
Abstract
Objective
To review recent use of three-dimensional (3D) imaging, specifically cone-beam computed tomography (CBCT), in the analysis of the upper airway for diagnosis or treatment outcomes in patients with sleep-disordered breathing (SDB).
Types of studies reviewed
Literature review of relevant medical and dental studies utilizing 3D imaging to assess the upper airway.
Results
Imaging of the upper airway provided insight into potential areas of obstruction. Accessibility of CBCT to dentists is reflected in several applications of upper airway diagnosis, treatment planning, and different treatment outcomes, as well as association with craniofacial development. However, multiple deficiencies in image acquisition, 3D reconstruction, and analysis are evident.
Practical implications
The role of CBCT in the analysis of the upper airway is growing; however, critical limitations remain. An understanding of these limitations, clarification of misconceptions, and improvements in analysis methods are required to ensure proper use and development of CBCT.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Visualization and calculation of the upper airway dimensions are of interest, because anatomical obstructions increase airway resistance, which may contribute to abnormal craniofacial growth. In addition to its contribution to diagnosing obstruction, airway imaging provides an objective tool with which to measure changes in the airway after therapy or correlate airway dimensions with craniofacial growth. The preferred radiological technique with which to evaluate upper airways with structural or functional abnormalities is determined by the patient’s clinical condition and the available diagnostic expertise and resources. For the past decade, cone-beam computed tomography (CBCT) has been advocated as a new tool that can be used to assess the upper airway. With the emerging role of dentists in the diagnosis or treatment of patients with sleep-disordered breathing (SDB) syndromes, including obstructive sleep apnea (OSA), a considerable amount of studies have utilized this tool in several capacities. These studies are herein reviewed along with other 3D imaging modalities.
Literature review
Upper airway imaging modalities
Imaging of the upper airway and associated dentofacial structures has traditionally been performed using lateral cephalometric radiography. Characteristic skeletal, oral, and pharyngeal differences have been described between patients with OSA and their normal peers. Cephalometry is informative and readily available; however, it possesses the limitations of any two-dimensional (2D) radiographic procedure: magnification, superimposition of surrounding structures, and the inability to visualize changes in the mediolateral dimension. With good to fair sensitivity (61–75%) and poor specificity (41–55%), lateral cephalography is considered a screening tool for adenoid hypertrophy that likely needs to be augmented with advanced three-dimensional (3D) imaging in complex cases such as patients with SDB [1, 2].
The upper airway extends from the tip of the nose to the superior aspect of the trachea and can be visualized with advanced imaging modalities such as magnetic resonance imaging (MRI), multidetector computed tomography (MDCT), and cone-beam CT (CBCT) scans, which usually include the jaws, teeth, cranial base, spine, and facial soft tissues. Of these three imaging modalities, MRI is the most desirable, because it produces no ionizing radiation and provides information on the airway space and soft tissues that form and surround the airway. However, MRI is not readily accessible to dentists, and static image sequences take a long time to complete. Although MDCT provides high-resolution images of the bone anatomy and soft tissue by means of its thin-collimation, fan-shaped beam, it subjects patients to high amounts of radiation (around 860 µSv for a 12-cm-high field of view) [3] and is not accessible to dentists. CBCT, however, is readily available to dentists and provides 10 times less ionizing radiation than does MDCT by means of its large, cone-shaped X-ray beam [3]. CBCT has been found to be more reliable than nasoendoscopy in evaluating the adenoid size and more effective than MDCT in measuring the volume of an air space surrounded by soft tissue; in addition, it allows for precise measurements because of its small isotropic pixels [4, 5]. Caveats to CBCT include its suboptimal resolution due to scatter radiation, lack of soft tissue delineation, and harmful ionizing radiation if the protocol is not adequately customized to fit the needs of each patient.
Supine vs. upright position
MDCT and MRI are performed while the patient is in the supine position, thus allowing imaging, while the patient is awake or asleep. Most CBCT units, on the other hand, acquire images with the patient in the seated position. Evidence shows that the airway dimensions decrease in the supine versus seated position because of the backward–downward position of the tongue, soft palate, and hyoid bone due to gravity [6, 7]. However, transitioning from wakefulness to sleep introduces additional neuromuscular factors that further affect airway dimensions through different stages of sleep or as the patient changes between different postures during sleep (right or left supine, semi-supine, or prone) [8]. Therefore, imaging the patient in the supine position should not be considered to “mimic” the sleep position.
Methods of airway analysis
The literature contains several studies in which different parts of the upper airway were analyzed by various methods. Such analyses are either static (linear, surface area, cross-sectional area, or volume) or dynamic [assessment of airflow by means of computational fluid dynamics (CFD)]. CFD is a computerized method of airflow analysis in which numerical methods and algorithms are used to simulate air or fluid flow. This technique is becoming more prominent, because it allows the clinician to obtain more detailed information about airflow with outcome measures such as resistance, velocity, changes in pressure, and turbulence [9]. However, CFD is complex, computationally demanding, and time-consuming because of the complex shape of the upper airway [9].
Most recent analyses require a 3D model of the upper airway reconstructed from a 3D imaging modality (MDCT, CBCT, or MRI). In addition, the segmentation technique plays an important role in depicting cross sections and volumes in 3D analysis. Segmentation involves the extraction of structural information of particular interest from surrounding images for visualization or characterization of the anatomy or pathology by means of 3D reconstruction. This process can be carried out manually, automatically, or semi-automatically. Manual segmentation requires the operator to manually trace the boundaries or adjust the pixel gray threshold in the area of interest. Thus, it requires a long time to perform; however, it provides accurate 3D rendering of the airway. Automatic segmentation is usually offered by commercial software products and is time-efficient, but it is not as accurate as manual segmentation, because such software products tend to “combine” the gray threshold levels of the entire area of interest rather than customize them depending on the location.
Applications of upper airway imaging
The most common applications of 3D analysis are comparison of airway dimensions between patients with SDB and controls, assessment of airway changes after therapy, and association of airway parameters with craniofacial growth.
Patients with SDB vs. controls
Recent studies have shown that anatomical properties determined from CT, MRI, or CBCT images correlate well with the severity of OSA by different means of measurements. Barkdull et al. [10] examined cross-sectional MDCT images of patients with OSA and found that a smaller retrolingual airway correlated with the severity of OSA as measured by the apnea–hypopnea index (AHI). MDCT and CBCT studies comparing patients with OSA versus controls revealed that the presence of OSA was associated with an increase in airway length, smaller minimum cross-sectional area, and elliptically shaped airways [11–13]. Several MRI studies have revealed that patients with OSA had larger soft tissues (adenoids, tonsils, and soft palate) [14–17], a narrower retropalatal airway space [16–18], a smaller mandibular volume [16], and larger fluctuations in tidal breathing [19]. Using fast MRI, a few studies analyzed the dynamic motion of the upper airway of patients with OSA and revealed transverse distention, pharyngeal collapse, and narrowing during tidal breathing [17, 20–23].
Application of CFD on 3D models generated from MRI [24] or MDCT [25, 26] has shown that flow resistance in the pharynx and pressure drops at the adenoid and tonsils were higher in patients with OSA than controls and were correlated with the AHI.
Assessment of treatment outcomes
Although adenotonsillectomy (AT) is the most common and first line of treatment for pediatric SDB, only one study [27] involved measurement of the upper airway changes after AT using MRI. Few MRI studies have revealed lingual tonsil hypertrophy as a cause of either residual OSA [17, 28] or significant residual adenoid tissue and volume increases in the tongue and soft palate after AT in obese children with OSA [27].
In MDCT and CBCT studies, maxillary or maxillomandibular advancement increased the minimum cross-sectional area and pharyngeal airway volume [29–33]. Conversely, a significant decrease was noted in the volumes of the oropharyngeal and hypopharyngeal airways after surgical mandibular set-back and in the oropharyngeal airway after bimaxillary surgery in patients with skeletal class III malocclusions [34–39]. While rapid maxillary expansion has been shown to increase the nasal or pharyngeal airway in a few studies [40–43], other studies revealed no changes in the oropharyngeal airway [44–50]. Using CBCT, a volume increase in the oropharynx was documented after twin block [51], crossbow (XBow) [52], and Herbst [53] appliance therapies.
Application of CFD to 3D models generated from MDCT [54], CBCT [55], or MRI [56] has revealed reduced air turbulence and pressure gradients along the pharyngeal airway and a strong correlation with reductions in the AHI after maxillomandibular advancement and AT. Nasal ventilation reportedly improved by rapid maxillary expansion due to a reduction in nasal resistance and the negative pressure in the pharynx as well as a reduction in velocity variations as shown by the application of CFD to CBCT-reconstructed airway models [41, 57, 58].
Association with craniofacial growth
The correlation between airway measures in CBCT and skeletal patterns is contradictory. Several studies have shown that the volume and several cross-sectional areas in at least one part of the pharyngeal airway differ among different skeletal patterns [59–64], with the pharyngeal airway being largest in patients with skeletal class III malocclusion (mandibular prognathism) or a low mandibular angle, followed by class I, and then class II (mandibular retrognathism) or a high mandibular angle. Other studies have shown no difference in airway measures among different skeletal malocclusion patterns [65–67].
Discussion
This review has shown that most CBCT studies of the upper airway used either manual or automatic segmentation of the pharynx [68]. Few attempts were made to create automatic segmentation algorithms; however, these were developed or tested only for the pharyngeal airway or required further tests to increase precision [68–70]. As the interest in airway imaging using CBCT has grown, a large influx of new commercial software programs or applications specific for airway analysis have been noted [68]. However, a few points are worth discussing, as outlined below.
Reasons to scan the airway
For analysis of the dimensions of the upper airway, especially in patients with or at risk of SDB, nasoendoscopy remains the standard of care [71]. Diagnosis of SDB or OSA using CBCT is a goal that is yet to be accomplished, and the use of CBCT for the sole purpose of airway analysis is not encouraged. Rather, secondary analysis of the upper airway can be carried out using CBCT scans acquired for other reasons for patients in whom the conventional radiography failed to provide adequate information, such as patients who have undergone orthognathic surgery or those with maxillary constriction, significant anteroposterior or vertical jaw discrepancies, or asymmetry. In patients with jaw disproportion and SDB symptoms who undergo AT, nasal surgery, maxillary expansion, or orthognathic surgery, the use of CBCT can support, not substitute for, other diagnostic information gathered from the otolaryngology and sleep medicine perspectives.
Gray thresholding
In CBCT, which has a low signal-to-noise ratio, the reliability and accuracy of automatic segmentation techniques or commercial software products are important. When such programs are tested and deemed reliable or accurate, it may be a result of using geometric phantoms consisting of cylinders or simple shapes as the “reference” or “gold standard” [72, 73]. A more representative reference would be manual segmentation of the true upper airway rather than a cylindrical phantom. Similarly, it is expected that automatic segmentation of the pharynx only closely represents manual segmentation, thus over-representing its reliability. For example, when the nasal cavity was included in the testing of automatic segmentation of a common software, the upper airway volume differed by 42% against manual segmentation, a result deemed unacceptable [74]. This is attributed to the fact that automatic segmentation relies on global thresholding, which refers to the process of selecting a range of gray threshold values that represent a tissue of interest. Gray values for the airway in CBCT are expected to be in the lower range (e.g., −700 or −3000). Although selecting a range for air in the pharyngeal airway could work, that range cannot and should not be extended to the nasal cavity. The gray values of air found in the pharynx are not as distinct in the nasal cavity because of volume averaging from surrounding thin bony boundaries or the mucous lining of the nose. Bone and mucous membranes increase the “low” gray values of the nasal airway and thus will not adequately fit into the selected pharyngeal airway threshold. The operator would then have to increase the range of the gray threshold to include the nose at the expense of causing over- or under-segmentation in other areas (consider Fig. 1). Furthermore, the range of the gray threshold cannot and should not be fixed, even for the pharyngeal airway or for specific software. This is because the gray value of a pixel depends not only on the tissue contrast but also on other factors, such as the type of CBCT machine used; the scanning parameters, which control the amount of radiation/signal; scattered radiation; metal artifact; patient motion; or machine calibration [75]. All factors will cast a change to that pixel value, and it is, therefore, unrealistic to standardize an airway threshold. Including the nasal cavity in the validation of segmentation methods is a more frequently used technique in the otolaryngology literature [76–78]. Semiautomatic segmentation of the nose and paranasal sinuses reduced the segmentation time by 78.1% in one study; however, the reduction to 3.5 h was still considered impractical for clinical and research purposes [78].

Axial cone-beam computed tomography image with “global thresholding.” The image shows a selected gray value range that perfectly segments the nasopharyngeal airway but “under-segments” in the nasal meatus (close-up image on the right) and “over-segments” the anterior part of the nose. Manual adjustment is necessary to include all airway passages without impacting the segmentation accuracy of others
Analysis beyond the pharynx
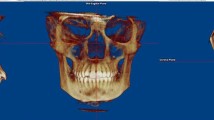
Although adenotonsillar hypertrophy is considered the main cause of airway obstruction in children and the condition toward which treatment is geared, other causes of nasal airway narrowing exist. During its journey from the nose to the lungs, air is affected by multiple anatomic factors such as turbinate hypertrophy, concha bullosa (pneumatized nasal turbinates), and a deviated nasal septum (Fig. 2). In patients with SDB, these factors result in the delivery of limited airflow to a susceptible pharynx, further compromising airflow to the lungs. Although these abnormalities are clearly depicted in CBCT images, studies evaluating or addressing such nasal obstructions are very limited.

Coronal cone-beam computed tomography image sections of the nasal cavity. Deviation of the nasal septum with concha bullosa (left) and a bone spur (right)
Analysis beyond size
The previous reports show multiple and inconsistent measurements of the upper airway that may or may not correlate with each other [79]. Upper airway analysis using CBCT cannot be accurately performed by single linear measurements, and volume alone does not depict the morphology of the airway. Because the upper airway exhibits a complex geometry, its assessment should reflect size and shape parameters; the conventional measures such as linear measurements, area, and volume may fall short with respect to the latter (Fig. 3).

Three-dimensional airway models generated from cone-beam computed tomography. Both models are similar in volume but significantly differ in shape; the left is a normal airway and the right is of a patient with obstructive sleep apnea
Serial images
When longitudinal CBCT analysis of the upper airway is carried out, most studies do not consider changes in the patient’s head position at the time of the scan. Furthermore, subdividing the pharyngeal airways into different segments appears erroneous and inconsistent and relies on unstable or unclear soft tissue landmarks. This will, in turn, impact the location and size of the linear, area, and volume measurements selected to analyze the upper airway. An accurate and reliable registration or superimposition technique must be used in longitudinal CBCT studies, and division of the pharyngeal airway should be based on reliable planes and represent the true anatomic definitions of each segment. Ideally, each dividing plane should be created by three reproducible points within osseous landmarks (such as the base of the odontoid and inferoanterior point of C3). The nasopharynx marks the pharyngeal airway posterior to the nasal cavity, usually contains the adenoids, and is bounded by the posterior nasal aperture anterosuperiorly and the tip of the soft palate inferiorly. The oropharynx marks the pharyngeal airway posterior to the oral cavity, contains the tonsils, and is bordered by the tongue anteriorly, tip of the soft palate superiorly, and tip of the epiglottis inferiorly. Finally, the hypopharynx marks a small part of the pharynx, is bordered by the tip of epiglottis superiorly, and opens into the larynx and esophagus inferiorly (Fig. 4).

Sagittal cone-beam computed tomography image showing anatomic sections of the upper airway. NP nasopharynx, OP oropharynx, HP hypopharynx, SP soft palate, (Asterisk) epiglottis
Neck and tongue
Because the pharyngeal airway is essentially composed of fat and muscles, it is expected to deform due to pressure from the cervical vertebrae posteriorly or the tongue anteriorly. In one study, the impact of neck flexion on serial airway imaging was evaluated using lateral cephalograms, where a 10° change in the craniocervical inclination (indicated by a line through C2 and the sella–nasion line) or a 10-mm change in the C3-to-menton distance increased the pharyngeal airway space (anteroposterior line from the back of the tongue to the post-pharyngeal wall) by about 4 mm [80]. More recently, neck flexion producing a >3-mm interdistance at C2–C3 (in at least one axis) was shown to be likely to produce larger discrepancies of up to about 5 mm between localized parts of the airway models over time [81]. Similar changes in volume, surface area, and point-based analysis (which produces a distance color map) were found in patients with tongue malpositioning; and example is shown in Fig. 5.

Sagittal cone-beam computed tomography images of a patient who underwent adenotonsillectomy. (Top): Before, (Middle): after surgery, and (Bottom): superimposition of before and after surgery. Note large registration error due to neck flexion and tongue curling and perfect registration in the cranial base, nasal cavity, and maxilla. Although the patient reported significant relief of symptoms after surgery, the airway dimensions appeared smaller after surgery because of neck and tongue malpositioning
CBCT airway scanning protocols should be chosen to maximize resolution, reduce the radiation dose, reduce the scan time to minimize motion (patients should be instructed to bite on the posterior teeth and relax the tongue against the anterior teeth), and avoid neck flexion.
Discussion
3D imaging of the upper airway provides insights into potential areas of obstruction and serves as an objective tool for airway measurements. Although upper airway imaging using CBCT shows the 3D aspects of airway anatomical obstruction during wakefulness, it provides only a “snapshot” of the head. It is an isolated observation of the upper airway and by no means dissects the complexity of airway function in the realm of SDB. Technical factors that define the image resolution obtained by CBCT, along with the operator’s expertise in segmentation, can vary widely and thus impact the dimensions of the 3D models generated. Patient movement, swallowing, breathing, neck flexion, or tongue malpositioning during the scan are inevitable, especially in younger patients, and methods to secure the head and neck and control the tongue position during the scan should be explored. Until then, upper airway changes with tongue or neck malpositioning, especially in the oropharyngeal airway, should be assessed with caution.
We can acknowledge that upper airway CBCT is advantageous in the assessment of SDB if it is part of an interdisciplinary approach by a team of specialists in orthodontics, pediatric sleep medicine, and otolaryngology for diagnosis, treatment planning, and assessment of treatment progress or outcomes.
To advance the use of CBCT in airway imaging, its limitations need to be addressed and future research must steer away from global measures and global segmentation. Global measures fail to reflect localized characteristics of the airway, and a gray threshold range in the pharynx does not fit the nose and cannot be replicated in other scans. Rather, it should be geared toward innovations in stabilizing the patient’s neck and tongue during the scan, improving imaging protocols, extending the analysis into the nasal cavity, and exploring new and meaningful analyses. Only then can we identify risk factors for SDB or predict treatment outcomes based on 3D-CBCT airway models.
References
Major MP, Flores-Mir C, Major PW. Assessment of lateral cephalometric diagnosis of adenoid hypertrophy and posterior upper airway obstruction: a systematic review. Am J Orthod Dentofac Orthop. 2006;130:700–8.
Major MP, Saltaji H, El-Hakim H, Witmans M, Major P, Flores-Mir C. The accuracy of diagnostic tests for adenoid hypertrophy: a systematic review. J Am Dent Assoc. 2014;145:247–54.
Ludlow JB, Ivanovic M. Comparative dosimetry of dental CBCT devices and 64-slice CT for oral and maxillofacial radiology. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2008;106:930–8.
Aboudara C, Nielsen I, Huang JC, Maki K, Miller AJ, Hatcher D. Comparison of airway space with conventional lateral headfilms and 3-dimensional reconstruction from cone-beam computed tomography. Am J Orthod Dentofac Orthop. 2009;135:468–79.
Yamashina A, Tanimoto K, Sutthiprapaporn P, Hayakawa Y. The reliability of computed tomography (CT) values and dimensional measurements of the oropharyngeal region using cone beam CT: comparison with multidetector CT. Dentomaxillofac Radiol. 2008;37:245–51.
Van Holsbeke CS, Verhulst SL, Vos WG, De Backer JW, Vinchurkar SC, Verdonck PR, et al. Change in upper airway geometry between upright and supine position during tidal nasal breathing. J Aerosol Med Pulm Drug Deliv. 2014;27:51–7.
Sutthiprapaporn P, Tanimoto K, Ohtsuka M, Nagasaki T, Iida Y, Katsumata A. Positional changes of oropharyngeal structures due to gravity in the upright and supine positions. Dentomaxillofac Radiol. 2008;37:130–6.
Tiotiu A, Mairesse O, Hoffmann G, Todea D, Noseda A. Body position and breathing abnormalities during sleep: a systematic study. Pneumologia. 2011;60:216–21.
Van Holsbeke C, Vos W, Van Hoorenbeeck K, Boudewyns A, Salgado R, Verdonck PR, et al. Functional respiratory imaging as a tool to assess upper airway patency in children with obstructive sleep apnea. Sleep Med. 2013;14:433–9.
Barkdull GC, Kohl CA, Patel M, Davidson TM. Computed tomography imaging of patients with obstructive sleep apnea. Laryngoscope. 2008;118:1486–92.
Abramson Z, Susarla S, August M, Troulis M, Kaban L. Three-dimensional computed tomographic analysis of airway anatomy in patients with obstructive sleep apnea. J Oral Maxillofac Surg. 2010;68:354–62.
Ogawa T, Enciso R, Memon A, Mah J, Clark G. Evaluation of 3D airway imaging of obstructive sleep apnea with cone-beam computed tomography. Stud Health Technol Inform. 2005;111:365–8.
Sato K, Shirakawa T, Sakata H, Asanuma S. Effectiveness of the analysis of craniofacial morphology and pharyngeal airway morphology in the treatment of children with obstructive sleep apnoea syndrome. Dentomaxillofac Radiol. 2012;41:411–6.
Arens R, McDonough JM, Costarino AT, Mahboubi S, Tayag-Kier CE, Maislin G, et al. Magnetic resonance imaging of the upper airway structure of children with obstructive sleep apnea syndrome. Am J Respir Crit Care Med. 2001;164:698–703.
Arens R, Sin S, Nandalike K, Rieder J, Khan UI, Freeman K, et al. Upper airway structure and body fat composition in obese children with obstructive sleep apnea syndrome. Am J Respir Crit Care Med. 2011;183:782–7.
Cappabianca S, Iaselli F, Negro A, Basile A, Reginelli A, Grassi R, et al. Magnetic resonance imaging in the evaluation of anatomical risk factors for pediatric obstructive sleep apnoea-hypopnoea: a pilot study. Int J Pediatr Otorhinolaryngol. 2013;77:69–75.
Donnelly LF, Shott SR, LaRose CR, Chini BA, Amin RS. Causes of persistent obstructive sleep apnea despite previous tonsillectomy and adenoidectomy in children with down syndrome as depicted on static and dynamic cine MRI. Am J Roentgenol. 2004;183:175–81.
Fregosi RF, Quan SF, Kaemingk KL, Morgan WJ, Goodwin JL, Cabrera R, et al. Sleep-disordered breathing, pharyngeal size and soft tissue anatomy in children. J Appl Physiol. 2003;95:2030–8.
Arens R, Sin S, McDonough JM, Palmer JM, Dominguez T, Meyer H, et al. Changes in upper airway size during tidal breathing in children with obstructive sleep apnea syndrome. Am J Respir Crit Care Med. 2005;171:1298–304.
Donnelly LF, Surdulescu V, Chini BA, Casper KA, Poe SA, Amin RS. Upper airway motion depicted at cine MR imaging performed during sleep: comparison between young patients with and those without obstructive sleep apnea. Radiology. 2003;227:239–45.
Abbott MB, Donnelly LF, Dardzinski BJ, Poe SA, Chini BA, Amin RS. Obstructive sleep apnea: MR imaging volume segmentation analysis. Radiology. 2004;232:889–95.
Persak SC, Sin S, McDonough JM, Arens R, Wootton DM. Noninvasive estimation of pharyngeal airway resistance and compliance in children based on volume-gated dynamic MRI and computational fluid dynamics. J Appl Physiol. 2011;111:1819–27.
Ikeda K, Ogura M, Oshima T, Suzuki H, Higano S, Takahashi S, et al. Quantitative assessment of the pharyngeal airway by dynamic magnetic resonance imaging in obstructive sleep apnea syndrome. Ann Otol Rhinol Laryngol. 2001;110:183–9.
Wootton DM, Luo H, Persak SC, Sin S, McDonough JM, Isasi CR, et al. Computational fluid dynamics endpoints to characterize obstructive sleep apnea syndrome in children. J Appl Physiol. 2014;116:104–12.
Van Holsbeke C, De Backer J, Vos W, Verdonck P, Van Ransbeeck P, Claessens T, et al. Anatomical and functional changes in the upper airways of sleep apnea patients due to mandibular repositioning: a large scale study. J Biomech. 2011;44:442–9.
Vos W, De Backer J, Devolder A, Vanderveken O, Verhulst S, Salgado R, et al. Correlation between severity of sleep apnea and upper airway morphology based on advanced anatomical and functional imaging. J Biomech. 2007;40:2207–13.
Nandalike K, Shifteh K, Sin S, Strauss T, Stakofsky A, Gonik N, et al. Adenotonsillectomy in obese children with obstructive sleep apnea syndrome: magnetic resonance imaging findings and considerations. Sleep. 2013;36:841–7.
Fricke BL, Donnelly LF, Shott SR, Kalra M, Poe SA, Chini BA, et al. Comparison of lingual tonsil size as depicted on MR imaging between children with obstructive sleep apnea despite previous tonsillectomy and adenoidectomy and normal controls. Pediatr Radiol. 2006;36:518–23.
Brunetto DP, Velasco L, Koerich L, Araújo MTDS. Prediction of 3-dimensional pharyngeal airway changes after orthognathic surgery: a preliminary study. Am J Orthod Dentofacial Orthop. 2014;146:299–309.
De Souza Carvalho ACG, Magro Filho O, Garcia IR, Araujo PM, Nogueira RLM. Cephalometric and three-dimensional assessment of superior posterior airway space after maxillomandibular advancement. Int J Oral Maxillofac Surg. 2012;41:1102–11.
Raffaini M, Pisani C. Clinical and cone-beam computed tomography evaluation of the three-dimensional increase in pharyngeal airway space following maxillo-mandibular rotation-advancement for class II-correction in patients without sleep apnoea (OSA). J Craniomaxillofac Surg. 2013;41:552–7.
Butterfield KJ, Marks PLG, McLean L, Newton J. Pharyngeal airway morphology in healthy individuals and in obstructive sleep apnea patients treated with maxillomandibular advancement: a comparative study. Oral Surg Oral Med Oral Pathol Oral Radiol. 2015;119:285–92.
Valladares-Neto J, Silva MAG, Bumann A, Paiva JB, Rino-Neto J. Effects of mandibular advancement surgery combined with minimal maxillary displacement on the volume and most restricted cross-sectional area of the pharyngeal airway. Int J Oral Maxillofac Surg. 2013;42:1437–45.
Park SB, Kim YI, Son WS, Hwang DS, Cho BH. Cone-beam computed tomography evaluation of short- and long-term airway change and stability after orthognathic surgery in patients with class III skeletal deformities: bimaxillary surgery and mandibular setback surgery. Int J Oral Maxillofac Surg. 2012;41:87–93.
Shin JH, Kim MA, Park IY, Park YH. A 2-year follow-up of changes after bimaxillary surgery in patients with mandibular prognathism: 3-dimensional analysis of pharyngeal airway volume and hyoid bone position. J Oral Maxillofac Surg. 2015;73:340.e1–9.
Gokce SM, Gorgulu S, Gokce HS, Bengi AO, Karacayli U, Ors F. Evaluation of pharyngeal airway space changes after bimaxillary orthognathic surgery with a 3-dimensional simulation and modeling program. Am J Orthod Dentofacial Orthop. 2014;146:477–92.
Hatab NA, Konstantinović VS, Mudrak JKH. Pharyngeal airway changes after mono- and bimaxillary surgery in skeletal class III patients: cone-beam computed tomography evaluation. J Craniomaxillofac Surg. 2014;43:491–6.
Li YM, Liu JL, Zhao JL, Dai J, Wang L, Chen JW. Morphological changes in the pharyngeal airway of female skeletal class III patients following bimaxillary surgery: a cone beam computed tomography evaluation. Int J Oral Maxillofac Surg. 2014;43:862–7.
Sears CR, Miller AJ, Chang MK, Huang JC, Lee JS. Comparison of pharyngeal airway changes on plain radiography and cone-beam computed tomography after orthognathic surgery. J Oral Maxillofac Surg. 2011;69:e385–e94.
Iwasaki T, Saitoh I, Takemoto Y, Inada E, Kakuno E, Kanomi R, et al. Tongue posture improvement and pharyngeal airway enlargement as secondary effects of rapid maxillary expansion: a cone-beam computed tomography study. Am J Orthod Dentofac Orthop. 2013;143:235–45.
Iwasaki T, Saitoh I, Takemoto Y, Inada E, Kanomi R, Hayasaki H, et al. Evaluation of upper airway obstruction in class II children with fluid-mechanical simulation. Am J Orthod Dentofac Orthop. 2011;139:e135–e45.
Bouserhal J, Bassil-Nassif N, Tauk A, Will L, Limme M. Three-dimensional changes of the naso-maxillary complex following rapid maxillary expansion. Angle Orthod. 2014;84:88–95.
Smith T, Ghoneima A, Stewart K, Liu S, Eckert G, Halum S, et al. Three-dimensional computed tomography analysis of airway volume changes after rapid maxillary expansion. Am J Orthod Dentofac Orthop. 2012;141:618–26.
Zhao Y, Nguyen M, Gohl E, Mah JK, Sameshima G, Enciso R. Oropharyngeal airway changes after rapid palatal expansion evaluated with cone-beam computed tomography. Am J Orthod Dentofac Orthop. 2010;137:S71–8.
Chang Y, Koenig LJ, Pruszynski JE, Bradley TG, Bosio JA, Liu D. Dimensional changes of upper airway after rapid maxillary expansion: a prospective cone-beam computed tomography study. Am J Orthod Dentofacial Orthop. 2013;143:462–70.
Ribeiro ANC, De Paiva JB, Rino-Neto J, Illipronti-Filho E, Trivino T, Fantini SM. Upper airway expansion after rapid maxillary expansion evaluated with cone beam computed tomography. Angle Orthod. 2012;82:458–63.
El H, Palomo JM. Three-dimensional evaluation of upper airway following rapid maxillary expansion: a CBCT study. Angle Orthod. 2014;84:265–73.
Zeng J, Gao X. A prospective CBCT study of upper airway changes after rapid maxillary expansion. Int J Pediatr Otorhinolaryngol. 2013;77:1805–10.
Fastuca R, Zecca PA, Caprioglio A. Role of mandibular displacement and airway size in improving breathing after rapid maxillary expansion. Prog Orthod. 2014;15:40.
Kabalan O, Gordon J, Heo G, Lagravère MO. Nasal airway changes in bone-borne and tooth-borne rapid maxillary expansion treatments. Int Orthod. 2015;13:1–15.
Li L, Liu H, Cheng H, Han Y, Wang C, Chen Y, et al. CBCT evaluation of the upper airway morphological changes in growing patients of class ii division 1 malocclusion with mandibular retrusion using twin block appliance: a comparative research. PLoS One. 2014;9:e94378.
Erbas B, Kocadereli I. Upper airway changes after Xbow appliance therapy evaluated with cone beam computed tomography. Angle Orthod. 2014;84:693–700.
Iwasaki T, Takemoto Y, Inada E, Sato H, Saitoh I, Kakuno E, et al. Three-dimensional cone-beam computed tomography analysis of enlargement of the pharyngeal airway by the Herbst appliance. Am J Orthod Dentofac Orthop. 2014;146:776–85.
Yu CC, Hsiao HD, Lee LC, Yao CM, Chen NH, Wang CJ, et al. Computational fluid dynamic study on obstructive sleep apnea syndrome treated with maxillomandibular advancement. J Craniofac Surg. 2009;20:426–30.
Huynh J, Kim D, McQuilling M. Pharyngeal airflow analysis in obstructive sleep apnea patients pre- and post-maxillomandibular advancement surgery. J Fluids Eng. 2009;131:091101–11.
Luo H, Sin S, McDonough JM, Isasi CR, Arens R, Wootton DM. Computational fluid dynamics endpoints for assessment of adenotonsillectomy outcome in obese children with obstructive sleep apnea syndrome. J Biomech. 2014;47:2498–503.
Iwasaki T, Saitoh I, Takemoto Y, Inada E, Kanomi R, Hayasaki H, et al. Improvement of nasal airway ventilation after rapid maxillary expansion evaluated with computational fluid dynamics. Am J Orthod Dentofac Orthop. 2012;141:269–78.
Iwasaki T, Takemoto Y, Inada E, Sato H, Suga H, Saitoh I, et al. The effect of rapid maxillary expansion on pharyngeal airway pressure during inspiration evaluated using computational fluid dynamics. Int J Pediatr Otorhinolaryngol. 2014;78:1258–64.
Abdelkarim A. A cone beam CT evaluation of oropharyngeal airway space and its relationship to mandibular position and dentocraniofacial morphology. J World Fed Orthod. 2012;1:e55–e9.
El H, Palomo JM. Airway volume for different dentofacial skeletal patterns. Am J Orthod Dentofac Orthop. 2011;139:e511–e21.
Alves M Jr, Franzotti ES, Baratieri C, Nunes LKF, Nojima LI, Ruellas ACO. Evaluation of pharyngeal airway space amongst different skeletal patterns. Int J Oral Maxillofac Surg. 2012;41:814–9.
Zheng ZH, Yamaguchi T, Kurihara A, Li HF, Maki K. Three-dimensional evaluation of upper airway in patients with different anteroposterior skeletal patterns. Orthod Craniofac Res. 2014;17:38–48.
Celikoglu M, Bayram M, Sekerci AE, Buyuk SK, Toy E. Comparison of pharyngeal airway volume among different vertical skeletal patterns: a cone-beam computed tomography study. Angle Orthod. 2014;84:782–7.
Claudino LV, Mattos CT, Ruellas ACDO, Sant Anna EF. Pharyngeal airway characterization in adolescents related to facial skeletal pattern: a preliminary study. Am J Orthod Dentofac Orthop. 2013;143:799–809.
Grauer D, Cevidanes LSH, Styner MA, Ackerman JL, Proffit WR. Pharyngeal airway volume and shape from cone-beam computed tomography: relationship to facial morphology. Am J Orthod Dentofac Orthop. 2009;136:805–14.
Alves PVM, Zhao L, O’Gara M, Patel PK, Bolognese AM. Three-dimensional cephalometric study of upper airway space in skeletal class II and III healthy patients. J Craniofac Surg. 2008;19:1497–507.
Di Carlo G, Polimeni A, Melsen B, Cattaneo PM. The relationship between upper airways and craniofacial morphology studied in 3D: a CBCT study. Orthod Craniofac Res. 2015;18:1–11.
Alsufyani NA, Flores-Mir C, Major PW. Three-dimensional segmentation of the upper airway using cone beam CT: a systematic review. Dentomaxillofac Radiol. 2012;41:276–84.
Shi H, Scarfe W, Farman A. Upper airway segmentation and dimensions estimation from cone-beam CT image datasets. Int J CARS. 2006;1:177–86.
Cheng I, Nilufar S, Flores-Mir C, Basu A. Airway segmentation and measurement in CT images. Conf Proc IEEE Eng Med Biol Soc. 2007;2007:795–9.
Parikh SR, Coronel M, Lee JJ, Brown SM. Validation of a new grading system for endoscopic examination of adenoid hypertrophy. Otolaryngol Head Neck Surg. 2006;135:684–7.
Weissheimer A, Menezes LMD, Sameshima GT, Enciso R, Pham J, Grauer D. Imaging software accuracy for 3-dimensional analysis of the upper airway. Am J Orthod Dentofac Orthop. 2012;142:801–13.
Ghoneima A, Kula K. Accuracy and reliability of cone-beam computed tomography for airway volume analysis. Eur J Orthod. 2013;35:256–61.
de Water VR, Saridin JK, Bouw F, Murawska MM, Koudstaal MJ. Measuring upper airway volume: accuracy and reliability of Dolphin 3D Software compared to manual segmentation in craniosynostosis patients. J Oral Maxillofac Surg. 2014;72:139–44.
Schulze R, Heil U, Gross D, Bruellmann DD, Dranischnikow E, Schwanecke U, et al. Artefacts in CBCT: a review. Dentomaxillofac Radiol. 2011;40:265–73.
Seo A, Chung SK, Lee J, Kim JI, Kim H. Semiautomatic segmentation of nasal airway based on collaborative environment. Proceedings of the International Symposium on Ubiquitous Virtual Reality ISUVR; 2010 July 7–10; Washington, DC, USA. doi:10.1109/ISUVR.2010.24.
Perchet D, Fetita C, Prêteux F. Three-dimensional reconstruction of upper airways from MDCT. Proceedings of SPIE5672, Image Processing: Algorithms and systems IV; 2005 March 8; San Jose, CA, USA. doi:10.1117/12.587741.
Tingelhoff K, Moral AI, Kunkel ME, Rilk M, Wagner I, Eichhorn KWG, et al. Comparison between manual and semi-automatic segmentation of nasal cavity and paranasal sinuses from CT images. Proceedings of the Annual International Conference of the IEEE Engineering in Medicine and Biology; 2007 August 23–26; Lyon, France. doi:10.1109/IEMBS.2007.4353592.
Alsufyani NA, Al-Saleh MA, Major PW. CBCT assessment of upper airway changes and treatment outcomes of obstructive sleep apnoea: a systematic review. Sleep Breath. 2013;17:911–23.
Muto T, Takeda S, Kanazawa M, Yamazaki A, Fujiwara Y, Mizoguchi I. The effect of head posture on the pharyngeal airway space (PAS). Int J Oral Maxillofac Surg. 2002;31:579–583.
Alsufyani NA, Dietrich NH, Lagravère MO, Carey JP, Major PW. Cone beam computed tomography registration for 3-D airway analysis based on anatomic landmarks. Oral Surg Oral Med Oral Pathol Oral Radiol. 2014;118:371–383.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
All authors have no conflict of interest.
This article does not contain any studies with human or animal subjects performed by any of the authors.
Rights and permissions
About this article

Cite this article
Alsufyani, N.A., Noga, M.L., Witmans, M. et al. Upper airway imaging in sleep-disordered breathing: role of cone-beam computed tomography. Oral Radiol 33, 161–169 (2017). https://doi.org/10.1007/s11282-017-0280-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11282-017-0280-1