
Abstract
Purpose
The association between tea consumption and kidney stones is inconsistent in observational studies. Thus, we performed a dose–response meta-analysis of prospective cohort studies and a two-sample Mendelian randomization (MR) analysis to identify this association.
Methods
The prospective cohort studies reporting the relationship between tea consumption and kidney stones were searched from PubMed, the Cochrane Library, EMBASE, and Web of Science from inception to December 1, 2023. For MR analysis, the summary-level data for tea consumption and kidney stones were extracted from the UK Biobank available data and the 8th release of the FinnGen consortium, respectively. The inverse-variance weighted (IVW) method was the primary analytical method.
Results
In our dose–response meta-analysis, four prospective cohort studies involving 1,263,008 participants were included, and tea consumption was found to have significant associations with kidney stones (RR: 0.80, 95% CI: 0.73–0.87). We also observed a substantially linear negative relationship between tea consumption and the risk of kidney stones. In MR analysis, the IVW method indicated that tea consumption was inversely associated with kidney stones (OR: 0.71, 95% CI: 0.53–0.94).
Conclusion
Our study confirmed a causal relationship between tea consumption and kidney stones, and higher tea consumption may reduce the risk of kidney stones.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Kidney stone is the most common urological disease affecting a large proportion of the population. Previous studies have shown that the prevalence of kidney stones in mainland China is 7.54%, and in the United States, approximately 11% of the population suffers from kidney stones [1, 2]. According to the latest Global Burden of Disease study, more than 115 million kidney stones occurred worldwide in 2019 [3]. In addition to high incidence rates, it is also characterized by high recurrence rates. It is estimated that about 50% of patients would relapse within 5 to 7 years after the first occurrence [4]. The high recurrence rate of kidney stones and the high rate of surgical intervention not only impose a huge economic burden but also seriously decline the quality of life for patients [5]. Therefore, prevention work is critical for kidney stones.
Previous studies have revealed that increased fluid intake could reduce the risk of kidney stones [6, 7]. As one of the most popular beverages worldwide, tea contains many bioactive components, which has attracted much attention for its potential health effects [8, 9]. Many studies have explored the association between tea consumption and kidney stones [10,11,12,13,14]. However, much of the evidence is equivocal and inconsistent. A meta-analysis based on 3 studies showed that the relationship between tea consumption and kidney stones was borderline nonlinear, with a 4% decrease in the risk of kidney stones for each 110 ml/day increase in tea consumption [15]. Nevertheless, most data in this review were derived from cross-sectional studies.
In observational studies, the results could be affected by confounders, reverse causation, and other biases. To avoid these limitations, we used Mendelian randomization (MR) analysis. MR is an approach in genetic epidemiology, which utilizes genetic variants as instrumental variables (IVs) to investigate the causal effect between exposure and outcome [16]. Like randomized controlled trials, the genetic variants are randomly assigned during meiosis. Furthermore, the development of disease and environmental factors cannot influence genetic variants. Consequently, this approach can reduce the impact of confounding factors and diminish reverse causality [16]. Two recent MR studies have demonstrated that obesity and diabetes can increase the risk of kidney stones, and coffee and caffeine consumption have been associated with a decreased risk of kidney stones [17, 18].
This study aims to comprehensively investigate the association between tea consumption and kidney stones. First, we performed a dose–response meta-analysis of cohort studies to quantify this association. Second, we used MR analysis to identify the potential causal association between tea consumption and kidney stones from a genetic perspective.
Method
Dose–response meta-analysis
Search strategy
This meta-analysis has been registered on the INPLASY website (number: INPLASY202330115), and it was reported following the PRISMA guidelines [19]. We systematically searched the relevant studies using PubMed, the Cochrane Library, EMBASE, and Web of Science through December 1, 2023. The search terms are shown in Supplementary Material 1. The references list of identified papers and review papers were also searched. Two authors independently selected the studies, and the studies met the following criteria were included in this meta-analysis: (1) the study was designed as a prospective cohort study; (2) the study investigated the association between tea consumption and kidney stones; (3) the study reported the distribution of person-years or total person-years, and (4) hazard ratio (HR) with 95% confidence intervals (CIs) were reported for at least 3 levels of tea consumption.
Data extraction
The data extraction processes and quality assessment were independently performed by two authors (Hao Yu and Zewu Zhu) and the disagreements were solved by a third author (Jian Wu). We collected the relevant data as follows from the full-text papers: the first author’s last name, publication year, country, the total number of participants, sex, total person-years, median follow-up years, the potential confounding factors adjusted in the multivariable analysis, and the HRs with 95% CIs for each level of tea consumption. The study quality was assessed using the Newcastle–Ottawa Scale (NOS) [20].
Mendelian randomization analysis
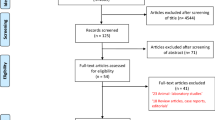
The study design overview is shown in Fig. 1B. We conducted a two-sample MR analysis utilizing publicly available genome-wide association study (GWAS) datasets. The original study had obtained ethical approval and informed consent.

Study design overview. A Flowchart of the literature search. B Analysis process of Mendelian randomization study
Genetic instruments for exposure
Like the previous study [21], we acquired IVs for tea consumption from the Neale Lab (http://www.nealelab.is/uk-biobank, GWAS round 2), which recruited 349,376 participants from the UK Biobank. All single-nucleotide polymorphisms (SNPs) associated with tea consumption at the genome-wide significance threshold (p < 5 × 10−8) were deemed as IVs. The clumping process (R2 < 0.001, clumping distance = 10,000 kb) was employed to confirm the independence of selected SNPs. Subsequently, 19 independent SNPs were identified, which was consistent with a prior study [21]. To eliminate potential pleiotropic effects, the phenotypes of each SNP were scrutinized through the PhenoScanner database, and SNPs associated with phenotypes linked to kidney stones (BMI [17], diabetes [17], coffee [18], and caffeine consumption [18]) were excluded. Moreover, we used F-statistic (F-statistic = Beta2/SE2) to evaluate the strength of IVs [22]. If F-statistic < 10, it was considered a weak instrument that could bias the results [23]. Consequently, SNPs with an F-statistic greater than 10 were ultimately selected.
Genetic summary data for kidney stones
In our study, the summary-level data for kidney and ureteral stones were extracted from the 8th release of the FinnGen consortium [24]. The 8th release of the FinnGen consortium data concluded 8,597 cases and 333,128 controls.
Statistical analysis
Dose–response meta-analysis
A random effect model was used to calculate the summary RR and 95% CI for the highest versus lowest level of tea consumption. In cohort studies, HRs could be considered equivalent to relative risks (RRs). We used the Cochran Q test and I2 statistic to evaluate the heterogeneity. Sensitivity analysis was conducted by sequentially omitting one study at a time to assess the stability of the results. We also performed a subgroup analysis based on geographic region to check for the potential source of heterogeneity. The publication bias could not be identified if less than 10 studies were included in the meta-analysis. Based on the method described by Greenland and Orsini et al. [25, 26], we further conducted a dose–response meta-analysis. This method requires the distribution of person-years. If the person-years in each exposure category were not reported, these data would be estimated from the total person-years. We used the midpoint of each category as the average level, since none of the selected studies provided a median or mean value. If the lowest category was open, we considered the lower boundary to be zero, while the highest category was open, we assumed the midpoint of the highest category to be 1.5 times that of the closest category. As different studies reported different exposure categories, we normalized these different exposure categories as one cup for each day. Consistent with a prior study, we defined 125 mL/day or 150 g/month as one cup/day [27]. Furthermore, the nonlinear dose–response relationship between tea consumption and risk of kidney stones was evaluated using a restricted cubic splines model with 3 knots at the percentiles 10, 50, and 90% of tea consumption distribution. All analyses were done with the use of R (version 4.0.5) software with the packages “dosresmeta”, “mvmeta”, “rms”, “Hmisc”, and “Metafor”.
Mendelian randomization analysis
Six different methods were used in this MR study: Inverse-variance weighted (IVW), MR-Egger, weighted median, Maximum likelihood, constrained maximum likelihood and model averaging (cML-MA), and robust adjusted profile score (MR-RAPS). In our study, the IVW method was applied as the primary analysis method (the selection of the random-effects model or fixed-effects model depended on the results of Cochrane’s Q test), and other methods were employed to detect the robustness of our results.
Heterogeneity among estimates for each SNP was assessed using Cochran’s Q test. If Q_pvalue > 0.05, the IVW method based on the fixed-effects model was performed; otherwise, choose the random-effects model. The MR-PRESSO method was utilized to identify and correct for outliers, thus improving the reliability of the results [28]. To evaluate the horizontal pleiotropy of IVs, we employed both the ME-Egger intercept test and the MR-PRESSO global test. Furthermore, we performed leave-one-out analyses to visualize the influence of a single SNP on results.
The reverse MR analysis was further performed to assess the potential causal relationship between kidney stones (exposure) and tea consumption (outcome) to rule out interference from reverse causation.
The association with the p value < 0.05 was regarded as a significant association. All analyses were conducted using the “TwoSampleMR (0.5.6)”, and “phenoscaner (1.0)” packages in R (version 4.0.5).
Results
Dose–response meta-analysis
Figure 1A shows the flowchart of the literature search. Finally, 4 studies were included in our meta-analysis, which included 7 cohorts and 1,263,008 participants [6, 12, 29, 30]. The main characteristics extracted from the whole included studies are shown in Table S1, and in our meta-analysis, all studies were assessed as low risk of bias, since the NOS scores were higher than 7.
The summary RR for the highest versus lowest categories of tea consumption is shown in Fig. 2A. The pooled results indicated that higher tea consumption was likely to be a protective factor for kidney stones (RR: 0.80, 95% CI: 0.73–0.87). Heterogeneity could be detected across the included studies (I2 = 58%). To verify the heterogeneity, we further performed a stratified analysis based on different study locations, and the results showed that heterogeneity mainly existed in the China subgroup (I2 = 41%). Furthermore, the sensitive analysis showed that the pooled RRs were not substantially affected by any single study, with the RRs and 95% CIs ranging from 0.78 (0.69–0.88) to 0.83 (0.80–0.87) (Figure S1). We could not assess the publication bias due to the small number of included studies (< 10).

The results of meta-analysis. A Forest plot of tea consumption and relative risk of kidney stones (highest versus lowest level). B Dose–response relationship between tea consumption and relative risk of kidney stones
As for dose–response analysis, we observed an almost linear association between tea consumption and the risk of kidney stones. Compared with no tea consumption, the estimated RRs for the risk of kidney stones were 0.97 (0.93–1.01) for 1 cup/day, 0.95 (0.89–1.00) for 2 cups/day, 0.93 (0.87–0.99) for 3 cups/day, 0.92 (0.87–0.98) for 4 cups/day, 0.91 (0.86–0.97) for 5 cups/day, 0.90 (0.86–0.95) for 6 cups/day, 0.90 (0.86–0.94) for 7 cups/day, and 0.89 (0.86–0.92) for 8 cups/day of tea consumption (Fig. 2B).
Mendelian randomization analysis
There were 12 SNPs included in our analysis, the detailed information on SNPs is provided in Table S2. The deleted SNPs associated with confounders are described in Table S3.
As shown in Fig. 3 and Figure S2, the estimated results of IVW, weighted median, maximum likelihood, cML-MA-BIC, and MR-RAPS method were consistent, which indicated that genetically predicted tea consumption was associated with a decreased risk of kidney stones. MR-Egger provided similar trends of effects, but the 95% CIs were broader and not statistically significant.

Associations of genetically predicted tea consumption with risk of kidney stones. OR odds ratio, CI confidence interval. * < 0.05; ** < 0.01
The results of the sensitivity analysis are summarized in Table 1. No heterogeneity was detected based on Cochran’s Q test (Q_pvalue > 0.05). Moreover, both the MR-Egger regression intercept test (p = 0.910 > 0.05) and the MR-PRESSO global test (p for global test > 0.05) indicated the absence of horizontal pleiotropy in this study. No outlier was detected by the MR-PRESSO method, and the result was the same as the IVW method. Additionally, the “Leave-one-out” analysis demonstrated that none of the single SNP significantly influenced the results, which indicated that our results were reliable (Figure S3).
As shown in Table S4, 10 SNPs identified as IVs for kidney stones were included in the reverse MR analysis. Based on the results of the IVW, there was no reverse causal relationship between kidney stones and tea consumption.
Discussion
To the best of our knowledge, the present study is the first to investigate the relationship between tea consumption and kidney stones by combining dose–response meta-analysis and MR analysis. We observed a preventive effect of tea consumption on kidney stones. The results of the meta-analysis, MR analysis, and additional validation analysis were consistent, demonstrating the reliability of our findings.
Previous observational studies on the association between tea consumption and kidney stones are inconsistent. The recent case–control study showed that people who consumed more than 4 cups/day of tea faced a higher risk of kidney stones compared to those who consumed less than 2 cups/day (OR: 2.73; 95% CI: 1.50–4.99) [11]. Similarly, a cross-sectional study conducted in northern China indicated that tea consumption increased the risk of kidney stones [14]. Conversely, a prospective cohort study based on the UK Biobank suggested that higher tea consumption was related to a lower risk of kidney stones [6]. Another prospective cohort study involving middle-aged and elderly Chinese individuals found that green tea intake was associated with a decreased risk of incident kidney stones [30]. Only one prior meta-analysis has investigated the dose-dependent relationship between tea consumption and kidney stones and observed a protective effect of tea when the participants consumed more than 250 mL/day [15]. It is pertinent to mention that this preceding dose–response meta-analysis encompassed solely three studies where just one was a cohort study. In contrast, our meta-analysis included four cohort studies that used large sample size, which could increase the statistical power to detect potential associations.
Our meta-analysis identified moderate heterogeneity, with subgroup analysis indicating that this heterogeneity was mainly observed within the Chinese cohort. This variation may be related to factors, such as living environment, lifestyle, and dietary pattern. Previous literature has reported rural residency as a risk factor for kidney stones within the Chinese population [31]. Further sensitivity analysis identified that the main source of heterogeneity was the study conducted by Shu et al. [30]. Notably, Shu et al.’s study only included the participants in Shanghai, a major urban center in China. Additionally, the individuals in this study were middle-aged and elderly, while the other three studies did not. Removal of this study from the meta-analysis resulted in a pooled RR of 0.83 (95% CI: 0.80–0.87), and the heterogeneity was reduced to a mild level (I2 = 25%), which suggested a preventive effect of tea consumption for kidney stones. However, due to the small number of included studies in our meta-analysis, additional well-designed, prospective, and multi-center studies with a large cohort of participants are required to valid our findings in the future.
The MR analysis found genetic support that tea consumption was related to the decreased risk of kidney stones. In the MR study, there were three assumptions must be met. First, the IVs should be strongly linked to the exposure. Second, the IVs should be independent of the confounders of exposure and outcome. Third, IVs affect the outcome only through exposure. In accordance with assumption 1, we selected the independent SNPs with genome-wide significant threshold (p = 5 × 10−8) related to tea consumption as IVs. To satisfy assumption 2, we identified and excluded SNPs associated with known confounding factors, including BMI, diabetes, caffeine consumption, and coffee intake, by referencing the PhenoScanner database for second phenotypes related to each SNP. As for assumption 3, both the MR-Egger regression intercept test and the MR-PRESSO global test did not provide evidence of horizontal pleiotropy in our study.
Some potential mechanisms support our findings. On the one hand, fluid intake would increase with increasing tea intake, which has been regarded as an effective method to prevent kidney stones [32]. On the other hand, tea contains caffeine, which has been reported to lower the risk of kidney stones [18]. Caffeine acts as a natural diuretic, promoting increased daily fluid intake and urine flow rate, both of which are major protective factors against kidney stone development [33]. Additionally, in vitro evidence suggests that caffeine can decrease the crystal-binding capacity of renal tubular epithelial cells, thus preventing kidney stone formation [34]. Furthermore, a study involving ten participants demonstrated that the consumption of black tea can increase urinary citrate levels, which is an important inhibitor of calcium stone formation [35]. Moreover, basic research has shown that tea polyphenols can mitigate the damage caused by CaOx crystals to human renal proximal tubular epithelial (HK-2) cells by reducing oxidative stress [36]. Tea polysaccharides have also been found to repair damaged HK-2 cells and inhibit the formation and recurrence of calcium oxalate kidney stones by inhibiting the adhesion of calcium oxalate crystals [37].
This study possessed both advantages and limitations. There are two main strengths in our study. First, our meta-analysis only included prospective cohort studies, which could minimize the influence of reverse causation and other biases. Second, we further performed an MR analysis, and the results were consistent with the meta-analysis, which strengthened the reliability of our results. Furthermore, the reverse MR analysis revealed no evidence of a reverse causal relationship between tea consumption and kidney stones. However, several limitations must be considered. First, owing to the limited number of studies integrated into our meta-analysis, we were unable to assess the presence of publication bias. Second, as for MR studies, horizontal pleiotropy is a significant limitation. Despite excluding the SNPs associated with confounding factors, the potential impact of pleiotropy cannot be entirely ignored. Nevertheless, both the MR-Egger regression intercept test and the MR-PRESSO global test provided limited evidence of horizontal pleiotropy. Additionally, the "Leave-one-out" analysis confirmed the robustness of our findings. Third, due to the lack of GWAS data from other population, the MR analysis only included individuals of European ancestry, which could reduce the generalizability of the results of MR analysis to other populations. Thankfully, our meta-analysis, which included studies from three different countries, yielded similar results to the MR analysis. Finally, we were unable to assess the influence of different types of tea on kidney stone formation due to a lack of specific information about tea varieties. Further rigorously designed studies are needed to corroborate our findings.
Conclusion
Altogether, the dose–response meta-analysis and MR analysis support tea consumption as a potential protective factor for kidney stones and increasing tea consumption may serve as a preventive strategy for kidney stones.
Data availability
The data analyzed in this study is presented in Supplementary material, and further inquiries can be directed to the corresponding author.
References
Wang W, Fan J, Huang G et al (2017) Prevalence of kidney stones in mainland China: a systematic review. Sci Rep 7:41630. https://doi.org/10.1038/srep41630
Hill AJ, Basourakos SP, Lewicki P et al (2022) Incidence of kidney stones in the United States: the continuous national health and nutrition examination survey. J Urol 207:851–856. https://doi.org/10.1097/JU.0000000000002331
Zhang L, Zhang X, Pu Y et al (2022) Global, regional, and national burden of urolithiasis from 1990 to 2019: a systematic analysis for the Global Burden of Disease Study 2019. CLEP 14:971–983. https://doi.org/10.2147/CLEP.S370591
Moe OW (2006) Kidney stones: pathophysiology and medical management. Lancet 367:333–344. https://doi.org/10.1016/S0140-6736(06)68071-9
Geraghty RM, Cook P, Walker V, Somani BK (2020) Evaluation of the economic burden of kidney stone disease in the UK: a retrospective cohort study with a mean follow-up of 19 years. BJU Int 125:586–594. https://doi.org/10.1111/bju.14991
Littlejohns TJ, Neal NL, Bradbury KE et al (2020) Fluid intake and dietary factors and the risk of incident kidney stones in UK Biobank: a population-based prospective cohort study. Eur Urol Focus 6:752–761. https://doi.org/10.1016/j.euf.2019.05.002
Siener R (2016) The role of fluid intake in the recurrence prevention of urinary stones. Urolithiasis 44:S3. https://doi.org/10.1007/s00240-016-0883-8
Chieng D, Kistler PM (2022) Coffee and tea on cardiovascular disease (CVD) prevention. Trends Cardiovasc Med. https://doi.org/10.1016/j.tcm.2021.08.004
Kuriyama S, Shimazu T, Ohmori K et al (2006) Green tea consumption and mortality due to cardiovascular disease, cancer, and all causes in Japan: the Ohsaki study. JAMA 296:1255–1265. https://doi.org/10.1001/jama.296.10.1255
Barghouthy Y, Corrales M, Doizi S et al (2021) Tea and coffee consumption and pathophysiology related to kidney stone formation: a systematic review. World J Urol 39:2417–2426. https://doi.org/10.1007/s00345-020-03466-8
Haghighatdoost F, Sadeghian R, Abbasi B (2021) The associations between tea and coffee drinking and risk of calcium-oxalate renal stones. Plant Foods Hum Nutr 76:516–522. https://doi.org/10.1007/s11130-021-00933-4
Wang H, Fan J, Yu C et al (2021) Consumption of tea, alcohol, and fruits and risk of kidney stones: a prospective cohort study in 0.5 million Chinese adults. Nutrients. https://doi.org/10.3390/nu13041119
Siener R, Hesse A (2021) Effect of black tea consumption on urinary risk factors for kidney stone formation. Nutrients. https://doi.org/10.3390/nu13124434
Wu ZB, Jiang T, Lin GB et al (2017) Tea consumption is associated with increased risk of kidney stones in Northern Chinese: a cross-sectional study. Biomed Environ Sci 30:922–926. https://doi.org/10.3967/bes2017.124
Xu C, Zhang C, Wang X-L et al (2015) Self-fluid management in prevention of kidney stones: a PRISMA-compliant systematic review and dose–response meta-analysis of observational studies. Medicine 94:e1042. https://doi.org/10.1097/MD.0000000000001042
Stephen B, Simon GT (2015) Mendelian randomization: methods for using genetic variants in causal estimation. Chapman and Hall/CRC
Yuan S, Larsson SC (2021) Assessing causal associations of obesity and diabetes with kidney stones using Mendelian randomization analysis. Mol Genet Metab 134:212–215. https://doi.org/10.1016/j.ymgme.2021.08.010
Yuan S, Larsson SC (2022) Coffee and caffeine consumption and risk of kidney stones: a Mendelian randomization study. Am J Kidney Dis 79:9-14.e1. https://doi.org/10.1053/j.ajkd.2021.04.018
Page MJ, McKenzie JE, Bossuyt PM et al (2021) The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ 372:n71. https://doi.org/10.1136/bmj.n71
Stang A (2010) Critical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. Eur J Epidemiol 25:603–605. https://doi.org/10.1007/s10654-010-9491-z
Chen L, Sun X, Zheng L (2022) No causal effect of tea consumption on cardiovascular diseases: a two-sample Mendelian randomization study. Front Cardiovasc Med 9:870972. https://doi.org/10.3389/fcvm.2022.870972
Chen L, Yang H, Li H et al (2022) Insights into modifiable risk factors of cholelithiasis: a Mendelian randomization study. Hepatology 75:785–796. https://doi.org/10.1002/hep.32183
Burgess S, Small DS, Thompson SG (2017) A review of instrumental variable estimators for Mendelian randomization. Stat Methods Med Res 26:2333–2355. https://doi.org/10.1177/0962280215597579
Kurki MI, Karjalainen J, Palta P et al (2023) FinnGen provides genetic insights from a well-phenotyped isolated population. Nature 613:508–518. https://doi.org/10.1038/s41586-022-05473-8
Greenland S, Longnecker MP (1992) Methods for trend estimation from summarized dose–response data, with applications to meta-analysis. Am J Epidemiol 135:1301–1309. https://doi.org/10.1093/oxfordjournals.aje.a116237
Orsini N, Li R, Wolk A et al (2012) Meta-analysis for linear and nonlinear dose–response relations: examples, an evaluation of approximations, and software. Am J Epidemiol 175:66–73. https://doi.org/10.1093/aje/kwr265
Yu F, Jin Z, Jiang H et al (2014) Tea consumption and the risk of five major cancers: a dose–response meta-analysis of prospective studies. BMC Cancer 14:197. https://doi.org/10.1186/1471-2407-14-197
Verbanck M, Chen CY, Neale B, Do R (2018) Detection of widespread horizontal pleiotropy in causal relationships inferred from Mendelian randomization between complex traits and diseases. Nat Genet 50:693–698. https://doi.org/10.1038/s41588-018-0099-7
Ferraro PM, Taylor EN, Gambaro G, Curhan GC (2013) soda and other beverages and the risk of kidney stones. Clin J Am Soc Nephrol 8:1389–1395. https://doi.org/10.2215/CJN.11661112
Shu X, Cai H, Xiang Y et al (2019) Green tea intake and risk of incident kidney stones: Prospective cohort studies in middle-aged and elderly Chinese individuals. Int J Urol 26:241–246. https://doi.org/10.1111/iju.13849
Zeng G, Mai Z, Xia S et al (2017) Prevalence of kidney stones in China: an ultrasonography based cross-sectional study. BJU Int 120:109–116. https://doi.org/10.1111/bju.13828
Cheungpasitporn W, Rossetti S, Friend K et al (2016) Treatment effect, adherence, and safety of high fluid intake for the prevention of incident and recurrent kidney stones: a systematic review and meta-analysis. J Nephrol 29:211–219. https://doi.org/10.1007/s40620-015-0210-4
Wu SE, Chen W-L (2020) Exploring the association between urine caffeine metabolites and urine flow rate: a cross-sectional study. Nutrients 12:E2803. https://doi.org/10.3390/nu12092803
Peerapen P, Thongboonkerd V (2016) Caffeine prevents kidney stone formation by translocation of apical surface annexin A1 crystal-binding protein into cytoplasm: in vitro evidence. Sci Rep 6:38536. https://doi.org/10.1038/srep38536
Siener R, Hesse A (2021) Effect of black tea consumption on urinary risk factors for kidney stone formation. Nutrients 13:4434. https://doi.org/10.3390/nu13124434
Li Z, Chang L, Ren X et al (2021) Modulation of rat kidney stone crystallization and the relative oxidative stress pathway by green tea polyphenol. ACS Omega 6:1725–1731. https://doi.org/10.1021/acsomega.0c05903
Zhao Y-W, Liu L, Li C-Y et al (2020) Preprotection of tea polysaccharides with different molecular weights can reduce the adhesion between renal epithelial cells and nano-calcium oxalate crystals. Oxid Med Cell Longev 2020:1817635. https://doi.org/10.1155/2020/1817635
Acknowledgements
The authors would like to thank the participants and all research staff of the FinnGen consortium and UK Biobank study for their valuable contributions.
Funding
The work of Hequn Chen was supported by the National Natural Science Foundation of China under Grant No. 82170781.
Author information
Authors and Affiliations
Contributions
JW: project development and manuscript writing. HY and ZZ: literature research, data acquisition, and analysis. JC: Manuscript editing. HC and ZC: project development and manuscript editing. All authors have approved the final manuscript.
Corresponding authors
Ethics declarations
Conflict of interest
The authors have no conflicts of interest to declare in this study.
Ethical approval
Our study involved analysis of public data; thus, ethics approval was not required for this study.
Consent for publication
Not applicable.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Wu, J., Yu, H., Zhu, Z. et al. Association between tea consumption and risk of kidney stones: results from dose–response meta-analysis of prospective studies and Mendelian randomization analysis. Int Urol Nephrol 56, 1835–1841 (2024). https://doi.org/10.1007/s11255-023-03918-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11255-023-03918-1