrospective analysis of the role and performance of family medicine versus emergency medical services in the pre-hospital management of patients with AMI in Banja Luka. Acta Med Acad. 2016;45(1):10–8.
Chang ZC, Hu FC, Lai E, Yao CC, Chen MH, Chen YJ. Landmark identification errors on cone-beam computed tomography-derived cephalograms and conventional digital cephalograms. Am J Orthod Dentofac Orthoped. 2011;140(6):e289–e97.
Damstra J, Huddleston Slater JJ, Fourie Z, Ren Y. Reliability and the smallest detectable differences of lateral cephalometric measurements. Am J Orthod Dentofac Orthoped. 2010;138(5):546.e541–8 (discussion 546–7).
Silverman F. Roentgen standards for size of the pituitary fossa from infancy through adolescence. Am J Roentgenol. 1957;78(3):45–60.
Hasan H, Alam M, Yusof A, Mizushima H, Kida A, Osuga N. Size and morphology of sella turcica in Malay populations: a 3D CT study. J Hard Tissue Biol. 2016;25(3):313–20.
IPérez I, Chávez A, Ponce D. Frequency of sella turcica bridge and clinoid enlargement in lateral cephalometric plain film radiography from Peruvians. Int J Morphol. 2013;31(2):373–7.
Koo T, Li M. A guideline of selecting and reporting intraclass correlation coefficients for reliability research. J Chiropr Med. 2016;15(2):155–63.
Andredaki M, Koumantanou A, Dorotheou D, Halazonetis DJ. A cephalometric morphometric study of the sella turcica. Eur J Orthod. 2007;29(5):449–56.
Ruiz C, Wafae N, Wafae G. Sella turcica morphometry using computed tomography. Eur J Anat. 2008;12:47–50.
Axelsson S, Storhaug K, Kjaer I. Post-natal size and morphology of the sella turcica. Longitudinal cephalometric standards for Norwegians between 6 and 21 years of age. Eur J Orthod. 2004;26(6):597–604.
Cederberg RA, Benson BW, Nunn M, English JD. Calcification of the interclinoid and petroclinoid ligaments of sella turcica: a radiographic study of the prevalence. Orthod Craniofac Res. 2003;6(4):227–32.
Kantor ML, Norton LA. Normal radiographic anatomy and common anomalies seen in cephalometric films. Am J Orthod Dentofac Orthoped. 1987;91(5):414–26.
Meyer-Marcotty P, Weisschuh N, Dressler P, Hartmann J, Stellzig-Eisenhauer A. Morphology of the sella turcica in Axenfeld-Rieger syndrome with PITX2 mutation. J Oral Pathol Med. 2008;37(8):504–10.
Islam M, Alam M, Yusof A, Kato I, Honda Y, Kubo K, et al. 3D CT study of morphological shape and size of sella turcica in Bangladeshi population. J Hard Tissue Biol. 2017;26(1):1–6.
Axelsson S, Storhaug K, Kjaer I. Post-natal size and morphology of the sella turcica in Williams syndrome. Eur J Orthod. 2004;26(6):613–21.
Jones RM, Faqir A, Millett DT, Moos KF, McHugh S. Bridging and dimensions of sella turcica in subjects treated by surgical-orthodontic means or orthodontics only. Angle Orthod. 2005;75(5):714–8.
Olubunmi O, Yinka O, Oladele O, Adimchukwunaka G, Afees O. An assessment of the size of sella turcica among adult Nigerians resident in Lagos. Int J Med Imaging. 2016;4(3):12–6.
Osunwoke E, Mokwe C, Amah-Tariah F. Radiologic measurements of the sella turcica in an adult Nigerian population. Int J Pharm Sci Res. 2014;4:115–7.
Chavan S, Kathole M, Katti A, Herekar N. Radiological analysis of sella turcica. Int J Recent Trends Sci Technol. 2012;4(1):36–40.
Acknowledgements
This work was supported by the Chinese Scholarship Council (CSC) under Grant number CSC-2016368012.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
Fenik Kaml Muhammed, Adil O. Abdullah, Zhwan Jamal Rashid, Tamara Pusic, Mohammed F. Shbair, and Yi Liu declare that they have no conflict of interest.
Human rights statement
All procedures followed were in accordance with the ethical standards of the responsible committee (institutional and national) and with the Helsinki Declaration of 1964 and later versions. The study protocol was approved by the Local Research Ethics Committee of Stomatology of China Medical University (Shenyang, People’s Republic of China). This article does not contain any studies with animal subjects performed by any of the authors.
Informed consent
Informed consent was not needed in the study.
Rights and permissions
About this article

Cite this article
Muhammed, F.K., Abdullah, A.O., Rashid, Z.J. et al. Morphology, incidence of bridging, and dimensions of sella turcica in different racial groups. Oral Radiol 35, 127–134 (2019). https://doi.org/10.1007/s11282-018-0328-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11282-018-0328-x