
Abstract
Purpose
Psychological positive health and health complaints have long been ignored scientifically. Sleep plays a critical role in children and adolescents development. We aimed at studying the association of sleep duration and quality with psychological positive health and health complaints in children and adolescents from southern Spain.
Methods
A randomly selected two-phase sample of 380 healthy Caucasian children (6–11.9 years) and 304 adolescents (12–17.9 years) participated in the study. Sleep duration (total sleep time), perceived sleep quality (morning tiredness and sleep latency), psychological positive health and health complaints were assessed using the Health Behaviour in School-aged Children questionnaire.
Results
The mean (standard deviation [SD]) reported sleep time for children and adolescents was 9.6 (0.6) and 8.8 (0.6) h/day, respectively. Sleep time ≥10 h was significantly associated with an increased likelihood of reporting no health complaints (OR 2.3; P = 0.005) in children, whereas sleep time ≥9 h was significantly associated with an increased likelihood of overall psychological positive health and no health complaints indicators (OR ~ 2; all P < 0.05) in adolescents. Reporting better sleep quality was associated with an increased likelihood of reporting excellent psychological positive health (ORs between 1.5 and 2.6; all P < 0.05). Furthermore, children and adolescents with no difficulty falling asleep were more likely to report no health complaints (OR ~ 3.5; all P < 0.001).
Conclusions
Insufficient sleep duration and poor perceived quality of sleep might directly impact quality of life in children, decreasing general levels of psychological positive health and increasing the frequency of having health complaints.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Total sleep time occupies about one-third of a human life. Thus, it is an extremely important factor for general health promotion and well-being. Indeed, sleep is especially important for children and adolescents’ general health [1]. It is noteworthy that total sleep time is positively associated with health status [2] and inversely associated with negative health outcomes [1] in the above populations. Furthermore, insufficient sleep duration is related to higher body mass index (BMI) and waist circumference, indicating a higher risk of poor health [3]. However, lifestyle changes in our modern society (stress, later bedtime, more media usage, etc.) result in a reduction in average total sleep time, especially in children and adolescents [4–6]. While several studies reported a direct association of sleep quality with obesity [7], with health-related quality of life [8] and with cardiovascular risk factors in youth [9], previous research has largely focused on sleep duration while neglecting its quality [7].
One goal of research in this area is to track the impact of sources of health-related problems. An important concept in this regard is positive health, which describes a state beyond the mere absence of disease [10]. It is defined as a multifactor construct encompassing subjective, biological and functional dimensions [10]. It has been suggested recently that positive health is a predictor of mental health in ageing, health costs and prognosis [10]. Subjective variables of positive health (also called psychological positive health) refer to both psychological and social well-being, which include life satisfaction, self-esteem, self-image and perceived physical health status [10]. Social relationships are also included in this broad concept [11] due to their close link with the person’s well-being [12]. The literature has mainly clustered around the biological–functional dimension of positive health and its relationship with cardiovascular diseases and obesity. To date, psychological positive health has been ignored scientifically in spite of its importance in humans’ overall health [10] and its potential as a survival predictor [13].
Another important marker in child and adolescent research is the construct of health complaints. These are heterogeneous conditions characterized by the persistent physical symptoms that cannot be explained by medical illness [14]. Abdominal pain, headaches, dizziness, musculoskeletal pain, fatigue, nausea and loss of appetite among others are considered as health complaints [15]. There is mounting evidence that health complaints are widespread and severe among children and adolescents [16]. These symptoms are everyday health problems that are often the cause of absence from school [17]. Moreover, health complaints frequently become chronic and lead to the development of somatisation disorder later in life [18].
Although there is an increasing interest in youth’s sleeping habits, the research is mainly focused on its impact on physical health factors [1, 2], with a special interest in BMI [3]. Whether sleep plays a role in youths’ psychological health levels and health complaints remains to be investigated. Therefore, the objective of the present study was to investigate the association of reported sleep time and perceived sleep quality with psychological positive health and health complaints in children and adolescents from southern Spain. Knowledge about sleep and health complaints would help us better understand how sleep is involved in children and adolescents’ psychological health. The study provides baseline data for implementing and evaluating interventions to improve children and adolescents’ health through changing their sleep behaviours.
Methods
Participants
A total of 389 healthy Caucasian children and 316 adolescents participated in the study. The sample was randomly selected using a two-phase, proportional cluster sampling method from the database of the census of the province of Cádiz (southern Spain). In the first phase, schools were selected from different strata according to the geographical localizations, age and sex. A total of 18 governmental schools agreed to participate in the study. Classes from the selected schools were randomly chosen and served as the smallest sampling units in the second phase. All the children of the selected classrooms were invited to participate in the study, and 95 % of the children agreed to take part in the study. In addition, a total of 9 children and 12 adolescents did not adequately complete the questionnaires, thereby excluding their data from the sample.
A comprehensive verbal description of the nature and purpose of the study was given to the children, adolescents, their parents and teachers. This information was also sent to parents or children supervisors by regular mail, and written consents from parents, children and adolescents were requested. The study was approved by the Review Committee for Research Involving Human Subjects at the University of Cádiz, Spain.
Procedure
Reported sleep time, perceived sleep quality (morning tiredness and sleep latency), psychological positive health and health complaints were assessed using the Health Behavior in School-aged Children (HBSC) questionnaire [19, 20]. The HBSC is an international WHO collaborative cross-national study [21]. All the questions used in the HBSC questionnaire showed a good reliability and validity in youth aged 10–18 years [21, 22]. Participants completed the questionnaire in their regular school classrooms, and trained investigators were available to answer questions of participants in order to avoid any confusion. Furthermore, these investigators followed a standardized protocol to ensure the consistency of data collection across classrooms.
Self-reported sleep measures
Total sleep time
These data were used to place participants in two groups: “good sleepers” or “poor sleepers”. Participants answered the question, “What time did you go to bed last night and wakeup this morning?” The reported sleep duration (hours) was calculated as the difference between wake-up time and bedtime. According to the National Sleep Foundation 2004 and 2006 polls [23, 24], the school-aged cut-off point for an optimal sleep is ≥10 h for children and ≥9 h for adolescents. These data are consistent with the mean total sleep time reported by the children and adolescents in the current sample. We, therefore, set the cut-offs for distinguishing between good and poor sleepers for children at poor sleepers <10 h and good sleeper ≥10 h. For adolescents, the group cut-offs are <9 h for poor sleepers and ≥9 h for good sleepers.
Morning tiredness
Participants were asked to indicate how often they felt tired (4-point scale: rarely or never, occasionally, 1–3 a week and 4 or more than week) when they went to school in the morning.
Perceived sleep latency
Participants indicated how often they had difficulty falling asleep (5-point scale: rarely or never, almost every month, almost every week, more than once a week and almost every day).
Psychological positive health measures
Perceived health status
Participants were asked to indicate how their health was overall by responding to the question on a 3-point Likert scale (excellent, good and fair).
Life satisfaction
Participants indicated how they felt about their life at present (4-point scale: very happy, happy, not very happy and not happy at all).
Quality of family relationships
Participants indicated how easy (4-point scale: very easy, easy, difficult and very difficult) was to talk to each family member about things that were bothering them. In those cases when the participant had no family member, the answer was “I do not have”. In total, there were five items (i.e. father, mother, other adults, brother and sister) measuring quality of family relationships. The internal consistency of the items was acceptable (Cronbach’s alpha = 0.734).
Quality of peer relationships
Participants indicated how easy (4-point scale: very easy, easy, difficult and very difficult) was to talk and interact with friends about things that were bothering them. In those cases when the participant had no relationships with friends, the answer was “I do not have relationships”. Four items (i.e. to talk with friends, to go out with friends, to have good friends and to find new friends) were used to measure the domain of quality of peer relationships, and the internal consistency of the domain was acceptable (Cronbach’s alpha = 0.684).
Academic performance
We also asked participants to indicate their thoughts (4-point scale: very good, good, average and under average) about their academic performance compared with their classmates.
Health complaints measure
Participants indicated how frequently [5-point scale: rarely or never (1), almost every month (2), almost every week (3), more than once a week (4) and almost every day (5)] they had each of the following eight symptoms: headache, stomach ache, backache, toothache, feeling low, irritability or bad temper, feeling nervous and feeling dizzy. Due to the fact that subjective health complaints tend to occur in clusters rather than as single symptoms [25], we computed a health complaints index by calculating the mean of all symptoms [26]. We used the aforementioned eight symptoms because they are the most commonly reported, according to the HBSC Symptom Checklist [27]. Although sleepiness is usually used in this index, we eliminated it in the present study since sleep variables are the main study outcomes. The internal consistency of the items of health complaints index was acceptable (Cronbach’s alpha = 0.708).
Data analysis
Since the study outcomes were assessed by means of categorical variables, we dichotomized the variables in order to perform binary logistic regression analyses. Dichotomization was done as follows: morning tiredness (No = rarely or never. Yes = occasionally, 1–3 a week and 4 or more than week), perceived sleep latency (No = rarely or never. Yes = almost every month, almost every week, more than once a week and almost every day), perceived health status (Excellent = excellent. Otherwise = good and fair), life satisfaction (Very happy = very happy. Lower = happy, not very happy and not happy at all), quality of family relationships (Very good = very easy. Lower = easy, difficult and very difficult), quality of peer relationships (Very good = very easy. Lower = easy, difficult and very difficult), academic performance (Very good = very good. Lower = good, average and under average), health complaints index (Never = rarely or never. Sometime = almost every month, almost every week, more than once a week, and almost every day). Sex (i.e. male and female) and age (i.e. children and adolescence) differences across the foregoing variables were analysed by chi-squared test.
The associations of sleep parameters with psychological positive health indicators and health complaints were examined by binary logistic regression analysis in children and adolescents, separately. Based on the findings reported by previous studies suggesting that sleep deprivation might aggravate health-related outcomes [28, 29], sleep-related variables were introduced as independent variables and psychological positive health and health complaints outcomes as dependent variables. All the analyses were performed jointly for boys and girls, and the models were adjusted for sex. Additionally, we included the categorical perceived sleep latency variable as a covariate (using the “enter” method) when studying the associations of reported sleep time with psychological positive health and health complaints (see Table 2). This was done because reported sleep time was calculated as the difference between wake-up time and bedtime, thus including sleep-onset latency.
To assess which sleep variable is possibly the most predictive of psychological positive health and health complaints, multivariate regression was used to test the combined association of sleep variables (reported sleep time, morning tiredness and perceived sleep latency) with each of the dependent variables (i.e. psychological positive health and health complaints) in children and adolescents, separately. The models were adjusted for sex. All statistical analyses were conducted using the Statistical Package for Social Sciences (IBM SPSS Statistics for Windows, version 20.0, Armonk, NY), and the level of significance was set at P < 0.05.
Results
The final study sample consisted of 380 Caucasian children (9.3 ± 1.6, 6–11.9 years) and 304 adolescents (14.8 ± 1.9, 12–17.9 years). The total percentage of male and female participants was 53.3 and 46.7, respectively. Approximately one-third of the participants reported that their parents had university studies. About the 98 % of the children and adolescents fathers were employed, whereas only ~50 % of their mothers were employed and the remaining ~50 % were housekeeper.
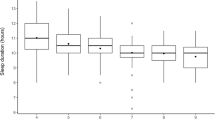
Descriptive characteristics of the study participants by sex and age are shown in Table 1. The mean (SD) total sleep time for children and adolescents were 9.6 (0.6) and 8.8 (0.6) h/day, respectively. Children reported better perceived sleep quality (i.e. less morning tiredness and lower perceived sleep latency) and higher levels of psychological positive health (all P < 0.05) than adolescents, except for quality of peers relationships and health complaints (see Table 1). There were no gender differences in psychological positive health and health complaints in children and adolescents, except for quality of family relationships and health complaints in adolescents. Specifically, adolescent boys reported lower percentages of very good quality of family relationships (68.6 vs. 79.0 %; P = 0.045) and higher percentages of having no health complaints (79.7 vs. 63.4 %; P = 0.002) than adolescent girls.
Total sleep time ≥10 h was significantly associated with an increased likelihood of reporting no health complaints (OR 2.347, 95 % CI 1.301–4.234; P = 0.005) in children (Table 2). Sleep time ≥9 h was significantly associated with an increased likelihood of perceived excellent health status (OR 1.964, 95 % CI 1.214–3.177; P = 0.006), very happy life satisfaction (OR 1.687, 95 % CI 1.020–3.010; P = 0.049), very good quality of family relationships (OR 2.105, 95 % CI 1.224–3.619; P = 0.007) and very good academic performance (OR 1.847, 95 % CI 1.089–3.134; P = 0.023) in adolescents. Sleeping ≥9 h was significantly associated with an increased likelihood of reporting no health complaints (OR 1.702, 95 % CI 1.018–3.021; P = 0.047) in adolescents. We repeated the analysis with the variable sleep time as a continuous variable, and the results did not change and thereby were not reported here.
Children who reported no morning tiredness versus having morning tiredness were more likely to have excellent perceived health status (OR 2.502, 95 % CI 1.644–3.809; P < 0.001), very happy life satisfaction (OR 2.650, 95 % CI 1.692–4.294; P < 0.001), very good quality of family relationships (OR 1.855, 95 % CI 1.710–2.940; P = 0.009) and very good academic performance (OR 1.521, 95 % CI 1.059–2.254; P = 0.039) (Table 3). Additionally, children who reported no morning tiredness versus having morning tiredness were more likely to have no health complaints (OR 2.372, 95 % CI 1.408–3.995; P = 0.001). Adolescents reporting no morning tiredness versus having morning tiredness were more likely to have excellent perceived health status (OR 2.106, 95 % CI 1.271–3.491; P = 0.004), very happy life satisfaction (OR 2.144, 95 % CI 1.286–3.576; P = 0.003), very good quality of family relationships (OR 1.821, 95 % CI 1.145–2.957; P = 0.04) and very good academic performance (OR 2.624, 95 % CI 1.526–4.513; P < 0.001). Furthermore, adolescents reporting no morning tiredness versus having morning tiredness were more likely to have no health complaints (OR 1.825, 95 % CI 1.072–3.070; P = 0.025).
For children, the absence of difficulty falling asleep was associated with an increased likelihood of reporting excellent perceived health status (OR 1.725, 95 % CI 1.101–2.657; P = 0.026) and very good quality of family relationships (OR 1.861, 95 % CI 1.016–2.867; P = 0.047). Additionally, children with no difficulty falling asleep versus difficulty falling asleep were more likely to report no health complaints (OR 3.805, 95 % CI 2.183–6.633; P < 0.001) (Table 4). In adolescents, the absence of difficulty falling asleep was associated with an increased likelihood of reporting excellent perceived health status (OR 1.814, 95 % CI 1.112–2.720; P = 0.008), very happy life satisfaction (OR 2.255, 95 % CI 1.362–3.732; P = 0.002), very good quality of family relationships (OR 1.914, 95 % CI 1.026–3.570; P = 0.041) and very good academic performance (OR 1.705, 95 % CI 1.001–3.044; P = 0.024). Moreover, adolescents who reported no difficulty falling asleep versus difficulty falling sleep were more likely to report no health complaints (OR 3.521, 95 % CI 2.072–5.983; P < 0.001).
The multivariate logistic regression analysis showed that the absence of morning tiredness was the most significant contributor of excellent perceived health status (OR 2.433, 95 % CI 1.581–3.742; P < 0.001), very happy life satisfaction (OR 2.843, 95 % CI 1.754–4.606; P < 0.001), very good quality of family relationships (OR 1.812, 95 % CI 1.142–2.893; P = 0.012) and very good academic performance (OR 1.584, 95 % CI 1.040–2.413; P = 0.032) in children (Table 5). Furthermore, the absence of perceived sleep latency was the most significant contributor of reporting no health complaints (OR 3.704, 95 % CI 2.077–6.605; P < 0.001). The absence of morning tiredness was the most significant contributor of excellent perceived health status (OR 1.979, 95 % CI 1.179–3.322; P < 0.010), very good quality of family relationships (OR 1.798, 95 % CI 1.116–2.862; P = 0.024) and very good academic performance (OR 2.451, 95 % CI 1.408–4.266; P = 0.002) in adolescents (Table 5). Furthermore, the absence of perceived sleep latency was the most significant contributor of very happy life satisfaction (OR 2.241, 95 % CI 1.338–3.753; P = 0.002) and reporting no health complaints (OR 3.527, 95 % CI 2.064–6.028; P < 0.001).
Discussion
The cross-sectional data from the present study demonstrate that both self-reported sleep time and perceived sleep quality are positively associated with positive health indicators and inversely associated with health complaints in children and adolescents. The youth with appropriate total sleep time and/or sleep quality are more likely to report a better psychological positive health and fewer health complaints. This is of clinical relevance since monitoring the sleep time and sleep quality may provide some insights to why children and adolescents could be developing adverse psychological positive health and health complaints issues. To our knowledge, this is the first study assessing the relationship between self-reported sleep duration and quality and psychological positive health or health complaints involving children and adolescents in Spain.
Our data showed that children generally sleep ~1 h more than adolescents, with children and adolescents from the present study sleeping ~10 and ~9 h on average, respectively. Although the “normal” sleep duration is 8–9 h [30], it remains unclear how much sleep is needed for children and adolescents to remain healthy and develop/mature fully. We believe the cut-off value for optimal sleep time for children (>10 h) and adolescents (>9 h) used in this study is reasonable as it is in line with the results found by the National Sleep Foundation 2004 and 2006 polls [23, 24]. Previous studies have shown an age-related decrease in objectively [4, 5] and subjectively assessed [6, 31, 32] total sleep time from childhood to adolescence. According to recent studies, the decline of total sleep time from childhood to adolescence is approximately 10–12 min/year [5, 31] and during adolescence is ~14 min/year [6]. Taking into account that our sample’s mean age was ~9 and ~15 years for children and adolescents, respectively, the observed differences of mean total sleep time matched previous international data [5, 6, 31]. Previous research has suggested that the decline of total sleep time in these age periods is not related to maturation but to other factors such as school demands [4, 6, 31] and a progressively age-related later bedtime [5] due to an increase in media usage prior to sleep onset [6].
Perceived health status can be a strong predictor of future functional limitations, cognitive impairment and mortality [33]. Surprisingly, in the present study, reported sleep time was not associated with perceived health status in children, whereas it was in adolescents, as previously described [2]. Sleep problems (duration and quality) have generally shown to be an important indicator of perceived physical and mental health in the general adult population [34, 35] and young, healthy college students [36]. The cause may be related to sleep deprivation, which has shown a relationship to a reduced immune profile in young adults [28] and an increased risk of an inflammatory-related disease [29]. As noted earlier, previous studies on the topic are focused on objective physical health measures, whereas we studied children and adolescents’ perceived health status. Furthermore, perceived sleep quality was associated with perceived health status in both children and adolescents in the present study. This finding highlights the greater impact of perceived sleep quality on children and adolescents’ health rather than total sleep time [7, 37]. In fact, a good quality of sleep may be an important factor to consider in the prevention of diseases [38, 39].
Life satisfaction is an essential criterion of psychological health [10]. Results of the present study showed an indirect association between morning tiredness and life satisfaction in children. Reported sleep time was directly associated with life satisfaction in adolescents, whereas morning tiredness and perceived sleep latency were indirectly associated with life satisfaction in adolescents. These associations have not been previously investigated in these populations. Previous studies have shown that poor total sleep time results in higher risk of depression in adolescents [40, 41] which can directly lead to greater levels of life dissatisfaction. Specifically, a predictive relationship between poor sleep quality and subsequent incident life dissatisfaction has been previously described in a prospective study with adult twins [42]. It has also been found that the treatment of sleep disorders can result in an increase in life satisfaction in the adult population [43]. However, few studies on this topic involving children and adolescents have been reported. The results of the current study have added to our knowledge about this issue by age.
While it has been well documented that sleep is a direct factor influencing health, it is also a critical contributor to the quality of family relationships. To date, numerous research studies have investigated the link between sleep and quality of family relationships [44, 45]. The results of our study are in line with a wealth of previous studies on sleep and perceived quality of family relationships involving children and adolescents. However, the causal direction of the relationship of the two variables is not clear. For example, recent research in the adult US population has thoroughly studied the link between family relationship characteristics and sleep [46], concluding that family relationships strongly influence quality of sleep. Additionally, it has also been reported that sleep problems change the mood of this population [47], which may affect the quality of family relationships. Most importantly, this bidirectional relationship between sleep and quality of family relationships has recently been found in children and adolescents [40]. Therefore, improving sleep may help children and adolescents develop good relationships with their family members. Future research on how to enhance the quality of sleep is needed.
We hypothesized that peer relationships would show similar associations with sleep outcomes, as those found in family relationships. However, surprisingly, this contention was not supported by the results of the study, as peer relationships was the only variable which was not significantly associated with reported sleep time and/or perceived sleep quality. Close peer relationships can be crucial for children and adolescents’ development since this variable is inversely related to depression [40]. We hypothesize that sleep problems may not be related strongly enough to directly affect the robust established vincula of peer relationships. As far as we know, there are no other studies focused on the association of sleep patterns and peer relationships, which hampers further comparison.
The role of total sleep time in academic performance has been widely studied in children and adolescents [48]. The lack of a significant association between sleep duration and academic performance in children in the present study is contradictory to preliminary research [48, 49]. This finding might be caused by several methodological differences between previous studies [48, 49] and ours (e.g. the assessment method of sleep and school performance). However, morning tiredness was associated with school performance in children in the present study, which concurs with the previous finding [48]. This may be due to sleep duration and quality making different contributions to school performance [38]. However, according to the existing evidence [48], adolescents reporting both small total sleep time and poor perceived sleep quality were more likely to show poorer school performance. This finding might be explained by the essential role of long and intense sleep for the process of learning and memory consolidation [50]. The association of reported sleep time with academic performance in adolescents, but not in children, found by the present study, may be due to the increase in school requirements in this later stage [4, 6, 31], which leads to later bedtimes during adolescence [5, 40, 48]. The data from the current study may also suggest that sleep duration plays a more critical role in academic performance in adolescents than in children.
Despite health complaints and sleep problems having previously been observed in children and adolescents [7, 15, 16], the relationship between them has not yet been extensively analysed. Recent studies have shown that sleep problems and some health complaints, such as headaches, abdominal pain and fatigue, often co-occur [51, 52]. This finding concurs with our results, which showed a high association of both sleep duration and quality with health complaints. Sleep and health complaints share similar associated psychosocial determinants [51]. For instance, sleep fragmentation (night-time awakening) is a consequence of social stressors [53], which in turn may be an important explanatory factor of increased subjective health complaints in adolescents [54]. Interestingly, our data showed that those children and adolescents with no difficulty falling asleep were nearly four times more likely to report no health complaints than those with difficulty falling asleep. Our results suggest that paediatricians, health professionals and caregivers should pay attention to sleep duration and quality since those variables might explain high levels of health complaints in this population.
Overall, our findings show that the associations of sleep with positive health and health complaints were more pronounced in adolescents than in children. Specifically, reported sleep time was more strongly and consistently associated with positive health in adolescents than in children. Adolescence is a maturational stage with several physiological and psychological changes [55]. As previously mentioned, school demands increase during the adolescence period, thus triggering later bedtimes and consequently reducing sleeping hours. Sleep difficulties might therefore strongly affect positive health indicators and health complaints in this specific population. In addition, children might not be able to self-report as accurately as adolescents, which may explain the absence of statistical associations between some of the study sleep variables and psychological positive health indicators.
There are some limitations in the current study, and caution needs to be exercised when generalizing the results to the population. First, the cross-sectional design does not allow us to establish causal relationships. Future experimental studies could more thoroughly examine whether improving the duration and quality of sleep affects the outcome of the variables measured in the present study. We did not assess sleep in weekdays and weekends separately (e.g. which would have allowed us to examine whether sleep deprivations throughout the week are compensated on weekends). Second, we used self-reported data to assess sleep, which might present some limitations: (i) some individuals with cognitive difficulties, different personalities and/or subjective perceptions might be unreliable when self-reporting. This could alter the real relationship between sleep and health observed in the present study. (ii) Self-report measures are not be able to detect sleep as precisely as those using an objective measure. However, sleep data presented in the present study concur with the previous studies using self-report and/or objective measures [4–6, 23, 24]. Furthermore, sleep duration (hours) was calculated as the difference between wake-up time and bedtime; thus, this variable included sleep-onset latency. This might affect the conclusions of the present study because participants with longer perceived sleep latency could appear to sleep a lot when it is not actually the case. To minimize the concomitant effect, the analyses assessing the association of reported sleep time with psychological positive health and health complaints were controlled for perceived sleep latency assessed with the 5-point Likert scale. Similarly, we did not objectively assess academic performance. However, a recent meta-analysis showed that the self-report method is as valid as objective methods for measuring participants’ school performance [48]. Third, the questions used in the present study are included in the HBSC questionnaire, which is a valid and reliable questionnaire in youth aged 10–18 years old [21, 22], whereas our population comprised youth aged 6–18 years old. In addition, trained investigators gave continuous instruction to all participants in order to avoid any kind of confusion, especially with those who were younger.
Alternatively, one strength of the present study was using not only reported sleep time but also qualitative sleep indicators, as suggested previously [7]. Moreover, according to recommendations of a recent study [48], we utilized sleep duration, perceived sleep quality and sleepiness as separate sleep variables. Finally, while a large sample size was used in the present study, this might be not representative of the entire Spanish child and adolescent population. However, the levels of subjective indicators (HBSC items) were similar to nationally representative data obtained from the HBSC survey [56], suggesting that the sample was consistent with those used in the comparative data source.
Conclusions
The present study highlights the close relationship between sleep characteristics (i.e. sleep duration and quality) and psychological positive health and health complaints in children and adolescents from southern Spain. The confluence of these findings suggests that improving both sleep duration and quality could lead to an improvement in psychological positive health and a decrease in health complaints in children and adolescents. Of more importance, sleep duration and quality may play a more important role in student academic performance in adolescents than that in children.
References
Matricciani, L., Blunden, S., Rigney, G., Williams, M. T., & Olds, T. S. (2013). Children’s sleep needs: Is there sufficient evidence to recommend optimal sleep for children? Sleep, 36(4), 527–534.
Chen, M. Y., Wang, E. K., & Jeng, Y. J. (2006). Adequate sleep among adolescents is positively associated with health status and health-related behaviors. BMC Public Health, 6, 59.
Cappuccio, F. P., Taggart, F. M., Kandala, N. B., Currie, A., Peile, E., Stranges, S., et al. (2008). Meta-analysis of short sleep duration and obesity in children and adults. Sleep, 31(5), 619–626.
Ohayon, M. M., Carskadon, M. A., Guilleminault, C., & Vitiello, M. V. (2004). Meta-analysis of quantitative sleep parameters from childhood to old age in healthy individuals: developing normative sleep values across the human lifespan. Sleep, 27(7), 1255–1273.
Feinberg, I., Davis, N. M., de Bie, E., Grimm, K. J., & Campbell, I. G. (2012). The maturational trajectories of NREM and REM sleep durations differ across adolescence on both school-night and extended sleep. American Journal of Physiology: Regulatory, Integrative and Comparative Physiology, 302(5), R533–R540.
Olds, T., Blunden, S., Petkov, J., & Forchino, F. (2010). The relationships between sex, age, geography and time in bed in adolescents: A meta-analysis of data from 23 countries. Sleep Medicine Reviews, 14(6), 371–378.
Jarrin, D. C., McGrath, J. J., & Drake, C. L. (2013). Beyond sleep duration: distinct sleep dimensions are associated with obesity in children and adolescents. International Journal of Obesity, 37(4), 552–558.
Roeser, K., Eichholz, R., Schwerdtle, B., Schlarb, A. A., & Kubler, A. (2012). Relationship of sleep quality and health-related quality of life in adolescents according to self- and proxy ratings: A questionnaire survey. Front Psychiatry, 3, 76.
Narang, I., Manlhiot, C., Davies-Shaw, J., Gibson, D., Chahal, N., Stearne, K., et al. (2012). Sleep disturbance and cardiovascular risk in adolescents. CMAJ, 184(17), E913–E920.
Seligman, M. E. P. (2008). Positive Health. Applied Psychology, 57, 3–18.
Ong, A. D., & van Dulmen, M. H. M. (2007). Oxford handbook of methods in positive psychology. New York: Oxford University Press.
Proulx, C. M., Helms, H. M., & Buehler, C. (2007). Marital quality and personal well-being: A meta-analysis. Journal of Marriage and Family, 69, 576–593.
Ortega, F. B., Lee, D. C., Sui, X., Kubzansky, L. D., Ruiz, J. R., Baruth, M., et al. (2010). Psychological well-being, cardiorespiratory fitness, and long-term survival. American Journal of Preventive Medicine, 39(5), 440–448.
Brown, R. J. (2007). Introduction to the special issue on medically unexplained symptoms: Background and future directions. Clinical Psychology Review, 27(7), 769–780.
Eminson, D. M. (2007). Medically unexplained symptoms in children and adolescents. Clinical Psychology Review, 27(7), 855–871.
Barkmann, C., Braehler, E., Schulte-Markwort, M., & Richterich, A. (2011). Chronic somatic complaints in adolescents: Prevalence, predictive validity of the parent reports, and associations with social class, health status, and psychosocial distress. Social Psychiatry and Psychiatric Epidemiology, 46(10), 1003–1011.
Mikkelsson, M., Salminen, J. J., & Kautiainen, H. (1997). Non-specific musculoskeletal pain in preadolescents. Prevalence and 1-year persistence. Pain, 73(1), 29–35.
Rocha, E. M., Prkachin, K. M., Beaumont, S. L., Hardy, C. L., & Zumbo, B. D. (2003). Pain reactivity and somatization in kindergarten-age children. Journal of Pediatric Psychology, 28(1), 47–57.
Balaguer, I. (2002). Estilos de vida en la adolescencia. Valencia: Promolibro.
Wold, B. (1995). Health-behavior in schoolchildren: A WHO cross-national survey. Resource package questions 1993–94. Bergen: University of Bergen.
Currie, C., Roberts, C., Morgan, A., Smith, R., Settertobulte, W., Samdal, O., et al. (2004). Young people’s health in context. Health Behaviour in School-aged Children (HBSC) study: international report from the 2001/2002 survey. WHO Policy Series: Health policy for children and adolescents Issue 4 Copenhagen: WHO Regional Office for Europe.
Roberts, C., Freeman, J., Samdal, O., Schnohr, C. W., de Looze, M. E., Nic Gabhainn, S., et al. (2009). The Health Behaviour in School-aged Children (HBSC) study: Methodological developments and current tensions. International Journal of Public Health, 54(Suppl 2), 140–150.
National Sleep Foundation. 2004 Sleep in America Poll: Children and Sleep. (2004). from http://www.sleepfoundation.org/.
National Sleep Foundation. 2006 Sleep in America Poll: Teens and Sleep. (2006). from http://www.sleepfoundation.org/.
Garralda, M. E. (1996). Somatisation in children. Journal of Child Psychology and Psychiatry, 37(1), 13–33.
Iannotti, R. J., Janssen, I., Haug, E., Kololo, H., Annaheim, B., & Borraccino, A. (2009). Interrelationships of adolescent physical activity, screen-based sedentary behaviour, and social and psychological health. International Journal of Public Health, 54(Suppl 2), 191–198.
Haugland, S., Wold, B., Stevenson, J., Aaroe, L. E., & Woynarowska, B. (2001). Subjective health complaints in adolescence. A cross-national comparison of prevalence and dimensionality. European Journal of Public Health, 11(1), 4–10.
Ozturk, L., Pelin, Z., Karadeniz, D., Kaynak, H., Cakar, L., & Gozukirmizi, E. (1999). Effects of 48 h sleep deprivation on human immune profile. Sleep Research Online, 2(4), 107–111.
Irwin, M. R., Wang, M., Ribeiro, D., Cho, H. J., Olmstead, R., Breen, E. C., et al. (2008). Sleep loss activates cellular inflammatory signaling. Biological Psychiatry, 64(6), 538–540.
Pepin, J. L., Borel, A. L., Tamisier, R., Baguet, J. P., Levy, P., & Dauvilliers, Y. (2014). Hypertension and sleep: Overview of a tight relationship. Sleep Med Rev.
Olds, T., Maher, C., Blunden, S., & Matricciani, L. (2010). Normative data on the sleep habits of Australian children and adolescents. Sleep, 33(10), 1381–1388.
Williams, J. A., Zimmerman, F. J., & Bell, J. F. (2013). Norms and trends of sleep time among US children and adolescents. JAMA Pediatrics, 167(1), 55–60.
van der Linde, R. M., Mavaddat, N., Luben, R., Brayne, C., Simmons, R. K., Khaw, K. T., et al. (2013). Self-rated health and cardiovascular disease incidence: results from a longitudinal population-based cohort in Norfolk, UK. PLoS ONE, 8(6), e65290.
Furihata, R., Uchiyama, M., Takahashi, S., Suzuki, M., Konno, C., Osaki, K., et al. (2012). The association between sleep problems and perceived health status: A Japanese nationwide general population survey. Sleep Medicine, 13(7), 831–837.
Shankar, A., Charumathi, S., & Kalidindi, S. (2011). Sleep duration and self-rated health: The national health interview survey 2008. Sleep, 34(9), 1173–1177.
Pilcher, J. J., & Ott, E. S. (1998). The relationships between sleep and measures of health and well-being in college students: A repeated measures approach. Behavioral Medicine, 23(4), 170–178.
Gupta, N. K., Mueller, W. H., Chan, W., & Meininger, J. C. (2002). Is obesity associated with poor sleep quality in adolescents? American Journal of Human Biology, 14(6), 762–768.
Pilcher, J. J., Ginter, D. R., & Sadowsky, B. (1997). Sleep quality versus sleep quantity: Relationships between sleep and measures of health, well-being and sleepiness in college students. Journal of Psychosomatic Research, 42(6), 583–596.
Lee, A. J., & Lin, W. H. (2007). Association between sleep quality and physical fitness in female young adults. Journal of Sports Medicine and Physical Fitness, 47(4), 462–467.
Lin, J. D., Tung, H. J., Hsieh, Y. H., & Lin, F. G. (2011). Interactive effects of delayed bedtime and family-associated factors on depression in elementary school children. Research in Developmental Disabilities, 32(6), 2036–2044.
Fredriksen, K., Rhodes, J., Reddy, R., & Way, N. (2004). Sleepless in Chicago: Tracking the effects of adolescent sleep loss during the middle school years. Child Development, 75(1), 84–95.
Paunio, T., Korhonen, T., Hublin, C., Partinen, M., Kivimaki, M., Koskenvuo, M., et al. (2009). Longitudinal study on poor sleep and life dissatisfaction in a nationwide cohort of twins. American Journal of Epidemiology, 169(2), 206–213.
Hossain, N. K., Irvine, J., Ritvo, P., Driver, H. S., & Shapiro, C. M. (2007). Evaluation and treatment of sleep complaints: Patients’ subjective responses. Psychotherapy and Psychosomatics, 76(6), 395–399.
Kalak, N., Gerber, M., Kirov, R., Mikoteit, T., Puhse, U., Holsboer-Trachsler, E., et al. (2012). The relation of objective sleep patterns, depressive symptoms, and sleep disturbances in adolescent children and their parents: A sleep-EEG study with 47 families. Journal of Psychiatric Research, 46(10), 1374–1382.
Lemola, S., Schwarz, B., & Siffert, A. (2012). Interparental conflict and early adolescents’ aggression: is irregular sleep a vulnerability factor? Journal of Adolescence, 35(1), 97–105.
Ailshire, J. A., & Burgard, S. A. (2012). Family relationships and troubled sleep among U.S. adults: Examining the influences of contact frequency and relationship quality. Journal of Health and Social Behavior, 53(2), 248–262.
Ong, S. H., Wickramaratne, P., Tang, M., & Weissman, M. M. (2006). Early childhood sleep and eating problems as predictors of adolescent and adult mood and anxiety disorders. Journal of Affective Disorders, 96(1–2), 1–8.
Dewald, J. F., Meijer, A. M., Oort, F. J., Kerkhof, G. A., & Bogels, S. M. (2010). The influence of sleep quality, sleep duration and sleepiness on school performance in children and adolescents: A meta-analytic review. Sleep Medicine Reviews, 14(3), 179–189.
Gruber, R., Laviolette, R., Deluca, P., Monson, E., Cornish, K., & Carrier, J. (2010). Short sleep duration is associated with poor performance on IQ measures in healthy school-age children. Sleep Medicine, 11(3), 289–294.
Wilhelm, I., Prehn-Kristensen, A., & Born, J. (2012). Sleep-dependent memory consolidation–what can be learnt from children? Neuroscience and Biobehavioral Reviews, 36(7), 1718–1728.
Luntamo, T., Sourander, A., Rihko, M., Aromaa, M., Helenius, H., Koskelainen, M., et al. (2012). Psychosocial determinants of headache, abdominal pain, and sleep problems in a community sample of Finnish adolescents. European Child and Adolescent Psychiatry, 21(6), 301–313.
Luntamo, T., Sourander, A., Santalahti, P., Aromaa, M., & Helenius, H. (2012). Prevalence changes of pain, sleep problems and fatigue among 8-year-old children: Years 1989, 1999, and 2005. Journal of Pediatric Psychology, 37(3), 307–318.
Pereira, D., & Elfering, A. (2014). Social stressors at work, sleep quality and psychosomatic health complaints: A longitudinal ambulatory field study. Stress Health, 30(1), 43–52.
Wiklund, M., Malmgren-Olsson, E. B., Ohman, A., Bergstrom, E., & Fjellman-Wiklund, A. (2012). Subjective health complaints in older adolescents are related to perceived stress, anxiety and gender: A cross-sectional school study in Northern Sweden. BMC Public Health, 12, 993.
Brooks-Gunn, J., Petersen, A. C., & Eichorn, D. (1985). The study of maturational timing effects in adolescence. Journal of Youth and Adolescence, 14(3), 149–161.
Moreno, C., Muñoz-Tinoco, V., Pérez, P., Sánchez-Queija, I., M.C., G., Ramos, P., et al. (2008). Desarrollo adolescente y salud. Resultados del Estudio HBSC-2006 con chicos y chicas españoles de 11 a 17 años.: Madrid: Ministerio de Sanidad y Consumo. Edición electrónica.
Acknowledgments
This study was funded by Centro Andaluz de Medicina del Deporte, Junta de Andalucía, Orden 4/02/05, BOJA No 37 (REF. JA-CTD2005-01), the Spanish Ministry of Education (AP-2010-0963) and the Spanish Ministry of Science and Innovation (RYC-2010-05957). We thank Dr. Marilla D. Svinicki at the University of Texas at Austin, TX, USA, for her help in editing the writing of the manuscript.
Conflict of interests
Authors declare no conflict of interests.
Ethical standard
A comprehensive verbal description of the nature and purpose of the study was given to the children, adolescents, their parents and teachers. This information was also sent to parents or children supervisors by regular mail, and written consents from parents, children and adolescents were requested. The study was approved by the Review Committee for Research Involving Human Subjects at the University of Cádiz, Spain.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Segura-Jiménez, V., Carbonell-Baeza, A., Keating, X.D. et al. Association of sleep patterns with psychological positive health and health complaints in children and adolescents. Qual Life Res 24, 885–895 (2015). https://doi.org/10.1007/s11136-014-0827-0
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11136-014-0827-0