
Abstract
Purpose
Nephrolithiasis is a urological pathology that occurs at high rates and carries a great burden in terms of costs. The probability of recurrence is significant, necessitating improvements in prophylaxis and understanding of the disease mechanism. Despite the high heritability of this disease, only five genome-wide association studies (GWAS) of nephrolithiasis have been published.
Methods
We selected 335 unrelated confirmed nephrolithiasis cases from two major sample collection projects (blood and buccal swabs) in Romania. DNA was extracted from whole blood and buccal swabs at deCODE Genetics (Reykjavik, Iceland) and genotyped.
Results
Single-nucleotide polymorphisms identified from this GWAS implicated biological pathways and gene ontologies involving solute transport, renal physiology, and calcium homeostasis. Three loci especially emerged as candidates with a highly significant association with nephrolithiasis: RS10917682 in Regulator of G protein signaling 5, which has crucial roles in mRNA regulation and has been linked to renal cell carcinoma; RS1118528 in Solute carrier family 25 member 24, which encodes a mitochondrial ATP-Mg/phosphate carrier protein that likely influences a variety of important cellular pathways; and the TOX2-associated locus rs4437026, because TOX2 is upregulated in several tumor types and linked to tumor progression.
Conclusion
This study is the largest kidney stone-related GWAS reported in an Eastern European population and the first GWAS performed in a Romanian population to investigate the genetic risk factors for nephrolithiasis. We identified several loci that warrant further investigation for a better understanding of this highly heritable condition.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
Introduction
The prevalence of nephrolithiasis is increasing, not only in developed countries but also in the rest of the world. Contributing factors include a shift from more traditional diets towards a western way of eating and the increasing prevalence of obesity, diabetes, and a more sedentary lifestyle. The many advances of the modern world come with a cost to health, including metabolic dysfunction, cardiovascular pathologies, and nephrolithiasis. Since the 1960s, when the first major epidemiological studies were undertaken, clinicians and statisticians witnessed an increase in the prevalence of kidney stones. For example, in the 1964–1972 period, the prevalence of nephrolithiasis in the United States was 2.62%. This rate increased to 3.84% during 1976–1980. After the 1980s, the prevalence stabilized at 5.2–5.4%, where it has largely stayed, since [1] the lifetime risk of kidney stones is 8.8% in the United States [2], with an estimated recurrence rate of 14% after 1 year and 35% after 5 years [3], placing a significant burden on the health care system. Another reason for the increased prevalence is broader access to medical facilities, allowing for discovery of many incidental kidney stones after a routine ultrasound or a computed tomography scan performed for another condition.
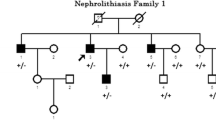
In addition to environmental factors such as diet, kidney stone formation has a heritable component, with almost 65% of kidney stones forming in patients with a family history of the condition. Both twin and genealogy studies have reported a strong heritability for kidney stone disease [4], and twin studies have identified a heritability of > 45% for stone disease and > 50% for hypercalciuria. A strong family history of urolithiasis, including in a parent or a sibling, results in a standard incidence ratio for stone formation of > 50, in contrast to a standard incidence ratio of 1.29 in spouses with no family history.
Five genome-wide association studies (GWAS) of nephrolithiasis have been published, identifying 15 loci associated with disease; however, no transethnic studies have been undertaken [5]. The five existing studies have been conducted in countries including Japan, the UK, and Iceland, but to date, no data have been published regarding the genetic variants linked to kidney stones in Romania. Here, we performed what is, to date, the largest kidney stone-related GWAS in an Eastern European population to uncover gene variants associated with the condition.
Materials and methods
Study population
We selected 335 unrelated confirmed nephrolithiasis cases from the ROMCAN and ProMark projects sample collection, a hospital‐based sample set of 5434 nephrolithiasis cases and controls recruited from five major hospitals in Bucharest between 2008 and 2017. Blood samples and buccal swabs were collected for the ROMCAN and ProMark, respectively [6]. Both ProMark and ROMCAN are large‐scale genetic epidemiological studies investigating the profile of prostate, colorectal, breast, and lung cancers. All participants included in this study as cases were cancer-free. A description of relevant epidemiological and clinical information can be found in the Table 1—ESM Annex 1.
Ethics statement
All participants gave written informed consent prior to enrollment and accepted the use of personal and clinical data and biological samples for genetic research. To collect personal data, trained interviewers performed face‐to‐face interviews using standardized questionnaires. The Bioethical Committee of the Romanian College of Physicians approved the study, and the study protocols were approved by the National Ethical Board of the Romanian Medical Doctors Association in Romania.
Genotyping and analysis of single-nucleotide polymorphism (SNP) data
DNA was extracted from whole blood for the ProMark samples and buccal swabs for the ROMCAN samples, respectively, at deCODE Genetics (Reykjavik, Iceland) and genotyped using Infinium OmniExpress‐24 bead chips (Illumina). DNA samples were prepared and hybridized following the manufacturer’s instructions. The genotype data were filtered using Plink! v1.07. A total of 104,390 markers met the filtering criteria. An association test was performed between the 104,390 markers and a phenotype represented by the confirmed nephrolithiasis diagnosis. The association test was calculated using Plink! v1.07 (6), with a single binary variable as a response. All reported P values are two‐sided. After filtering, only 329 cases were included in the study because of genotyping failures.
Results
Of 5434 included participants (4234 men, 1200 women), there are 329 with stones and 5105 controls. The distribution of association P values (Manhattan plot) for this trait is shown in Fig. 1.

Manhattan plot of all P values for associations of SNPs with the kidney stone phenotype
The ten top scoring SNPs for association with nephrolithiasis are shown in Table 1. The SNP with the lowest P value (1.59 × 10−5) for this trait was rs1980221, located on chromosome 5. This intronic SNP lies in the uncharacterized gene LOC105374686 with similar minor allele frequencies (GG = 0.044828-, TOPMED; G = 0.04018, GnomAD). Other interesting variants from the top 10 scoring SNPs included the intronic variants rs2637748 in the uncharacterized gene LOC107986098, rs4437026 in the TOX2 (TOX high-mobility group-box family member 2) gene, and rs124899 in the SMIM15-AS1 (SMIM15 antisense RNA 1) gene, along with rs10917682, a 3′ untranslated region variant in the RGS5 (Regulator of G protein signaling 5) gene, and RS1118528 in the SLC25A24 (Solute carrier family 25 member 24) gene. Despite the possible biological implications of these variants, neither of these SNPs showed genome-wide significance for association with nephrolithiasis.
Of those in the top 10, the RGS5 RS10917682 variant showed a phenotype association with a P value of 7.94 × 10–5, an odds ratio of 1.634 for the tested allele (G), and a minor allele frequency of 0.1204. The region of this variant is linked to crucial roles in gene expression by influencing the localization, stability, export, and translation efficiency of mRNA.
The SLC25A24 RS1118528 variant showed a phenotype association with a P value of 9.54 × 10–5 and an odds ratio of 0.71 for the G allele. The mitochondrial ATP-Mg/phosphate carrier protein that this gene encodes may affect mitochondrial adenine-nucleotide-dependent enzymes that regulate gluconeogenesis from lactate, urea synthesis, mitochondrial DNA replication, transcription, and protein synthesis, among others [7]. In addition, TOX2 is involved in a variety of relevant pathways, so we further analyzed the results for the TOX2-related rs4437026.
Given the lack of GWAS studies investigating this phenotype and the limitations of our study, we did not follow up our GWAS with a replication study. Despite this issue, we identified 567 markers as associated with nephrolithiasis at P < 0.005 (Table 2—Annex 1 is considered for future replication studies).
Discussion
Our study represents the largest kidney stone-related GWAS to date from an East European population. The analysis integrates data from 329 cases involving kidney stones and 5105 controls of Romanian ancestry, providing a genetic profile of associations with nephrolithiasis. The genes implicated by our GWAS are linked to biological pathways and gene ontologies involving solute transport, renal physiology, and calcium homeostasis.
Among the loci falling in the top 10 for association strength, the RGS5-associated locus RS10917682 occurs at a higher frequency in the Romanian population compared with results based on TOPMED [8] (G = 0.060780) and GnomAD [9] (G = 0.05805), making this variant a strong candidate for future research. RGS5 expression levels are reported to be above average in the kidney, at 110.7 transcripts per million of total transcripts (pTPM) reported by HPA [10] and 44.2 pTPM reported by GTEx, respectively [11]. In one recent study, RGS5 was found to have a significant role in renal cell carcinoma (RCC) and to show a significant association at high expression levels with low serum calcium and increased white blood cell count. The RGS family regulates cellular signaling events downstream of G protein-coupled receptors, which are associated with the initiation and progression of multiple cancers [12]. Gene expression thus might be prognostic and have a significant role in initiation and progression of RCC, as first hypothesized in 2004 with findings linking RGS5 to G protein-mediated signaling in tumor vessels in RCC [13]. Later work in animal models indicated that RGS5 is a potent GTPase-activating protein for Giα and Gqα, which are expressed in vascular smooth muscle, and has been considered as a marker for pericytes, which express RGS5 at high levels [14]. Indeed, this protein is expressed at levels sevenfold higher in renin cells compared with the total kidney cortex, by the smooth muscle cells of the developing kidney arterioles, and by mesangial cells in the adult animal [15].
Considering these previous findings and our current association of this allele with kidney stone formation, the pathological implication of this variant in renal physiopathology is of interest. The 3′ prime untranslated location of RS10917682 appears to have a crucial role in gene expression by influencing the localization, stability, export, and translation efficiency of mRNA.
The SLC25A24-associated RS1118528 allele also was in the top 10 candidates showing a significant association with kidney stone diagnosis. SLC25A24 has previously been identified among 21 genes with the highest expression increase during the stone elimination period [15]. The mitochondrial ATP-Mg/phosphate carrier protein encoded by SLC25A24 is broadly expressed and facilitates the exchange of adenine nucleotides, including ATP-Mg, ATP, ADP, and AMP, and phosphate between mitochondrial matrix and cytosol. As noted, this transporter regulates adenine-nucleotide concentrations in the mitochondrial matrix and may influence many crucial cellular processes [16]. Expression of this gene in kidney varies from 8.4 pTPM, as reported by HPA, to 4.0 pTPM, as reported by GTEx [11].
A third allele that warranted a closer look was rs4437026, an intronic variant in the TOX2 gene, which modifies chromatin structure and is almost identical to high-mobility group-box DNA-binding domains [17]. A recent study showed that TOX and TOX2 are targets of the calcium/calcineurin-regulated transcription factor NFAT [18]. In addition, TOX expression is frequently upregulated in diverse types of human tumors, and its overregulation often is associated with tumor progression and with the control of apoptosis, cell growth, metastasis, and DNA repair. Because of this diversity of roles for TOX2, we also singled it out from our results for the top 10 loci most significantly associated with kidney stone diagnosis.
Conclusions
The pathophysiology of nephrolithiasis is complex, with strong evidence pointing to a genetic predisposition toward stone formation. Although GWAS can give clues to the underlying biological mechanism and despite the heritability of this disease, only five GWAS of nephrolithiasis have been published. This study is the first in a Romanian population and the largest in an Eastern European population to use GWAS to investigate genetic risk factors for nephrolithiasis. The results of the association test identified 567 markers with an observed P < 0.005 for this phenotype. In addition, we highlighted three especially promising association loci in the top 10 that were most significantly linked to nephrolithiasis, and we expect closer analysis of these candidates to facilitate a better understanding of the biological processes underlying this disease.
References
Akpinar H, Assimos DG, Assimos V (2010) Kidney stones: a global picture of prevalence, incidence, and associated risk factors. Rev Urol 12(2–3):e86–e96
Smith AC, Hanley JM, Saigal CS, Scales SCD Jr (2012) Prevalence of kidney stones in the United States. Eur Urol 62(1):160–165. https://doi.org/10.1016/j.eururo.2012.03.052
Oh MS, Carroll HJ, Uribarri J (1989) The first kidney stone. Ann Intern Med 111(12):1006–1009. https://doi.org/10.7326/0003-4819-111-12-1006
Sulem P, Helgason H, Edvardsson VO, Thorleifsson G, Sveinbjörnsson G, Haraldsdottir E, Eyjolfsson GI, Sigurdardottir O, Olafsson I, Masson G, Holm H, Gudbjartsson DF, Thorsteinsdottir U, Indridason OS, Palsson R, Stefansson K, Oddsson A (2015) Common and rare variants associated with kidney stones and biochemical traits. Nat Commun. https://doi.org/10.1038/ncomms8975
Wiberg A, Goldsworthy M, Howles SA et al (2019) Genetic variants of calcium and vitamin D metabolism in kidney stone disease. Nat Commun. https://doi.org/10.1038/s41467-019-13145-x
Mates D, Gunnarsson B, Iordache PD et al (2018) Profile of common prostate cancer risk variants in an unscreened Romanian population. J Cell Mol Med 22(3):1574–1582. https://doi.org/10.1111/jcmm.13433
Sequeira-Lopez MLS, Pentz ES, Lin E, Yu J, Aronow BJ, Potter SS, Gomez RA, Brunskill EW (2011) Genes that confer the identity of the renin cell. JASN 22(12):2213–2225. https://doi.org/10.1681/ASN.2011040401
Harris DN, Kessler MD, Carlson J, Szpiech ZA, Torres R, Taliun SAG, Corvelo A, Gogarten SM, Kang HM, Pitsillides AN, LeFaive J, Lee S, Tian X, Browning BL, Das S, Emde A-K, Clarke WE, Loesch DP, Shetty AC, Blackwell TW, Wong Q, Aguet F, Albert C, Alonso A, Ardlie KG, Aslibekyan S, Auer PL, Barnard J, Barr RG, Becker LC, Beer RL, Benjamin EJ, Bielak LF, Blangero J, Boehnke M, Bowden DW, Brody JA, Burchard EG, Cade BE, Casella JF, Chalazan B, Chen Y-DI, Cho MH, Choi SH, Chung MK, Clish CB, Correa A, Curran JE, Custer B, Darbar D, Daya M, de Andrade M, DeMeo DL, Dutcher SK, Ellinor PT, Emery LS, Fatkin D, Forer L, Fornage M, Franceschini N, Fuchsberger C, Fullerton SM, Germer S, Gladwin MT, Gottlieb DJ, Guo X, Hall ME, He J, Heard-Costa NL, Heckbert SR, Irvin MR, Johnsen JM, Johnson AD, Kardia SLR, Kelly T, Kelly S, Kenny EE, Kiel DP, Klemmer R, Konkle BA, Kooperberg C, Köttgen A, Lange LA, Lasky-Su J, Levy D, Lin X, Lin K-H, Liu C, Loos RJF, Garman L, Gerszten R, Lubitz SA, Lunetta KL, Mak ACY, Manichaikul A, Manning AK, Mathias RA, McManus DD, McGarvey ST, Meigs JB, Meyers DA, Mikulla JL, Minear MA, Mitchell B, Mohanty S, Montasser ME, Montgomery C, Morrison AC, Murabito JM, Natale A, Natarajan P, Nelson SC, North KE, O’Connell JR, Palmer ND, Pankratz N, Peloso GM, Peyser PA, Post WS, Psaty BM, Rao DC, Redline S, Reiner AP, Roden D, Rotter JI, Ruczinski I, Sarnowski C, Schoenherr S, Seo J-S, Seshadri S, Sheehan VA, Shoemaker MB, Smith AV, Smith NL, Smith JA, Sotoodehnia N, Stilp AM, Tang W, Taylor KD, Telen M, Thornton TA, Tracy RP, Van Den Berg DJ, Vasan RS, Viaud-Martinez KA, Vrieze S, Weeks DE, Weir BS, Weiss ST, Weng L-C, Willer CJ, Zhang Y, Zhao X, Arnett DK, Ashley-Koch AE, Barnes KC, Boerwinkle E, Gabriel S, Gibbs R, Rice KM, Rich SS, Silverman E, Qasba P, Gan W, Trans-Omics for Precision Medicine (TOPMed) Program, TOPMed Population Genetics Working Group, Papanicolaou GJ, Nickerson DA, Browning SR, Zody MC, Zöllner S, Wilson JG, Cupples LA, Laurie CC, Jaquish CE, Hernandez RD, O’Connor TD, Taliun GRAD (2020) Sequencing of 53,831 diverse genomes from the NHLBI TOPMed Program. Biorxiv. https://doi.org/10.1101/563866
Laurent C. Francioli, Grace Tiao, Beryl B. Cummings, Jessica Alföldi, Qingbo Wang, Ryan L. Collins, Kristen M. Laricchia, Andrea Ganna, Daniel P. Birnbaum, Laura D. Gauthier, Harrison Brand, Matthew Solomonson, Nicholas A. Watts, Daniel Rhodes, Moriel Singer-Berk, Eleina M. England, Eleanor G. Seaby, Jack A. Kosmicki, Raymond K. Walters, Katherine Tashman, Yossi Farjoun, Eric Banks, Timothy Poterba, Arcturus Wang, Cotton Seed, Nicola Whiffin, Jessica X. Chong, Kaitlin E. Samocha, Emma Pierce-Hoffman, Zachary Zappala, Anne H. O’Donnell-Luria, Eric Vallabh Minikel, Ben Weisburd, Monkol Lek, James S. Ware, Christopher Vittal, Irina M. Armean, Louis Bergelson, Kristian Cibulskis, Kristen M. Connolly, Miguel Covarrubias, Stacey Donnelly, Steven Ferriera, Stacey Gabriel, Jeff Gentry, Namrata Gupta, Thibault Jeandet, Diane Kaplan, Christopher Llanwarne, Ruchi Munshi, Sam Novod, Nikelle Petrillo, David Roazen, Valentin Ruano-Rubio, Andrea Saltzman, Molly Schleicher, Jose Soto, Kathleen Tibbetts, Charlotte Tolonen, Gordon Wade, Michael E. Talkowski, Genome Aggregation Database (gnomAD) Consortium, Benjamin M. Neale, Mark J. Daly, Daniel G. MacArthur Konrad J. Karczewski, "The mutational constraint spectrum quantified from variation in 141,456 humans," bioRxiv, https://doi.org/10.1101/531210.
Fagerberg L, Hallstrom BM, Lindskog C, Oksvold P, Mardinoglu A, Sivertsson A, Kampf C, Sjostedt E, Asplund A, Olsson I, Edlund K, Lundberg E, Navani S, Szigyarto CA-K, Odeberg J, Djureinovic D, Takanen JO, Hober S, Alm T, Edqvist P-H, Berling H, Tegel H, Mulder J, Rockberg J, Nilsson P, Schwenk JM, Hamsten M, von Feilitzen K, Forsberg M, Persson L, Johansson F, Zwahlen M, von Heijne G, Nielsen J, Ponten F, Uhlen M (2015) Proteomics. tissue-based map of the human proteome. Science 347(6220):260419–1260419. https://doi.org/10.1126/science.1260419
Ardlie K, Barcus M, Philip BA, Britton A, Buia SA, Compton CC, DeLuca DS, Peter-Demchok J, Gelfand ET, Guan P, Korzeniewski GE, Lockhart NC, Rabiner CA, Rao AK, Robinson KL, Roche NV, Sawyer SJ, Segrè AV, Shive CE, Smith AM, Sobin LH, Undale AH, Valentino KM, Vaught J, Young TR, Moore HM, Carithers JL, GTEx Consortium (2015) A novel approach to high-quality postmortem tissue procurement: the GTEx project. Biopreserv Biobank 13(5):311–319. https://doi.org/10.1089/bio.2015.0032
Shahriyari L, Su S (2020) RGS5 plays a significant role in renal cell carcinoma. R Soc Open Sci. https://doi.org/10.1098/rsos.191422
Nishiyama M, Kimura S, Suyama T, Naya Y, Ito H, Nikaido T, Furuya HIM (2004) Expression of regulator of G protein signalling protein 5 (RGS5) in the tumour vasculature of human renal cell carcinoma. J Pathol 203(1):551–558. https://doi.org/10.1002/path.1543
Song S, Bergers G (2005) The role of pericytes in blood-vessel formation and maintenance. Neuro-Oncology 7(4):452–64. https://doi.org/10.1215/S1152851705000232
Yasui T, Hamamoto S, Hirose M, Kubota Y, Itoh Y, Tozawa K, Hayashi Y, Okada KKA (2009) Genome-wide analysis of genes related to kidney stone formation and elimination in the calcium oxalate nephrolithiasis model mouse: detection of stone-preventive factors and involvement of macrophage activity. J Bone Miner Res 24(5):908–924. https://doi.org/10.1359/JBMR.081245
Rébeillé F, Douce R, Bligny R, Gout E (2014) Interplay of Mg2+, ADP, and ATP in the cytosol and mitochondria: unravelling the role of Mg2+ in cell respiration. Proc Natl Acad Sci (PNAS) 111(43):E4560–E4567. https://doi.org/10.1073/pnas.1406251111
Kaye J, O'Flaherty E (2003) TOX defines a conserved subfamily of HMG-box proteins. BMC Genom. https://doi.org/10.1186/1471-2164-4-13
Chen J, González-Avalos E, Seo H et al (2019) TOX and TOX2 transcription factors cooperate with NR4A transcription factors to impose CD8+ T cell exhaustion. Proc Natl Acad Sci USA 116(25):12410–12415. https://doi.org/10.1073/pnas.1905675116
Acknowledgements
This study was funded by the EEA Grant “Integrated Applied Genetics Training—AppGENEdu” Project, ID: EY-COP-0029, with data gathered in the EEA Grant—ROMCAN project RO14‐0017 EEAJRP‐RO‐NO‐20131‐10191 and the European Union FP7 Program—ProMark project 202059.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors confirm that there are no conflicts of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Sima, C., Iordache, P., Poenaru, E. et al. Genome-wide association study of nephrolithiasis in an Eastern European population. Int Urol Nephrol 53, 309–313 (2021). https://doi.org/10.1007/s11255-020-02606-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11255-020-02606-8