
Abstract
Adolescents with intellectual disabilities (ID) represent an invisible at-risk population for multiple negative health outcomes. Much like their non-disabled peers, promoting healthy behaviors during adolescence has the potential to improve quality of life later on in life (McPherson et al. in J Appl Res Intellect Disabil 30(2):360, 2017). Many studies have analyzed disparities in obesity (Phillips et al. in Matern Child Health J 18(8):1964, 2014; Stancliffe et al. in Am J Intellect Dev Disabil 116(6):401, 2011), mental health (Charlot and Beasley in J Ment Health Res Intellect Disabil 6(2):74, 2013), and health care access (Baller and Barry in J Disabil Policy Stud 27(3):148, 2016), however sexual health needs further research and translation to practice. Access to sexual health education is limited for many youth with ID (Barnard-Brak et al. in Ment Retard 52(2):85–97, 2014). Studies have shown that students with ID experience higher rates of sexual abuse and assault than their non-disabled peers (Haydon et al. in J Interpers Violence 26(17):3476, 2011; Mahoney and Poling in J Dev Phys Disabil 23(4):369, 2011). Sexually active youth with ID are at a higher risk for contracting sexually transmitted infections compared to their non-disabled peers (Cheng and Udry in J Dev Phys Disabil 17(2):155–172, 2005; Mandell et al. in J School Health 78(7):382–388, 2008). Additional barriers exist including stigma and misperceptions around disability and sexuality and the assumption that the developmental status of the student will prevent sex education comprehension (Sinclair et al. in Educ Train Autism Dev Disabil 50(1):3–16, 2015). Qualitative studies of adult providers (Linton et al. in Sex Disabil 34(2):145–156, 2016; Murphy et al. in J Genet Couns 25(3):552, 2016), parents (Kok and Akyuz in Sex Disabil 33(2):157–174, 2015), and adolescents with ID (Löfgren-Mårtenson in Sex Disabil 30(2):209–225, 2012) have found overwhelming support for tailored sexual risk reduction interventions (Swango-Wilson in Sex Disabil 27(4):223, 2009). Developing evidence-based, inclusive curricula to prevent sexual coercion as well as promote sexual health self-determination for this vulnerable population is long overdue (McDaniels and Fleming in Sex Disabil 34(2):215, 2016). This study demonstrates the use of Universal Design for Learning (UDL), an educational framework, guidelines, and checklist tools (Eagleton, Universal Design for Learning (UDL), Salem Press, Ipswich, 2015; Center for Applied Special Technology, UDL curriculum self-check 2011 (updated 2011), 2011. http://udlselfcheck.cast.org/resources.php) to increase accessibility in HIPTeens, an evidence-based sexual risk reduction intervention (Morrison-Beedy et al. in J Assoc Nurses AIDS Care 13(1):21–27, 2002; Res Nurs Health 28(1):3–15, 2005; AIDS Behav 10(5):541, 2006; J Assoc Nurses AIDS Care 21(2):153–161, 2010; West J Nurs Res 33(5):690–711, 2011; J Adolesc Health 52(3):314–321, 2013; J Assoc Nurses AIDS Care 28(6):877–887, 2017). As a result, supplemental curriculum components were developed with UDLguided technology use recommendations. A UDL-integrated evidence-based sexual risk reduction intervention could increase accessibility and, with additional research, could help inform inclusive policy.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Over the past century, the classroom and community have become more inclusive for adolescents and adults with disabilities (both physical and intellectual) since the passage of the Individuals with Disabilities Education and Americans with Disabilities Acts. These landmark pieces of legislation sought to create a culture and society where individuals with disabilities had expanded access and opportunities to pursue their dreams and a better quality of life. Despite progress made in policy, individuals with disabilities still suffer disproportionately from negative health outcomes and stigma [1]. Individuals with intellectual disabilities (ID) have significantly different health and social needs compared to their physically disabled counterparts due to developmental differences impacting behavior, communication, and independence [2].
Adolescents with ID represent an underrecognized at-risk population for multiple negative health outcomes. Much like their non-disabled peers, promoting healthy behaviors during this period of adolescence has the potential to improve quality of life later on in life and reduce the common morbidities of adolescence [3]. Many studies have analyzed disparities in obesity [4, 5], mental health [6], health care access [7] but many other topics need further exploration, research, and evidence-based practices including sexual health in this population [8].
The U.S. has made significant strides in reducing unplanned pregnancy among teens in the past decade. However, there are still some populations that are affected disproportionately by unplanned pregnancy, including adolescent minorities and special needs groups [9]. Access to sexual health education is limited for many youth with ID; students with moderate to profound ID were significantly less likely to receive sex education [10]. Adolescents with ID experience higher rates of sexual coercion [11] and sexual abuse and assault [12] than their non-disabled peers. Youth with intellectual disabilities are at a higher risk for contracting sexually transmitted infections compared to their non-disabled peers [13, 14]. A number of other barriers exist for adolescents with ID including stigma and misperceptions around disability and sexuality and the assumption that the developmental status of the student will prevent students from learning valuable skills and concepts related to sexual health education [15]. The overwhelming majority of qualitative studies of adult providers for adolescents with ID [16, 17], parents of adolescents with ID [18], and adolescents with ID [19] have found support from various stakeholders for population-specific sexual risk reduction interventions [20]. Developing evidence-based, inclusive curriculum to prevent sexual coercion [21] as well as promote sexual health self-determination for this vulnerable population is long overdue [8, 22]. Currently, the only comprehensive sex education curriculum for special education classrooms identified is Family Life and Sexual Health (FLASH). FLASH is being tested in a longitudinal, randomized, behavioral evaluation in King County, Washington by a national evaluation firm and the U.S. Department of Health and Human Services [23]. Preliminary results of the evaluation have not been released yet.
Addressing Accessibility with Universal Design for Learning
Universal design for learning (UDL) is a cognitive framework that focuses on removing barriers within learning environments by modifying curriculum, concepts, materials, and environments for all learners and abilities through the use of technology and creative options [24, 25]. This framework has roots in architecture and neuroscience and its use is encouraged by multiple national disability policy initiatives like the IDEA act [24, 25]. UDL focuses on the integration of curriculum for the learner rather than forcing the learner to adapt to the curriculum. This type of curricula considers different learning abilities, skills, needs, and the technological modifications that can meet all learning styles and needs. The UDL framework consists of three learning principles developed from neuroscience research: the recognition network of learning, the strategic network of learning, and the affective network of learning [24, 25]. Each network represents different aspects of learning; “what” (“what is it?”), “how” (“how do I do it?”), and “why” (“why should I do it?”) respectively [24, 25]. The Recognition Networks in the brain are responsible for how information is analyzed by our senses, therefore, providing multiple means of representation is important to help learners with different abilities [24, 25]. Strategic Networks control how the brain plans and performs different tasks, organizes ideas, expresses concepts, and devises solutions and strategies. To address different forms of comprehension demonstration, the UDL framework requires modifications for multiple methods of expression [24, 25]. Learners have multiple motivations and interests to fuel engagement; the UDL framework provides different ways to engage different learners in the Affected Networks of the brain [24, 25]. The UDL curriculum is comprised of four components, goals, methods, materials, and objectives, informed by the three principles [24, 25]. These components work together to foster the development of expert learners to become: (a) strategic, skillful, and goal-oriented; (b) knowledgeable, and (c) purposeful and motivated to learn more [24, 25]. The American Association on Intellectual and Developmental Disabilities (AAIDD) has recognized the need for further research on the efficacy and use of UDL as a framework for more inclusive and accessible curriculum modifications in K-12 education [26]. The National Center on Universal Design for Learning (NCUDL) has developed comprehensive guidelines and tools for UDL curriculum development and integration as well as an online curriculum checklist to ensure that each component of the cognitive networks and UDL curriculum is addressed [27]. This project used these guidelines and checklist tools to integrate the UDL framework into the HIPTeens intervention curriculum and facilitator manual by developing supplemental UDL curriculum components. This article illustrates the process as an example for other evidence-based intervention seeking to make their curriculum and practice more inclusive and accessible.
Methods
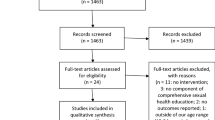
The first stage of this project was conducting a curriculum assessment of HIPTeens using the UDL Curriculum Self-Check online web application [27]. HIPTeens was identified as the evidence-based intervention for UDL integration because it is brief, has different activities that could be modified for different learning styles, and each session focuses on skill-building, role playing, and risk assessment which can be applicable to the ID adolescent population [28,29,30,31,32,33,34,35,36,37]. This evidence-based intervention was recognized by the Department of Health and Human Services Office of Adolescent Health for its multiple positive behavioral outcomes in reducing teen pregnancy [38] as well as the Centers for Disease Control for its behavioral outcomes impacting the HIV prevention [39]. The HIPTeens curriculum consists of four 90-min sessions and two 120-min booster sessions with visual presentations of various sexual health, communication, and risk behavior reduction information, condom demonstrations, kinesthetic activities related to risk behavior assessment (general and self), communication and partner negotiation role playing, and written activities using a custom workbook [28,29,30,31,32,33,34,35,36,37]. This assessment provided checkpoints for each UDL principle and curriculum component to inventory what the curriculum offers students of different learning styles as well as what approaches could be expanded to meet the needs of adolescents with ID. The Self-Check online application [27] allows users to add “lessons” to assess the goals, methods, materials, and assessments integrated with nine UDL principle checkpoints with expanded information available online (see Table 1).
Once the HIPTeens curriculum assessment was completed (components inventory and needs identified), the researcher used the UDL Curriculum Adaptation Guidelines Overview to help guide the development of supplemental curriculum materials and methods to provide learning options for all learners [24]. The Center for Applied Special Technology or CAST (who founded and manages the NCUDL) provides research-based online tools for educators and other teaching professionals to develop and share UDL lessons and tools as well as learn about new practices and technology in UDL. For example, the UDL Exchange allows educators to build UDL lessons using guided prompts that address each UDL curriculum component and principle [40]. Once the goals or learning objectives for each session were determined, the researcher then identified the methods, materials, and approaches needed to facilitate learning and uptake.
Results
Established Components
Assessing the current HIPTeens curriculum and materials using the UDL Curriculum Self-Check provided by [27] helped identify established UDL components. One of the promising and insightful results of the curriculum self-check was the significant amount of established UDL components embedded into the HIPTeens curriculum. This discovery could help support the various positive behavioral outcomes of the original randomized controlled trial that tested the efficacy of HIPTeens [29, 31, 37]. HIPTeens curriculum and activities included many concepts and components from each UDL Principle (See Table 2), most notable in means of action and expression (See Table 3) as well as Means of Engagement (See Table 4) [24]. HIPTeens intervention activities provide various ways for learners to interact with the learning environment and express the knowledge they have acquired in the session. Activities included opportunities for physical movement by using role-playing and physical interaction with curriculum materials [25]. There are various modes for expression and communication, including written composition, multimedia interaction, and verbal discussion and experience sharing [25]. Throughout each session, activities provide scaffolding to help participants set goals for healthy behavior change and assess various challenges and smaller, sequential steps in reaching short and long term goals [25]. Facilitators and associated activity materials provide models for goal setting and task completion to help participants achieve success [25]. The HIPTeens curriculum also provides embedded prompts for facilitators to elicit feedback from participants about their progress, questions about concepts or information, and difficulties related to personal behavior change [25]. Because HIPTeens is a theoretically-driven intervention based on the information-motivation-behavioral-skills model of HIV prevention [41, 42], there are various means of engagement established throughout the curriculum to increase and sustain motivation [25]. The curriculum is participant-centered, drawing on participant experience, attitudes, and motivations to sustain engagement throughout the sessions and boosters. Autonomy and choice are featured in multiple activities that focus on individual goal-setting, behavioral assessment, and levels of motivation to change [25]. HIPTeens was developed using target audience input [28], therefore, culturally and linguistically relevant information and language are used throughout the curriculum [25]. However, as additional audiences are considered for implementation, further research will be needed to ensure audience cultural, linguistic, and social relevance. Incorporating these components for adolescents with ID could be done using a similar formative approach employed by the developer of HIPTeens [28].
Integration Results
A couple of curricular gaps were found during the UDL assessment including a lack of graphic and visual information, visual and informational aids for students with sensory difficulties, and limited options for information organization, retention, and comprehension. To address the UDL gap areas identified in the curriculum assessment, a supplemental package of educational materials was created for the HIPTeens curriculum. These supplements were developed using UDL-guided principles addressing various types of learners and barriers to comprehension. HIPTeens uses PowerPoint slide sets to display information, concepts, and prompt discussion in the facilitated groups. Additional graphics, icons, visual organizers, and multimedia were added to the slides to help facilitate comprehension for those needing alternative visual and informational organization options and preferences to address the gaps found in Multiple Means of Representation [25]. For example, videos explaining complex concepts like HIV transmission and consent were provided as options for students needing visual cues and multimedia to enhance comprehension. Handouts with templates and graphic and information organizers were created for activities in each session and booster session were created to help students who may need additional support organizing and retaining important information from each activity and concept. These organizers are available online and in print for participants. Displays and PowerPoint slides for group goals were created to provide options for executive function, outline group expectations, and manage group and individual progress. Custom videos were included in HIPTeens using young adults who act out different, real world risk scenarios for participants to evaluate and apply concepts like assertive statements, negotiating safer sex practices and condom use, and identifying trigger behaviors that lead to negative sexual-decision making and outcomes. However, these videos did not include captions for students with auditory impairments, therefore, captions were added using Adobe Premiere Pro. Online activities that mirrored the group activities were a critical component of providing additional alignment with all three UDL Principles. After searching for a comprehensive online learning management platform that could host multiple, custom activities, it became apparent that developing an online learning platform that could provide additional support for basic vocabulary and glossary terms with definitions for unfamiliar terms throughout each session as well as alternative text for visual objects, screen reader, automatic voicing and speech-to-text capabilities, and opportunities to clarify vocabulary and symbols would be needed [25]. Assistive technology and tools, online construction and composition tools and media, and alternative tools for information gathering are also innovative integrations for potential use in an online environment and recommended for future development and implementation. The following table illustrates the UDL guidelines and how the deliverable package addressed each guideline (See Table 5).
Lessons Learned
The singular task of applying UDL to a developed evidence-based curriculum for people living with intellectual disabilities was no small feat. Understanding the needs of those with intellectual disabilities requires the collaboration and expertise of professionals in the special education, psychology, instructional design, and technology fields. To further complicate this endeavor, meeting the broad needs of those with diverse array of intellectual disabilities is difficult (e.g. autism, Downs Syndrome). The need for interdisciplinary collaboration from aforementioned fields is crucial for further intervention tailoring, pilot-testing, and eventual, wider dissemination. This doctoral project provided the foundational work for future collaborative work, intervention testing, and community implementation and dissemination. Fortunately, there has been momentum for tailored sex education curricula for people (adults and adolescents) with intellectual disabilities, making collaboration and interdisciplinary work more likely [8, 43, 44].
Future Recommendations and Discussion
Because UDL is widely used in the education field and promotes the use of technology [25], there are easy-to-use, comprehensive online tools for educators to use for self-checking curriculum [27], developing curriculum, and sharing UDL-guided curriculum with others [40]. To assess the HIPTeens curriculum, the CAST UDL Curriculum Self-Check online tool was used and provided guided questions to assess if the curriculum included specific UDL curriculum components, examples of curriculum elements, and space for note-taking [27]. This tool was extremely useful for those with limited background and knowledge of UDL. Using this online tool, a complete assessment of the HIPTeens curriculum was generated, identifying established components and elements, gap areas, explore examples when needed, and take detailed notes for curriculum development and considerations. Wider marketing of these tools to professionals outside of the education field should be considered, specifically to those developing and disseminating evidence-based interventions with educational components.
The assessment of HIPTeens using UDL principles and guidelines also helped generate ideas for future technology use in the intervention as well as pilot-testing. Using the limited scope of design skills and resources, the development of supplemental educational components for HIPTeens provides a first step in wider development of technology and web-based educational activities and assistive tools for participants needing various learning alternatives and sensory support. As the curriculum was assessed, it became clear that a comprehensive online component was needed to address those needing additional information context (ex. Glossary of terms, multimedia examples), text to speech or screen readers, additional practice and repetition opportunities, and a space to learn about safely exploring the internet and social media and how to determine the informational credibility of websites. Development of this online learning platform would require activity customization to safeguard HIPTeens intervention fidelity as well as integration of the Web Content Accessibility Guidelines (WCAG) in web application development and maintenance [45].
The next step toward practical application of this project would be planning for a pilot study to test the HIPTeens curriculum, supplemental materials, and gather feedback from participants and facilitators about implementation and learning barriers for further intervention tailoring. This would include identification of potential sites with access to adolescents with ID. The scope and need of this intervention and population require an interdisciplinary approach, meaning that the content area experts and stakeholders are necessary for further deficit identification due to their unique experiences and knowledge. Interest in this curriculum and its supplements has increased as awareness of the needs of those with ID and spotlight on sexual assault among vulnerable populations has increased [43, 44]. Local and state sites in public schools and transition education programs at vocational and college campuses have been identified as potential pilot studies and should be further explored for partnerships. With pilot testing, the development of an online learning platform is recommended for testing and refinement based on feedback from the focus population, stakeholders, and content area experts. In addition, basic background information regarding reproductive organs, biologic processes, and sexual health and hygiene are recommended as topics to be appended to the current curriculum. Adolescents and young people with ID are less likely to receive any sex education than their non-disabled peers [10] and therefore may lack basic knowledge of reproductive processes and anatomy [8]. This knowledge is critical to scaffolding learning activities focused on sexual risk, behaviors, and ultimately supporting healthy behavior change and choices.
References
Krahn, G.L., Walker, D.K., Correa-De-Araujo, R.: Persons with disabilities as an unrecognized health disparity population. Am. J. Public Health 105(Suppl 2), S198–S206 (2015)
Krahn, G.L., Fox, M.H.: Health disparities of adults with intellectual disabilities: what do we know? What do we do? J. Appl. Res. Intellect. Disabil. JARID 27(5), 431–446 (2014)
McPherson, L., Ware, R.S., Carrington, S., Lennox, N.: Enhancing self-determination in health: results of an RCT of the Ask Project, a school-based intervention for adolescents with intellectual disability. J. Appl. Res. Intellect. Disabil. 30(2), 360 (2017)
Phillips, K., Schieve, L., Visser, S., Boulet, S., Sharma, A., Kogan, M., et al.: Prevalence and impact of unhealthy weight in a national sample of US adolescents with autism and other learning and behavioral disabilities. Matern. Child Health J. 18(8), 1964 (2014)
Stancliffe, R.J., Lakin, K.C., Larson, S., Engler, J., Bershadsky, J., Taub, S., et al.: Overweight and obesity among adults with intellectual disabilities who use intellectual disability/developmental disability services in 20 U.S. States. Am. J. Intellect. Dev. Disabil. 116(6), 401 (2011)
Charlot, L., Beasley, J.B.: Intellectual disabilities and mental health: United States-based research. J. Ment. Health Res. Intellect. Disabil. 6(2), 74 (2013)
Baller, J.B., Barry, C.L.: State variation in school-based disability services financed by medicaid. J. Disabil. Policy Stud. 27(3), 148 (2016)
Schwartz, R.J., Robertson, R.E.: A review of research on sexual education for adults with intellectual disabilities. Career Dev. Transit. Except. Individ. (2018). https://doi.org/10.1177/2165143418756609
Decker, M.J., Berglas, N.F., Brindis, C.D.: A call to action: developing and strengthening new strategies to promote adolescent sexual health. Societies 5(4), 686 (2015)
Barnard-Brak, L., Schmidt, M., Chesnut, S., Tianlan, W., Richman, D.: Predictors of access to sex education for children with intellectual disabilities in public schools. Intellect. Dev. Disabil. 52(2), 85–97 (2014)
Haydon, A.A., McRee, A.-L., Tucker, H.C.: Unwanted sex among young adults in the United States: the role of physical disability and cognitive performance. J. Interpers. Violence 26(17), 3476 (2011)
Mahoney, A., Poling, A.: Sexual abuse prevention for people with severe developmental disabilities. J. Dev. Phys. Disabil. 23(4), 369 (2011)
Mandell, D., Eleey, C., Cederbaum, J., Hutchinson, M., Jemmott, L.S., Blank, M.: Sexually transmitted infection among adolescents receiving special education services. J. Sch. Health 78(7), 382–388 (2008)
Cheng, M.M., Udry, J.R.: Sexual experiences of adolescents with low cognitive abilities in the U.S. J. Dev. Phys. Disabil. 17(2), 155–172 (2005)
Sinclair, J., Unruh, D., Lindstrom, L., Scanlon, D.: Barriers to sexuality for individuals with intellectual and developmental disabilities: a literature review. Educ. Train. Autism Dev. Disabil. 50(1), 3–16 (2015)
Linton, K.F., Rueda, H.A., Williams, L.R., Sandoval, A., Bolin, S.: Reproductive and sexual healthcare needs among adults with disabilities as perceived by social workers. Sex. Disabil. 34(2), 145–156 (2016)
Murphy, C., Lincoln, S., Meredith, S., Cross, E.M., Rintell, D.: Sex education and intellectual disability: practices and insight from pediatric genetic counselors. J. Genet. Couns. 25(3), 552 (2016)
Kok, G., Akyuz, A.: Evaluation of effectiveness of parent health education about the sexual developments of adolescents with intellectual disabilities. Sex. Disabil. 33(2), 157–174 (2015)
Löfgren-Mårtenson, L.: “I want to do it right!” A pilot study of swedish sex education and young people with intellectual disabilities. Sex. Disabil. 30(2), 209–225 (2012)
Swango-Wilson, A.: Perception of sex education for individuals with developmental and cognitive disability: a four cohort study. Sex. Disabil. 27(4), 223 (2009)
Martinello, E.: Reviewing strategies for risk reduction for sexual abuse of children with intellectual disabilities: a focus on early intervention. Sex Disabil. 32, 167–174 (2014)
McDaniels, B., Fleming, A.: Sexuality education and intellectual disability: time to address the challenge. Sex. Disabil. 34(2), 215 (2016)
Winges-Yanez, N.: Discourse analysis of curriculum on sexuality education: FLASH for special education. Sex. Disabil. 32(4), 485–498 (2014)
Eagleton, M.: Universal Design for Learning (UDL). Salem Press, Ipswich (2015)
Meyer, A., Rose, D., Gordon, D.: Universal Design for Learning: Theory and Practice. CAST Professional Publishing, Wakefield, MA (2014)
Smith, S.J., Lowrey, K.A.: Applying the universal design for learning framework for individuals with intellectual disability: the future must be now. Intellect. Dev. Disabil. 55(1), 48 (2017)
Center for Applied Special Technology: UDL curriculum self-check 2011 (updated 2011). http://udlselfcheck.cast.org/resources.php. Accessed 22 Jan 2018
Morrison-Beedy, D., Carey, M.P., Aronowitz, T., Mkandawire, L., Dyne, J.: Adolescents’ input on the development of an HIV risk reduction intervention. J. Assoc. Nurses AIDS Care 13(1), 21–27 (2002)
Morrison-Beedy, D., Carey, M.P., Crean, H.F., Jones, S.H.: Risk behaviors among adolescent girls in an HIV prevention trial. West. J. Nurs. Res. 33(5), 690–711 (2011)
Morrison-Beedy, D., Carey, M.P., Crean, H.F., Jones, S.H.: Determinants of adolescent female attendance at an HIV risk reduction program. J. Assoc. Nurses AIDS Care 21(2), 153–161 (2010)
Morrison-Beedy, D., Carey, M.P., Kowalski, J., Tu, X.: Group-based HIV risk reduction intervention for adolescent girls: evidence of feasibility and efficacy. Res. Nurs. Health 28(1), 3–15 (2005)
Morrison-Beedy, D., Carey, M.P., Tu, X.: Accuracy of audio computer-assisted self-interviewing (ACASI) and self-administered questionnaires for the assessment of sexual behavior. AIDS Behav. 10(5), 541 (2006)
Morrison-Beedy, D., Grove, L., Ji, M., Baker, E.: Understanding the “why” for high-risk behavior: adolescent girls’ motivations for sex. J. Assoc. Nurses AIDS Care 28(6), 877–887 (2017)
Morrison-Beedy, D., Jones, S.H., Xia, Y., Tu, X., Crean, H.F., Carey, M.P.: Reducing sexual risk behavior in adolescent girls: results from a randomized controlled trial. J. Adolesc. Health 52(3), 314–321 (2013)
Morrison-Beedy, D., Carey, M.P., Côté-Arsenault, D., Seibold-Simpson, S., Robinson, K.A.: Understanding sexual abstinence in urban adolescent girls. J. Obstet. Gynecol. Neonatal. Nurs. 37(2), 185–195 (2008)
Morrison-Beedy, D., Nelson, L.E.: HIV prevention interventions in adolescent girls: what is the state of the science? Worldviews Evid Based Nurs. 1(3), 165–175 (2004)
Morrison-Beedy, D., Passmore, D., Carey, M.P.: Exit interviews from adolescent girls who participated in a sexual risk-reduction intervention: implications for community-based health education promotion for adolescents. J. Midwifery Women’s Health 58(3), 313–320 (2013)
U.S. Department of Health and Human Services Office of Adolescent Health: Teen pregnancy prevention evidence review: health improvement project for teens (hipteens)
Centers for Disease Control and Prevention: Compendium of evidence-based interventions and best practices for HIV prevention. http://www.cdc.gov/hiv/prevention/research/compendium/rr/hip.html. Accessed 22 Jan 2018
Center for Applied Special Technology: UDL Exchange 2012. http://udlexchange.cast.org/home. Accessed 22 Jan 2018
Fisher, J.D., Fisher, W.A.: Changing AIDS-risk behavior. Psychol. Bull. 111(3), 455–474 (1992)
Fisher, J.D., Fisher, W.A., Bryan, A.D., Misovich, S.J.: Information-motivation-behavioral skills model-based HIV risk behavior change intervention for inner-city high school youth. Health Psychol. 21(2), 177–186 (2002)
Shapiro, J.: The sexual assault epidemic no one talks about [Radio broacast episode and online article]. National Public Radio (2018). https://www.npr.org/2018/01/08/570224090/the-sexual-assault-epidemic-no-one-talks-about. Accessed 22 Jan 2018
Shapiro, J.: For some with intellectual disabilities, ending abuse starts with sex ed [Radio broadcast episode and web article]. National Public Radio (2018). https://www.npr.org/2018/01/09/572929725/for-some-with-intellectual-disabilities-ending-abuse-starts-with-sex-ed. Accessed 22 Jan 2018
W3C: Web Content Accessibility Guidelines (WCAG) 2.1 2018 (updated January 30, 2018). 2.1. https://www.w3.org/TR/WCAG21/
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have not conflict of interest and authors Morrison-Beedy, Kirby and Hess were member of Grove’s doctoral dissertation committee.
Ethical approval
This article does not contain any studies with human participants or animals performed by any of the authors.
Rights and permissions
About this article

Cite this article
Grove, L., Morrison-Beedy, D., Kirby, R. et al. The Birds, Bees, and Special Needs: Making Evidence-Based Sex Education Accessible for Adolescents with Intellectual Disabilities. Sex Disabil 36, 313–329 (2018). https://doi.org/10.1007/s11195-018-9547-7
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11195-018-9547-7