
Abstract
People who self-objectify perceive their bodies as objects which exist for the pleasure of others. Personality traits are important factors that might moderate the pathway between self-objectification and body image concerns. In the present paper, we explore if narcissism moderates this relationship, and we do so by exploring the facets of grandiose narcissism (associated with an inflated sense of self-importance) and hypersensitive narcissism (a more defensive and insecure narcissism). A convenience sample of 277 young Australian women (Mage = 21.34 years, SD = 3.25, range = 18–30) completed an online battery comprising measures of self-objectification, subclinical grandiose and hypersensitive narcissism, and measures designed to capture concerns related to body image. We found that hypersensitive narcissism, but not grandiose narcissism, predicted higher levels of self-objectification. Grandiose narcissism scores predicted lower levels of body shame and less weight discrepancy, indicating more positive body image, and also moderated the relationship between self-objectification and body shame (i.e., women who report lower levels of narcissism are more vulnerable to body shame associated with self-objectification). In contrast, hypersensitive narcissism scores predicted higher levels of both body shame and discrepancies in actual-ideal weight. These findings suggest that grandiose narcissism may have a protective relationship regarding body image in this population, whereas hypersensitive narcissism may be a risk factor.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Body image is a leading concern for young people. For example, around one quarter of young Australians aged 15–19 years-old report feeling very or extremely concerned about their body, with approximately three times more young women than young men reporting body image concerns (Cave et al. 2015). Objectification theory (Fredrickson and Roberts 1997) posits that in modern Western societies, women are sexualised and treated merely “as bodies” that exist for the use and pleasure of others. It is through these interpersonal experiences of being treated as an object (e.g., being gawked and whistled at), in combination with consistently being exposed to sexualized media depictions, that women begin to internalise cultural appearance ideals and thus self-objectify, engaging in a psychological process whereby they perceive their own bodies as objects (Fredrickson and Roberts 1997). This theoretical framework, and its related psychological processes that focus on the body, serve as a useful vehicle to explore the socio-psychological phenomenon which drives prevalent body image concerns among women (Aubrey and Frisby 2011; Graff et al. 2013; Hatton and Trautner 2011).
Persistent self-objectification (i.e., trait self-objectification) is theorised to contribute to a series of negative outcomes (Fredrickson and Roberts 1997). Theoretical conceptualizations predict that women learn to internalize an observer’s perspective, which then facilitates a host of negative mental health outcomes for the self, such as body shame and depression. In addition, Moradi and Huang (2008) suggest that self-objectification provokes interaction effects with related constructs (such as body surveillance) which result in a series of follow-on effects including increases in public self-consciousness (Breines et al. 2008) and decreases in flow of consciousness (Fredrickson and Roberts 1997). They then theorise that these effects can result in more serious dysfunction, including serious body image concerns and eating disorders (Muehlenkamp and Saris–Baglama 2002).
Indeed, these theoretical predictions have been ratified empirically. For example, previous studies have linked self-objectification and depressive symptomology (Jones and Griffiths 2015), decreased well-being (Breines et al. 2008), a reduction in sexual self-esteem (Calogero and Thompson 2009), and an increase in some risky sexual behaviours (e.g., having sex under the influence of alcohol; Anderson et al. 2017). One key correlate of self-objectification is negative body image, as women who are more conscious of their bodies engage in more self-scrutiny (Grippo and Hill 2008). More specifically, self-objectification has been linked to different operationalisations of negative body image including body shame (Noll and Fredrickson 1998), body dissatisfaction (Grippo and Hill 2008), and an increase in the discrepancy between one’s actual and ideal weight (McKinley 1998). There is also evidence linking trait self-objectification with the development of eating disorders (Noll and Fredrickson 1998; Tiggemann and Lynch 2001).
Considering the high prevalence of eating disorders, particularly among young women (Deloitte Access Economics 2012), it is important to identify which factors may influence the pathway between self-objectification and body image in order to inform interventions. For example, it is understood that these associations tend to occur more strongly among women with low self-esteem (Breines et al. 2008) and with fewer stereotypically masculine traits (Choma et al. 2010). Personality traits are individual differences in consistent patterns of emotions, thoughts, and behaviours (Cattell et al. 1970; Costa and McCrae 2008; Eysenck 1950), and these individual differences are factors that might influence this pathway. A series of personality traits have previously been empirically associated with self-objectification, including perfectionism (Davis et al. 2001, 2005), neuroticism (Davis et al. 2005; Tylka 2004), and narcissism (Davis et al. 2001; Fox and Rooney 2015; Lipowska and Lipowski 2015). Certain personality traits have also been established as correlates of negative body image; a recent systematic review of Big Five traits reported that higher levels of neuroticism and lower levels of extraversion were associated with negative body image (Allen and Walter 2016). Other studies have identified associations between negative body image and narcissism (Swami et al. 2015; see Carrotte and Anderson 2018 for a recent review). Narcissism, and its role in the self-objectification→body image relationship, is of key interest to the present study.
Narcissism, Self-Objectification, and Body Image
Researchers are reporting that narcissism rates are on the rise. For example, Twenge et al. (2008) have reported that narcissism scores in American college students were 30% higher in 2006 than in 1979. Moreover, claims have been made that narcissism rates are rising as rapidly as obesity, and these inflation rates have been labelled an epidemic (Twenge and Campbell 2008, see also Twenge and Foster 2010). At its most extreme, narcissism is associated with the development of Narcissistic Personality Disorder, involving both personal and interpersonal distress (American Psychiatric Association 2013). However, narcissistic traits also occur along a continuum in subclinical populations.
Distinctions have been made between grandiose and hypersensitive types of narcissistic traits. Grandiose narcissism is associated with an inflated sense of self-importance, dominance, and entitlement (Dickinson and Pincus 2003; Wink 1991). To contrast, hypersensitive narcissism (also referred to throughout the literature as vulnerable, covert, or hypervigilant narcissism) involves a more defensive and insecure narcissism that is associated with low-self-esteem and shame (Dickinson and Pincus 2003; Wink 1991). Hypersensitive narcissism is associated with outward humility and inhibition, which masks underlying grandiose views and entitlement (Dickinson and Pincus 2003). It is possible that both of these distinct traits influence individuals’ levels of self-objectification and related body image outcomes in different ways (Swami et al. 2015; Zeigler-Hill et al. 2008).
Several studies have explored grandiose narcissism in this domain. Although research readily identifies positive associations between grandiose narcissism and self-objectification (Davis et al. 2001, 2005; Lipowska and Lipowski 2015), mixed results have been produced concerning the relationship between grandiose narcissism and both body image and eating disorder-related outcomes. For example, some studies have reported no relationship between grandiose narcissism with drive for thinness (Gordon and Dombeck 2010; Swami et al. 2015), body dissatisfaction and weight discrepancy (Swami et al. 2015), and disordered eating (Gordon and Dombeck 2010). Conversely, other studies have found that grandiose narcissism is related to increases in positive body image, including more body esteem (Davis et al. 1996) and satisfaction (Jackson et al. 1992). It is possible that grandiose narcissism may have a type of “protective” effect, buffering against the development of negative body image in the presence of self-objectification. Thus, establishing the existence of this effect is one of the major aims of our paper. Grandiose narcissism may also inflate self-esteem (Bosson et al. 2008), resulting in a neutral or even positive body image, regardless of self-objectification levels.
To our knowledge, no studies have explored the relationship between hypersensitive narcissism and self-objectification. Despite recent evidence suggesting that narcissism might be higher in men than in women (Grijalva et al. 2015), we are interested in this relationship because it is likely that young women exhibiting high levels of hypersensitive narcissism may be more sensitive to the societal cues which celebrate narrow appearance ideals than are men and because women face the heightened possibility of rejection if they do not meet these ideals. Thus, these women who are high in hypersensitive narcissism may base their self-worth upon their appearance (Gordon and Dombeck 2010; Swami et al. 2015). The evidence reveals associations between hypersensitive narcissism and preoccupation with one’s weight (Davis et al. 1997), drive for thinness and disordered eating (Gordon and Dombeck 2010), and actual-ideal weight discrepancy (Swami et al. 2015), yet research in the objectification literature that simultaneously explores the multi-dimensional nature of narcisissm is absent from the literature. We argue that it is vital to fully understand the complexities of narcissism and thus to explore the connection between the various forms of narcissism with self-objectification and body image-relevant outcomes with a sample of young women, a second major aim of our paper.
Aims and Hypotheses
In the present study we explored the relationship between facets of subclinical narcissism, self-objectification, and two types of negative body image: body shame and actual-ideal weight discrepancy. Each of these body image concerns have been conceptually linked to self-objectification (Fitzsimmons-Craft 2011; Fitzsimmons-Craft et al. 2012; Tylka and Hill 2004). For example, self-objectification often manifests as routine body surveillance in which self-objectifing individuals engage in a self-comparison against an unrealistic thin-ideal. Given that these cultural ideals are uncharacteristic of what women typically look like, self-objectifying women are likely to experience disappointment in their bodies (e.g., body shame). Indeed, increases in the frequency or severity of self-objectification (and thus body surveillance) heighten prospects for experiencing body shame. Similarly, this consistent comparison against an unrealistic ideal can lead to cognitive distortions about what an individual might or should perceive as their ideal weight, thus further driving discrepancies between their actual and ideal weight.
In addition, we aimed to determine whether facets of subclinical narcissistic personality traits moderate this established relationship between self-objectification and body image-related outcomes in young women. We are interested in narcissism because of the tendency for narcissists to habitually compare themselves to others and because of their drive to attain cultural ideals (such as thinness) in order to gain social approval. These behaviours lend themselves well to self-objectifying and body-surveillance tendencies, and indeed the two have been empirically linked (see Carrotte and Anderson 2018, for a review). However, based on knowledge that narcissist also inhibit emotions related to feeling inferior to others (Swami et al. 2015), it is tempting to assume that individuals with higher levels of sub-clinical narcissism are protected from the negative impacts of self-objectification.
In the present paper, we have highlighted that there are certain elements of narcissism that vary between the facets that might results in differential moderation effects. For example, research has demonstrated that the protective factors associated with narcissism (e.g., improved psychological health) only exist in individuals with higher levels of self-esteem (Sedikides et al. 2004). Thus, we argue that whereas grandiose narcissism might be protective against the negative consequences of self-objectification on body image, this might not be true for all facets of narcissism. In the present paper, we will test this postulation by exploring if vulnerable narcissism (associated with more defensiveness, insecurity, and shame than grandiose narcissism; Maples et al. 2014) might actually place individuals who score higher in this trait at greater risk.
Based on the existing literature and the arguments we made here, we formulated a series of hypotheses. First, in our objectification hypotheses (Hypothesis 1), we predict that that self-objectification will correlate with body shame (Hypothesis 1a) and actual-ideal weight discrepancy scores (Hypothesis 1b). Second, in our narcissism hypotheses (Hypothesis 2), we predict that grandiose narcissism and hypersensitive narcissism scores will both be positively associated with self-objectification scores (Hypothesis 2a: Davis et al. 2001, 2005; Lipowska and Lipowski 2015). We hypothesise that grandiose narcissism could be a protective factor against body concerns and thus scores will be negatively associated with body shame and actual-ideal weight discrepancy scores, indicative of a more positive body image (Hypothesis 2b: Davis et al. 1996; Jackson et al. 1992). We also hypothesise that hypersensitive narcissism will be positively associated with both body shame and actual-ideal weight discrepancy, indicating more negative body image (Hypothesis 2c: Davis et al. 1997; Gordon and Dombeck 2010; Swami et al. 2015).
Third, in our moderation hypotheses (Hypothesis 3), we predict that narcissism will moderate the relationship between self-objectification and body image outcomes. Again, based on the idea that grandiose narcissism may be protective in this context, we hypothesise that grandiose narcissism will moderate this relationship, with the magnitude of the correlation being attenuated when higher levels of grandiose narcissism are present (Hypothesis 3a). Finally, we hypothesise that hypersensitive narcissism will moderate this relationship, with the magnitude of the correlation being ameliorated when higher levels of hypersensitive narcissism are present (Hypothesis 3b).
Method
Participants and Procedure
We recruited female participants who were aged 18–30. Participants accessed the online questionnaire (reviewed by the human research ethics committee at Australian Catholic University: 2016-264E) and after giving consent, participants provided demographic details and then were presented with the measures detailed in the following in a randomised order. The sample comprised 277 participants (Mage = 21.34 years, SD = 3.25), which is sufficient to detect medium-sized effects with five predictor variables (i.e., n > 200, based on n > 50 + 8 k: 277 > 50 + [8 × 5]; Field 2013). The majority of participants (n = 167) were undergraduate psychology students, who participated in exchange for research participation credit, and the remainder were recruited via social media and were offered entry into a prize draw to win one of five AUD$50 vouchers. (The student and non-student parts of the sample did not differ on any key variables; ps > .476.) Most participants were Caucasian (n = 208), followed by Asian (n = 32); mixed heritage (n = 7); Latina/Hispanic, Middle Eastern or African (n = 5 each); and other (n = 2). Most participants were heterosexual (n = 242, 87%), followed by bisexual (n = 23), lesbian (n = 3) or other sexual orientation (n = 9). Most had not completed any post-high school studies (n = 199, 72%) and reported their relationship status as either single or dating (n = 160, 58%).
Measures
Self-Objectification
The Self-Objectification Questionnaire (SOQ) was used to assess trait-based differences in self-objectifying processes (Noll and Fredrickson 1998). Participants rank 12 body attributes in order of how important each is to their physical self-concept, from most important (rank = 1) to least important (rank = 12). Half of the attributes represent physical appearance (e.g., physical attractiveness, sex appeal) and the rest represent physical competence (e.g., muscular strength, health). This scale measures the degree to which respondents place importance on their physical appearance relative to their physical competence (such that an appearance > competence focus represents self-objectification). Scoring involved adding the rank value of all competence items and all appearance items, then calculating the difference between each set of items. Possible scores range from −36 to +36, with higher scores reflecting more self-objectification. The SOQ possesses adequate construct validity (Noll and Fredrickson 1998; Tiggemann and Lynch 2001). Because of the rank-order nature of the responses to the scale, internal consistency cannot be calculated. In accordance with Hill and Fischer (2008), correlations between the sum of appearance-based items and the sum of competence-based items were calculated as a proxy for an estimate of internal consistency; a perfect negative correlation was obtained between the two sets of items, r(275) = −1.00, p < .001.
Body Image
Because of diverse operationalisations of body image, two measures were chosen for our study. First, the Body Shame subscale of the Objectified Body Consciousness Scale (OBCS; McKinley and Hyde 1996) was used to assess aversion and contempt toward one’s body. This subscale contains eight items rated on a 7-point scale ranging from 1 (strongly disagree) to 7 (strongly agree; e.g., “I feel like I must be a bad person if I don’t look as good as I could”). Scores were averaged, with higher scores indicating more shame felt toward one’s body. The scale yielded acceptable internal consistency in our sample (Cronbach’s α = .85).
Second, the Photographic Figure Rating Scale (PFRS; Swami et al. 2008) was used to measure actual-ideal weight discrepancy, a form of weight dissatisfaction. The scale consists of ten greyscale photographs of women with smaller body types (1) to larger body types (10). Participants first select which image they feel represents their current body, and then they select the image which represents their ideal body. Actual-ideal weight discrepancy is calculated by the difference between the two selections, with higher, positive scores indicating greater weight discrepancy because of perceptions of one’s body being too large. Internal consistency estimates cannot be calculated for this scale because of its design but the scale has demonstrated good construct validity and test-retest reliability in prior research (test-retest rs = .85–.90 over a period of 3 weeks; Swami et al. 2008).
Narcissism
The Narcissistic Personality Inventory-13 (NPI-13; Gentile et al. 2013) is a shortened form of the Narcissistic Personality Inventory (NPI-40; Raskin and Terry 1988), a widely-used 40-item scale measuring grandiose subclinical narcissism. The Grandiose/Exhibitionism subscale was used in the present study, which comprises five forced-choice dyads, such as participants must agree with either “I will usually show off if I get the chance” (scored 1) or “I try not to be a show off” (scored 0). Scores were summed, with possible score range of 0–5, with higher scores reflecting higher levels of grandiose narcissism. We used a Kuder-Richardson Formula 20 (KR-20) to calculate internal consistency estimates, and the alpha for the subscale in our sample was .68. Although this is slightly below the standard cut-off (i.e., .70; Cronbach 1990), we also note that the mean inter-item correlation (M = .29) and the range of these correlations (.16–.46) fall within the recommendations suggested by Clark and Watson (1995; suggestion of Minter-item correlation between .15–.50, and range between .15–.85). In combination with the knowledge that a small number of items decreases the internal consistency estimate (Kline 2015), we used this scale despite its weaker alpha.
The Hypersensitive Narcissism Scale was used to measure subclinical hypersensitive narcissism (HSNS; Hendin and Cheek 1997). The HSNS comprises ten items that participants endorse on a scale ranging from 1 (very uncharacteristic or untrue, strongly disagree) to 5 (very characteristic or true, strongly agree; e.g., “I often interpret the remarks of others in a personal way”). Scores were summed, with higher scores reflecting higher levels of hypersensitive narcissism. The scale demonstrated acceptable internal consistency in our sample (Cronbach’s α = .71). The scale did not significantly correlate with the NPI-13 Grandiose/Exhibitionism subscale (Table 1), suggesting these scales represent different constructs.
Data Analyses
Data were analysed in IBM SPSS Statistics v20. We used Pearson product-moment correlations with bootstrapped confidence intervals to explore bivariate correlations between continuous variables. For multivariate analyses, we analysed data with hierarchical multiple linear regressions based on the ordinary least squares model. Interaction terms (self-objectification x both narcissism scales) were used in the latter two regressions to explore moderation effects, and we unpacked moderation analyses with the PROCESS macro by Hayes (2012; analyses set to 5000 bootstrap samples). We performed analyses using centred data (Aiken and West 1991; Field 2013), but since there were no meaningful differences to analyses using non-centred data, we opted to present the analyses using non-centred data for ease of interpretability.
To reduce the risk of Type 1 error, we adjusted p-values using Bonferroni corrections. To do so, we created “families” of analyses according to our hypotheses, with four families for univariate analyses and six for multivariate analyses. Eight of these families involved a pair of analyses and so for these analyses we used a critical alpha of .025 (i.e., p = .05/2) for each individual analysis. Moderation analyses involved only one analysis per family, thus we used the standard alpha value (i.e., p < .05) for these analyses.
Results
Univariate Analyses
Univariate analyses are presented in Table 1. Negative correlations were observed between age and self-objectification. Significant positive correlations were observed between self-objectification with both body shame (supporting Hypothesis 1a; medium effect) and actual-ideal weight discrepancy (supporting Hypothesis 1b, small effect). A small, but significant positive correlation existed between self-objectification and hypersensitive narcissism, but not grandiose narcissism, partially supporting Hypothesis 2a. Grandiose narcissism was negatively related to actual-ideal weight discrepancy and body shame (moderate and small correlations, respectively), supporting Hypothesis 2b. A medium-sized, significant positive correlation existed between hypersensitive narcissism and body shame, and a small, significant positive correlation was observed between hypersensitive narcissism and actual-ideal weight discrepancy, supporting Hypothesis 2c.
Multivariate Analyses
To further explore Hypothesis 2a, a hierarchical linear regression was conducted with self-objectification as the dependent variable (see Table 2). Before conducting this analysis, we explored for demographic variables that were systematically related to the key variables of our study. Age was correlated with SOQ (see Table 1), and in Mann-Whitney U-tests, ethnic majority status members had significantly higher mean rank scores on both types of narcissistic traits (ps < .046); no other demographic variables were related to the dependent or independent variables. Thus, both age and ethnicity were controlled for in Step 1, and these variables accounted for a significant 3.90% of the variance in self-objectification scores, F(2, 260) = 5.30, p = .006. Both types of narcissism were entered in Step 2, and this model accounted for an additional significant 7.60% variance, ΔF(2, 258) = 11.11, p < .001. Overall, predictor variables accounted for 11.50% variance in self-objectification, a small effect (Cohen’s f2 = .13).
As we anticipated, once entered in Step 2, hypersensitive narcissism positively predicted self-objectification scores, contributing a unique 7.56% of the variance in self-objectification (sr2 = .08). Unexpectedly, grandiose narcissism scores did not predict self-objectification in this analysis. In sum, these findings partially support Hypothesis 2a.
To further explore Hypothesis 2b–Hypothesis 3b, we conducted two hierarchical linear regressions, with the first involving OBCS Body Shame as the dependent variable and the second involving PFRS actual-ideal weight discrepancy as the dependent variable. Because age and ethnicity both demonstrated significant relationships with the variables of interest, these were originally included in both analyses in Step 1. However, they were unrelated to the dependent variables, and thus these variables were removed from final analyses to simplify presentation of findings.
In the first of these regressions (see Table 3) variables in Step 1 accounted for a significant 12.80% of the variance in body shame, F(1, 255) = 37.30, p < .001. Both types of narcissism were entered in Step 2, and this step accounted for an additional significant 14.20% of the variance, ΔF(1, 253) = 24.65, p < .001. Interaction terms were entered in Step 3, which accounted for a significant additional 1.80% variance, ΔF(1, 251) = 3.26, p = .04. In combination, predictor variables accounted for 28.80% variance in body shame, which can be considered a large effect (Cohen’s f2 = .40).
In Steps 1 and 2, self-objectification significantly predicted body shame (supporting Hypothesis 1a), although this relationship was no longer significant in Step 3 once interaction terms were introduced. In both Steps 2 and 3, grandiose narcissism predicted lower levels of body shame (uniquely accounting for 6.60% variance in Step 2 and 6.97% variance in Step 3), supporting Hypothesis 2b. To contrast, hypersensitive narcissism predicted higher levels of body shame, accounting for 6.81% variance in body shame in Step 2 and 7.02% variance in Step 3 (supporting Hypothesis 2c). The interaction between self-objectification and hypersensitive narcissism was not significant.
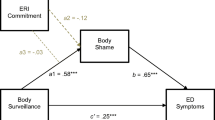
However, the interaction between self-objectification and grandiose narcissism was significant, accounting for 1.85% variance in body shame. The significant increase in variance accounted for by the interaction term suggests that the effect of self-objectification on body shame depends on the level of grandiose narcissism, and thus simple slopes for the association between self-objectification and body shame were tested at low (M - 1SD), moderate (M), and high (M + 1SD) levels of grandiose narcissism. Figure 1 shows the simple slopes for the interaction. Supporting Hypothesis 3a, simple slope tests revealed a significant positive effect of self-objectification on body shame that increases as levels of grandiose narcissism decrease. Specifically, the relationship was strongest when levels of grandiose narcissism were low (b = .25, SEb = .04, p < .001), compared to both moderate (b = .18, SEb = .03, p < .001), and high (b = .12, SEb = .04, p = .003).

Moderating effects of grandiose narcissism on the relationship between self-objectification and body shame. Low scores = M – 1SD, high scores = M + 1SD. NPI = narcissistic personality inventory (NPI) grandiose/exhibitionism subscale. All simple slopes are significant, but the relationship between self-objectification and body shame was strongest among women scoring lower in grandiose narcissism compared to both moderate and higher scoring women
In the final regression (see Table 4), variables in Step 1 accounted for a significant 3.60% of the variance in weight discrepancy, F(1, 273) = 10.25, p = .002. Both types of narcissism were entered in Step 2, and this step accounted for an additional significant 13.50% variance, ΔF(2, 271) = 21.99, p < .001. Interaction terms were entered in Step 3, which accounted for an additional non-significant 1.60% variance, ΔF(2, 269) = 2.57, p = .08. In combination, predictor variables accounted for 18.60% variance in weight discrepancy, which can be considered a medium effect (Cohen’s f2 = .23).
In all steps of the model, self-objectification significantly predicted actual-ideal weight discrepancy (supporting Hypothesis 1b). In both Steps 2 and 3, grandiose narcissism predicted lower levels of weight discrepancy (uniquely accounting for 12.46% variance in Step 2 and 12.53% in Step 3), supporting Hypothesis 2b. To contrast, hypersensitive narcissism did not predict weight discrepancy, contrary to Hypothesis 2c. Interaction terms were not significant predictors of weight discrepancy, contrary to Hypotheses 3a and 3b.
Discussion
Our study aimed to explore the relationship among narcissism, self-objectification, and body image-related outcomes in a sample of young women. Specifically, we explored whether hypersensitive and grandiose forms of narcissism moderate the relationship between self-objectification and two operationalisations of body image. Our objectification hypotheses were supported, and our narcissism and moderation hypotheses were partly supported. Specifically, we have corroborated the literature which documents that self-objectification processes are related to increases in body-image outcomes (Hypothesis 1a and b). We have added to the body of evidence exploring the relationship between self-objectification and narcissism by showing that self-objectification is related to the hypersensitive facet of narcissism, but not to the grandiose facet (at least, in our sample; supporting Hypothesis 2a). Finally, we have contributed to the literature by presenting evidence that hypersensitive narcissism moderated the relationship between self-objectification and body shame (supporting Hypothesis 3b). We argue that this is evidence that hypersensitive narcissism may be a risk factor for body image concerns, as well as conversely that grandiose narcissism might be a protective factor.
With regard to hypersensitive narcissism, our results were mostly as we anticipated. First, we found that hypersensitive narcissism was associated with higher levels of self-objectification at both the univariate and multivariate levels, supporting Hypothesis 2a. Although this was only a small effect, this finding is novel but expected, considering those higher in hypersensitive narcissism may be more sensitive to external stimuli such as the pressure to value and monitor one’s appearance (Swami et al. 2015). Moreover, participants higher in hypersensitive narcissism reported more body shame compared to those lower in the trait. However, hypersensitive narcissism predicted weight discrepancy in univariate analyses, but not in multivariate analyses, suggesting that this relationship is reduced when controlling for self-objectification and grandiose narcissism. These findings partially support Hypothesis 2c. They also contribute toward a growing body of literature that has demonstrated hypersensitive narcissism is associated with negative body image (Davis et al. 1997; Gordon and Dombeck 2010), suggesting that these women may be particularly vulnerable to feelings of guilt and shame regarding the body, rather than weight dissatisfaction. These results also suggest that women with higher levels of hypersensitive narcissism may be more vulnerable to other factors associated with self-objectification and poor body image, and as such, future research should consider if individuals high in hypersensitive narcissism are also more vulnerable to factors such as depression and disordered eating (Jones and Griffiths 2015).
With regard to grandiose narcissism, results provided mixed support for our hypotheses. The lack of a significant relationship between grandiose narcissism and self-objectification was unexpected and contrary to Hypothesis 2a, considering that a small but consistent body of literature has found associations with self-objectification in women (Davis et al. 2001; Davis et al. 2005; Lipowska and Lipowski 2015). It is possible that this finding is a result of study limitations (discussed in the following). Furthermore, grandiose narcissism was associated with lower levels of both body shame and weight discrepancy at the multivariate level, representing more positive body image. This result supported Hypothesis 2b and is consistent with two known studies (Davis et al. 1996; Jackson et al. 1992). It is possible that having pre-existing positive body image results in exacerbation of grandiose traits. It is also possible that subclinical grandiose narcissism may be adaptive or “healthy” in this context, promoting positive body image (Ackerman et al. 2010; Bosson et al. 2008; Watson et al. 1998).
We observed one significant interaction, with grandiose narcissism moderating the relationship between self-objectification and body shame. This result indicated that the relationship between self-objectification and body shame is stronger in the presence of moderate and lower levels of grandiose narcissism. In other words, women who report less narcissism are especially vulnerable to the negative impacts of body shame that are associated with self-objectification. This again suggests that grandiose narcissism may be “healthy” or “protective” in this context; perhaps individuals higher in this trait are less likely to experience negative body-related thoughts when self-objectifying. Contrary to expectations, other interaction terms were not significant. The results of our study suggest that the relationship between self-objectification and body image-related outcomes is generally similar regardless of participants’ narcissistic personality traits. It may be that contrary to hypotheses, hypersensitive narcissism does not significantly impact the development of body image concerns as a result of self-objectification. Other variables such as neuroticism (Davis et al. 1996) and self-esteem (Breines et al. 2008) may be stronger moderators relative to narcissism, but these need to be compared within the same study.
Research Limitations and Future Research Directions
The interpretability of our study was limited by several factors. As a cross-sectional study, causality cannot be determined, and data may have been influenced by recall and subjectivity. The majority of participants were Australian undergraduate students, and all were under age 30, limiting the generalisability of results. We did not screen for participants with personality disorders, meaning the study may not have examined subclinical personality traits as accurately as intended. It is important to note that if grandiose narcissism reaches pathological levels—that is, if grandiose narcissism is more extreme, more defensive, and causes more distress—young women may experience poor body image, including more weight discrepancy and a higher drive for thinness (Swami et al. 2015). This relationship could not be explored in the current study, which only assessed subclinical narcissism.
Future studies should continue to explore potential moderators of the self-objectification and body image relationship, including personality traits, within both clinical and subclinical samples. It will be important to extend our study to a male sample, considering men tend to exhibit higher levels of grandiose, but not hypersensitive, narcissism (Grijalva et al. 2015) and more muscularity-based body image concerns. Given our evidence that reporting higher levels of grandiose narcissism buffers the negative consequences of self-objectification (at least in terms of body image concerns), and knowledge that men are more often higher in this trait, this could partly explain why women tend to experience body image concerns more than men. Future research could also explore these relationships in relation to body mass index, femininity and masculinity, neuroticism, and self-esteem.
Practice Implications
Our study contributes toward understandings of objectification theory and the factors that may influence the development of both self-objectification and body image outcomes in women. These results add to a growing body of literature indicating associations between personality traits and body image-related variables (e.g., Allen and Walter 2016). Our results also expand upon the personality literature by further supporting the idea that grandiose narcissism can be somewhat protective or adaptive in the subclinical context.
For clinicians working in the field of body image or disordered eating, the results of our study may be useful in informing practice. For example, during assessment, it may be useful to assess clients’ personality traits, particularly hypersensitive narcissism, in order to understand how they internalise and interpret objectifying messages. Some eating disorder treatment protocols include content aimed to reduce the relationship between personality traits and body image—for example, enhanced cognitive behaviour therapy (CBT-E, Fairburn 2009) includes content addressing clinical perfectionism. Cognitions and behaviours associated with hypersensitive narcissism may be a useful target in future treatment protocols. This may involve reinterpreting others’ comments in a more realistic manner and reducing reassurance-seeking behaviours in the context of body image and eating. Moreover, for clinicians working with clients exhibiting higher levels of hypersensitive narcissism outside of eating disorder services, it may be useful to consider clients’ self-objectification and body image as targets for treatment as a means of early intervention.
Conclusions
We found that in a sample of young Australian women, hypersensitive narcissism was associated with higher levels of self-objectification and poorer body image, as represented by body shame. Grandiose narcissism was associated with more positive body image (less body shame and less actual-ideal weight discrepancy) and moderated the relationship between self-objectification and body shame. We have interpreted this last finding as evidence that grandiose narcissism may play a somewhat protective role against negative body image concerns that are related to self-objectification. Conversely, hypersensitive narcissism was associated with more negative body image (more body shame and more actual-ideal weight discrepancy), suggesting that this facet of subclinical narcissism is a risk factor for negative body image concerns among young women.
References
Ackerman, R. A., Witt, E. A., Donnellan, M. B., Trzesniewski, K. H., Robins, R. W., & Kashy, D. A. (2010). What does the narcissistic personality inventory really measure? Assessment, 18(1), 67–87. https://doi.org/10.1177/1073191110382845.
Aiken, L. S., & West, S. G. (1991). Multiple regression. Beverly Hills: Sage Publishing.
Allen, M. S., & Walter, E. E. (2016). Personality and body image: A systematic review. Body Image, 19, 79–88. https://doi.org/10.1016/j.bodyim.2016.08.012.
American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders (5th ed.). Washington, DC: American Psychiatric Publications.
Anderson, J. R., Holland, E., Koc, Y., & Haslam, N. (2017). iObjectify: Exploring self- and other-objectification of men on Grindr, a geosocial networking application designed for men who have sex with men. European Journal of Social Psychology. Advance online publication. https://doi.org/10.1002/ejsp.2350.
Aubrey, J. S., & Frisby, C. M. (2011). Sexual objectification in music videos: A content analysis comparing gender and genre. Mass Communication and Society, 14(4), 475–501. https://doi.org/10.1080/15205436.2010.513468.
Bosson, J. K., Lakey, C. E., Campbell, W. K., Zeigler-Hill, V., Jordan, C. H., & Kernis, M. H. (2008). Untangling the links between narcissism and self-esteem: A theoretical and empirical review. Social and Personality Psychology Compass, 2(3), 1415–1439. https://doi.org/10.1111/j.1751-9004.2008.00089.x.
Breines, J. G., Crocker, J., & Garcia, J. A. (2008). Self-objectification and well-being in women's daily lives. Personality and Social Psychology Bulletin, 34(5), 583–598. https://doi.org/10.1177/0146167207313727.
Calogero, R. M., & Thompson, J. K. (2009). Sexual self-esteem in American and British college women: Relations with self-objectification and eating problems. Sex Roles, 60(3), 160–173. https://doi.org/10.1007/s11199-008-9517-0.
Carrotte, E., & Anderson, J. R. (2018). A systematic review of the relationship between trait self-objectification and personality traits. Personality and Individual Differences, 132, 20–31. https://doi.org/10.1016/j.paid.2018.05.015.
Cattell, R. B., Eber, H. W., & Tatsuoka, M. M. (1970). Handbook for the sixteen personality factor questionnaire (16 PF): In clinical, educational, industrial, and research psychology, for use with all forms of the test. Chapaign: Institute for Personality and Ability Testing.
Cave, L., Fildes, J., Luckett, G., & Wearring, A. (2015). Mission Australia's 2015 youth survey report. Sydney: Mission Australia. Retrieved from https://www.missionaustralia.com.au.
Choma, B. L., Visser, B. A., Pozzebon, J. A., Bogaert, A. F., Busseri, M. A., & Sadava, S. W. (2010). Self-objectification, self-esteem, and gender: Testing a moderated mediation model. Sex Roles, 63(9), 645–656. https://doi.org/10.1007/s11199-010-9829-8.
Clark, L. A., & Watson, D. (1995). Constructing validity: Basic issues in objective scale development. Psychological Assessment, 7, 309–319. https://doi.org/10.1037/1040-3590.7.3.309.
Costa, P. T., & McCrae, R. R. (2008). The revised NEO personality inventory (NEO-PI-R). In G. J. Boyle, G. Matthews, & D. H. Saklofske (Eds.), The SAGE handbook of personality theory and assessment (Vol. 2, pp. 179–198). New York, NY: Sage Publications.
Cronbach, L. (1990). Essentials of psychological testing. New York: Happer and Row publishers.
Davis, C., Claridge, G., & Brewer, H. (1996). The two faces of narcissism: Personality dynamics of body esteem. Journal of Social and Clinical Psychology, 15(2), 153–166. https://doi.org/10.1521/jscp.1996.15.2.153.
Davis, C., Claridge, G., & Cerullo, D. (1997). Reflections on narcissism: Conflicts about body-image perceptions in women. Personality and Individual Differences, 22(3), 309–316. https://doi.org/10.1016/S0191-8869(96)00210-3.
Davis, C., Dionne, M., & Shuster, B. (2001). Physical and psychological correlates of appearance orientation. Personality and Individual Differences, 30(1), 21–30. https://doi.org/10.1016/S0191-8869(00)00006-4.
Davis, C., Karvinen, K., & McCreary, D. R. (2005). Personality correlates of a drive for muscularity in young men. Personality and Individual Differences, 39(2), 349–359. https://doi.org/10.1016/j.paid.2005.01.013.
Deloitte Access Economics. (2012). Paying the price: The economic and social impact of eating disorders in Australia. Sydney: Butterfly Foundation. Retrieved from https://thebutterflyfoundation.org.au.
Dickinson, K. A., & Pincus, A. L. (2003). Interpersonal analysis of grandiose and vulnerable narcissism. Journal of Personality Disorders, 17(3), 188–207. https://doi.org/10.1521/pedi.17.3.188.22146.
Eysenck, H. J. (1950). Dimensions of personality (Vol. 5). London: Transaction Publishers.
Fairburn, C. G. (2009). Cognitive behavior therapy and eating disorders. New York: Guildford Press.
Field, A. (2013). Discovering statistics using SPSS (4th ed.). London: Sage Publications.
Fitzsimmons-Craft, E. E. (2011). Social psychological theories of disordered eating in college women: Review and integration. Clinical Psychology Review, 31(7), 1224–1237. https://doi.org/10.1016/j.cpr.2011.07.011.
Fitzsimmons-Craft, E. E., Harney, M. B., Koehler, L. G., Danzi, L. E., Riddell, M. K., & Bardone-Cone, A. M. (2012). Explaining the relation between thin ideal internalization and body dissatisfaction among college women: The roles of social comparison and body surveillance. Body Image, 9(1), 43–49. https://doi.org/10.1016/j.bodyim.2011.09.002.
Fox, J., & Rooney, M. C. (2015). The dark triad and trait self-objectification as predictors of men’s use and self-presentation behaviors on social networking sites. Personality and Individual Differences, 76, 161–165. https://doi.org/10.1016/j.paid.2014.12.017.
Fredrickson, B. L., & Roberts, T.-A. (1997). Objectification theory. Psychology of Women Quarterly, 21(2), 173–206. https://doi.org/10.1111/j.1471-6402.1997.tb00108.x.
Gentile, B., Miller, J. D., Hoffman, B. J., Reidy, D. E., Zeichner, A., & Campbell, W. K. (2013). A test of two brief measures of grandiose narcissism: The narcissistic personality inventory–13 and the narcissistic personality inventory–16. Psychological Assessment, 25(4), 1120–1136. https://doi.org/10.1037/a0033192.
Gordon, K. H., & Dombeck, J. J. (2010). The associations between two facets of narcissism and eating disorder symptoms. Eating Behavior, 11(4), 288–292. https://doi.org/10.1016/j.eatbeh.2010.08.004.
Graff, K. A., Murnen, S. K., & Krause, A. K. (2013). Low-cut shirts and high-heeled shoes: Increased sexualization across time in magazine depictions of girls. Sex Roles, 69(11), 571–582. https://doi.org/10.1007/s11199-013-0321-0.
Grijalva, E., Newman, D. A., Tay, L., Donnellan, M. B., Harms, P. D., Robins, R. W., … Yan, T. (2015). Gender differences in narcissism: A meta-analytic review. Psychological Bulletin, 141(2), 261–310. https://doi.org/10.1037/a0038231.
Grippo, K. P., & Hill, M. S. (2008). Self-objectification, habitual body monitoring, and body dissatisfaction in older European American women: Exploring age and feminism as moderators. Body Image, 5(2), 173–182. https://doi.org/10.1016/j.bodyim.2007.11.003.
Hatton, E., & Trautner, M. N. (2011). Equal opportunity objectification? The sexualization of men and women on the cover of rolling stone. Sexuality & Culture, 15(3), 256–278. https://doi.org/10.1007/s12119-011-9093-2.
Hayes, A. F. (2012). PROCESS: A versatile computational tool for observed variable mediation, moderation, and conditional process modeling. University of Kansas, KS. Retrieved from http://www.afhayes.com/public/process2012.pdf.
Hendin, H. M., & Cheek, J. M. (1997). Assessing hypersensitive narcissism: A reexamination of Murray's Narcism scale. Journal of Research in Personality, 31(4), 588–599. https://doi.org/10.1006/jrpe.1997.2204.
Hill, M. S., & Fischer, A. R. (2008). Examining objectification theory: Lesbian and heterosexual women's experiences with sexual-and self-objectification. The Counseling Psychologist, 36(5), 745–776. https://doi.org/10.1177/0011000007301669.
Jackson, L. A., Ervin, K. S., & Hodge, C. N. (1992). Narcissism and body image. Journal of Research in Personality, 26(4), 357–370. https://doi.org/10.1016/0092-6566(92)90065-C.
Jones, B. A., & Griffiths, K. M. (2015). Self-objectification and depression: An integrative systematic review. Journal of Affective Disorders, 171, 22–32. https://doi.org/10.1016/j.jad.2014.09.011.
Kline, R. B. (2015). Principles and practice of structural equation modelling (4th ed.). New York: Guilford.
Lipowska, M., & Lipowski, M. (2015). Narcissism as a moderator of satisfaction with body image in young women with extreme underweight and obesity. PLoS One, 10(5). https://doi.org/10.1371/journal.pone.0126724.
Maples, J. L., Lamkin, J., & Miller, J. D. (2014). A test of two brief measures of the dark triad: The dirty dozen and short dark triad. Psychological Assessment, 26(1), 326–331. https://doi.org/10.1037/a0035084.
McKinley, N. M. (1998). Gender differences in undergraduates' body esteem: The mediating effect of objectified body consciousness and actual/ideal weight discrepancy. Sex Roles, 39(1), 113–123. https://doi.org/10.1023/A:1018834001203.
McKinley, N. M., & Hyde, J. S. (1996). The objectified body consciousness scale: Development and validation. Psychology of Women Quarterly, 20(2), 181–215. https://doi.org/10.1111/j.1471-6402.1996.tb00467.x.
Moradi, B., & Huang, Y. P. (2008). Objectification theory and psychology of women: A decade of advances and future directions. Psychology of Women Quarterly, 32(4), 377–398. https://doi.org/10.1111/j.1471-6402.2008.00452.x.
Muehlenkamp, J. J., & Saris–Baglama, R. N. (2002). Self–objectification and its psychological outcomes for college women. Psychology of Women Quarterly, 26(4), 371–379. https://doi.org/10.1111/1471-6402.t01-1-00076.
Noll, S. M., & Fredrickson, B. L. (1998). A mediational model linking self-objectification, body shame, and disordered eating. Psychology of Women Quarterly, 22(4), 623–636. https://doi.org/10.1111/j.1471-6402.1998.tb00181.x.
Raskin, R., & Terry, H. (1988). A principal-components analysis of the narcissistic personality inventory and further evidence of its construct validity. Journal of Personality and Social Psychology, 54(5), 890–902. Retrieved from http://psycnet.apa.org/record/1988-25254-001.
Sedikides, C., Rudich, E. A., Gregg, A. P., Kumashiro, M., & Rusbult, C. (2004). Are normal narcissists psychologically healthy?: Self-esteem matters. Journal of Personality and Social Psychology, 87(3), 400–416. https://doi.org/10.1037/0022-3514.87.3.400.
Swami, V., Salem, N., Furnham, A., & Tovée, M. J. (2008). Initial examination of the validity and reliability of the female photographic figure rating scale for body image assessment. Personality and Individual Differences, 44(8), 1752–1761. https://doi.org/10.1016/j.paid.2008.02.002.
Swami, V., Cass, L., Waseem, M., & Furham, A. (2015). What is the relationship between facets of narcissism and women's body image? Personality and Individual Differences, 87, 185–189. https://doi.org/10.1016/j.paid.2015.08.006.
Tiggemann, M., & Lynch, J. E. (2001). Body image across the life span in adult women: The role of self-objectification. Developmental Psychology, 37(2), 243–253. https://doi.org/10.1037/0012-1649.37.2.243.
Twenge, J. M., & Campbell, W. K. (2008). Increases in positive self-views among high school students: Birth-cohort changes in anticipated performance, self-satisfaction, self-liking, and self-competence. Psychological Science, 19, 1082–1086. https://doi.org/10.1111/j.1467-9280.2008.02204.x.
Twenge, J. M., & Foster, J. D. (2010). Birth cohort increases in narcissistic personality traits among American college students, 1982-2009. Social Psychological and Personality Science, 1, 99–106. https://doi.org/10.1177/1948550609355719.
Twenge, J. M., Konrath, S., Foster, J. D., Campbell, W. K., & Bushman, B. J. (2008). Egos inflating over time: A cross-temporal meta-analysis of the narcissistic personality inventory. Journal of Personality, 76, 875–902. https://doi.org/10.1111/j.1467-6494.2008.00507.x.
Tylka, T. L. (2004). The relation between body dissatisfaction and eating disorder symptomatology: An analysis of moderating variables. Journal of Counseling Psychology, 51(2), 178–191. https://doi.org/10.1037/0022-0167.51.2.178.
Tylka, T. L., & Hill, M. S. (2004). Objectification theory as it relates to disordered eating among college women. Sex Roles, 51, 719–730. https://doi.org/10.1007/s11199-004-0721-2.
Watson, P. J., Morris, R. J., & Miller, L. (1998). Narcissism and the self as continuum: Correlations with assertiveness and hypercompetitiveness. Imagination, Cognition and Personality, 17(3), 249–259. https://doi.org/10.2190/29jh-9gdf-hc4a-02we.
Wink, P. (1991). Two faces of narcissism. Journal of Personality and Social Psychology, 61(4), 590–597. https://doi.org/10.1037//0022-3514.61.4.590.
Zeigler-Hill, V., Clark, C. B., & Pickard, J. D. (2008). Narcissistic subtypes and contingent self-esteem: Do all narcissists base their self-esteem on the same domains? Journal of Personality, 76(4), 753–774. https://doi.org/10.1111/j.1467-6494.2008.00503.x.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
The protocol for this study was reviewed by the human research ethics committee at Australian Catholic University: 2016-264E.
Rights and permissions
About this article

Cite this article
Carrotte, E., Anderson, J. Risk Factor or Protective Feature? The Roles of Grandiose and Hypersensitive Narcissism in Explaining the Relationship between Self-Objectification and Body Image Concerns. Sex Roles 80, 458–468 (2019). https://doi.org/10.1007/s11199-018-0948-y
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11199-018-0948-y