
Abstract
Repetitive transcranial magnetic stimulation (rTMS) is increasingly used as a therapeutic intervention for neuropsychiatric illnesses and has demonstrated efficacy for treatment of major depression. However, an unresolved question is whether a course of rTMS treatment results in effects on cognitive functioning. In this systematic review and meta-analysis we aimed to quantitatively determine whether a course of rTMS has cognitive enhancing effects. We examined cognitive outcomes from randomised, sham-controlled studies conducted in patients with neuropsychiatric conditions where rTMS was administered to the dorsolateral prefrontal cortex (DLPFC) across repeated sessions, searched from PubMed/MEDLINE and other databases up until October 2015. Thirty studies met our inclusion criteria. Cognitive outcomes were pooled and examined across the following domains: Global cognitive function, executive function, attention, working memory, processing speed, visual memory, verbal memory and visuospatial ability. Active rTMS treatment was unassociated with generalised gains across the majority of domains of cognitive functioning examined. Secondary analyses revealed a moderate sized positive effect for improved working memory in a small number of studies in patients with schizophrenia (k = 3, g = 0.507, 95 % CI = [0.183–0.831], p < .01). Therapeutic rTMS when administered to the DLPFC in patients with neuropsychiatric conditions does not result in robust cognitive enhancing effects.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
Introduction
Since the advent of transcranial magnetic stimulation (TMS) in the mid 1990s, non-invasive brain stimulation methodologies have rapidly evolved to become both established neuroscientific tools for the investigation of brain functioning and innovative therapeutic approaches for a number of difficult- to- treat neuropsychiatric conditions. TMS involves the passing of strong, focal, time- varying magnetic pulses through the skull into underlying cortex, in which eddy currents are generated, depolarising neurons via electromagnetic induction. The technological development of TMS to allow for the delivery of multiple repeated strong magnetic pulses into the brain (i.e., repetitive transcranial magnetic stimulation (rTMS)) has proven to be a major advancement for neuropsychiatry, with rTMS now considered an efficacious and safe treatment option, particularly for patients with major depression (Lefaucheur et al. 2014). Despite its increasing clinical use, however, an unresolved question is if a course of rTMS treatment additionally results in effects on cognitive functioning. Thus, in this systematic review and meta-analysis we aimed to quantitatively determine whether a course of rTMS, given to the prefrontal cortex for treatment of neuropsychiatric disorders, has cognitive enhancing effects.
rTMS when given therapeutically for neuropsychiatric disorders is most commonly administered to the prefrontal cortex, specifically the dorsolateral prefrontal cortex (DLPFC), as this region is known to be structurally and functionally dysfunctional in a number of neuropsychiatric conditions, including major depression (Grimm et al. 2008; Khundakar et al. 2009) and schizophrenia (Meyer-Lindenberg et al. 2002; Weickert et al. 2009). Abnormal functioning in this region is considered to subserve poorer cognitive function in these conditions on tests of working memory (Marquand et al. 2008; Chen et al. 2014) and executive function (Harvey et al. 2004). rTMS stimulation administered in daily treatments over at least 2 weeks to either the left or right DLPFC has been shown to have antidepressant effects (O’Reardon et al. 2007; George et al. 2010; Berlim et al. 2013b, 2014). These effects are associated with structural changes through increased grey matter volumes in depression affected regions (Lan et al. 2016). Based on these positive findings in depression, therapeutic rTMS administered in a similar manner has additionally been explored in a number of other neuropsychiatric conditions, including schizophrenia (e.g., Wobrock et al. 2015) and obsessive compulsive disorder (OCD) (e.g., Sachdev et al. 2007), albeit with mixed results (Berlim et al. 2013a; Dougall et al. 2015). Whilst the mechanisms underlying therapeutic effects remains unclear, it is generally considered that these may result from cumulative functional changes within directly stimulated regions (e.g., increased regional cerebral blood flow, neurotransmitter levels; Noda et al. 2015) and/or changes in interconnected brain regions (e.g. Lan et al. 2016).
Interestingly, a single session of rTMS has been demonstrated to have acute cognitive enhancing effects. For example, high frequency rTMS when administered to task-related cortical regions immediately prior to task performance has been shown to improve response inhibition (Vanderhasselt et al. 2006), mental rotation (Klimesch et al. 2003) and confrontation naming (Cappa et al. 2002). These acute effects are consistent with regional cerebral blood flow increases shown during high frequency stimulation (Loo et al. 2003b) and increases in prefrontal gamma oscillatory activity immediately following stimulation (Barr et al. 2009). Proposed mechanisms for these site- specific cognitive enhancing effects have included neuronal priming, driving of oscillatory activity, and synaptic neuroplastic changes (Luber and Lisanby 2014). Given that the site of stimulation (i.e., DLPFC) frequently used for therapeutic rTMS is known to subserve multiple higher level cognitive functions including executive function, learning and memory, and working memory, and that repeated daily administration to this same region over several weeks has proven therapeutic effects, the possibility of cognitive enhancement following repeated rTMS administration remains an open question. Recent systematic reviews conducted in both mixed (Guse et al. 2010) and depressed samples (Serafini et al., 2015) indeed have suggested that rTMS has promising cognitive enhancing effects.
In the current systematic review and meta-analysis we aimed to delineate quantitatively whether rTMS treatment as typically applied therapeutically has cognitive enhancing effects. We chose to examine effects across domains of cognitive function, both to determine whether rTMS treatment has effects on particular cognitive abilities and to allow for collation of outcomes from different tests that measure the same abilities. The evidence evaluated was limited to randomised, sham- controlled clinical trials where rTMS was administered to the prefrontal cortex for the treatment of neuropsychiatric conditions, as it is in these clinical populations where the therapeutic use of rTMS has been most rigorously examined. Effects of repeated treatments over an acute treatment course were examined based on assessments performed before and at the end of the acute treatment period. We hypothesised that repeated rTMS administration to the prefrontal cortex would cause generalised improvement in fronto-executive cognitive abilities (i.e., executive function, working memory) subserved by the DLPFC.
Methods
We performed a systematic review and meta-analysis in accordance with the PRISMA guidelines (Liberati et al. 2009). A literature search was conducted in the following databases: Pubmed/MEDLINE, EMBASE (Ovid) and PsychINFO (Ovid). Articles were searched from the year 1995 (i.e., the first published pilot study of rTMS for depression (Kolbinger et al. 1995)) until 29 October 2015. The search terms were: ‘repetitive transcranial magnetic stimulation’ OR ‘rTMS’, AND ‘neurocognition’ OR ‘neurocognitive performance’ OR ‘cognitive effects’ OR ‘cognitive’ OR ‘neuropsychological’, AND ‘randomized controlled trial’ OR ‘randomised controlled trial’) OR ‘controlled clinical trial’ OR ‘RCT’ OR ‘sham controlled’. These specific search terms were chosen to be broad enough to capture studies of rTMS conducted in clinical populations, regardless of diagnosis or site of stimulation, and specific enough to limit results to randomised controlled trials where cognitive outcomes were examined. Further, the bibliographies of published systematic reviews of the cognitive effects of rTMS were searched for additional studies (i.e., Guse et al. 2010; Dougall et al. 2015; Serafini et al. 2015), and we contacted study authors as needed to attain additional data. Results were limited to studies in humans and those published in English language.
Selection Criteria
Studies were required to meet the following inclusion criteria: 1) the study was conducted to examine rTMS treatment in a neuropsychiatric population; 2) the study involved the administration of multiple (at least 2) repeated stimulation sessions 3) the stimulation was administered only to the prefrontal cortex, and 4) sham stimulation was used as a comparator. Exclusion criteria were: 1) the therapeutic intervention targeted a primary neurodegenerative or neurological condition, substance use or personality disorder, 2) rTMS treatment was administered with concurrent training or during completion of any other task, and 3) stimulation was administered to a different region other than the prefrontal cortex. Included studies must also have used standardised cognitive test(s) with established psychometric properties, and reported post-acute treatment results (mean, SD, and Ns per condition).
Data Extraction
Following retrieval of studies, all review articles, conference abstracts and duplicates were removed. The title and abstracts for each study were then screened against the selection criteria by two authors (DM and JF). Full texts were screened in cases where the title and abstract provided insufficient information. All discrepancies were resolved by consensus. Where studies met all other inclusion criteria, but provided insufficient detail for reported outcomes, the corresponding authors were contacted to obtain missing data. Further, where multiple outcomes from the same cognitive test were reported (e.g., accuracy and reaction time), only the results from one outcome were analysed (see Table 1 for a description of all outcomes included in the analysis). The following additional study data were further extracted from included studies: neuropsychiatric condition, sample sizes for the active and sham conditions, frequency of stimulation sessions, site of stimulation (left, right or bilateral DLPFC), number of sessions, rTMS frequency, number of pulses/session, whether pharmacological treatment resistance was an inclusion criterion, age of participants in each condition, gender, duration of current illness, and other/comorbid diagnoses. All data were extracted by a single author (DM). Where studies included two active conditions, results from both active conditions were averaged and compared to sham for analysis. This was done in accordance with the analysis assumption for fixed effects models that the effect sizes would not vary according to rTMS stimulus parameters or other differences between studies. If standard errors were reported, standard deviations for outcome measures were calculated using the eq. SD = SE x √N.
Statistical Analysis
The standardised mean difference (Hedge’s g) was calculated for each outcome measure to minimise bias from small sample sizes (Deeks and Higgins 2010). Positive effect sizes indicated an advantage for the active stimulation condition. Scores for reaction times and errors were recoded such that a positive result indicated superior performance for the active treatment condition. Where multiple outcomes representing the same cognitive domain were reported from an individual study, or outcomes were reported from more than one active condition, the average of the respective effect sizes was calculated. Effect sizes were calculated to evaluate treatment effects of the following cognitive domains: global cognitive function, executive function, attention, working memory, processing speed, visual memory, verbal memory and visuospatial ability. For n back tasks, 0 and 1 back outcomes were analysed in the attention domain, and 2 and 3 back outcomes were analysed in the working memory domain, consistent with prior research showing that higher difficulty n back conditions are analogous to other working memory tasks (Haatveit et al. 2010). We analysed only cognitive domains where outcomes were available from at least three different studies. Effect sizes were adjusted for small sample bias through the inverse variance method and weighted and pooled using fixed effects models. Fixed effects models were chosen a priori so as to determine whether rTMS has effects on specific particular cognitive abilities from stimulating similar neurocircuitry across neuropsychiatric conditions, the high similarity between studies for the intervention in question (i.e., rTMS dose was individually titrated using similar methodologies, rTMS was focally administered to the left or right dorsolateral prefrontal cortex and administered daily over consecutive days) and to maximise statistical power. Due to possible heterogeneity in the fixed effects models, results for the main analyses were also repeated using random effects models. Homogeneity of each weighted effect size was tested using the Q statistic. Where pooled weighted effect sizes reached statistical significance according to the Z statistic (p < .05), secondary exploratory analyses examined weighted effect sizes for specific neuropsychiatric diagnoses where sufficient data were available. This variable was chosen for sub-group analysis based on differences in therapeutic efficacy for rTMS treatment between clinical conditions despite use of similar treatment parameters (see Table 2). Publication bias was examined using funnel plots and the Egger’s test, and we used Review Manager software (version 5.3.5 for Macintosh) to assess risk of bias in randomised trials following published recommendations (Higgins et al. 2011). Analyses were conducted using SAS/STAT software Version 9.4 (SAS Institute Inc., Cary, NC).
Results
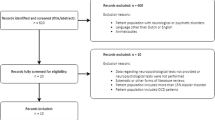
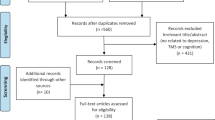
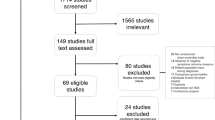
Our search criteria identified 351 references. Following removal of duplicates, reviews, and conference abstracts, this left 264 references for title/abstract review. Additional data was subsequently received from seven studies. Figure 1 summarises the search and selection process. A total of 30 studies were included in the quantitative analysis. Of the included studies, 18 were conducted in depressed patients, 8 in patients with schizophrenia, 2 in patients with posttraumatic stress disorder (PTSD), 1 in patients with obsessive compulsive disorder (OCD), and 1 in patients with panic disorder (PD). rTMS was administered at least once daily in every study (range 5–30 sessions). Twenty three studies involved administration of high frequency (5-30 Hz) LDLPFC rTMS, 2 involved low frequency (1 Hz) RDLPFC rTMS, and 7 involved bilateral DLPFC rTMS stimulation. A description of the treatment characteristics of the studies included in the analysis is outlined in Table 2.

Flowchart of search and study selection process
Patient Characteristics
Table 3 shows the clinical and patient characteristics of the included studies. Across all studies, the mean age of participants across conditions ranged from 27 to 67 years and illness duration ranged from 0.4 to 41 years. For studies conducted in depressed patients, 10 of 18 studies were conducted in patients with treatment resistant depression. The mean duration of the current depressive episode across studies ranged from 0.35 to 8.5 years. Nine of 18 studies included patients with bipolar disorder, 2 studies included patients with Parkinson’s disease, and 1 study included patients with stroke. For the studies in patients with schizophrenia, illness duration ranged from 7.5 to 25 years. Two of 8 studies included patients with schizoaffective disorder. For studies in patients with PTSD, illness duration ranged from 3.4 to 41 years. Single studies were included which examined effects in patients with OCD and PD/Agoraphobia.
Quality Assessment
The quality of each included study was assessed using the Cochrane Collaboration’s tool for assessing risk of bias in randomised trials (Higgins et al. 2011). In brief, the Cochrane Collaboration’s risk of bias assessment tool assesses five specific types of study biases including, selection bias (random sequence generation, allocation concealment), performance bias (blinding of participants and study personnel), detection bias (blinding of outcome assessment), attrition bias (incomplete outcome data), and reporting bias (selective outcome reporting) (Higgins and Green 2008) The majority of studies had a low risk bias across most standard criteria including random sequence generation, blinding of participants, blinding outcome assessment, and incomplete outcome data. However, most studies had an unclear risk of bias for allocation concealment, and as expected based on published recommendations (Higgins et al. 2011), all studies showed unclear risk of bias for selective reporting of results (see Fig. 2).

Summary plot showing assessment of risk of bias
Cognitive Domains
Global Cognitive Function
From 10 studies, outcomes from four measures of global cognitive function were extracted for analysis and included 314 participants. Results showed no difference in global cognitive test performance following acute active or sham rTMS treatment (see Fig. 3). This result remained unchanged using a random effects model.

Forest plots for effects of rTMS on global cognitive function, executive function and attention
Executive Function
From 25 studies, results from 15 different outcomes were analysed, which included a total of 768 participants. Results showed no difference in executive function performance following acute active or sham rTMS treatment (see Fig. 3). This result remained unchanged using a random effects model.
Attention
From 12 studies, results from 5 different outcomes were analysed, with the analysis comprising 475 patients. Results showed no difference in attention performance following acute active or sham rTMS treatment (see Fig. 3). This result remained unchanged using a random effects model.
Processing Speed
A total of 20 studies were included in the analysis with 7 different outcomes compiled from a total of 641 participants. There was no difference in processing speed performance between the active and sham rTMS conditions (see Fig. 4). This result remained unchanged using a random effects model.

Forest plots for effects of rTMS on processing speed, visual memory, verbal memory and visuospatial ability
Visual Memory
Outcomes were analysed from 3 studies that included 2 different outcome measures and 84 participants. Results showed no visual memory performance difference between active and sham rTMS (see Fig. 4). This result remained unchanged using a random effects model.
Verbal Memory
Fourteen studies were included with outcomes analysed from 6 different outcome measures, with a total of 285 participants. There was no verbal memory performance difference between active and sham rTMS (see Fig. 4). This result remained unchanged using a random effects model.
Visuospatial Ability
Three studies were included which used three different outcome measures and had a total of 94 participants. Results showed no visuospatial ability performance differences between active and sham rTMS (see Fig. 4). This result remained unchanged using a random effects model.
Working Memory
From 13 studies, outcomes from 5 measures comprising 460 participants were analysed. These results showed a statistically significant advantage for active rTMS compared to sham for improvement in working memory performance (see Fig. 5.). This effect was at trend level statistical significance using a random effects model (g = 0.208, 95 % CI = [−0.030–0.446], p = 0.09). Figure 6 shows the funnel plot for the effect sizes reported from the individual studies, which due to asymmetry, indicated potential risk of publication bias. This was not supported, however, by the results of the Egger’s test (p = 0.43). Secondary analyses conducted to examine specific effects in studies with depressed participants showed that by only including studies in patients with depression, the advantage of active rTMS was no longer significant (k = 9, g = 0.087, 95 % CI = [−0.154–0.328], p = 0.48). However, for results of studies conducted only in patients with schizophrenia (k = 3, g = 0.507, 95 % CI = [0.183–0.831], p < 0.01) there was a moderate sized effect favouring active rTMS relative to sham (see Fig. 5). This effect remained statistically significant when this analysis was repeated excluding the study by Guse et al. (2013), as this study included the same participants as the Hasan et al. (2015) study (i.e., k = 2, g = 0.458, 95 % CI = [0.105–0.811], p = 0.01).

Forest plots of effects of rTMS on working memory

Funnel plot for working memory outcomes
Discussion
To the best of our knowledge, this is the first meta-analysis to quantitatively assess whether an acute course of therapeutic rTMS administered to the prefrontal cortex has cognitive enhancing effects in patients with neuropsychiatric conditions. The majority of studies included in this meta-analysis showed a low risk of bias across most risk criteria as outlined by the Cochrane Collaboration (Higgins et al. 2011). Across the majority of cognitive domains analysed, results showed no overall effect of active rTMS treatment for enhancing cognition, with the exception of a small sized effect for improvement in working memory. Secondary exploratory analyses revealed that this advantage was specific to a small number of studies in patients with schizophrenia.
While robust therapeutic effects of rTMS have been demonstrated, particularly for major depression, it has remained an open question in the field whether treatment has concomitant cognitive enhancing effects. Unfortunately, the current findings from aggregated data extracted from 30 controlled clinical trials showed no overall effect for active rTMS compared to sham across the majority of cognitive domains tested, including executive functioning, attention, and verbal memory, cognitive abilities known to be subserved by the stimulated brain region (i.e., DLPFC). These results therefore have two main implications: first, that repeated rTMS treatment does not cause generalised upregulation of DLPFC functioning, and second, that any potential cognitive enhancing changes due to rTMS may be neuropsychiatric disorder or ability/task specific.
The DLPFC is known to be integral to multiple executive functions, including verbal generativity (Gaillard et al. 2000), set-shifting (Moll et al. 2002) and response inhibition (Vanderhasselt et al. 2006), as well as working (Cabeza and Nyberg 2000; Mull and Seyal 2001) and verbal memory (Nikolin et al. 2015). These cognitive abilities were examined by the majority of the studies included in this current meta-analysis. The failure to find a generalised cognitive enhancing effect across any of these specific cognitive domains is therefore suggestive that repeated rTMS administration does not cause broader upregulation of DLPFC functioning. This finding may have potential important implications for the understanding of the mechanisms underlying rTMS’s therapeutic effects, which remain poorly understood. Specifically, rTMS’s therapeutic mechanisms (e.g., antidepressant effects) may be independent to broader cognitive changes. This finding is consistent with the results from a retrospective analysis of four rTMS studies in depressed patients which similarly found a dissociation between cognitive and therapeutic outcomes; namely, that cognitive changes across the full treatment course were not associated with therapeutic effects, however, early cognitive changes in visual memory during the treatment course predicted subsequent therapeutic outcomes (Hoy et al. 2012). Therefore, whilst there appears to be a direct lack of association between cognitive and therapeutic outcomes, the possibility that rTMS related cognitive enhancement occurs across a separate time-course independent of therapeutic effects cannot be ruled out at this stage. Further, over the last decade it has become increasingly recognised that accurate targeting of rTMS within the DLPFC is critical for therapeutic efficacy, particularly for treatment of depression (Fitzgerald et al. 2009; Fox et al. 2012; Herbsman et al. 2009; Johnson et al. 2013). Functional neuroimaging research has further identified specific subregions of the DLPFC to be parts of functionally distinct distributed connected networks, including the frontoparietal and default mode networks (Yeo et al. 2011; Opitz et al. 2015), which highlights the potential importance for regional specificity and accurate rTMS targeting. Thus, given the importance of rTMS targeting within the DLPFC in relation to therapeutic outcomes, the potential for associations with more highly specific cognitive abilities or functions that are regionally and/or network specific (e.g., emotion regulation functions of the DLPFC) also remains a possibility.
Interestingly, the only domain where a significant cognitive enhancing effect was found was for working memory, with this advantage found only in a small number of studies in patients with schizophrenia. In contrast to depression, trait cognitive deficits in patients with schizophrenia are known to be far more robust with large- sized generalised deficits apparent from onset of illness, with worse deficits in the domains of verbal memory and processing speed (Mesholam-Gately et al. 2009; Schaefer et al. 2013). Neuroimaging studies have similarly implicated dysfunction in specific dorsal and ventral regions related to poorer verbal memory functioning (Ragland et al. 2009; Rimol et al. 2010; Ragland et al. 2015). For working memory specifically, rTMS stimulation when administered to the LDLPFC during task performance in healthy participants (i.e., in an inhibitory paradigm) impaired performance (Mull and Seyal 2001), implicating an important functional role of this region. Conversely, rTMS administered immediately prior to performance in an intermittent theta-burst pattern, a modified rTMS approach that involves the application of very high frequency rTMS (i.e., 50 Hz) in an excitatory paradigm, improved performance post stimulation in healthy volunteers (Hoy et al. 2015). Similar performance enhancing effects on working memory were additionally seen with stimulation applied during task performance in a healthy sample using transcranial direct current (tDCS) (Nikolin et al. 2015), another facilitatory non-invasive brain stimulation method demonstrated to have cognitive enhancing effects (Brunoni and Vanderhasselt 2014; Coffman et al. 2014). The current finding of a positive effect of multiple rTMS sessions for enhancing working memory performance in patients with schizophrenia therefore suggests potential benefits of repeated stimulation sessions when applied to this clinical population. Future studies are required to replicate this finding.
Limitations to the current analysis include that data from different cognitive tests were aggregated for analysis for each cognitive domain (e.g., executive functioning), which may have limited specificity for the examination of cognitive effects, and that effects were examined across studies which included different neuropsychiatric populations using heterogeneous rTMS parameters and stimulation site targeting methodologies. Nevertheless, despite this potential heterogeneity in outcomes and studies, we note that effect sizes between studies were homogenous, the tests for heterogeneity were negative, and that there was no evidence found for publication risk bias. Furthermore, the effect of heterogeneity would be to reduce power to detect positive findings and our primary aim was to investigate robust effects across commonly accepted cognitive domains which nonetheless are more likely to be evident using fixed effects models. Other limitations include the inclusion of a small number of studies conducted in patients with OCD, PTSD, and PD which potentially precluded the potential to conduct sub-group analyses in these populations, and that included articles were restricted to those written in the English language.
In conclusion, the results from this first quantitative meta-analytic examination of the cognitive effects of therapeutic rTMS from a large number of randomised controlled clinical trials found no robust effect of active rTMS across multiple different cognitive domains. However, an isolated positive effect was observed for improved working memory performance in a small number of studies conducted in patients with schizophrenia, indicating the possibility for specificity of effects in this clinical population. Future controlled studies are required to replicate this effect before rTMS to improve cognition in this population is recommended as a clinical treatment. Future research is further required to determine whether rTMS treatment has more highly specific cognitive effects (e.g., for specific executive abilities, or on specific tasks).
References
Avery, D. H., Claypoole, K., Robinson, L., Neumaier, J. F., Dunner, D. L., Scheele, L., et al. (1999). Repetitive transcranial magnetic stimulation in the treatment of medication-resistant depression: preliminary data. The Journal of Nervous and Mental Disease, 187(2), 114–117.
Barr, M. S., Farzan, F., Rusjan, P. M., Chen, R., Fitzgerald, P. B., & Daskalakis, Z. J. (2009). Potentiation of gamma oscillatory activity through repetitive transcranial magnetic stimulation of the dorsolateral prefrontal cortex. Neuropsychopharmacology, 34(11), 2359–2367.
Barr, M. S., Farzan, F., Rajji, T. K., Voineskos, A. N., Blumberger, D. M., Arenovich, T., et al. (2013). Can repetitive magnetic stimulation improve cognition in schizophrenia? Pilot data from a randomized controlled trial. Biological Psychiatry, 73(6), 510–517.
Berlim, M. T., Neufeld, N. H., & Van den Eynde, F. (2013a). Repetitive transcranial magnetic stimulation (rTMS) for obsessive-compulsive disorder (OCD): an exploratory meta-analysis of randomized and sham-controlled trials. Journal of Psychiatric Research, 47(8), 999–1006.
Berlim, M. T., Van den Eynde, F., & Jeff Daskalakis, Z. (2013b). Clinically meaningful efficacy and acceptability of low-frequency repetitive transcranial magnetic stimulation (rTMS) for treating primary major depression: a meta-analysis of randomized, double-blind and sham-controlled trials. Neuropsychopharmacology, 38(4), 543–551.
Berlim, M. T., van den Eynde, F., Tovar-Perdomo, S., & Daskalakis, Z. J. (2014). Response, remission and drop-out rates following high-frequency repetitive transcranial magnetic stimulation (rTMS) for treating major depression: a systematic review and meta-analysis of randomized, double-blind and sham-controlled trials. Psychological Medicine, 44(2), 225–239.
Blumberger, D. M., Mulsant, B. H., Fitzgerald, P. B., Rajji, T. K., Ravindran, A. V., Young, L. T., et al. (2012). A randomized double-blind sham-controlled comparison of unilateral and bilateral repetitive transcranial magnetic stimulation for treatment-resistant major depression. The World Journal of Biological Psychiatry, 13(6), 423–435.
Boggio, P. S., Fregni, F., Bermpohl, F., Mansur, C. G., Rosa, M., Rumi, D. O., et al. (2005). Effect of repetitive TMS and fluoxetine on cognitive function in patients with Parkinson's disease and concurrent depression. Movement Disorders, 20(9), 1178–1184.
Boggio, P. S., Rocha, M., Oliveira, M. O., Fecteau, S., Cohen, R. B., Campanha, C., et al. (2010). Noninvasive brain stimulation with high-frequency and low-intensity repetitive transcranial magnetic stimulation treatment for posttraumatic stress disorder. The Journal of Clinical Psychiatry, 71(8), 992–999.
Brunoni, A. R., & Vanderhasselt, M. A. (2014). Working memory improvement with non-invasive brain stimulation of the dorsolateral prefrontal cortex: a systematic review and meta-analysis. Brain and Cognition, 86, 1–9.
Cabeza, R., & Nyberg, L. (2000). Imaging cognition II: An empirical review of 275 PET and fMRI studies. Journal of Cognitive Neuroscience, 12(1), 1–47.
Cappa, S. F., Sandrini, M., Rossini, P. M., Sosta, K., & Miniussi, C. (2002). The role of the left frontal lobe in action naming: rTMS evidence. Neurology, 59(5), 720–723.
Chen, C. M., Stanford, A. D., Mao, X., Abi-Dargham, A., Shungu, D. C., Lisanby, S. H., et al. (2014). GABA level, gamma oscillation, and working memory performance in schizophrenia. Neuroimage Clinic, 4, 531–539.
Coffman, B. A., Clark, V. P., & Parasuraman, R. (2014). Battery powered thought: enhancement of attention, learning, and memory in healthy adults using transcranial direct current stimulation. NeuroImage, 85(Pt 3), 895–908.
Deeks, J.J., & Higgins, J.P.T. 2010. Statistical algorithms in Review Manager 5. Retrieved from http://ims.cochrane.org/revman/documentation/Statistical-methods-in-RevMan-5.pdf
Deppermann, S., Vennewald, N., Diemer, J., Sickinger, S., Haeussinger, F. B., Notzon, S., et al. (2014). Does rTMS alter neurocognitive functioning in patients with panic disorder/agoraphobia? An fNIRS-based investigation of prefrontal activation during a cognitive task and its modulation via sham-controlled rTMS. Biomed Research International, 2014, 542526.
Dlabac-de Lange, J. J., Bais, L., van Es, F. D., Visser, B. G. J., Reinink, E., Bakker, B., et al. (2015a). Efficacy of bilateral repetitive transcranial magnetic stimulation for negative symptoms of schizophrenia: results of a multicenter double-blind randomized controlled trial. Psychological Medicine, 45(6), 1263–1275.
Dlabac-de Lange, J. J., Liemburg, E. J., Bais, L., Renken, R. J., Knegtering, H., & Aleman, A. (2015b). Effect of rTMS on brain activation in schizophrenia with negative symptoms: A proof-of-principle study. Schizophrenia Research, 168(1–2), 475–482.
Dougall, N., Maayan, N., Soares-Weiser, K., McDermott, L. M., & McIntosh, A. (2015). Transcranial magnetic stimulation (TMS) for schizophrenia. Cochrane Database of Systematic Reviews, 8, CD006081. doi:10.1002/14651858.CD006081.pub2.
Fitzgerald, P. B., Herring, S., Hoy, K., McQueen, S., Segrave, R., Kulkarni, J., et al. (2008). A study of the effectiveness of bilateral transcranial magnetic stimulation in the treatment of the negative symptoms of schizophrenia. Brain Stimulation, 1(1), 27–32.
Fitzgerald, P. B., Hoy, K., McQueen, S., Maller, J. J., Herring, S., Segrave, R., et al. (2009). A randomized trial of rTMS targeted with MRI based neuro-navigation in treatment-resistant depression. Neuropsychopharmacology, 34(5), 1255–1262.
Fox, M. D., Buckner, R. L., White, M. P., Greicius, M. D., & Pascual-Leone, A. (2012). Efficacy of transcranial magnetic stimulation targets for depression is related to intrinsic functional connectivity with the subgenual cingulate. Biological Psychiatry, 72(7), 595–603.
Gaillard, W. D., Hertz-Pannier, L., Mott, S. H., Barnett, A. S., LeBihan, D., & Theodore, W. H. (2000). Functional anatomy of cognitive development: fMRI of verbal fluency in children and adults. Neurology, 54(1), 180–185.
George, M. S., Lisanby, S. H., Avery, D., McDonald, W. M., Durkalski, V., Pavlicova, M., et al. (2010). Daily left prefrontal transcranial magnetic stimulation therapy for major depressive disorder: a sham-controlled randomized trial. Archives of General Psychiatry, 67(5), 507–516.
Grimm, S., Beck, J., Schuepbach, D., Hell, D., Boesiger, P., Bermpohl, F., et al. (2008). Imbalance between left and right dorsolateral prefrontal cortex in major depression is linked to negative emotional judgment: an fMRI study in severe major depressive disorder. Biological Psychiatry, 63(4), 369–376.
Guse, B., Falkai, P., Gruber, O., Whalley, H., Gibson, L., Hasan, A., et al. (2013). The effect of long-term high frequency repetitive transcranial magnetic stimulation on working memory in schizophrenia and healthy controls--a randomized placebo-controlled, double-blind fMRI study. Behavioural Brain Research, 237, 300–307.
Guse, B., Falkai, P., & Wobrock, T. (2010). Cognitive effects of high-frequency repetitive transcranial magnetic stimulation: a systematic review. Journal of Neural Transmission (Vienna), 117(1), 105–122.
Haatveit, B. C., Sundet, K., Hugdahl, K., Ueland, T., Melle, I., & Andreassen, O. A. (2010). The validity of d prime as a working memory index: Results from the “Bergen n-back task”. Journal of Clinical and Experimental Neuropsychology, 32(8), 871–880.
Harvey, P. O., Le Bastard, G., Pochon, J. B., Levy, R., Allilaire, J. F., Dubois, B., & Fossati, P. (2004). Executive functions and updating of the contents of working memory in unipolar depression. Journal of Psychiatric Research, 38(6), 567–576.
Hasan, A., Guse, B., Cordes, J., Wolwer, W., Winterer, G., Gaebel, et al. (2015). Cognitive Effects of High-Frequency rTMS in Schizophrenia Patients With Predominant Negative Symptoms: Results From a Multicenter Randomized Sham-Controlled Trial. Schizophr Bull. doi: 10.1093/schbul/sbv142
Hausmann, A., Pascual-Leone, A., Kemmler, G., Rupp, C. I., Lechner-Schoner, T., Kramer-Reinstadler, K., et al. (2004). No deterioration of cognitive performance in an aggressive unilateral and bilateral antidepressant rTMS add-on trial. The Journal of Clinical Psychiatry, 65(6), 772–782.
Herbsman, T., Avery, D., Ramsey, D., Holtzheimer, P., Wadjik, C., Hardaway, F., et al. (2009). More lateral and anterior prefrontal coil location is associated with better repetitive transcranial magnetic stimulation antidepressant response. Biological Psychiatry, 66(5), 509–515.
Higgins, J. P., Altman, D. G., Gotzsche, P. C., Juni, P., Moher, D., Oxman, A. D., et al. (2011). The Cochrane Collaboration's tool for assessing risk of bias in randomised trials. BMJ, 343, d5928.
Higgins, J. P. T., & Green, S. (2008). Assessing risk of bias in included studies. In J. P. T. Higgins & S. Green (Eds.), Cochrane Handbook for Systematic Reviews of Interventions (pp. 197–241). Chichester (UK): John Wiley & Sons.
Holtzheimer 3rd, P. E., Russo, J., Claypoole, K. H., Roy-Byrne, P., & Avery, D. H. (2004). Shorter duration of depressive episode may predict response to repetitive transcranial magnetic stimulation. Depression and Anxiety, 19(1), 24–30.
Hoy, K. E., Bailey, N., Michael, M., Fitzgibbon, B., Rogasch, N. C., Saeki, T., et al. (2015). Enhancement of Working Memory and Task-Related Oscillatory Activity Following Intermittent Theta Burst Stimulation in Healthy Controls. Cerebral Cortex. doi:10.1093/cercor/bhv193.
Hoy, K. E., Segrave, R. A., Daskalakis, Z. J., & Fitzgerald, P. B. (2012). Investigating the relationship between cognitive change and antidepressant response following rTMS: a large scale retrospective study. Brain Stimulation, 5(4), 539–546.
Huang, M. L., Luo, B. Y., Hu, J. B., Wang, S. S., Zhou, W. H., Wei, N., et al. (2012). Repetitive transcranial magnetic stimulation in combination with citalopram in young patients with first-episode major depressive disorder: a double-blind, randomized, sham-controlled trial. The Australian and New Zealand Journal of Psychiatry, 46(3), 257–264.
Johnson, K. A., Baig, M., Ramsey, D., Lisanby, S. H., Avery, D., McDonald, W. M., et al. (2013). Prefrontal rTMS for treating depression: location and intensity results from the OPT-TMS multi-site clinical trial. Brain Stimulation, 6(2), 108–117.
Jorge, R. E., Robinson, R. G., Tateno, A., Narushima, K., Acion, L., Moser, D., et al. (2004). Repetitive transcranial magnetic stimulation as treatment of poststroke depression: a preliminary study. Biological Psychiatry, 55(4), 398–405.
Khundakar, A., Morris, C., Oakley, A., McMeekin, W., & Thomas, A. J. (2009). Morphometric analysis of neuronal and glial cell pathology in the dorsolateral prefrontal cortex in late-life depression. The British Journal of Psychiatry, 195(2), 163–169.
Klimesch, W., Sauseng, P., & Gerloff, C. (2003). Enhancing cognitive performance with repetitive transcranial magnetic stimulation at human individual alpha frequency. The European Journal of Neuroscience, 17(5), 1129–1133.
Kolbinger, H., Koflich, G., Hufnagel, A., Moller, H., & Kasper, S. (1995). Transcranial magnetic stimulation (TMS) in treatment of major depression: A pilot study. Human Psychopharmacology, 10, 305–310.
Lan, M. J., Chhetry, B. T., Liston, C., Mann, J. J., & Dubin, M. (2016). Transcranial Magnetic Stimulation of Left Dorsolateral Prefrontal Cortex Induces Brain Morphological Changes in Regions Associated with a Treatment Resistant Major Depressive Episode: An Exploratory Analysis. Brain Stimul. doi:10.1016/j.brs.2016.02.011
Lefaucheur, J. P., Andre-Obadia, N., Antal, A., Ayache, S. S., Baeken, C., Benninger, D. H., et al. (2014). Evidence-based guidelines on the therapeutic use of repetitive transcranial magnetic stimulation (rTMS. Clinical Neurophysiology, 125(11), 2150–2206.
Liberati, A., Altman, D. G., Tetzlaff, J., Mulrow, C., Gotzsche, P. C., Ioannidis, J. P., et al. (2009). The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: explanation and elaboration. BMJ, 339, b2700.
Loo, C., Sachdev, P., Elsayed, H., McDarmont, B., Mitchell, P., Wilkinson, M., et al. (2001). Effects of a 2- to 4-week course of repetitive transcranial magnetic stimulation (rTMS) on neuropsychologic functioning, electroencephalogram, and auditory threshold in depressed patients. Biological Psychiatry, 49(7), 615–623.
Loo, C. K., Mitchell, P. B., Croker, V. M., Malhi, G. S., Wen, W., Gandevia, S. C., et al. (2003a). Double-blind controlled investigation of bilateral prefrontal transcranial magnetic stimulation for the treatment of resistant major depression. Psychological Medicine, 33(1), 33–40.
Loo, C. K., Sachdev, P. S., Haindl, W., Wen, W., Mitchell, P. B., Croker, V. M., et al. (2003b). High (15 Hz) and low (1 Hz) frequency transcranial magnetic stimulation have different acute effects on regional cerebral blood flow in depressed patients. Psychological Medicine, 33(6), 997–1006.
Loo, C. K., Mitchell, P. B., McFarquhar, T. F., Malhi, G. S., & Sachdev, P. S. (2007). A sham-controlled trial of the efficacy and safety of twice-daily rTMS in major depression. Psychological Medicine, 37(3), 341–349.
Luber, B., & Lisanby, S. H. (2014). Enhancement of human cognitive performance using transcranial magnetic stimulation (TMS). NeuroImage, 85(Pt 3), 961–970.
Marquand, A. F., Mourao-Miranda, J., Brammer, M. J., Cleare, A. J., & Fu, C. H. (2008). Neuroanatomy of verbal working memory as a diagnostic biomarker for depression. Neuroreport, 19(15), 1507–1511.
McDonald, W. M., Easley, K., Byrd, E. H., Holtzheimer, P., Tuohy, S., Woodard, J. L., et al. (2006). Combination rapid transcranial magnetic stimulation in treatment refractory depression. Neuropsychiatric Disease and Treatment, 2(1), 85–94.
Mesholam-Gately, R. I., Giuliano, A. J., Goff, K. P., Faraone, S. V., & Seidman, L. J. (2009). Neurocognition in first-episode schizophrenia: a meta-analytic review. Neuropsychology, 23(3), 315–336.
Meyer-Lindenberg, A., Miletich, R. S., Kohn, P. D., Esposito, G., Carson, R. E., Quarantelli, M., et al. (2002). Reduced prefrontal activity predicts exaggerated striatal dopaminergic function in schizophrenia. Nature Neuroscience, 5(3), 267–271.
Mogg, A., Pluck, G., Eranti, S. V., Landau, S., Purvis, R., Brown, R. G., et al. (2008). A randomized controlled trial with 4-month follow-up of adjunctive repetitive transcranial magnetic stimulation of the left prefrontal cortex for depression. Psychological Medicine, 38(3), 323–333.
Mogg, A., Purvis, R., Eranti, S., Contell, F., Taylor, J. P., Nicholson, T., et al. (2007). Repetitive transcranial magnetic stimulation for negative symptoms of schizophrenia: a randomized controlled pilot study. Schizophrenia Research, 93(1–3), 221–228.
Moser, D. J., Jorge, R. E., Manes, F., Paradiso, S., Benjamin, M. L., & Robinson, R. G. (2002). Improved executive functioning following repetitive transcranial magnetic stimulation. Neurology, 58(8), 1288–1290.
Mosimann, U. P., Schmitt, W., Greenberg, B. D., Kosel, M., Muri, R. M., Berkhoff, M., et al. (2004). Repetitive transcranial magnetic stimulation: a putative add-on treatment for major depression in elderly patients. Psychiatry Research, 126(2), 123–133.
Moll, J., de Oliveira-Souza, R., Moll, F. T., Bramati, I. E., & Andreiuolo, P. A. (2002). The cerebral correlates of set-shifting: an fMRI study of the trail making test. Arquivos de Neuro-Psiquiatria, 60(4), 900–905.
Mull, B. R., & Seyal, M. (2001). Transcranial magnetic stimulation of left prefrontal cortex impairs working memory. Clinical Neurophysiology, 112(9), 1672–1675.
Myczkowski, M. L., Dias, A. M., Luvisotto, T., Arnaut, D., Bellini, B. B., Mansur, C. G., et al. (2012). Effects of repetitive transcranial magnetic stimulation on clinical, social, and cognitive performance in postpartum depression. Neuropsychiatric Disease and Treatment, 8, 491–500.
Nadeau, S. E., Bowers, D., Jones, T. L., Wu, S. S., Triggs, W. J., & Heilman, K. M. (2014). Cognitive effects of treatment of depression with repetitive transcranial magnetic stimulation. Cognitive and Behavioral Neurology, 27(2), 77–87.
Nikolin, S., Loo, C. K., Bai, S., Dokos, S., & Martin, D. M. (2015). Focalised stimulation using high definition transcranial direct current stimulation (HD-tDCS) to investigate declarative verbal learning and memory functioning. NeuroImage, 117, 11–19.
Noda, Y., Silverstein, W. K., Barr, M. S., Vila-Rodriguez, F., Downar, J., Rajji, T., et al. (2015). Neurobiological mechanisms of repetitive transcranial magnetic stimulation of the dorsolateral prefrontal cortex in depression: a systematic review. Psychological Medicine, 45, 3411–3432.
Opitz, A., Fox, M. D., Craddock, R. C., Colcombe, S., & Milham, M. P. (2015). An integrated framework for targeting functional networks via transcranial magnetic stimulation. NeuroImage. doi:10.1016/j.neuroimage.2015.11.040.
O’Reardon, J. P., Solvason, H. B., Janicak, P. G., Sampson, S., Isenberg, K. E., Nahas, Z., et al. (2007). Efficacy and safety of transcranial magnetic stimulation in the acute treatment of major depression: a multisite randomized controlled trial. Biological Psychiatry, 62(11), 1208–1216.
Pal, E., Nagy, F., Aschermann, Z., Balazs, E., & Kovacs, N. (2010). The impact of left prefrontal repetitive transcranial magnetic stimulation on depression in Parkinson's disease: a randomized, double-blind, placebo-controlled study. Movement Disorders, 25(14), 2311–2317.
Ragland, J. D., Laird, A. R., Ranganath, C., Blumenfeld, R. S., Gonzales, S. M., & Glahn, D. C. (2009). Prefrontal activation deficits during episodic memory in schizophrenia. The American Journal of Psychiatry, 166(8), 863–874.
Ragland, J. D., Ranganath, C., Phillips, J., Boudewyn, M. A., Kring, A. M., Lesh, T. A., et al. (2015). Cognitive control of episodic memory in schizophrenia: differential role of dorsolateral and ventrolateral prefrontal cortex. Frontiers in Human Neuroscience, 9, 604.
Rimol, L. M., Hartberg, C. B., Nesvag, R., Fennema-Notestine, C., Hagler, D. J., Jr., Pung, C. J., et al. (2010). Cortical thickness and subcortical volumes in schizophrenia and bipolar disorder. Biological Psychiatry, 68(1), 41–50.
Rollnik, J. D., Huber, T. J., Mogk, H., Siggelkow, S., Kropp, S., Dengler, R., et al. (2000). High frequency repetitive transcranial magnetic stimulation (rTMS) of the dorsolateral prefrontal cortex in schizophrenic patients. Neuroreport, 11(18), 4013–4015.
Sachdev, P. S., Loo, C. K., Mitchell, P. B., McFarquhar, T. F., & Malhi, G. S. (2007). Repetitive transcranial magnetic stimulation for the treatment of obsessive compulsive disorder: a double-blind controlled investigation. Psychological Medicine, 37(11), 1645–1649.
Schaefer, J., Giangrande, E., Weinberger, D. R., & Dickinson, D. (2013). The global cognitive impairment in schizophrenia: consistent over decades and around the world. Schizophrenia Research, 150(1), 42–50.
Serafini, G., Pompili, M., Belvederi Murri, M., Respino, M., Ghio, L., Girardi, P., et al. (2015). The effects of repetitive transcranial magnetic stimulation on cognitive performance in treatment-resistant depression. A systematic review. Neuropsychobiology, 71(3), 125–139.
Vanderhasselt, M. A., De Raedt, R., Baeken, C., Leyman, L., & D'Haenen, H. (2006). The influence of rTMS over the left dorsolateral prefrontal cortex on Stroop task performance. Experimental Brain Research, 169(2), 279–282.
Wajdik, C., Claypoole, K. H., Fawaz, W., Holtzheimer, P. E., 3rd, Neumaier, J., Dunner, D. L., et al. (2014). No change in neuropsychological functioning after receiving repetitive transcranial magnetic stimulation treatment for major depression. The Journal of ECT, 30(4), 320–324.
Watts, B. V., Landon, B., Groft, A., & Young-Xu, Y. (2012). A sham controlled study of repetitive transcranial magnetic stimulation for posttraumatic stress disorder. Brain Stimulation, 5(1), 38–43.
Weickert, T. W., Goldberg, T. E., Callicott, J. H., Chen, Q., Apud, J. A., Das, S., et al. (2009). Neural correlates of probabilistic category learning in patients with schizophrenia. The Journal of Neuroscience, 29(4), 1244–1254.
Wobrock, T., Guse, B., Cordes, J., Wolwer, W., Winterer, G., Gaebel, W., et al. (2015). Left prefrontal high-frequency repetitive transcranial magnetic stimulation for the treatment of schizophrenia with predominant negative symptoms: a sham-controlled, randomized multicenter trial. Biological Psychiatry, 77(11), 979–988.
Yeo, B. T., Krienen, F. M., Sepulcre, J., Sabuncu, M. R., Lashkari, D., Hollinshead, M., et al. (2011). The organization of the human cerebral cortex estimated by intrinsic functional connectivity. Journal of Neurophysiology, 106(3), 1125–1165.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
Author Martin declares that he has no conflict of interest. Author McClintock has received research support from the NIH/NIMH (K23 MH087739) and has received honoraria for teaching from TMS Health Solutions. Author Forster declares that she has no conflict of interest. Author Loo has received equipment on loan from the Neuronetics company.
Ethical Approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed Consent
Informed consent was obtained from all individual participants included in studies conducted by the authors.
Rights and permissions
About this article

Cite this article
Martin, D.M., McClintock, S.M., Forster, J. et al. Does Therapeutic Repetitive Transcranial Magnetic Stimulation Cause Cognitive Enhancing Effects in Patients with Neuropsychiatric Conditions? A Systematic Review and Meta-Analysis of Randomised Controlled Trials. Neuropsychol Rev 26, 295–309 (2016). https://doi.org/10.1007/s11065-016-9325-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11065-016-9325-1