
Abstract
Purpose
Poor self-rated health (SRH) is linked to an increased risk of injury, future healthcare services utilization, and morbidity and mortality. This study aimed to identify correlates of a single-item measure of health in 8070 US Army personnel.
Methods
Responses were collected from the Army’s global assessment tool (GAT) 2.0, an online questionnaire that assesses physical and psychosocial health. SRH was measured by the item, “How do you consider your health?” (four response categories: “poor,” “fair,” “good,” and “excellent”). Ordinal logistic regression (OLR) was used to evaluate how various health and psychosocial factors contribute to Soldiers’ ratings of SRH. Unadjusted and adjusted cumulative odds ratios (ORs) are presented and discussed.
Results
Most participants reported “good” health (57%), followed by “excellent” (24%), “fair” (17%), and “poor” (2%). Sleep quality (OR 2.48; 95% CI 2.34, 2.63) was the largest correlate of SRH, followed by obesity (OR 0.50; 95% CI 0.43, 0.58), emotional fitness (OR 1.68, 95% CI 1.56, 1.82), and Army physical fitness test (APFT) scores (OR 1.43; 95% CI 1.36, 1.51).
Conclusions
Single-item measures of self-reported health can cover a broad spectrum across physical and mental health. Among a large US Army sample, sleep quality was most strongly associated with SRH, followed by emotional fitness and APFT scores. In contrast, service-component and other sociodemographic characteristics had relatively small effects on general health. Military investigators and leaders who must rely on various subjective general health measures should interpret them as a combination of these factors.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Service members face a unique combination of health risk factors when compared with their civilian counterparts: multiple and prolonged deployments, separation from family and support networks, adjustment to new physical and cultural environments, and irregular sleep–wake schedules [1–3]. Even the most resilient warfighters experience the toll these stressors can impose on their overall health and wellbeing. In order to measure an individual’s overall health, one approach is simply to ask him or her: “How do you consider your general health?” This type of question, often referred to as single-item self-rated health (SRH), is commonly used in population research [4–8]. The present study explored a variety of health behaviors and their associations with SRH in a large sample of Active Duty (AD) and Reserve/National Guard (RNG) army members.
Background
For a broad range of civilian populations, SRH has been shown to be an effective and economical way to assess total health [9–11]. Research has shown that SRH is predictive of future health services utilization, disability, morbidity and mortality, and injury risk [12–15]. Additionally, poor SRH is strongly associated with death due to specific causes (e.g., diabetes, infectious disease, and respiratory disease) [16, 17], risky health behaviors (e.g., alcohol misuse, smoking) [5, 6, 18], lack of social support [19], and a number of psychosocial risk and resilience factors [18, 20–23].
One view of SRH is that of a largely subjective self-assessment, where many individually relevant components are weighed internally and translated into a response. Thus, it is not an objective measure of health (like blood pressure or heart rate); rather, it is the result of a cognitive process combining the different physiological, psychological, and social factors an individual sees personally as “health-related” [24]. In this way, SRH may reflect spontaneous self-assessments of health as well as “enduring self-concepts” [25], both of which can be influenced by an individual’s expectations, peers, and environment.
One frequent theme of the research is of the multidimensional nature of SRH; an individual’s global health encompasses both physical and psychological dimensions. This is explicitly reflected in the National Institute of Health (NIH)-funded Patient-Reported Outcomes Measurement Information System (PROMIS) global health scale [26] and the center for disease control and prevention (CDC)’s Healthy Days scale [27]. Both of these measures have one SRH item, alongside other items measuring physical and mental health. A large body of empirical research supports relations between SRH and physical health symptoms [25, 28, 29], social support [25, 28, 29], cardiovascular disease [17], depression [5, 28, 30], and mood/vitality [29, 31]. SRH also moderately-to-weakly relates to various health behaviors: sleep [4, 32–34], alcohol use [5, 31, 35], smoking [25, 35, 36], exercise [31, 36, 37], and diet [37]. In sum, there is compelling support for the view that SRH reflects a range of physical, mental, and social factors, and furthermore these relations are relatively consistent across different age and gender groups [28].
Military research into SRH has been far less comprehensive, focusing mainly on relations between SRH and military-specific health factors, such as combat exposure, PTSD and brain trauma, poor sleep, and physical injury [2, 7, 15, 19, 38–40]. Poor SRH has also been found to predict high outpatient services upon return from deployment [41] and a higher risk of musculoskeletal injury in female Soldiers [42]. The high sensitivity but relative lack of specificity of SRH may be an advantage or a disadvantage, depending on how the measure is used. Although it may lack diagnostic precision in clinical contexts, SRH and similar measures of total health have been proposed as efficient population-monitoring tools [11, 24, 27, 28, 30]. Owing to a number of factors, there is growing interest in SRH, and in related constructs such as health-related quality of life, in military research.
Within the Department of Defense (DoD), initiatives frequently adopt an integrative approach to health, wellbeing, and readiness. One widespread tenet is that “humans are more important than hardware” [43]. The importance of this tenet is underscored by two longstanding trends: the job demands of modern warfare have increased and diversified; and non-communicable diseases are posing greater threats to health, both in general and military populations [44]. Initiatives such as Total Force Fitness (TFF) [45] and comprehensive soldier fitness [46, 47] adopt the philosophy that many distinct aspects contribute to human performance, including physical and mental health, spiritual wellbeing, family relations, and work-related demands. There is a clear need to understand how these various interrelated components affect overall health and performance.
The present analysis used data from the Global Assessment Tool (GAT), which began under the comprehensive soldier fitness program in October, 2009 [48, 49]. The GAT primarily consists of scales that measure psychosocial wellbeing (or “fitness”) in four core domains: emotional, social, spiritual, and family fitness. These domains have various subscales, as previously detailed by others [48]. The largest is the emotional domain, which is composed of six scales (adaptability, bad/good coping, catastrophizing, depression, optimism, positive/negative affect), followed by social (friendship, loneliness, engagement, and organizational trust), family (satisfaction and support), and spiritual (only one scale) support. In 2012, pilot items were added to the GAT to measure a fifth dimension of physical fitness. The new items covered nutrition behaviors, sleep quality, physical activity, and other indicators of general health, such as SRH (which has since been removed, and other items modified). The GAT is also completed annually by all Army personnel, which allows for the comparison of various subgroups, based on service-component (i.e., Active Duty, Reserve, National Guard) and demographic characteristics.
SRH, although a highly sensitive global measure, certainly has shown predictive value and validity for inferences into health. In the medical community, despite ongoing debate, many recognize that patient-reported outcomes play a fundamental role in clinical trials and disease monitoring [50]. A deeper understanding of factors that do and do not relate to SRH can better hone initiatives seeking to improve health. Since the GAT covers a breadth of areas of human performance, it affords a unique opportunity to understand how these factors relate to SRH. The present study builds off of previous military SRH research, while including a larger, more diverse sample size and a greater range of variables than previous studies. The goals of the present study were therefore to (1) examine group differences in SRH along demographic and military-specific variables, (2) explore relations between GAT scales/items and SRH, and (3) examine whether these relations differed by various groups.
Methods
The GAT 2.0 is an online survey taken annually by all US Army personnel. The survey assesses wellness and risk factors across five core components of fitness (physical, social, emotional, family, and spiritual), with the goal of promoting psychological resilience and overall wellbeing among warfighters and their families. GAT data are confidentially reported by Soldiers as part of an annual requirement in the US Army. Any data reported for research are derived from respondents who had directly consented to allowing their data for such use and then can only be assessed in aggregate form to ensure anonymity and confidentiality of responses.Footnote 1 The Uniformed Services University of the Health Sciences Institutional Review Board approved the analyses of these data from those that agreed for their responses to be used for research purposes.
The data used in our analyses were from Soldiers who took the GAT during a 2-week period in July 2012 as part of a pilot project assessing items on a newly added fifth (physical) domain. Scores were collected from 14,148 Soldiers across all three Army components (AD, Reserve and NG). The current study used an ordinal logistic regression (OLR) approach to analyze a subset of 8070 participants who completed all measures used. Participants were 86% male, 27.5 ± 8.1 years old on average, 51% married, 16% officer (vs. enlisted), 57% AD, 26% NG, and 17% Reserve Component (R). Respondents were not sampled at random; however, the larger sample includes all Soldiers who took the GAT over the 2-week period, and its demographic characteristics are comparable with those of the Army as a whole in 2012 [51].
Health and behavioral indicators
Psychosocial factors
The primary purpose of the GAT is to assess Soldiers’ fitness across four psychosocial dimensions: social, emotional, family, and spiritual. Pilot items for a fifth physical health dimension were added later. Measures on the GAT were developed by Seligman et al. [47] and others [48, 52, 53], and the details of its evaluation and reliability have been described previously in other available reports [48, 49, 54, 55]. As described by Lester et al. [56], each dimension is a combination of a number of different interrelated constructs. The dimensions comprise various smaller subscales, some of which were adapted from previously published work, and others which were created specifically for the GAT. The present study analyzed GAT responses primarily at the dimension level, as it is beyond the scope of this article to summarize each individual subscale.
Specifically, social fitness consists of four scales (work engagement, friendship, loneliness, organizational trust; sample item from organizational trust scale: “Overall, I trust my immediate supervisor”[57]); emotional fitness consists of eight scales (adaptability, bad/good coping, catastrophizing, depression, optimism, positive/negative affect; sample item from adaptability scale: “I can usually fit myself into any situation”[58]); family fitness consists of two scales (family satisfaction, military family support; sample item from family satisfaction scale: “How satisfied are you with your marriage/relationship?”); and spiritual fitness consists of one scale (search for meaning; sample item: “my life has lasting meaning”). Subsequent analyses suggest that GAT psychosocial scales predict a range of both positive (e.g., completion of Ranger training) and negative (e.g., Army reprimands) outcomes in military personnel [49, 56, 59]. The current study includes additional pilot questions to assess physical dimension items, which were added later.
Physical dimension
The items for the physical dimension of the GAT assessed nutritional habits and behaviors, physical activity patterns, sleep quality, and other lifestyle behaviors (alcohol and tobacco use). Self-reported army physical fitness test (APFT) scores were collected as a measure of overall physical fitness. The APFT comprise three sub-tests: a 2-mile run time, maximal sit-ups in 2 min, and maximal push-ups in 2 min. Participants entered their raw values for each test (run time, number of sit-ups, and number of push-ups). These data were then used to compute a total APFT score on a scale of 1–300 in accordance with Army guidelines [60]. Research suggests that self-reported APFT scores are accurate indicators of actual APFT score [61]. Body mass index (BMI) was calculated from participants’ self-reported height and weight measurements, and categorized as obese, overweight, or neither obese nor overweight [62].
Nutrition
The Healthy Eating Score (HES-5) was developed based on the US Department of Agriculture’s (USDA) healthy eating index (HEI) [63, 64]. The HES-5 consists of five survey questions assessing the frequency of fruit, vegetable, whole grain, dairy, and fish consumption. Responses to HES had adequate internal consistency (α = 0.76) and have been associated with other important health metrics such as BMI, physical fitness scores, and psychological health [64]. Scores range from 0 to 25, with higher scores indicating healthier eating (interpretive cutoffs have not yet been developed). In the present study, a third (33%) of participants reported getting at least two servings of fruits and two servings of vegetables per day, while slightly more than half (53%) reported at least two servings per day of either fruits or vegetables.
Alcohol and tobacco
Participants were asked if they had exceeded five alcoholic drinks on any single occasion during the past 3 months (yes or no), and if they currently had been smoking cigarettes or cigars for three or more months. Responses were dichotomized to determine binge drinkers (≥5 drinks on one occasion) versus non-binge drinkers, and smokers versus non-smokers.
Sleep
Sleep was assessed using the two-item Pittsburgh Insomnia Rating Scale (PIRS-2), a self-reported measure of perceived sleep quality. The PIRS-2 was created to be used as an efficient screening tool for risk of insomnia [65–67]. It results in a score ranging from 0 to 6, where higher scores indicate greater potential risk for insomnia. The PIRS-2 asks about (1) overall sleep satisfaction, and (2) how much a person was bothered by lack of energy due to perceived poor sleep in the past 7 days. Items are rated on a four-point Likert-type scale, with higher scores indicating poorer sleep habits. Approximately one-third (34%) of participants in the present study indicated that their sleep quality was excellent (i.e., scored 0 or 1 out of 6 on the PIRS-2), though nearly one in four (24%) reported potential sleep deficits (i.e., scored 4 or higher on the PIRS-2). For the present analysis, scores were reverse-coded so that higher scores indicate better quality sleep and lower scores indicate greater risk of insomnia. The PIRS-2 demonstrated adequate internal consistency in the present study (α = 0.80).
Outcome variable
The main outcome variable used was overall general health, which was measured by a single, self-reported item, “How do you consider your general health?” The item on SRH was answered on a four-point Likert-type scale (1 = poor, 2 = fair, 3 = good, 4 = excellent). An additional option for “don’t know” was offered; those who selected this option (<1%) were excluded from the present analysis.
Statistical analyses
An ordered logistic regression (OLR) model was built to examine the relation between the SRH outcome measure and other health risk and protective factors. Cumulative odds ratios (ORs) were obtained, where ORs greater than one indicate better SRH status (i.e., the odds of increasing by one level of the outcome for every one unit change in the covariate). Univariate analyses were also performed to obtain unadjusted ORs for each predictor. All ORs are reported with 95% confidence intervals (CIs). Available demographic characteristics controlled for were age, sex, marital status, military rank, and service component. Health and psychosocial variables were considered, based on known or suspected health risk or protective factors, for poor overall health identified from the literature.
GAT psychosocial scores (e.g., emotional, social, family, and spiritual fitness), sleep scores (PIRS-2), and APFT scores were converted to standardized z-values. This was done for ease of interpreting results of the regression model, particularly where dichotomization of scores seemed arbitrary. After viewing the results, a factor analysis on the emotional fitness dimension was performed to determine if specific components were disproportionately driving results of the OLR. All predictor variables were coded such that higher scores indicate healthier functioning in that area. Lastly, interactions between demographic variables (gender, marriage, officer versus enlisted, Army component, age group) and independent variables were examined. Because of the large number of potential interactions, p was set at 0.01. All analyses were conducted using IBM SPSS version 22.0.
Results
Tables 1 and 2 present descriptive statistics for the entire sample (n = 8,070), by self-rated health status, for demographic characteristics and behavioral information, respectively. Participants generally reported being in good or excellent health, with 24% indicating “excellent,” 57% indicating “good,” 17% indicating “fair,” and just 2% indicating “poor” to the SRH item. Unadjusted ORs of better SRH were examined across demographic groups (Table 3, univariate model). Overall, those rating their health as “excellent” were more frequently officers (unadjusted OR 1.79; 95% CI 1.59, 2.00), not married (unadjusted OR 1.34; 95% CI 1.23, 1.45), National Guardsmen (unadjusted OR 1.31; 95% CI 1.19, 1.45), and male (unadjusted OR 1.18; 95% CI 1.05, 1.34).
Participants with higher SRH also tended to report better quality sleep (unadjusted OR 3.37; 95% CI 3.19, 3.55) and physical fitness test (APFT) scores (unadjusted OR 1.58; 95% CI 1.51, 1.65). Binge drinkers (unadjusted OR 0.71; 95% CI 0.65, 0.79) and current smokers (unadjusted OR 0.61; 95% CI 0.55, 0.67) rated their health lower than non-drinkers and non-smokers, respectively. All four dimensions of psychosocial fitness were positively associated with SRH: emotional fitness had the largest association (unadjusted OR 2.79; 95% CI 2.65, 2.93), followed by social fitness (unadjusted OR 2.39; 95% CI 2.28, 2.51), spiritual fitness (unadjusted OR 1.86; 95% CI 1.77, 1.94), and family fitness (unadjusted OR 1.71; 95% CI 1.64, 1.79).
Model 1 in Table 3 presents adjusted ORs and 95% CIs from the full OLR. After adjusting for all other factors and covariates, sleep quality remained the strongest predictor of SRH (OR 2.48; 95% CI 2.34, 2.63), indicating that those who reported better sleep were approximately 2.5 times more likely to report better overall health as well. Emotional fitness (OR 1.68; 95% CI 1.56, 1.82) and BMI were the next strongest predictors. Participants in the “normal” BMI category were twice as likely as those in the “obese” category (OR 0.50; 95% CI 0.43, 0.58) to report better SRH. APFT scores (OR 1.43; 95% CI 1.36, 1.51) and Healthy Eating Scores (OR 1.27; 95% CI 1.21, 1.34) exhibited weaker, but still notable associations with SRH. Smokers (OR 0.84; 95% CI 0.76, 0.93) were only marginally less likely to report better SRH than non-smokers, while the relation between binge drinking and SRH was slightly positive but not significant (OR 1.08; 95% CI 0.96, 1.20).
Although each of the psychosocial dimensions was positively associated with SRH in univariate analyses (inter-correlations among the four GAT psychosocial dimensions ranged from 0.35 to 0.70), only emotional fitness retained any notable effect in the model after adjusting for the other predictors. When SRH was regressed only on the four GAT dimensions, emotional fitness was the only variable with any notable effect (OR 2.14; 95% CI 1.99, 2.30). Given that emotional fitness encompasses a number of smaller, but interrelated, subscales, factor analysis (using maximum likelihood extraction and varimax rotation) was performed on emotional fitness scale items to determine factors driving the specific results. This revealed two main factors: positive emotional traits (good coping, adaptability, positive affect, optimism), which accounted for 35% of the variance in the emotional domain, and negative emotional traits (negative affect, catastrophizing, and depression), which accounted for 19% of the variance in the emotional domain. (Note: higher scores on the GAT indicate healthy traits; therefore, higher scores on the negative emotional trait factor indicate a lack of negative emotional traits). Subsequently, in Model 2, these two factors were used instead of the four psychosocial GAT domain scores. This revealed scoring high on positive traits as the stronger predictor of better SRH (OR 1.72; 95% CI 1.63, 1.81), though low scoring on negative traits was also uniquely associated with the outcome (OR 1.49; 95% CI 1.40, 1.57).
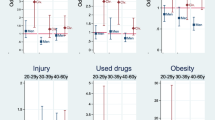
Interactions among demographic variables and other independent variables (from Model 2 in Table 3) were examined. The only statistically significant interaction was between gender and the positive emotional trait factor (p = 0.002), such that the adjusted OR for positive emotional trait was greater for males (OR 1.77; 95% CI 1.67, 1.88) than for females (OR 1.40; 95% CI 1.21, 1.63). The interaction between gender and negative emotional traits was associated with a p value of 0.04, and the adjusted OR for negative emotional traits was also higher for males (OR 1.52; 95% CI 1.42, 1.62) than for females (OR 1.24; 95% CI 1.05, 1.46). No other significant interactions were noted.
Discussion
The intent of this study was to examine characteristics of SRH among a large Army sample and to explore correlates of SRH. Among a large, relatively young, and healthy sample of US Army Soldiers, the vast majority of participants consider themselves to be in “good” or “excellent” overall health. Results from the OLR model demonstrate that self-reported sleep quality was by far the strongest predictor of SRH, even when controlling for age, gender, marital status, and Army component (AD/R/NG). APFT score and BMI were also uniquely associated with SRH, whereas emotional fitness was one of the four psychosocial dimensions to notably contribute to the model. In contrast, smoking and healthy eating showed only weak associations with SRH, and binge drinking was not a statistically significant predictor once the model had been adjusted for covariates. Although the remaining three psychosocial scores (social, family, and spiritual fitness) showed slightly positive associations with SRH, the results suggest that these dimensions contributed minimally to perceived overall health from beyond what is accounted for by emotional fitness.
Group comparisons revealed some key differences in how participants rated their overall health. Most notably, officers and males were somewhat more likely to report better SRH than enlisted personnel and females. Previous research has generally found little overall difference in SRH between sexes when other sociodemographic characteristics are controlled for [8, 29, 68], although it should be noted that military samples have also seen higher SRH in men [5, 15]. Associations between and among various independent variables and SRH were consistent across officers and enlisted personnel, along with most other demographic groups, with the exception of sex and positive emotional traits. Interestingly, the relation between positive emotional traits and SRH was weaker for females than males. Since this interaction was in the opposite direction as would have been expected, more research may be required to properly interpret it.
Within a clinical context, extensive discussion has focused on patient-reported outcomes [50]. Specific to SRH, previous research has contrasted SRH with clinical symptoms, clinical conditions, and objective outcomes [69]. However, many DoD health initiatives take a preventive approach and are aimed at the healthy military population. Frequently, these initiatives implicitly recognize that health and human performance are multifaceted and the sum of many parts [45–47]. Within a preventive context, improvement in subjective outcomes, such as SRH, may be necessary for Soldiers to buy-in to a program as a whole. Testing this notion is beyond the scope of this analysis, but it does provide the impetus for understanding and applying the pattern of results. Below, we begin with sleep.
Our findings regarding sleep quality are consistent with previous research showing that both too little and too much sleep can lead to a wide range of physical and mental health detriments [33, 34, 70, 71]. In general, negative effects of poor sleep can include an increased risk of mortality, obesity, poor cognitive performance, and a number of additional health outcomes [72–77]. This is particularly relevant with regard to military populations, where limited or fragmented sleep can be commonplace, if not the norm [67, 78, 79]. Recent epidemiological surveys have found approximately half of all AD Army personnel report getting fewer than 6 h of sleep per night [1] and may develop sleep disorders that persist beyond return from deployment [80].
Results from the present study highlight the importance of sleep for military health and performance, both overall, and to a lesser extent, relative to comparable health behaviors. Numerous health campaigns in the military target sleep, either directly or indirectly [80]. Sleep, physical activity, and diet are all targeted under the Army’s Performance Triad program [81]. All three areas are typically seen as intractable modern problems, which are easy to identify and hard to fix. All three areas also connect to distinct job-related military policies. Frequently, nutrition and physical activity are seen as complementary components to a healthy lifestyle. Yet, in the present study, sleep demonstrated a stronger relation to SRH than physical fitness (which is related to but different from physical activity) and nutrition. This does not indicate that sleep is more important than fitness or nutrition; but it does imply that sleep may have more direct subjective benefits, which may in turn improve objective health outcomes. There is also a larger case to be made that the cognitive and physiological effects of sleep make it a primary foundation for other health behaviors such as diet and exercise [82]. Key areas for future military policy on sleep include positive (rather than deficit-based) health messaging and evidence-based preventive interventions [80].
Although a great deal of literature has focused on short sleep duration, less population-level research has looked at the impact of sleep quality on overall health status. This is potentially problematic because laboratory studies have shown that self-reports of sleep duration can be unreliable, particularly in those previously diagnosed with sleep difficulties [83, 84]. Furthermore, consensus is lacking over the optimal cutoff for a “healthy” sleep duration [85, 86], and whether this differs between individuals of the same age. A previous study by Rice et al. (2011) found no relation between self-reported sleep duration and SRH in a sample of Army trainees [40]. The present study uses an established measure of sleep quality (the PIRS-2) [65, 67] and, in this way, may expound upon existing knowledge of the detrimental effects of poor sleep on total health.
A number of health and behavioral factors, such as binge drinking, smoking, and healthy eating, showed only trivial effects on SRH. Although univariate analyses showed a negative association with SRH and binge drinking (unadjusted OR 0.71; 95% CI 0.65, 0.79), this effect became slightly positive and non-significant after adjusting for covariates. Results showed that smoking and healthy eating were significantly related to SRH, but this relation was relatively weak compared to the stronger predictors like sleep, BMI, and positive and negative emotional traits. Previous research has produced mixed results over any links between self-reported healthy eating behaviors and SRH [37, 87]; however, excessive alcohol use and smoking have previously been suggested as risk factors for poorer SRH [5, 35, 36, 67, 69]. It is especially surprising that behaviors conventionally viewed as unequivocally unhealthy can have such a negligible effect on SRH.
Emotional fitness was the only one of the four psychosocial dimensions showing a noteworthy association with SRH. The other three psychosocial dimensions (social, family, and spiritual) were essentially overshadowed by emotional fitness (Table 3 for ORs). Although certainly overlap exists between these four dimensions, they are implicitly considered non-redundant scores (i.e., each should contribute uniquely to overall health). However, our analyses suggest little if any additional effect on overall health from each of the social, family, and spiritual dimensions. It should also be noted that the emotional fitness dimension of the GAT has approximately twice as many scales as the other three psychosocial dimensions combined: this imbalance may in part account for the difference in effect sizes. However, more research is clearly needed to identify how distinct these dimensions are from each other, and whether other types of positive outcomes can be associated with high scores in these areas.
One interpretation of the overall pattern of results is that affective states influence the responses of participants to SRH items. Participants who sleep poorly, for example, may feel worse at the time they are surveyed and in turn be more likely to rate their overall health as poor. Consistent with this, emotional health was one of the largest predictors of SRH in our model, which broke down namely into factors of negative and positive emotion. Previous studies have also reported notable associations between positive and negative affect and SRH [20, 88, 89]. In contrast, the other psychosocial dimensions may be indicative of longer-term stability in relationships and self-identity. Longitudinal research suggests that respondents’ SRH remains generally stable over short periods of time [90]. Over a few years though, it may fluctuate relative to changes in a variety of health status measures, including behavioral intentions and social support [25]. It is possible that the other psychosocial dimensions are influenced themselves by one’s emotional health, but separately are not as important to overall health ratings. It seems plausible then that one’s self-rating of health might be particularly sensitive to immediate, if temporary, changes in feelings, moods, or emotional state.
A related view is that self-ratings of health are influenced by a person’s contextual thought processes and personal characteristics relative to their peers [24, 91]. Consequently, self-ratings of health may be influenced by the environment the individual lives in, the perceived health of others around them, and their own expectations of how “healthy” they should be. Because Soldiers are generally young, active, and otherwise healthy individuals, and surrounded by others similar to themselves, the question raised is whether certain behaviors—such as drinking, smoking, and poor nutrition, which typically carry longer-term health risks—are minimized or even neglected altogether when considering one’s immediate health status. It is also noteworthy that age was not a significant factor in our regression model, which supports a context-dependent view of how individuals self-rated health. Future research should investigate whether these findings are consistent across different age groups of military subsets, and whether there are factors that mediate the relation between risky health behaviors and SRH.
To some extent, our results are consistent with the view of SRH as a situational assessment of overall health. The counterpoint is that subjective states are often indicators of overarching traits and may in fact be indicative of more stable characteristics that themselves drive SRH. For instance, physical fitness (as measured by APFT scores and BMI) was also positively associated with SRH in our analysis, which is unlikely itself to be directly influenced by subjective emotional states on a given day. Mood may be a driving factor of an individual’s level of physical activity; however, the degree of sustained care and habit required to maintain a particular level of fitness suggests lasting characteristics beyond one’s immediate state of mind. The observed relation between physical fitness and SRH is also well supported in the literature. For example, regular physical activity and higher aerobic capacity have been linked to better SRH [36, 92–94], whereas obesity and cardiovascular disease are associated with worse SRH [4, 6, 17]. Philips et al. [95] found that self-reported physical fitness was at least as effective as SRH in predicting future mortality. Future research should examine the extent to which temporary affective states as opposed to lasting characteristics influence SRH, and whether these relations are consistent across different populations.
Importantly, the use of a few, simple, direct questions may be preferable to the current practice of multiple, often redundant questions. The National Research Center [96] recently reported on the concept of survey fatigue, where respondents become overwhelmed with the number of questions and/or surveys they are asked to take. Survey fatigue likely results in lower response rates and incomplete or inaccurate information. Having fewer questions and knowing the various areas that they explain would be very useful for maximizing the likelihood of complete and accurate responses.
Conclusion
This study provides further support for the idea that perceived health status is a multifaceted assessment of one’s physical and emotional wellbeing, which is subject to both intrinsic and extrinsic views of what an individual considers part of their “overall health.” By design, self-reported items of health are broad, inclusive measures that may be sensitive to underlying health conditions missed by more objective and specific measures of health. The results of the current study identified various psychosocial and behavioral correlates that consistently relate to SRH in a large military sample—namely sleep quality, emotional fitness, and physical fitness. These associations were largely consistent with the civilian literature; however, they also underscore the need for additional studies examining drivers of SRH among unique populations—such as military personnel and different cultures. In particular, some risky health behaviors showed decidedly little relation with overall health, which runs counter to findings from previous research examining SRH in the military [5]. Furthermore, only one of the GAT psychosocial measures showed a notable association with SRH. Although additional research delineating the relation between overall health and the social, family, and spiritual fitness dimensions may be important, our analyses suggest that SRH may be useful as a surrogate for sleep quality, emotional fitness, and physical fitness. A single question could potentially be considered as a replacement for multiple questions to reduce participant burden and propensity for survey fatigue.
Our findings include some caveats about how they should be interpreted, not the least of which is the use of entirely self-reported data as well as the cross-sectional nature of the study. Some additional demographic variables were also not available (race/ethnicity, education level, and a more detailed description of rank), but the demographic characteristics available showed a sample remarkably representative of the Army as a whole (as previously mentioned) [51]. This is important given that the sample was not randomly drawn. Considering the limitations, generalizing the findings to other military branches, or more heterogeneous civilian populations, may be problematic. A recent study by Vie et al. [55] provides preliminary evidence for the factorial validity of the psychosocial scales; additional work might focus on examining the properties of the physical health scales (e.g., healthy eating, sleep). These limitations notwithstanding, the data presented here offer valuable insights into our current understanding of the various factors driving self-ratings of health, particularly in a highly unique population such as the Army. The use of self-rated health items offers a practical outcome measure for researchers and policy makers to gauge the overall health of the force and may be a valuable benchmark in evaluating more precise measures of psychological health and resilience. When administered over time, SRH can also be a useful tool in screening for health disparities among different subgroups, which can be addressed by policy changes and interventions targeting these gaps. Finally, because SRH can be measured in as few as one or two items, both the burden on respondents and the cost for researchers are decreased. This efficiency is in part what makes single-item SRH especially well suited to epidemiological research and surveillance, where longer measures of global health can be impractical and cost prohibitive.
Future directions might include examining the extent to which immediate versus long-term considerations determine self-ratings of health; how sleep quality as opposed to sleep quantity affects overall ratings of health; and the precise psychological, physiological, and behavioral components that drive self-ratings of health. Additional studies should also determine to what extent, if any, these results can be generalized to demographically similar populations, such as branches of the other armed services or athletes.
Notes
The Uniformed Services University of the Health Sciences Institutional Review Board concluded that a full review was not required for this investigation. This study was not classified as human subjects research since the Army provided data stripped of identification elements to the Consortium for Health and Military Performance per an established data use agreement.
References
Barlas, F. M., Higgins, W. B., Pflieger, J. C., & Diecker, K. (2013). 2011 Department of defense health related behaviors survey of active duty military personnel. (Final report). Fairfax, VA: ICF International.
Bramoweth, A. D., & Germain, A. (2013). Deployment-related insomnia in military personnel and veterans. Current Psychiatry Reports, 15(10), 401. doi:10.1007/s11920-013-0401-4.
Campbell, D. J., & Nobel, O. B. Y. (2009). Occupational stressors in military service: A review and framework. Military Psychology, 21(Suppl. 2), S47–S67.
Geiger, S. D., Sabanayagam, C., & Shankar, A. (2012). The relationship between insufficient sleep and self-rated health in a nationally representative sample. Journal of Environment and Public Health, 2012, 518263. doi:10.1155/2012/518263.
Haddock, C. K., Poston, W. S., Pyle, S. A., Klesges, R. C., Vander Weg, M. W., Peterson, A., & Debon, M. (2006). The validity of self-rated health as a measure of health status among young military personnel: evidence from a cross-sectional survey. Health and Quality of Life Outcomes, 4, 57. doi:10.1186/1477-7525-4-57.
Wagner, D. C., & Short, J. L. (2014). Longitudinal predictors of self-rated health and mortality in older adults. Preventing Chronic Disease, 11, E93. doi:10.5888/pcd11.130241.
Wang, J. M., Lee, L. O., & Spiro, A. (2015). Gender differences in the impact of warfare exposure on self-rated health. Women’s Health Issues, 25(1), 35–41. doi:10.1016/j.whi.2014.09.003.
Rohrer, J. E., Arif, A., Denison, A., Young, R., & Adamson, S. (2007). Overall self-rated health as an outcome indicator in primary care. Journal of Evaluation in Clinical Practice, 13(6), 882–888. doi:10.1111/j.1365-2753.2006.00766.x.
Ahmed, S. M., Rana, A. K., Chowdhury, M., & Bhuiya, A. (2002). Measuring perceived health outcomes in non-western culture: does SF-36 have a place? Journal of Health, Population, and Nutrition, 20(4), 334–342.
Barile, J. P., Reeve, B. B., Smith, A. W., Zack, M. M., Mitchell, S. A., Kobau, R., … Thompson, W. W. (2013). Monitoring population health for healthy people 2020: Evaluation of the NIH PROMIS(R) global health, CDC healthy days, and satisfaction with life instruments. Quality of Life Research, 22(6), 1201–1211. doi:10.1007/s11136-012-0246-z.
Hays, R. D., Spritzer, K. L., Thompson, W. W., & Cella, D. (2015). U.S. general population estimate for “excellent” to “poor” self-rated health item. Journal of General Internal Medicine, 30(10), 1511–1516. doi:10.1007/s11606-015-3290-x.
Cunningham, R., Carter, K., Connor, J., & Fawcett, J. (2010). Does health status matter for the risk of injury? The New Zealand Medical Journal, 123(1327), 35–46.
DeSalvo, K. B., Bloser, N., Reynolds, K., He, J., & Muntner, P. (2006). Mortality prediction with a single general self-rated health question: A meta-analysis. Journal of General Internal Medicine, 21(3), 267–275. doi:10.1111/j.1525-1497.2005.00291.x.
Ferraro, K. F., & Su, Y. P. (2000). Physician-evaluated and self-reported morbidity for predicting disability. American Journal of Public Health, 90(1), 103–108.
Rice, V. J., Mays, M. Z., & Gable, C. (2009). Self-reported health status of students in-processing into military medical advanced individual training. Work (Reading, Mass.), 34(4), 387–400. doi:10.3233/WOR-2009-0939.
Benjamins, M. R., Hummer, R. A., Eberstein, I. W., & Nam, C. B. (2004). Self-reported health and adult mortality risk: an analysis of cause-specific mortality. Social Science & Medicine (1982), 59(6), 1297–1306. doi:10.1016/j.socscimed.2003.01.001.
Rumsfeld, J. S., Alexander, K. P., Goff, D. C. Jr., Graham, M. M., Ho, P. M., Masoudi, F. A., … Spertus, J. A. (2013). Cardiovascular health: The importance of measuring patient-reported health status: A scientific statement from the American Heart Association. Circulation, 127(22), 2233–2249. doi:10.1161/CIR.0b013e3182949a2e.
Waller, M., McGuire, A. C., & Dobson, A. J. (2015). Alcohol use in the military: Associations with health and wellbeing. Substance Abuse Treatment, Prevention, and Policy, 10, 27. doi:10.1186/s13011-015-0023-4.
Lehavot, K., Der-Martirosian, C., Simpson, T. L., Shipherd, J. C., & Washington, D. L. (2013). The role of military social support in understanding the relationship between PTSD, physical health, and healthcare utilization in women veterans. Journal of Traumatic Stress, 26(6), 772–775. doi:10.1002/jts.21859.
Cundiff, J. M., Smith, T. W., Uchino, B. N., & Berg, C. A. (2013). Subjective social status: Construct validity and associations with psychosocial vulnerability and self-rated health. International Journal of Behavioral Medicine, 20(1), 148–158. doi:10.1007/s12529-011-9206-1.
Franks, P., Gold, M. R., & Fiscella, K. (2003). Sociodemographics, self-rated health, and mortality in the US. Social Science & Medicine (1982), 56(12), 2505–2514.
Melchior, M., Berkman, L. F., Niedhammer, I., Chea, M., & Goldberg, M. (2003). Social relations and self-reported health: a prospective analysis of the French Gazel cohort. Social Science & Medicine (1982), 56(8), 1817–1830.
Mora, P. A., DiBonaventura, M. D., Idler, E., Leventhal, E. A., & Leventhal, H. (2008). Psychological factors influencing self-assessments of health: Toward an understanding of the mechanisms underlying how people rate their own health. Annals of Behavioral Medicine, 36(3), 292–303. doi:10.1007/s12160-008-9065-4.
Jylhä, M. (2009). What is self-rated health and why does it predict mortality? Towards a unified conceptual model. Social Science & Medicine (1982), 69(3), 307–316. doi:10.1016/j.socscimed.2009.05.013.
Bailis, D. S., Segall, A., & Chipperfield, J. G. (2003). Two views of self-rated general health status. Social Science & Medicine (1982), 56(2), 203–217.
Hays, R. D., Bjorner, J. B., Revicki, D. A., Spritzer, K. L., & Cella, D. (2009). Development of physical and mental health summary scores from the patient-reported outcomes measurement information system (PROMIS) global items. Quality of Life Research, 18(7), 873–880. doi:10.1007/s11136-009-9496-9.
Centers for Disease Control and Prevention (2000). Measuring Healthy Days (CDC). Atlanta, GA: CDC.
Mavaddat, N., Kinmonth, A. L., Sanderson, S., Surtees, P., Bingham, S., & Khaw, K. T. (2011). What determines self-rated health (SRH)? A cross-sectional study of SF-36 health domains in the EPIC-Norfolk cohort. Journal of Epidemiology and Community Health, 65(9), 800–806. doi:10.1136/jech.2009.090845.
Unden, A. L., & Elofsson, S. (2006). Do different factors explain self-rated health in men and women? Gender Medicine, 3(4), 295–308.
Smith, P. M., Glazier, R. H., & Sibley, L. M. (2010). The predictors of self-rated health and the relationship between self-rated health and health service needs are similar across socioeconomic groups in Canada. Journal of Clinical Epidemiology, 63(4), 412–421. doi:10.1016/j.jclinepi.2009.08.015.
Singh-Manoux, A., Dugravot, A., Shipley, M. J., Ferrie, J. E., Martikainen, P., Goldberg, M., & Zins, M. (2007). The association between self-rated health and mortality in different socioeconomic groups in the GAZEL cohort study. International Journal of Epidemiology, 36(6), 1222–1228. doi:10.1093/ije/dym170.
Magee, C. A., Caputi, P., & Iverson, D. C. (2011). Relationships between self-rated health, quality of life and sleep duration in middle aged and elderly Australians. Sleep Medicine, 12(4), 346–350. doi:10.1016/j.sleep.2010.09.013.
Kim, J. H., Kim, K. R., Cho, K. H., Yoo, K. B., Kwon, J. A., & Park, E. C. (2013). The association between sleep duration and self-rated health in the Korean general population. Journal of Clinical Sleep Medicine, 9(10), 1057–1064. doi:10.5664/jcsm.3082.
Silva-Costa, A., Griep, R. H., & Rotenberg, L. (2015). Associations of a short sleep duration, insufficient sleep, and insomnia with self-rated health among nurses. PLoS ONE, 10(5), e0126844. doi:10.1371/journal.pone.0126844.
Poikolainen, K., Vartiainen, E., & Korhonen, H. J. (1996). Alcohol intake and subjective health. American Journal of Epidemiology, 144(4), 346–350.
Froom, P., Melamed, S., Triber, I., Ratson, N. Z., & Hermoni, D. (2004). Predicting self-reported health: the CORDIS study. Preventive Medicine, 39(2), 419–423. doi:10.1016/j.ypmed.2004.02.006.
Zarini, G. G., Vaccaro, J. A., Canossa Terris, M. A., Exebio, J. C., Tokayer, L., Antwi, J., … Huffman, F. G. (2014). Lifestyle behaviors and self-rated health: the living for health program. Journal of Environmental and Public Health, 2014, 9. doi:10.1155/2014/315042.
Barrett, D. H., Doebbeling, C. C., Schwartz, D. A., Voelker, M. D., Falter, K. H., Woolson, R. F., & Doebbeling, B. N. (2002). Posttraumatic stress disorder and self-reported physical health status among U.S. Military personnel serving during the Gulf War period: a population-based study. Psychosomatics, 43(3), 195–205. doi:10.1176/appi.psy.43.3.195.
Heltemes, K. J., Holbrook, T. L., Macgregor, A. J., & Galarneau, M. R. (2012). Blast-related mild traumatic brain injury is associated with a decline in self-rated health amongst US military personnel. Injury, 43(12), 1990–1995. doi:10.1016/j.injury.2011.07.021.
Rice, V. J. B., Banderet, L. E., Marra, D., & Butler, J. (2011). The Relationship of self-reported health to other indices of physical health and performance among soldiers. Proceedings of the Human Factors and Ergonomics Society Annual Meeting, 55(1), 1140–1144. doi:10.1177/1071181311551238.
Trump, D. H., Brady, J., & Olsen, C. H. (2004). Self-rated health and subsequent health care use among military personnel returning from international deployments. Military Medicine, 169(2), 128–133.
Kazman, J. B., de la Motte, S., Bramhall, E. M., Purvis, D. L., & Deuster, P. A. (2015). Physical fitness and injury reporting among active duty and National Guard/Reserve women: Associations with risk and lifestyle factors. US Army Medical Department Journal, 49–57.
Deuster, P. A., Grunberg, N. E., & O’Connor, F. G. (2014). An integrated approach for special operations. Journal of Special Operations Medicine, 14(2), 86–90.
Deuster, P. A., & O’Connor, F. G. (2015). Human performance optimization: culture change and paradigm shift. J Strength Cond Res, 29(Suppl 11), S52–56, doi:10.1519/JSC.0000000000001118.
Jonas, W., O’Connor, F. G., Deuster, P. A., Peck, J., Shake, C., & Frost, S. S. (2010). Why total force fitness? Military Medicine, 175(8), S6–S13.
Cornum, R., Matthews, M. D., & Seligman, M. E. (2011). Comprehensive soldier fitness: building resilience in a challenging institutional context. The American Psychologist, 66(1), 4–9. doi:10.1037/a0021420.
Seligman, M. E., & Fowler, R. D. (2011). Comprehensive Soldier Fitness and the future of psychology. The American Psychologist, 66(1), 82–86. doi:10.1037/a0021898.
Peterson, C., Park, N., & Castro, C. A. (2011). Assessment for the U.S. Army comprehensive soldier fitness program: the global assessment tool. The American Psychologist, 66(1), 10–18. doi:10.1037/a0021658.
Lester, P. B., Harms, P. D., Herian, M. N., & Sowden, W. J. (2015). A force of change: Chris Peterson and the US Army’s Global Assessment Tool. The Journal of Positive Psychology, 10(1), 7–16. doi:10.1080/17439760.2014.927904.
Weil, A. R. (2016). The Patient engagement imperative. Health Affairs, 35(4), 563. doi:10.1377/hlthaff.2016.0337.
Department of Defense (2012). Demographics Profile of the Military Community (DOD). Washington, DC: DOD.
Carver, C. S., Scheier, M. F., & Weintraub, J. K. (1989). Assessing coping strategies: a theoretically based approach. Journal of Personality and Social Psychology, 56(2), 267–283.
Spitzer, R. L., Kroenke, K., & Williams, J. B. (1999). Validation and utility of a self-report version of PRIME-MD: the PHQ primary care study. Primary care evaluation of mental disorders. Patient health questionnaire. JAMA, 282(18), 1737–1744.
Lester, P. B., McBride, S., Bliese, P. D., & Adler, A. B. (2011). Bringing science to bear: an empirical assessment of the Comprehensive Soldier Fitness program. The American Psychologist, 66(1), 77–81. doi:10.1037/a0022083.
Vie, L. L., Scheier, L. M., Lester, P., & Seligman, M. E. (2016). Initial validation of the U.S. Army global assessment tool. Military Psychology, 28(6), 468–487.
Lester, P. B., Harms, P. D., Bulling, D. J., Herian, M. N., & Spain, S. M. (2011). Evaluation Of Relationships Between Reported Resilience And Soldier Outcomes. Report #1: Negative outcomes (Suicide, drug use and violent crime).
Sweeney, P. J., Thompson, V., & Blanton, H. (2009). Trust and influence in combat: An interdependence model. Journal of Applied Social Psychology, 39(1), 235–264. doi:10.1111/j.1559-1816.2008.00437.x.
Multidimensional measurement of religiousness/spirituality for use in health research: A Report of the Fetzer Institute/ National Institute on Aging Working Group (1999). Kalamazoo, MI: Fetzer Institute.
Lester, P. B., Harms, P. D., Bulling, D. J., Herian, M. N., Beal, S. J., & Spain, S. M. (2011). Evaluation Of Relationships Between Reported Resilience And Soldier Outcomes. Report #2: Positive Performance Outcomes in Officers (Promotions, Selections, & Professions).
Field Manual 7–22 (2012). Army physical readiness training. Washington, DC: Headquarters Department of the Army.
Jones, S. B., Knapik, J. J., Sharp, M. A., Darakjy, S., & Jones, B. H. (2007). The validity of self-reported physical fitness test scores. Military Medicine, 172(2), 115–120.
Centers for Disease Control and Prevention (CDC) “About Adult BMI” (2016). https://www.cdc.gov/healthyweight/assessing/bmi/adult_bmi/index.html. Accessed 1 September 2016.
Guenther, P. M., Kirkpatrick, S. I., Reedy, J., Krebs-Smith, S. M., Buckman, D. W., Dodd, K. W., … Carroll, R. J. (2014). The healthy eating index-2010 is a valid and reliable measure of diet quality according to the 2010 dietary guidelines for Americans. The Journal of Nutrition, 144(3), 399–407. doi:10.3945/jn.113.183079.
Purvis, D. L., Lentino, C. V., Jackson, T. K., Murphy, K. J., & Deuster, P. A. (2013). Nutrition as a component of the performance triad: how healthy eating behaviors contribute to soldier performance and military readiness. US Army Medical Department Journal, 66–78.
Moul, D. E., Mai, E., & Shablesky, M. (2009). The 2-item and 20-item versions of the Pittsburgh Insomnia Rating Scale (PIRS): Design methods and initial modeling. Melbourne: Paper presented at the Annual Meeting of the World Psychiatric Association. Accessed 29 November 2009.
Moul, D. E., Pilkonis, P. A., Miewald, J. M., Carey, T. J., & Buysse, D. J. (2002). Preliminary study of the test-retest reliability and concurrent validities of the Pittsburgh Insomnia Rating Scale (PIRS). Sleep 25 Abstract Supplement, A246–A247.
Lentino, C. V., Purvis, D. L., Murphy, K. J., & Deuster, P. A. (2013). Sleep as a component of the performance triad: the importance of sleep in a military population. US Army Medical Department Journal, 98–108.
Cooper, H. (2002). Investigating socio-economic explanations for gender and ethnic inequalities in health. Social Science & Medicine (1982), 54(5), 693–706.
Altman, C. E., Van Hook, J., & Hillemeier, M. (2016). What does self-rated health mean? changes and variations in the association of obesity with objective and subjective components of self-rated health. Journal of Health and Social Behavior, 57(1), 39–58. doi:10.1177/0022146515626218.
Frange, C., de Queiroz, S. S., da Silva Prado, J. M., Tufik, S., & de Mello, M. T. (2014). The impact of sleep duration on self-rated health. Sleep Science, 7(2), 107–113. doi:10.1016/j.slsci.2014.09.006.
Gottlieb, D. J., Redline, S., Nieto, F. J., Baldwin, C. M., Newman, A. B., Resnick, H. E., & Punjabi, N. M. (2006). Association of usual sleep duration with hypertension: the sleep heart health study. Sleep, 29(8), 1009–1014.
Boyko, E. J., Seelig, A. D., Jacobson, I. G., Hooper, T. I., Smith, B., Smith, T. C., … Millennium Cohort Study Team. (2013). Sleep characteristics, mental health, and diabetes risk: A prospective study of U.S. military service members in the millennium cohort study. Diabetes Care, 36(10), 3154–3161. doi:10.2337/DC13-0042.
Cappuccio, F. P., D’Elia, L., Strazzullo, P., & Miller, M. A. (2010). Sleep duration and all-cause mortality: A systematic review and meta-analysis of prospective studies. Sleep, 33(5), 585–592.
Cappuccio, F. P., Taggart, F. M., Kandala, N.-B., Currie, A., Peile, E., Stranges, S., & Miller, M. A. (2008). Meta-analysis of short sleep duration and obesity in children and adults. Sleep, 31(5), 619–626.
Gangwisch, J. E., Heymsfield, S. B., Boden-Albala, B., Buijs, R. M., Kreier, F., Pickering, T. G., … Malaspina, D. (2007). sleep duration as a risk factor for diabetes incidence in a large US sample. Sleep, 30(12), 1667–1673.
Hoevenaar-Blom, M. P., Spijkerman, A. M., Kromhout, D., van den Berg, J. F., & Verschuren, W. M. (2011). Sleep duration and sleep quality in relation to 12-year cardiovascular disease incidence: the MORGEN study. Sleep, 34(11), 1487–1492. doi:10.5665/sleep.1382.
Knutson, K. L., Spiegel, K., Penev, P., & Van Cauter, E. (2007). The metabolic consequences of sleep deprivation. Sleep medicine reviews, 11(3), 163–178. doi:10.1016/j.smrv.2007.01.002.
Capaldi II, V. F., Guerrero, M. L., & Killgore, W. D. (2011). Sleep disruptions among returning combat veterans from Iraq and Afghanistan. Military Medicine, 176(8), 879–888.
Crowley, S. K., Wilkinson, L. L., Burroughs, E. L., Muraca, S. T., Wigfall, L. T., Louis-Nance, T., & Burroughs, E. L. (2012). Sleep during basic combat training: A qualitative study. Military Medicine, 177(7), 823–828.
Troxel, W. M., Shih, R. A., Pedersen, E. R., Geyer, L., Fisher, M. P., Griffin, B. A., … Steinberg, P. S. (2015). Sleep in the military: promoting healthy sleep among U.S. service members. Santa Monica, CA: RAND.
The Performance Triad (2016). http://armymedicine.mil/Pages/performance-triad.aspx. Accessed 10 June 2016.
Lundahl, A., & Nelson, T. D. (2015). Sleep and food intake: A multisystem review of mechanisms in children and adults. Journal of Health Psychology, 20(6), 794–805. doi:10.1177/1359105315573427.
Cespedes, E. M., Hu, F. B., Redline, S., Rosner, B., Alcantara, C., Cai, J., & Reid, K. J. (2016). Comparison of self-reported sleep duration with actigraphy: results from the hispanic community health study/study of latinos sueno ancillary study. American Journal of Epidemiology, 183(6), 561–573. doi:10.1093/aje/kwv251.
Lauderdale, D. S., Knutson, K. L., Yan, L. L., Liu, K., & Rathouz, P. J. (2008). Self-reported and measured sleep duration: how similar are they? Epidemiology (Cambridge, Mass.), 19(6), 838–845. doi:10.1097/EDE.0b013e318187a7b0.
Buysse, D. J., Grunstein, R., Horne, J., & Lavie, P. (2010). Can an improvement in sleep positively impact on health? Sleep Medicine Reviews, 14(6), 405–410. doi:10.1016/j.smrv.2010.02.001.
Wesensten, N. J., & Balkin, T. J. (2013). The challenge of sleep management in military operations. US Army Medical Department Journal, 109–118.
Goodwin, D. K., Knol, L. L., Eddy, J. M., Fitzhugh, E. C., Kendrick, O. W., & Donahue, R. E. (2006). The relationship between self-rated health status and the overall quality of dietary intake of US adolescents. Journal of the American Dietetic Association, 106(9), 1450–1453. doi:10.1016/j.jada.2006.06.011.
Dua, J. K. (1994). Comparative predictive value of attributional style, negative affect, and positive affect in predicting self-reported physical health and psychological health. Journal of Psychosomatic Research, 38(7), 669–680.
Pettit, J. W., Kline, J. P., Gencoz, T., Gencoz, F., & Joiner, T. E. Jr. (2001). Are happy people healthier? The specific role of positive affect in predicting self-reported health symptoms. Journal of Research in Personality, 35(4), 521–536. doi:10.1006/jrpe.2001.2327.
Miilunpalo, S., Vuori, I., Oja, P., Pasanen, M., & Urponen, H. (1997). Self-rated health status as a health measure: the predictive value of self-reported health status on the use of physician services and on mortality in the working-age population. Journal of Clinical Epidemiology, 50(5), 517–528.
Beland, F., Birch, S., & Stoddart, G. (2002). Unemployment and health: contextual-level influences on the production of health in populations. Social Science & Medicine (1982), 55(11), 2033–2052.
Berglund, E., Lytsy, P., & Westerling, R. (2016). Active traveling and its associations with self-rated health, BMI and physical activity: A comparative study in the adult swedish population. International Journal of Environmental Research and Public Health, 13(5), doi:10.3390/ijerph13050455.
Jones, S. A., Wen, F., Herring, A. H., & Evenson, K. R. (2016). Correlates of US adult physical activity and sedentary behavior patterns. Journal of Science and Medicine in Sport/Sports Medicine Australia. doi:10.1016/j.jsams.2016.03.009.
Kantomaa, M. T., Tammelin, T., Ebeling, H., Stamatakis, E., & Taanila, A. (2015). High levels of physical activity and cardiorespiratory fitness are associated with good self-rated health in adolescents. Journal of Physical Activity and Health, 12(2).
Phillips, A. C., Der, G., & Carroll, D. (2010). Self-reported health, self-reported fitness, and all-cause mortality: prospective cohort study. British Journal of Health Psychology, 15(Pt 2), 337–346. doi:10.1348/135910709x466180.
National Research Center. (2016). How to Avoid Survey Fatigue. http://www.n-r-c.com/how-to-avoid-survey-fatigue/. Accessed 12 December 2016.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflicts of interest.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Disclaimer
The views expressed are those of the authors and do not reflect the official policy or position of the Uniformed Services University of the Health Sciences, the Department of the Defense, or the U.S. Government.
Funding
This research was supported by a Grant from Comprehensive Soldier and Family Fitness (CSF2; HT9404-12-1-0017; F191GJ).
Rights and permissions
About this article

Cite this article
Golenbock, S., Kazman, J.B., Krauss, S. et al. General health status in army personnel: relations with health behaviors and psychosocial variables. Qual Life Res 26, 1839–1851 (2017). https://doi.org/10.1007/s11136-017-1523-7
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11136-017-1523-7