
Abstract
The study evaluated the reliability of polymorphonuclear (PMN) cell count in endometrial cytology by cytobrush technique as a diagnostic for subclinical endometritis (SCE) at the time of estrus and its relationship with bacterial presence and fertility in buffaloes. Healthy pluriparous buffaloes (n = 115) were subjected to endometrial sampling by cytobrush technique (for cytology and bacterial isolation) and ultrasonography of genitalia prior to insemination at the time of spontaneous estrus. Buffaloes were inseminated at the same estrus and were confirmed for pregnancy by ultrasonography at day 40 post-insemination. Growth of aerobic bacteria was recorded in 26.1% (30/115) of estrual buffaloes. Bacteria of eight distinct genera (Staphylococcus spp., Bacillus spp., Proteus spp., Escherichia coli, Klebsiella spp., Streptococcus spp., Pseudomonas spp. and T. pyogenes) were isolated. Presence of bacterial infection was considered as the standard, against which PMN threshold for SCE was calculated by receiver operator curve (ROC). The PMN count of ≥ 5% with good sensitivity (66.7, 95% CI 50.9–81.4) and specificity (87.0%, 95% CI 78.0–94.6) with an overall high diagnostic accuracy (81.7%) for predicting SCE was obtained. Based on calculated PMN threshold, buffaloes were divided into subclinical endometritic (SCE; ≥ 5% PMNs) and control (< 5% PMNs) groups. Thirty-one buffaloes (27.0%, 31/115) had ≥ 5% PMNs in the endometrial cytology at estrus. Ultrasonographic evaluation showed that size of largest follicle, endometrial thickness, and uterine horn diameter did not differ significantly (P > 0.05) between the two groups. Significantly, lower conception rate (22.58 vs 36.90%, P < 0.05) for first artificial inseminations (AIs) and significantly higher number of AIs per pregnancy (2.81 ± 0.27 vs 1.75 ± 0.15, P < 0.05) were recorded in SCE compared to control group. The results indicated that cytobrush based endometrial cytology with 5% PMN cut-off value has a good accuracy for predicting subclinical endometritis at estrus in buffaloes.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Subclinical endometritis (SCE), also known as cytological endometritis, is the inflammation of endometrium without clinical manifestations or systemic illness (Kasimanickam et al. 2004). Since subclinical endometritis remains undiagnosed, it causes serious economic losses. Studies had demonstrated the presence of SCE to be a key factor in pregnancy rate, with an increase in days open ranging from 16 days (Dubuc et al. 2011) to 50 days (Brodzki et al. 2014) and an increase in number of services per conception (Brodzki et al. 2014) in subclinical endometritic cows. The extra days without conception (Kasimanickam et al. 2004; Gilbert et al. 2005; Barlund et al. 2008), extra artificial inseminations (Gilbert et al. 2005; Barlund et al. 2008), and subsequent culling result in economic losses. It is speculated that losses due to SCE may exceed billions of dollars annually for the global dairy industry (Ghasemi et al. 2012). Therefore, there is a need to develop feasible and reliable diagnostic tests to characterize SCE.
Polymorphonuclear (PMN) granulocytes represent the first and principal immunologic defense mechanism in the uterus. The elevated PMN count in endometrial cytology indicates an endometrial inflammatory condition and is the most convenient method to diagnose SCE (Sheldon et al. 2006; Barlund et al. 2008). The proportion of PMN cells to define SCE decreases over time during postpartum period (Wagener et al. 2017). Diverse time frames of examination (7–60 dpp; days postpartum) with different % PMN thresholds (ranging from 5% to > 25%) in endometrial cytology by cytobrush and uterine lavage had been used to diagnose SCE during postpartum period (Kasimanickam et al. 2004; Barlund et al. 2008; Carneiro et al. 2014; Gahlot et al. 2017). During the last decade, endometrial cytology by cytobrush method has established its superior efficacy and acceptability for diagnosis of SCE as it is non-invasive, easy, and a practical technique generating good picture of various representative cells (Sheldon et al. 2006; Ghasemi et al. 2012).
The lack of a standard test necessitates the use of reproductive performance as a reference for evaluating diagnostic methods for SCE. Consequently, this has resulted in different PMN cut-offs as reproductive performance is affected by multiple factors viz. estrus detection efficiency, length of voluntary waiting period, use of synchronization programs etc. (Wagener et al. 2017). Endometrial sampling especially during estrus could be ideal in this perspective as it offers the opportunity to determine the uterine health status at the time when the animal is fertile and thus allow to study the effect of SCE on the subsequent conception rate (Pascottini et al. 2016; Singh et al. 2018). Estrus could also provide a standard time for the use of an universal cut-off point without interference of normal uterine involution process, thus further increasing sensitivity and specificity of the diagnostic test (Kaufmann et al. 2009). Objective of present study is the diagnosis of SCE by endometrial cytology and to evaluate its relationship with reproductive performance in estrual buffaloes.
Materials and methods
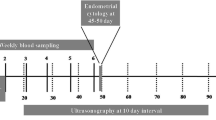
Healthy (body condition score = 2.5 to4) normal cyclic buffaloes in spontaneous estrus presented for artificial insemination (n = 115) were enrolled in the present study. The selected buffaloes were in the second to fifth parity with mean age of 6.4 ± 1.7 years. Animals were stall-fed or managed under a loose housing system and identified with ear tags. All animals were evaluated for reproductive health by trans-rectal ultrasonographic examination and quality of cervico-vaginal discharge at the time of enrollment. Healthy buffaloes (> 60 days postpartum) with normal spontaneous estrus without clinical endometritis or any reproductive problem were enrolled into this experiment and subjected to uterine bacterial isolation and endometrial cytology by cytobrush method. All the buffaloes were inseminated following sampling at the same estrus (twice as per AM/PM rule) and pregnancy diagnosis was carried out at 40 days post-insemination.
Ultrasonography of reproductive organs
Ultrasound scanning was carried out to record the size of largest follicle, endometrial thickness, and horn diameter of both the uterine horns prior to insemination. Real-time B-mode ultrasonography using 7.5 MHz frequency transducer (Z5 Model, Mindray, Shenzhen Mindray Biomedical Electronics Co. Ltd., Germany) was used for imaging reproductive organs. Uterine horn at about 2.0 cm from internal uterine bifurcation was used to serve as a consistent landmark to obtain valid measurements of endometrial thickness and uterine horn diameter. The average of two measurements of diameter and endometrial thickness (ET) of both horns was taken for each buffalo. Both ovaries in each buffalo were scanned gently on several planes to identify various ovarian structures and record diameter of largest follicle.
Endometrial cytology
A cytobrush assembly was fabricated by modification of bovine uterine swab catheter to collect cellular material from bovine endometrium, aseptically. Briefly, the modification consisted of replacing the swab stylette with sharpened tip stylette so that pap smear brush for human use (Hi-Cytobrush, HI-MEDIA Laboratories Limited, India) can snuggly fit on the tip of stylette. Prior to use, cytobrush units (metallic catheter and stylette) were sterilized by hot air oven. The cytobrush assembly was passed through cervix aseptically and guided past the uterine bifurcation into uterine horn ipsilateral to dominant follicle. Two cytobrush samples were collected at each occasion by this technique (Barlund et al. 2008). The first cytobrush was aseptically put into a sterile 15 ml tube containing 2.0 ml of autoclaved Brain Heart infusion (BHI) broth media and used for bacterial isolation. The second brush was used to make smears for cytological examination. The slides were fixed with methanol and stained with modified Wright Giemsa stain (Sigma-Aldrich Inc., USA) as per the guidelines. Slides were examined using light microscopy under oil immersion with 100× objective to identify endometrial epithelial and PMN cells. A total of 300 cells per slide were counted (Melcher et al. 2014).
Isolation and identification of bacteria
Samples in broth media were first incubated at 37 °C for 6–8 h and then cultured for aerobic bacteria by gently streaking broth onto sterile culture media (Brain Heart Infusion agar, Mannitol Salt agar, Eosin Methylene Blue agar, MacConkey Lactose agar, and Blood agar) plates and incubated at 37 °C for 24 h as described by Quinn et al. (1999). The plates were examined for growth at 24 h post incubation. If no growth was present, the plates were further incubated for 48 h at 37 °C before declaring a sample bacteriologically negative. Plates with one or more colony-forming units were designated as positive for bacterial growth, and those with more than three species or with mixed culture of moderate or higher degree were considered contaminated. Isolation and identification of bacteria were further carried out based on the morphology, cultural characters, Gram staining, and biochemical tests in the positive samples as described by Quinn et al. (1999).
Statistical analysis
All statistical analyses were carried out using IBM SPSS Statistics 16.0 (SPSS, Chicago, IL). The diagnostic potential of PMN cell threshold was compared against presence of bacterial infection of uterine bacteria by using receiver operator characteristic (ROC) curve analysis and the optimum PMN cell cut-off was taken as a point at which the Youden’s index (Se + Sp − 1) was maximum (Habibzadeh et al. 2016). The sensitivity (Se) of cytobrush cytology is defined as the probability of having ≥ 5% PMN cells in animals with presence of infection, whereas the specificity (Sp) is the likelihood of < 5% PMN in an animal without the presence of infection. Ultrasonographic parameters of two groups were compared using student’s t test. p Value of less than 0.05 was considered as statistically significant. The effect of subclinical endometritis on fertility parameters was analyzed by Kaplan-Meier survival analysis, and median values were compared by logrank test. Conception rates were compared by chi-square test.
Results
Uterine bacterial profiles
The bacteria of seven distinct genera were isolated viz. Staphylococcus spp., Bacillus spp., Proteus spp., Escherichia coli, Klebsiella spp., Streptococcus spp., Pseudomonas spp., and T. pyogenes. Bacterial infection was observed in 26.1% (30/115) of estrual buffaloes. The cut-off value of PMN cells was calculated by receiver operating characteristic (ROC) against presence of uterine bacterial infection. The area under the curve (AUC) was 0.73 (95% CI 0.68 to 0.82) (Fig. 1). The PMN value ≥ 5%, with highest Youden’s index, was selected as optimum cut-off value. The sensitivity and specificity of ≥ 5% PMN cut-off was used for predicting SCE in relation to bacterial isolation. The sensitivity of 66.7 (95% CI 50.9–81.4) and specificity of 87.0% (95% CI 78.0–94.6) was obtained. The overall diagnostic accuracy of ≥ 5% PMN cut-off as reference test for SCE was 81.7%. Based on the calculated PMN cell threshold (≥ 5%), prevalence rate of 27.0% (31 out of 115) was recorded for SCE. Buffaloes positive for SCE had mean PMN % of 13.62 ± 1.52 and buffaloes negative for SCE had mean PMN of 3.44 ± 0.25 at the time of estrus. Bacterial infection was recorded in 20 out of 31 buffaloes positive for SCE as compared to 10 out of 84 negative buffaloes. Presence of T. pyogenes was observed only in four buffaloes positive for SCE.

Receiver operator curve for percent polymorphonuclear (PMN) cells in relation to presence of uterine bacterial infection. The sensitivity = 66.0 (95% CI 50.9–81.4); specificity = 87.0 (95% CI 78.0–94.6); area under curve = 0.73 (95% CI 0.68–0.82)
Effect of subclinical endometritis at estrus on utero-ovarian parameters
The mean endometrial thickness did not vary significantly (P > 0.05) between buffaloes with (7.13 ± 0.18 mm) and without (6.72 ± 0.13 mm) SCE (Table 1). Similarly, the buffaloes positive for SCE had similar (P > 0.05) uterine horn diameter (21.67 ± 0.49 versus 20.83 ± 0.71 mm) at estrus as of control group. The size of largest follicle at estrus also did not differ (P > 0.05) between the buffaloes of the SCE and the control group (Table 1).
Effect of subclinical endometritis at estrus on fertility parameters
Buffaloes positive for SCE has lower (P < 0.05) conception rate at the first examined spontaneous estrus as compared to buffaloes negative for SCE (22.58 vs 36.90%). However, the overall pregnancy rate (up to 100 days from the time of diagnosis of SCE) was similar in both the groups, i.e., 77.38% (65/84) in control and 74.19% (23/31) in SCE group. Buffaloes affected by SCE took twice the median number of days to conception as compared to control (Table 2). By 50 days post- diagnosis of SCE, approximately 57% of buffaloes were pregnant in the control group compared to only 42% in SCE group (Fig. 2). Moreover, the mean number of AIs per pregnancy was significantly (P < 0.05) higher in the SCE group as compared to the control group (Table 2).

Kaplan-Meier survival curves for proportion of pregnant buffaloes up to 100 days from diagnosis of subclinical endometritis at estrus
Discussion
The present study evaluated the applicability of endometrial cytology samples for diagnosis of SCE and its relationship with reproductive performance in estral buffaloes. Endometritis has been reported as the most common pathological abnormality affecting reproductive tract in buffaloes (Azawi et al. 2008). Based on calculated PMN cell count threshold value (more than or equal to 5 percent PMN cells), a prevalence of 26.9% (31/115) was recorded for SCE at estrus in buffaloes. The results of the present study were in agreement with Gahlot et al. (2017), who reported prevalence of 23.08% in postpartum buffaloes based on the cytobrush cytology (5% PMN cut-off). A higher prevalence of 41.7% at 30–31 days postpartum (dpp) in Murrah buffaloes was reported by Dar et al. (2015) employing uterine lavage cytology technique. The prevalence of SCE recorded in the present experiment was lower than reported by most of other studies at different postpartum periods in cows (34%, Kasimanickam et al. 2004; 53%, Gilbert et al. 2005; 38%, Galvao et al. 2009; 31%, Ricci et al. 2015). This discrepancy can be due to invariable presence of bacterial contamination and inflammation during the postpartum period, different PMN thresholds used, and species differences (buffalo versus cow). Another reason for comparatively low SCE prevalence in the present study could be the use of endometrial cytology as an exclusive diagnostic criterion, whereas some researchers had considered any amount of echogenic fluid in the postpartum uterus to be associated with SCE (Kasimanickam et al. 2004; Barlund et al. 2008).
The PMN% profiles (mean and its range) of estrual buffaloes were almost similar to those reported by Brodzki et al. (2014) during follicular phase in cows. It was proposed that high estrogen concentration at estrus stage might incite a physiological PMN infiltration into the endometrium that might lead to false-positive SCE results for samples taken at AI (Subandrio et al. 2000). However, Madoz et al. (2013) studied the normal (healthy) endometrial PMN profile in cattle and reported far below values during different stages of estrous cycle, i.e., estrus (1.26%), metestrus (1.78%), diestrus (1.95%), and prestrus (1.07%). PMN infiltration recorded during different stages of estrous cycle was always below the minimum thresholds reported for SCE diagnosis and hence risk of false-positive cases as a consequence of physiological PMN infiltration is low (Madoz et al. 2013). It remains debatable, as in one study (Pascottini et al. 2016), no PMN cells were reported in > 92% of samples harvested during AI in dairy heifers.
Limited reports were available about the relationship of bacterial findings and the proportion of PMNs (Galvao et al. 2009), and none was available for estral buffaloes. Recently, Ricci et al. (2015) observed 8% of SCE cows to be bacteriologically negative whereas Madoz et al. (2014) failed to isolate bacteria in postpartum cows positive for SCE. Similarly, no correlation between proportions of PMN cells with bacteriological growth density on the agar plates was reported, suggesting that not all the cases of SCE were caused by infection with culturable bacteria or that the inflammation lasts longer than the infection (Westermann et al. 2010; Baranski et al. 2012). However, in cows with clinical endometritis, Westermann et al. (2010) had observed a significant positive correlation between PMN% and the presence of T. pyogenes. The low level of agreement between the presence of intrauterine pathogens and endometrial PMN% was also reported by McDougall et al. (2011), as in some SCE cows, no bacteria were isolated, possibly due to resolution of bacterial infection by uterine defense mechanism while inflammatory response was still underway (Madoz et al. 2014). However, bacterial presence in uterine samples displayed a significant positive correlation with PMN % (r = 0.295; < 0.01) and endometrial thickness (r = 0.208; P < 0.05), whereas correlation with horn diameter and size of largest follicle was not significant.
A good accuracy and strong validation of 5% PMN threshold as a diagnostic criterion for endometrial inflammation (and in turn SCE) at estrus in buffaloes was recorded in this experiment. This is in agreement with McDougall et al. (2011), who suggested the percentage of PMN cells as a better predictor of reproductive performance than either intrauterine bacteriology or gross inflammation score. The present investigation is perhaps the first to study prevalence of subclinical endometritis at estrus in buffaloes as majority of available reports are in cattle, during mid or late postpartum period.
In recent years, several publications had reported a negative impact of SCE on subsequent reproductive performance in dairy cattle (Gilbert et al. 2005; Barlund et al. 2008; Kaufmann et al. 2009; McDougall et al. 2011). However, similar studies on buffalo are lacking in literature. The only study that analyzed the effect of SCE immediately prior to AI on conception in cows observed a very low conception rate 17.8% based on ≥ 5% cut-off (Pascottini et al. 2016). Kaufmann et al. (2009) prepared cytosmears 4 h post-insemination and reported a significant reduction in first service conception rate in cows with high PMN count (15% PMN) as compared to medium PMN count (0–15% PMN) (29.6 vs 57.6%). Supporting the present finding, reduction in proportion of pregnant cows at 300 dpp (63.0 versus 89.0%, respectively) in SCE compared to healthy cows had been reported previously (Gilbert et al. 2005). Likewise, Barrio et al. (2015) found that 60% of cows with SCE were pregnant within 200 days postpartum as opposed to 80% of healthy cows. In contrast, Carneiro et al. (2014) failed to arrive at an association between presence of subclinical endometritis (32–70 dpp) and first service conception rate and pregnancy rate at 150 days postpartum in cows. Recently, Plöntzke et al. (2010) also reported no effect of SCE on days to first service, FSCR, days open and pregnancy rate in grazing dairy cows in Argentina.
No significant difference in endometrial thickness (ET) was observed in the present study. Endometrial thickness was reported to have the highest sensitivity and specificity for diagnosing SCE in relation to pregnancy status at 150 dpp in Holstein cows (Barlund et al. 2008). However, a recent study (Salah and Yimer 2017) found endometrial thickness (≥ 5 cm) alone not to be a reliable indicator of cytological endometritis (≥ 8% PMN). Information concerning morphologic changes (particularly ET) of the bovine endometrium during the estrous cycle is scanty, and no study was available for buffaloes in the literature searched. Nevertheless, previous findings in cows had indicated an increase in endometrial thickness in uterine body 3 to 4 days prior to ovulation, a decrease 1 to 3 days after ovulation, and constant ET during diestrus in cows (Souza et al. 2011). However, in the present study, correlation between PMN% and endometrial thickness was low, since ultrasound and cytology measure two different representations of SCE, i.e., clearance mechanism of the uterus (luminal fluid) and cellular response of the inflamed uterus (PMNs in cytology slides), respectively (Kasimanickam et al. 2004; Barlund et al. 2008). However, use of ultrasonography for SCE diagnosis has not been explored much, since it could easily be influenced by location of probe on the uterine horn. Consequently, ultrasonography alone was not considered accurate unless accompanied by endometrial cytology (Barlund et al. 2008). The buffaloes suffering from SCE in the present experiment tended to have a larger uterine horn diameter at estrus compared to control. Almost similar values for right (19.8 ± 0.43 mm) and left horn diameters (18.7 ± 0.37 mm) in buffaloes at estrus were reported, and the dimensions also did not vary with respect to stage of estrus (Honparkhe et al. 2004). Abayawansa et al. (2012) also reported comparable diameters of non-gravid uterine horn (on 56 dpp) in buffaloes having calvings in winter (22.76 ± 0.94 mm) and summer (21.43 ± 0.88 mm). No report regarding the uterine horn diameter in subclinical endometritic-affected bovines was available in the literature searched.
The present finding contradicted the earlier reports in which uterine infection was suggested to perturb ovarian follicular growth and function in cows and buffaloes (Sheldon et al. 2002, 2009). The contradiction may be attributed to less severity of subclinical endometritis as compared to overt clinical endometritis in aforesaid studies. Uterine infection and associated bacterial products suppressed follicular growth, decreased estradiol production, and inhibited LH surge and ovulation, thereby causing persistence of dominant follicle leading to interference with the estrous cycle (Peter et al. 1989; Suzuki et al. 2001). The effect of uterine infection on follicle growth and function was believed to be mediated through a centralized effect by disruption of LH secretion or a direct effect on the ovary (Battaglia et al. 2000). Sampling at insemination may be ideal as it offers the opportunity to determine the uterine health status at the moment when normal uterine involution would not interfere with the cytological results. Moreover, fertilization takes place at this point which allows studying the precise effect of SCE on the resultant conception rate, and hence, samples harvested at the time of AI may better reflect the health of endometrium in relation to conception (Pascottini et al. 2016). Whereas, SCE diagnosed during the postpartum period could resolve before insemination at the ensuing estrus. Furthermore, cytobrush sampling at estrus (prior to AI) was comparatively easy, fast (due to open cervix), and yields high-quality samples (due to absence of erythrocytes in cytosmears) as compared to postpartum sampling.
In conclusion, the present investigation indicated that use of endometrial cytology (≥ 5 PMN% threshold) as an effective technique for diagnosis of subclinical endometritis at estrus in buffaloes and SCE has negative impact on reproductive performance.
References
Abayawansa, W.D., Prabhakar, S., Singh, A.K. and Brar, P.S., 2012. Seasonal variations in uterine involution in buffalo following normal puerperium. Indian Journal of Animal Sciences, 82: 859–862.
Azawi, O.I., Ali, A.J. and Lazim, E.H., 2008. Pathological and anatomical abnormalities affecting buffalo cows reproductive tracts in Mosul. Iraqi Journal of Veterinary Science, 22: 59–67.
Baranski, W., Podhalicz-Dziegielewska, M., Zdunczyk, S. and Janowski, T., 2012. The diagnosis and prevalence of subclinical endometritis in cows evaluated by different cytologic thresholds. Theriogenology, 78: 1939–1947.
Barlund, C.S., Carruthers, T.D., Waldner, C.L. and Palmer, C.W., 2008. A comparison of diagnostic techniques for postpartum endometritis in dairy cattle. Theriogenology, 69: 714–723.
Barrio, M., Marcos, V., Quintela L.A., Becerra, J.J., Pedro, J., Herradón G., Martínez-Bello, D., Fernandez-Sanchez, F.I., Prieto, A., Cainzos, J. and Peña, A.I., 2015. Influence of subclinical endometritis on the reproductive performance of dairy cows. Spanish Journal of Agricultural Research, 13: e05SC02.
Battaglia, D.F., Krasa, H.B., Padmanabhan, V., Viguie, C. and Karsch, F.J., 2000. Endocrine alterations that underlie endotoxin-induced disruption of the follicular phase in ewes. Biology of Reproduction, 62: 45–53.
Brodzki P, Krzysztof, N., Krzysztof K.,, Brodzki, A., Kurek, L. and Marczuk, J., 2014. Cytological evaluation of inflammation of the uterus and influence of endometritis on selected reproductive parameters in dairy cows. Bulletin of Veterinary Institute, Pulawy, 58: 235–242.
Carneiro L.C., Ferreira, A.F., Padua, M., Saut, J.P., Ferraudo, A.S. and dos Santos, R.M., 2014. Incidence of subclinical endometritis and its effects on reproductive performance of crossbred dairy cows. Tropical Animal Health and Production, 46: 1435–1439.
Dar, S.H., Chaudhary, G.R., Mehrotra, S., Qureshi, S. D, Sankar, M, Jan, M.H., Kumar, H., Chaudhary, R.K., Palanivelu, M. and Narayanan, K., 2015. Association of Escherichia coli and Fusobacterium necrophorum with subclinical endometritis in postpartum Murrah buffalo. Indian Journal of Veterinary Pathology, 39: 311–315.
Dubuc, J., Duffield, T.F., Leslie, K.E., Walton, J.S. and Leblanc, S.J., 2011. Randomized clinical trial of antibiotic and prostaglandin treatments for uterine health and reproductive performance in dairy cows. Journal of Dairy Science, 94: 1325–1338.
Gahlot, S.C., Kumar, S., Kumaresan, A., Chand, S., Baithalu R.K., Lathika, S., Patbandha, T.K., Lathwal, S.S. and Mohanty, T.K., 2017. Efficiency of uterine fluid cytology in the diagnosis of subclinical endometritis in the water buffalo (Bubalus bubalis). Reproduction in Domestic Animals, 53(1): 1–4.
Galvao, K.N., Frajblat, M., Brittin, S.B., Butler, W.R., Guard, C.L. and Gilbert, R.O., 2009. Effect of prostaglandin F2α on subclinical endometritis and fertility in dairy cows. Journal of Dairy Science, 92: 4906–4913.
Ghasemi F., Gonzalez-Cano P., Griebel P.J. and Palmer C., 2012. Proinflammatory cytokine gene expression in endometrial cytobrush samples harvested from cows with and without subclinical endometritis. Theriogenology, 78: 1538–1547.
Gilbert, R.O., Shin, S.T., Guard, C.L., Erb, H.N. and Frajblat, M., 2005. Incidence of endometritis and its effects on reproductive performance of dairy cows. Theriogenology, 64: 1879–1888.
Habibzadeh, F., Habibzadeh, P. and Yadollahie, M., 2016. On determining the most appropriate test cut-off value: the case of tests with continuous results. Biochemia Medica: Biochemia Medica, 26(3): 297–307.
Honparkhe, M., Gandotra, V.K. and Nanda, A.S., 2004. Ultrasonographic measurements in comparison with the rectal palpation and echotexture of reproductive organs of buffaloes (Bubalus bubalis) during different stages of the estrous cycle. Asian-Australasian Journal of Animal Sciences, 17(7): 919–923.
Kasimanickam, R., Duffield, T.F., Foster, R.A., Gartley, C.J., Leslie, K.E., Walton, J.S. and Johnson, W.H., 2004. Endometrial cytology and ultrasonography for the detection of subclinical endometritis in postpartum dairy cows. Theriogenology, 62: 9–23.
Kaufmann, T.B., Drillich, M., Tenhagen, B.A., Forderung, D. and Heuwieser, W., 2009. Prevalence of bovine subclinical endometritis 4 h after insemination and its effects on first service conception rate. Theriogenology, 71: 385–391.
Madoz, L., Giuliodori, M., Jaureguiberry, M., Plöntzke, J., Drillich, M. and De la Sota, R., 2013. The relationship between endometrial cytology during estrous cycle and cutoff points for the diagnosis of subclinical endometritis in grazing dairy cows. Journal of Dairy Science, 96, 4333–4339.
Madoz, L.V., Giuliodori, M.J., Migliorisi, A.L., Jaureguiberry, M. and de la Sota, R.L., 2014. Endometrial cytology, biopsy, and bacteriology for the diagnosis of subclinical endometritis in grazing dairy cows. Journal of Dairy Science, 97: 195–201.
McDougall, S., Hussein, H., Aberdein, D., Buckle, K., Roche, J., Burke, C., Mitchell, M. and Meier, S., 2011. Relationships between cytology, bacteriology and vaginal discharge scores and reproductive performance in dairy cattle. Theriogenology, 76, 229–240.
Melcher, Y., Prunner, I. and Drillich, M., 2014. Degree of variation and reproducibility of different methods for the diagnosis of subclinical endometritis. Theriogenology, 82(1): 57–63.
Pascottini O.B., Hostens, M., Dini, P., Van Eetvelde, M., Vercauteren, P. and Opsomer, G., 2016. Prevalence of cytological endometritis and effect on pregnancy outcomes at the time of insemination in nulliparous dairy heifers. Journal of Dairy Science, 99: 9051–9056.
Peter, A.T., Bosu, W.T.K. and DeDecker, R.J., 1989. Suppression of preovulatory luteinizing hormone surges in heifers after intrauterine infusions of Escherichia coli endotoxin. American Journal of Veterinary Research, 50: 368–373.
Plöntzke, J., Madoz, L.V., De la Sota, R.L., Drillich, M. and Heuwieser, W., 2010. Subclinical endometritis and its impact on reproductive performance in grazing dairy cattle in Argentina. Animal Reproduction Science, 122(1–2): 52–57.
Quinn, P.J., Carter, M.E., Markey, B. and Carter, G.R., 1999. Bacterial pathogen, microscopy culture and identification. Text Book of Clinical Veterinary Microbiology. Mosby publication, New York.
Ricci, A., Gallo, S., Molinaro, F., Dondo, A., Zoppi, S. and Vincenti, L., 2015. Evaluation of subclinical endometritis and consequences on fertility in Piedmontese beef cows. Reproduction in Domestic Animals, 50: 142–148.
Salah, N. and Yimer, N., 2017. Cytological endometritis and its agreement with ultrasound examination in postpartum beef cows. Veterinary World, 10(6): 605–609.
Sheldon, I.M., Noakes, D.E., Rycroft, A.N. and Dobson, H., 2002. Effect of postpartum manual examination of the vagina on uterine bacterial contamination in cows. Veterinary Record, 151: 531–534.
Sheldon, I.M., Lewis, G.S., LeBlanc, S. and Gilbert, R.O., 2006. Defining postpartum uterine disease in cattle. Theriogenology, 65: 1516–1530.
Sheldon, I.M., Cronin, J., Goetze, L., Donofrio, G. and Schuberth, H.J., 2009. Defining postpartum uterine disease and mechanisms of infection and immunity in the female reproductive tract in cattle. Biology of Reproduction, 81: 1025–1032.
Singh, H., Brar, P. S, Arora, A.K., Dhindsa, S.S. and Honparkhe, M., 2018. Bacterial presence and fertility in subclinical endometritic buffaloes at oestrus. Indian Journal of Animal Sciences, 88(4): 415–419.
Souza, A.H., Silva, E.P.B., Cunha, A.P., Gümen, A., Ayres, H., Brusveen, D.J., Guenther, J.N. and Wiltbank, M.C., 2011. Ultrasonographic evaluation of endometrial thickness near timed AI as a predictor of fertility in high-producing dairy cows. Theriogenology, 75: 722–733.
Subandrio, A.L., Sheldon, I.M. and Noakes, D.E., 2000. Peripheral and intrauterine neutrophil function in the cow: the influence of endogenous and exogenous sex steroid hormones. Theriogenology, 53: 1591–1608.
Suzuki, C., Yoshioka, K., Iwamura, S. and Hirose, H., 2001. Endotoxin induces delayed ovulation following endocrine aberration during the proestrous phase in Holstein heifers. Domestic Animal Endocrinology, 20: 267–278.
Wagener, K., Gabler, C. and Drillich, M., 2017. A review of the ongoing discussion about definition, diagnosis and pathomechanism of subclinical endometritis in dairy cows. Theriogenology, 94: 21–30.
Westermann, S., Drillich, M., Kaufmann, T.B., Madoz, L.V. and Heuwieser, W.A., 2010. Clinical approach to determine false positive findings of clinical endometritis by vaginoscopy by the use of uterine bacteriology and cytology in dairy cows. Theriogenology, 74, 1248–1255.
Acknowledgements
The authors are thankful to owners of dairy farms included in the study. The authors are also grateful to Head, Department Veterinary Gynecology & Obstetrics, GADVASU, Ludhiana for providing the necessary facilities.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Ethical approval
All applicable international, national, and/or institutional guidelines for the care and use of animals were followed.
Conflict of interest
The authors declare that they have no conflict of interest.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Singh, H., Brar, P.S., Honparkhe, M. et al. Subclinical endometritis in estrual buffaloes: diagnosis, prevalence and impact on reproductive performance. Trop Anim Health Prod 52, 357–363 (2020). https://doi.org/10.1007/s11250-019-02022-w
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11250-019-02022-w