
Abstract
Purpose
The aim of the study was to summarize the evidence of the validation of CKD-EPI equation and alternative creatinine-based equations in Asian population.
Methods
Relevant validation studies of CKD-EPI and other creatinine-based equations were identified by a systematic literature searching of PubMed conducted from January 2009 through August 2014. Searching terms included “CKD EPI”, “Kidney function test [MeSH] and validation”, and “Glomerular filtration rate [MeSH] and validation” without language or design of study restrictions. The quality of each study was assessed using Quality Assessment of diagnostic Accuracy studies-2 tool.
Results
Of 1064 studies identified, 10 studies were included in the present systematically review. The CKD-EPI equation has been validated in several Asian population including Thai, Japanese, Chinese, Taiwanese, Pakistani as well as Arabic. CKD-EPI equation met the clinically significant 75 % P30 value in several populations, although corrections of some factors may increase the accuracy of the equation. However, some populations may need to find more accurate equations or methods to estimate GFR for the patients.
Conclusions
CKD-EPI is a good equation to start with for estimation of patients’ renal function but for certain disease states and racial populations, the CKD-EPI should be validated before applying. More research is needed in order to develop validated eGFR equations for specific populations and to improve upon the accuracies of currently acceptable equations to better guide therapy and improve patient outcomes.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Chronic kidney disease (CKD) is a recognized global public health challenge, with it comes the importance of being able to properly identify kidney function in order to accurately guide therapy. Glomerular filtration rate (GFR) is regarded as being a predicting factor for kidney function [1]. Measured glomerular filtration rate (mGFR) using an exogenous substance, such as inulin, is ideal; however, this can be costly and time-consuming [2]. Several equations have been developed to estimate glomerular filtration rate (GFR) in order to make GFR assessment faster, more accessible, and cheaper.
The 2002 Kidney Disease Outcomes Quality Initiative (KDOQI) guidelines recommended the use of the Modification of Diet in Renal Disease (MDRD) equation or the Cockcraft–Gault (CG) equation [3]. The MDRD equation is limited by underestimation of estimated GFR (eGFR) in patients with near normal to normal kidney function [1]. In 2009 the Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) equation was released. The CKD-EPI equation was shown to be equivalent to the MDRD equation in accuracy of eGFR compared to mGFR in patients with mGFR below 60 mL/min/1.73 m2 in addition to being superior in patients with mGFR greater than 60 mL/min/1.73 m2 [1].
CKD-EPI seems to be the superior equation; however, the initial paper had a limited patient population of patients from the USA with overwhelming racial majority of patients being Caucasian or black. Further validation in minorities is needed before the CDK-EPI can be generalized to other populations [1]. The 2013 published Kidney Disease Improving Global Outcomes (KDIGO) guidelines recommended the calculation of eGFR alongside any labs that measure a patient’s serum creatinine (SCr). KDIGO also recommended the use of the CKD-EPI equation for assessing eGFR unless there is an alternative equation, with higher accuracy, for the patient population being assessed [4, 5]. This review was undertaken to determine in which patient populations the CKD-EPI equation has since been validated and whether there is an alternative equation with higher accuracy for the given population.
Methods
Identification and selection of studies
Relevant validation studies of CKD-EPI equation and other creatinine-based equations were identified by a systematic literature searching of PubMed conducted from January 1st, 2009, through August 31st, 2014. Medical Subject Headings (MeSH) terms were utilized for the medical searching terms related to the study. Searching terms included “CKD EPI”, “Kidney function test [MeSH] and validation”, and “Glomerular filtration rate [MeSH] and validation” without language or design of study restrictions. Systemic reviews, letters, animal studies, meta-analyses, studies which included no other solely SCr-based equations outside of CKD-EPI, and studies which did not use an exogenous marker to obtain mGFR were excluded.
Data extraction and quality assessment
Review of all abstracts and full texts as well as data extraction were independently conducted by 2 investigators. Data extractions for the included studies were study design, number and characteristics of participants, standard equation used to determine glomerular rate filtration (GFR), tested equation, and accuracy of the equation, 30 % accuracy (P30).
The quality of each study was assessed using Quality Assessment of diagnostic Accuracy studies-2 (QUADAS-2) tool [6]. The QUADAS-2 tool includes the signal questions assessing risk of bias and applicability, and each item is rated “low risk,” “high risk,” or unclear. Discrepancies between the two investigators were resolved by discussion and consensus.
Results
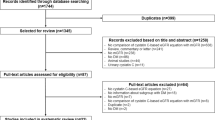
All of 44 articles were collected to be reviewed after initial screening; 22 studies were dismissed due to not being validation studies or not using creatinine-based equations. Therefore, 22 studies were identified as validating CKD-EPI against another Scr-based equation. Six studies were further dismissed, for the use of non-exogenous markers to determine mGFR. It has been known that inulin clearance is the gold standard for determining mGFR [2] but not all studies used inulin as an indicator. However, other exogenous markers for determining GFR have been shown to be comparable [7]. KDOQI warns against the use of non-exogenous markers for determining GFR, such as 24-h urine collections, as non-exogenous derived determination may only be as accurate as an eGFR [3]. Six studies were further excluded because the populations of the studies were not Asian. Therefore, a total of ten studies were included in the systematic review (Fig. 1).

Flow diagram of study identification, inclusion, and exclusion
The results of quality assessment of the included studies by QUADAS-2 tools are shown in Table 1. Considering risk of bias, the present review found that there were three of ten studies which had high risk of bias in domain of patient selection. Besides, most of studies did not stated about the interval between the index test and reference standards which ideally should be collected on the same patients at the same time. Therefore, most of included studies were rated in domain of flow and timing as “unclear”. Moreover, the result of applicability concerns showed similar trend as the result of risk of bias (Table 1).
There are several ways to assess the equations, such as bias, precision, and least squares regression. This review looked at accuracy of the equation, 30 % accuracy (P30) because this measure has been recommended in the guideline [3] wildly used in many GFR validation studies. In addition, this measure is easy to be understood and is available for all of the included studies. P30 is the percentage of eGFR that falls within 30 % of the mGFR. KDOQI considers an equation to be significantly accurate enough for clinical decision making if 75 % of the eGFR falls within 30 % of the mGFR [3]. The summary of P30 values of validated equations for all studies is illustrated in Table 2.
In Thai population, creatinine-based CKD-EPI validation has been tested in 3 studies. In 2011 Praditpornsilpa and colleagues tested the MDRD, CKD-EPI, Chinese MDRD, Japanese MDRD, Thai MDRD, and Thai eGFR equations in 350 Thai CKD patients. Of the reported P30 values, the Thai eGFR and Thai MDRD performed with significantly greater (p < 0.05) P30 values of 90 and 73 %, respectively, compared to CKD-EPI and MDRD P30 values of 68 and 62.7 %, respectively [8]. In addition, a following study tested all these equations and CG equation, excepting for Chinese MDRD and Japanese MDRD equations, in 196 Thai HIV patients. Similar results to previous study [8] were observed which showing that Thai MDRD and the Thai eGFR were the best equations for estimation of GFR in Thai HIV populations with the P30 of 84 % [7]. However, the CKD-EPI was also effective to estimate GFR in this population with a P30 value of 80 %, making the CKD-EPI equation still a reasonable equation for determination of eGFR in this population [7]. Another study was conducted in 98 post-renal transplant patients. No equation was found to be significantly superior to the others; the CKD-EPI equation had the highest P30 value but failed to reach the 75 % threshold [9].
Japanese MDRD and Japanese CKD-EPI equations were developed in 413 and validated in 350 Japanese patients, both groups including CKD and non-CKD patients. The Japanese MDRD had a P30 value of 73 %, while the Japanese CKD-EPI equation had a value of 75 % [10].
Another validation study was done in a group of Chinese CKD population comparing CKD-EPI and other creatinine-based equations [11, 12]. A small study in Chinese CKD patient shows that CKD-EPI was better than other equations in predicting of GFR in the population [11]. Supported by a larger study in this population [12], CKD-EPI with 2-level race equation (black, white, or other) showed equally accuracy with Chinese equation and were better than other equations including CKD-EPI with 4-level race equation (Black, Asian, Native American and Hispanic, White and other). However, all equations failed to reach a P30 of 75 % or greater [11, 12].
Similar trend was reported in another recent study in Chinese population [13] which showed that CKD-EPI was superior to re-expressed 4-variable MDRD and Asian modified CKD-EPI equations in both type-2 diabetes and non-diabetes. However, the accuracy of these equations was low. Therefore, the new modified equation of CKD-EPI was developed and validated in diabetes patients. The study found that the accuracy of the new modified equation was the highest value (71.4 %) compared to other 3 equations [13]. Considering SCr-based equations, CKD-EPI and modified versions of the CKD-EPI equations equally perform in predicting of eGFR in Chinese populations and better than other equations.
Racial factors were developed for the CKD-EPI equation with a group of 556 Taiwanese adults with CKD rate of 75 % and validated in a group of 136 adults, with CKD rate of 100 %. No equation reached a P30 of 75 % or greater including CKD-EPI. However, the Taiwanese four-level CKD-EPI, Taiwanese CKD-EPI, and Taiwanese MDRD had the highest accuracies more than 70 %. The authors recommended the use of the Taiwanese MDRD equation as it has the lowest root mean square error of 21.4 mL/min/1.73 m2 even though it failed to reach a 75 % P30 [14].
Equations for estimation of kidney function in a South Asian population from Pakistan with a CKD rate of 16 % were also validated in 581 patients. The CKD-EPI, MDRD, Pakistani CKD-EPI, and two new formulated equations (PK#1 and PK#2) were tested. The Pakistani CKD-EPI equation had a significantly better accuracy compared to the original, 81.6 and 76.1 %, respectively (p < 0.001). PK#1 and PK#2 also had high P30 values of 82.7 % and 82.5 %, respectively [15]. PK#1 and PK#2 had P30 values similar to the modified CKD-EPI; however, the PK equations are complicated and inconvenient for use; in conclusion the authors recommended the use of the Pakistani CKD-EPI [15]. Moreover, another study was conducted in 158 Arabic kidney transplant patients. No equation was found to be suitable replacements of mGFR as none of them reached P30 values of 75 % or greater [16]. Further investigation is needed in this patient population.
Discussion
This systematic review summarized the evidence of the validation of CKD-EPI equation to estimate GFR in Asian population. The CKD-EPI equation has been validated in several Asian population including Thai, Japanese, Chinese, Taiwanese, Pakistani as well as Arabic. The results illustrated that CKD-EPI equation may need to be adjusted with some factors before it can be use more accurate in each population.
In Thai population, the Thai GFR equation derived from several crucial factors such as GFR, SCr, blood urea nitrogen (BUN), age, albumin, and body surface area [8] showed superior performance, compared to CKD-EPI, which possibly due to its incorporation of body surface area into the equation, a variable that could be important for Thai GFR determination. Similar findings were observed in Thai HIV patients with the majority of patients had low skeletal muscle mass and high body fat. This is likely a result of the disease and also a racial factor may play important role [7]. In contrast, the study in Thai renal transplant patients showed that the CKD-EPI equation performed better than other equations, although neither CKD-EPI nor other equation reached the 75 % of P30 value. This study provided evidence that other factors are needed to be taken into account outside of race for estimation of GFR in Thai renal transplant population [9]. These findings were supported by other studies in Arabic [16] and German kidney transplant populations [17]. Since the CKD-EPI equation is known to be the best at determining GFR in patients with higher levels of kidney function, the equation may have performed better if a larger cohort had been obtained with some healthier kidney function added to the data pool. Moreover, BMI may not be an important factor for determining GFR in kidney transplant patients [16]. Since SCr-based equations may not be suitable, other endogenous markers possibly are needed to determine accurate eGFR equation for kidney transplant patients.
However, CKD-EPI and modified CKD-EPI equations were found to be better than other serum creatinine-based equations but their accuracy was still low (P30 < 75 %) in Chinese populations [11–13]. Another validation study using 99mTc-DTPA renal gamma imaging method was done in a group of Chinese elderly population to validate the CKD-EPI and a new formulated equation (Chinese elderly equation). Although the Chinese elderly equation performed significantly better than the CKD-EPI with reported P30 values of 71.1 and 47.2 % (p < 0.001), respectively, both equations failed to reach a P30 of 75 % or greater [18]. The Maclsaac equation was also studied in this population and showed high P30 > 80 %; however, this equation was not SCr-based equation [19].
A cystatin C (Cys-c)-based equation was also examined along with the CKD-EPI and MDRD equations. SCr-based equations have long been the norm to use for estimating GFR as SCr is a classic kidney function biomarker. However, Cys-c is the newer and possibly better biomarker to use. The racially modified CKD-EPI and MDRD performed at a significantly better level compared to the original equations, near that of the Cys-c equation, which did not improve significantly after modification [19]. This could indicate that SCr was more greatly affected by race than Cys-c, possibly suggesting that racial modification and validation were more crucial for SCr-based equations, compared to those of Cys-c-based equations. Although the new modified equation of CKD-EPI was more suitable to determine GFR in Chinese DM population [13], the CKD-EPI and the Chinese equation were comparable in CKD populations [11, 12]. Further investigation is needed to determine an accurate correction factor in estimating eGFR in Chinese population regarding racial age and disease factors.
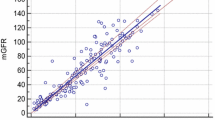
On the other hand, the MDRD equation performed better than that of the CKD-EPI in Taiwanese adults, especially when restricting analysis to patients with lower than normal levels of mGFR (<60 ml/min/1.73 m2). After racial correction applied, these equations were comparable with P30 values of almost reaching 75 %. The explanation may be from the exogenous marker used to determine mGFR introduced bias. Since this study used inulin clearance to determine its mGFR, which could in turn predispose CKD-EPI to overestimate its GFR [14]. Moreover, similar to CKD-EPI equation derived by using iothalamate [1], the equations [7–9, 11–13, 16] using 99mTc-DTPA as a standard biomarker also overestimated mGFR, compared to those using inulin clearance [4, 10, 14].
The first general population study of South Asian (Pakistani) patients validated an eGFR equation by using the gold standard, inulin. However, both the MDRD and the CKD-EPI overestimated the mGFR and were needed for corrections of other factors such as BMI and waist circumference to improve the accuracy [15]. This suggests that BMI and waist circumference may be important factors in determining GFR in South Asian population.
The correction factor determined in the study of Japanese populations found that a coefficient of 0.813 was needed for the CKD-EPI equation. This suggests that Japanese populations have lower SCr levels, compared to Caucasian populations. The explanation was most likely due to Japanese has lower skeletal muscle mass [10]. This finding reinforces that the CKD-EPI equation is needed to validate the equation and correction of crucial factors for specific races before being applied.
Conclusions
This systematic review illustrated that the CKD-EPI equation met the clinically significant 75 % P30 value in several populations, although corrections of some factors may increase the accuracy of the equation. However, some populations may need to find more accurate equations or methods to estimate GFR for the patients. The review reinforced the accurate use of CKD-EPI in patients without suspected kidney function loss. On the other hand, racial correction may be needed before the equation can be generalized in patients with renal impairment. Moreover, BMI and weight may be important cofactors of racial factor but not a specific disease state when modifying the equations. Besides, SCr-based equations are needed for racial correction, compared to Cys-c-based equations.
Some limitations of this review were its use of only one search engine leading to the possibility of missed studies that may otherwise have been included. Other limitations were that this review only looked at SCr-based equations while Cys-c is a rapidly developing new endogenous marker being validated in new equations. As pointed out Cys-c may be a more suitable endogenous biomarker for determining GFR, such as in elderly populations, cirrhosis and kidney transplant patients.
This systematic review provides evidence that there is no one equation that can be generalized in all populations. CKD-EPI is a good equation to start with, especially in patients with normal kidney function, but for certain disease states and racial populations, the CKD-EPI should be validated before applying. More research is needed in order to develop validated eGFR equations for specific populations and to improve upon the accuracies of currently acceptable equations to better guide therapy and improve patient outcomes.
References
Levey AS, Stevens LA, Schmid CH et al (2009) A new equation to estimate glomerular filtration rate. Ann Intern Med 150:604–612
Falbriard A, Zender R (1964) Measurement of glomerular function by plasma decrease of a substance analogous to inulin (polyfructoses): clinical importance and comparison with classical glomerular clearance. Nephron 1:277–294 (Abstract)
National Kidney Foundation (2002) K/DOQI clinical practice guidelines for chronic kidney disease: evaluation, classifications and stratification. Am J Kidney Dis 39:S1–S266
Kidney Disease: Improving Global Outcomes (KDIGO) Acute Kidney Injury Work Group (2012) KDIGO clinical practice guideline for acute kidney injury. Kidney Int 2:S1–S138
Kidney Disease: Improving Global Outcomes (KDIGO) CKD Work Group (2013) KDIGO 2012 clinical practice guideline for the evaluation and management of chronic kidney disease. Kidney Int 3:S1–S150
Whiting PF, Rutjes AW, Westwood ME et al (2011) QUADAS-2: a revised tool for the quality assessment of diagnostic accuracy studies. Ann Intern Med 155:529–536
Praditpornsilpa K, Avihingsanon A, Chaiwatanarat T et al (2012) Comparisons between validated estimated glomerular filtration rate equations and isotopic glomerular filtration rate in HIV patients. AIDS 26:1781–1788
Praditpornsilpa K, Townamchai N, Chaiwatanarat T et al (2011) The need for robust validation for MDRD-based glomerular filtration rate estimation in various CKD populations. Nephrol Dial Transplant 26:2780–2785
Townamchai N, Praditpornsilpa K, Chawatanarat T et al (2013) The validation of estimated glomerular filtration rate (eGFR) equation for renal transplant recipients. Clin Nephrol 79:206–213
Horio M, Imai E, Yasuda Y et al (2010) Modification of the CKD epidemiology collaboration (CKD-EPI) equation for Japanese: accuracy and use for population estimates. Am J Kidney Dis 56:32–38
Xie P, Huang JM, Lin HY et al (2013) CDK-EPI equation may be the most proper formula based on creatinine in determining glomerular filtration rate in Chinese patients with chronic kidney disease. Int Urol Nephrol 45:1057–1064
Kong X, Ma Y, Chen J et al (2013) Evaluation of the Chronic Kidney Disease Epidemiology Collaboration equation for estimating glomerular filtration rate in the Chinese population. Nephrol Dial Transplant 28:641–651
Liu X, Gan X, Chen J et al (2014) A new modified CKD-EPI equation for Chinese patients with type 2 diabetes. PLoS One 9:e109743
Chen LI, Guh JY, Wu KD et al (2014) Modification of diet in renal disease (MDRD) study and CKD epidemiology collaboration (CKD-EPI) equations for Taiwanese adults. PLoS One 9:e99645
Jessani S, Levey AS, Bux R et al (2014) Estimation of GFR in South Asians: a study from the general population in Pakistan. Am J Kidney Dis 63:49–58
El-minshawy O, El-bassuoni E (2013) Validity of current equations to estimate glomerular filtration rate in kidney transplant recipients. Transpl Proc 45:2165–2170
Pöge U, Gerhardt T, Stoffel-wagner B et al (2011) Validation of the CKD-EPI formula in patients after renal transplantation. Nephrol Dial Transplant 26:4104–4108
Liu X, Wang Y, Wang C et al (2013) A new equation to estimate glomerular filtration rate in Chinese elderly population. PLoS One 8:e79675
Pei X, Yang W, Wang S et al (2013) Using mathematical algorithms to modify glomerular filtration rate estimation equations. PLoS One 8:e57852
Acknowledgments
This work was investigator initiated. No funding was provided for support. S. Laehn was a candidate of Doctor of Pharmacy at the School of Pharmacy, University of Wisconsin-Madison.
Authors’ contribution
Patcharaporn Sudchada conceived, supervised, and conducted the study. Patcharaporn Sudchada and Spencer Laehn search, screened, extract, and analyze the data. Spencer Laehn wrote the initial draft of the paper. Patcharaporn Sudchada review and edited the paper.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors (PS and SL) declare that they have no potential conflict of interest regarding the publication of the paper.
Ethical approval
This article does not contain any studies with human participants or animals performed by any of the authors.
Rights and permissions
About this article

Cite this article
Sudchada, P., Laehn, S. Comparisons of GFR estimation using the CKD Epidemiology Collaboration (CKD-EPI) equation and other creatinine-based equations in Asian population: a systematic review. Int Urol Nephrol 48, 1511–1517 (2016). https://doi.org/10.1007/s11255-016-1357-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11255-016-1357-1