
Abstract
Purpose
To analyse whether the WHO grade of intracranial meningiomas differs itself depending on patients and meningioma characteristics at diagnosis.
Methods
Single center retrospective study of a series of consecutive patients with primary intracranial meningiomas who underwent surgery between January 2007 and March 2014. Patients (age, sex, outcome) and meningioma characteristics (histological diagnosis, tumor location, WHO grading, size, extend of peritumoral edema and tumor recurrence rate) were analysed.
Results
Of 240 included patients, 184 (76.7%) were female and 56 (23.3%) were male. 17 patients (7.1%) were in age group 20–40 years, 112 (46.7%) in group 41–60 years and 111 (46.3%) were in age group > 60 years. 189 patients (78.8%) were diagnosed with WHO grade I, 49 (20.4%) WHO grade II and 2 (0.8%) had a WHO grade III meningioma. WHO grade II meningiomas were significantly more frequent in the age group 20–40 years compared to age group 41–60 years (chi-square p < 0.05). Convexity meningiomas were significantly more frequent classified as WHO grade II meningiomas compared to all other locations (chi-square, p < 0.01). Mean calculated tumor volume and the tumor volume determined by volumetric measurement was significantly larger in grade II meningioma patients compared to grade I (46.3 ± 40.5 cc grade II versus 21.8 ± 27.8 cc grade I and 45.3 ± 38.2 cc versus 23.1 ± 30.0 cc respectively; t test < 0.01). Extend of the peritumoral edema was significantly larger in patients with grade II meningiomas (Wilcoxon test, p < 0.05). Short term outcome did not differ between different age groups nor was it associated with tumor size. During a mean follow up of 49 months (min 3, max 144 months) recurrence rate was significantly higher in WHO grade II (4 out of 49 [8.2]%) compared to WHO grade I patients (3 out if 186, [1.6%]; Chi-square, p < 0.05).
Conclusion
In this series atypical meningioma was associated with younger age, location on the convexity, larger tumor size and more peritumoral edema.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Meningiomas are usually slow growing extra-axial brain tumors deriving from arachnoid cap cells. They are the most frequently diagnosed benign primary brain tumor accounting for 33.8% of all primary brain and central nervous system tumors reported in the United States between 2002 and 2006 [1]. Prevalence rates for meningiomas range from 50.4/100,000 [2] to 70.7/100,000 [3, 4]. Meningiomas can occur at many sites which render them amenable to microsurgical removal. Complete resection of the tumor and the dural attachment still is the primary goal of treatment. However, eloquent location and/ or encasement of critical neurovascular structures preclude complete resection without severely compromising functional outcome. For petroclival meningiomas [5, 6] and meningiomas with involvement of the cavernous sinus [7, 8], this has led to a more conservative surgical strategy with intended partial or subtotal resection to improve patient´s functional outcome and quality of life [9].
The most common meningiomas are WHO grade I and have a low risk of recurrence. However, atypical meningiomas classified as WHO grade II exhibit increased mitotic activity and have a higher recurrence rate (up to 40% at 5 years) [10-14]. Anaplastic meningiomas are malignant tumors (WHO grade III) with a very high rate of recurrence and the 5 year progression free survival (PFS) is only 10% [15]. Since the 2007 WHO classification system has included brain invasion as a controversial feature for the diagnosis of atypical meningiomas the reported incidence of atypical meningioma increased from 7 to 20–30%, due to reclassifying of grade I cases as grade II meningiomas [10, 16-19]. Unfortunately no imaging criteria are accepted to preoperatively differentiate between different WHO grades of intracranial meningiomas. Thus uncertainty persists regarding which patient’s should be operated on early versus followed with MR imaging.
Thus, beside patient related factors, meningioma size, location, extent of peritumoral edema, the assumed extent of resection and the potential surgical morbidity have implications for patients counselling, as well as patient’s management and outcome. Therefore the aim of this analysis was to investigate the relationship of patient´s age, meningioma location, extent of peritumoral edema and size with WHO grade and potential risk factors for tumor recurrence.
Material and methods
Study design
This is a retrospective, single center observational surgical case series, performed in a tertiary referral center. The study was approved by the local ethics committee (Nr.22748/2018/6). Data of all patients who underwent craniotomy for microsurgical resection of an intracranial meningioma were retrieved from an electronic database. From January 2007 to March 2014, 240 consecutive patients with a newly diagnosed intracranial meningioma were included. Patients with Neurofibromatosis Type II or a previous operation of the same meningioma were excluded. In 1 patient, who was operated on 2 different intracranial meningiomas, each surgery was assessed separately.
Demographic data were retrieved from the hospital´s medical record system. Age, sex, and clinical symptoms at the time of diagnosis were recorded in a database. Operative notes were screened for resection status and classified according to the Simpson classification [20]. All preoperative MRI´s were re-evaluated for assessment of tumor location, size and extent of edema. Peritumoral edema was classified as no edema (absence of increased T2 signal surrounding the meningioma), mild edema (rim or crescent of increased T2 signal surrounding the meningioma without mass effect), moderate edema (more extensive increased T2 signal surrounding the meningioma without mass effect) and severe edema (mass effect from edema and/or tongues of advancing edema) [21, 22]. In a few patients, where MRI was not available edema was assessed on CT scans.
Tumor volume was calculated using the formula AxBxC/2 at the largest dimension. In 172 patients thin sliced contrasted enhanced CT (35 patients) and MRI-scans (137 patients) were available for volumetric analysis using the BrainLab neuronavigation software iPlan cranial 3.0 (Brainlab, Munich, Germany). Contrast enhanced tumor was manually segmented after loading the preoperative imaging into iPlan cranial 3.0 navigation software.
All perioperative complications were documented. Outcome was assessed using the mRS at discharge and the latest follow up.
Patients had their first follow up 3 months after surgery and were referred to our outpatient department. Further control intervals were selected with regard to meningioma resection status, WHO grade and the short term clinical course of the patient. For data collection the most recent follow up where patients had a full clinical and radiological evaluation was assessed. During all follow- up visits a standard contrast enhanced MRI/ (in patients with contraindications for MRI a contrast enhanced CT scan) was available and the clinical course was documented. In cases of suspected or obvious recurrent tumor or growth of residual tumor, an interdisciplinary case discussion was initiated in a certified neurooncological tumor board. The decision about further treatment options (reoperation or radiotherapy) depended on the recommendation of this tumor board.
Histological investigations were performed at the Department of Neuropathology by one neuropathologist (MB) according to a standardized protocol. Classification was done according to the WHO 2007 classification system based on paraffin embedded tumor sections stained for hematoxylin–eosin (HE) and using immunohistochemical stainings for epithelial membrane antigen (EMA), progesterone receptors, somatostatin receptors (SSTR2A), mitosis-specific antibody anti-phosphohistone-H3 (pHH-3) and Ki-67 (VENTANA BenchMark ULTRA, Roche).
Surgical treatment
All patients were treated according to standard microsurgical principles. Surgery was performed by all staff members of the Department of Neurosurgery. Frameless neuronavigation (BrainLab®, München) was applied according to the surgeon´s preference. The CUSA was used to debulk the tumors internally, facilitating dissection from the surrounding structures without damage.
Statistical analysis
Statistical analysis was performed using SPSS software version 25.0 (Chicago, USA). Patients were categorized into 3 age groups (20–40 years, 41–60 years and > 60). The Chi-square test and T-test were used to compare categorical variables and the Mann–Whitney U-test, or Wilcoxon Test were employed when the sample sizes were small or the data did not approximate a normal distribution. Correlation of calculated tumor volume to the volumetric determined volume was done using a bivariate correlation analysis. For the conducted analysis, p values less than 0.05 were considered to be statistically significant.
Results
Between 2007 and 2014, 240 patient (184 [76.7%] female and 56 [23.3%] male) were surgically treated. The mean age was 59.0 ± 12.8 years (Table 1).
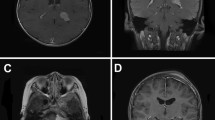
Table 2 depicts the different locations of meningiomas with regard to their histological grading. Histology revealed grade I meningioma in 189 (78.8%) cases, grade II in 49 (20.4%) and grade III in 2 (0.8%), respectively. Histological grading did not differ between male and female patients (Chi-square, p = 0.06). Compared to all other locations, convexity meningiomas were significantly more frequent classified as WHO grade II (Chi-square, < 0.01, Fig. 1).

Compared to all other locations, convexity meningiomas were significantly more frequently classified as WHO grade II (*p < 0.01)
17 patients (7.1% were in the age group 20–40 years, 112 patients (46.7%) in the age group 41–60 years and 111 (46.3%) in the group > 60 years, respectively. Regarding the distribution in age groups, no statistical difference between male and female patients was found. We found 11 (64.7%) WHO grade I and 6 (35.3%) WHO grade II meningiomas in the younger age group (20–40 years). In the group 41–60 years 96 patients (85.7%) had WHO grade I, 16 (14.3%) had grade II tumors and none suffered from WHO grade III meningioma. In the group of patients > 60 years 82 patients (73.9%), 27 (24.3%) and 2 (1.8%) had a WHO grade I, grade II and grade III meningioma, respectively. Thus, WHO grade II meningioma patients were significantly more frequent in the younger age group (20–40 years) compared to the group 41–60 years (Chi-square, p < 0.05) (Fig. 2). However no significant difference was found between groups 41–60 years and > 60 years or 20–40 years and > 60 years.

WHO grade II and III meningioma patients were significantly more frequent in the young age group (20–40 years) compared to age group 41–60 years (p < 0.05). No difference was found between the groups 41–60 years and > 60 years or 20–40 years and > 60 years
Tumor volume was assessed using 2 different approaches. Calculations to approximate the tumor volume was correlated to the volumetric assessed tumor volume and showed a significant correlation (Pearson correlation coefficient 0.95). Mean calculated tumor volume was significantly larger in grade II meningiomas (46.3 ± 40.5 cc) compared to grade I meningiomas (21.8 ± 27.8 cc, t test < 0.01). Data sets for volumetric analysis were available for 42 patients with grade II meningiomas and 84 patients with grade I meningiomas and confirmed the significant larger tumor volume in grade II meningiomas (45.3 ± 38.2 cc) compared to 23.1 ± 30.0 cc (t test < 0.01). No statistical difference of the tumor volume was found between grade I and grade III and grade II and grade III meningiomas (Fig. 3). Peritumoral edema was significantly larger in patients with grade II and III meningiomas compared to grade I meningiomas (Mann Whitney U test, p < 0.01).

Tumor volume was significantly larger in grade II meningioma patients compared to grade I meningiomas (*p < 0.01). No statistical difference of the tumor volume was found between grade I and grade III and grade II and grade III meningiomas
Microsurgical resection was assessed using Simpson grading; we achieved grade 1 in 96 patients (40.0%), grade 2 in 99 patients (41.3%), grade 3 in 25 patients (10.4%) grade 4 in 16 patients (6.7%), and grade 5 in 4 patients (1.7%). Therefore a gross total resection (Simson grade 1–3) was achieved in 220 patients (91.7%). Simpson grade 1 resection was significantly less frequently in patients with WHO II meningioma (p < 0.05) compared to grade I meningioma patients. Resection rate differed neither between age groups (Chi-square, p = 0.4) nor between males and females (U, p = 0.5).
Short term (3 months) outcome showed improved clinical status in 62.5%, while 30% of patients were unchanged and 7.5% worsened. Complication rate did not differ between groups (tumor size, Simpson resection).
224 patients were available for a mean follow up of 49.5 ± 31.7 months (Min 3, Max 144). In 27 patients (11.2%) residual tumor was seen on follow up MRI at 3 months (4 [100%] patients with Simpson 5, 16 [100%] with Simpson 4, 7 [87%] of Simpson 3 and none in Simpson grade 2 and 1 patients, respectively).
Further treatment was indicated in all patients with Simpson grade 5 resection (3 patients with fSRT, 1 patient with RS), in 12 with grade 4 resection (7 patients with fSRT, 5 patients with RS (3 patients were only followed and 1 patients was lost to follow up)) Table 3. 5 patients underwent reoperation after progression of the residual tumor was seen (3 patients before fSRT, 1 patient before RS and 1 patient after fSRT). 2 patients underwent intentional second surgery before RS using a different approach both were Simpson grade 5 resection during their first surgery. Mean time to fSRT was 11.6 months (min 1, max 45) and the mean dose was 55.5 Gy (Table 4). for patients who underwent RS the mean interval was 24.4 months and the dose was 15.7 Gy. 1 patient with WHO grade III meningioma underwent immediate postoperative fSTR.
7 patients (2.9%) presented with recurrent tumors at either the convexity (n = 3), the posterior fossa, sphenoid wing, the tentorium and at the frontal skull base (n = 1, respectively). Recurrence rate was significantly higher in WHO grade II (4 out of 49 [8.2]%) compared to WHO grade I patients (3 out if 186, [1.6%]; Chi-square, p < 0.05). No association was found between age groups and recurrent tumor (U, p = 0.46)). 3 patients underwent fSRT (mean 55.3 Gy) after 16 months (min 10, max 20) and 4 patients underwent RS (mean 14.75 Gy) after 27 months (min 5, max 48).
Discussion
Meningiomas are the most common benign intracranial tumors [1]. Despite the facts that patients with these tumors are frequently treated in neurosurgical units and that there is an extensive body of literature, evidence-based treatment recommendations are scarcer than for malignant intrinsic brain tumors. Recently, current guidelines for the diagnosis and treatment of meningiomas have been summarised by the EANO [23].
Meningiomas are frequently diagnosed incidently and up to date no reliable clinical or imaging biomarker is available to identify atypical meningioma or anaplastic variants prior to surgery. Radiographic findings, including brain invasion, bone invasion, tumor necrosis and peritumoral edema in the surrounding brain, have been found to be associated with higher-grade meningiomas [21, 24] However, no clear decision-making criteria are accepted for patient counselling, especially in patients with asymptomatic meningiomas. We have analysed a retrospective cohort of patients with intracranial meningiomas to identify patient-related factors like sex, age, size, and meningioma location as well as atypical or malignant histopathological features that would possibly be associated with a higher risk for recurrence. The vast majority of meningiomas have a benign behaviour, but atypical and malignant meningiomas comprise a small fraction. Following the 2007 update of the WHO classification of brain tumors these variants are more frequently diagnosed based on histopathological criteria [10]. In our study the overall rate of atypical meningioma and malignant meningiomas was 20.4% and 2.1%, respectively. This is in accordance with other larger series [10, 25].
A review published by Jenkinson et al. [10] summarized that atypical meningiomas do not show any predilection for specific anatomical sites, and that their distribution is similar to grade I meningiomas, with the majority occurring in the parasagittal/falx (~25%), convexity (~19%) and sphenoid wing (~17%). Recently, Sade et al. reported that skull base meningiomas have a fourfold decreased risk of being atypical or malignant as compared with nonskull base tumors [26], although some of them may also have an aggressive growth pattern, which may require extensive resection [27]. Other studies, however, controversially indicated, that atypical and malignant meningiomas are more frequently found at the convexity [21, 25, 28]. By analysing MRI features and locations of intracranial meningiomas Hale et al. found, that location along the falx and convexity was predictive for atypical meningioma [21].
There are 4 important findings in our study. The first major finding is, that convexity meningiomas were significantly more frequent classified as WHO grade II. The skull convexity is known to represents one of the most frequent meningioma locations [29, 30]. The majority of patients having convexity meningiomas can undergo complete resection (Simpson Grade 1 and 2) with a low morbidity [31, 32]. The risk of recurrence was reported to be similar according to Simpson grade 1 or 2 resection of convexity meningiomas but higher for incomplete resection [33] and residual tumor and atypical histology are accepted risk factors for recurrent disease [14]. If the majority of the higher grade meningiomas are convexity-based and they could all be completely resected, then we would conclude that the surgery alone should be sufficient to cure all patients harbouring convexity meningiomas. However, while some authors analysed convexity and parasagittal meningioma together as one single entity [21, 25] we have separated parasagittal meningiomas from all other meningiomas at the convexity, because they frequently invade the sinus, rendering complete resection impossible with posteriorly located tumors. Although different strategies with complete removal of parasagittal meningiomas including the sinus are described [34-36] in a number of cases we (and others) feel that it is better to be more conservative and leave a patent sagittal sinus intact [37, 38].
Alvernia et al. [39] studied recurrence factors with special emphasis on the cleavage plane in a series of 100 consecutive patients with convexity meningiomas. They found that pial and vascular invasion affected the recurrence rate in convexity meningioma surgery. Another important finding of asymptomatic meningiomas was demonstrated in a study by Jadid et al. who observed meningioma growth over a more than 10 year period in more than 35% of patients with incidentally diagnosed asymptomatic meningiomas [40]. The growth rates were similar in smaller (<2 cm) and larger tumors, while calcified tumors grew at a lower rate. The latter difference was, however, not statistically significant [40].
In contrast to the feasibility of a gross total resection of a convexity meningiomas, microsurgical resection of skull base meningiomas, e.g. cavernous sinus or petroclival meningiomas, is associated with higher morbidity and mortality. Therefore a less aggressive approach was suggested by many experienced surgeons [5, 8, 41] and a subtotal removal followed by watch and scan or radiation therapy (radiosurgery or stereotactic fractionated radiotherapy) has been recommended to improve functional outcome [41-46]. This is warranted not only because of the high surgical morbidity but also because skull base meningiomas are less likely to be WHO grade II or III meningiomas as indicated by this study and others [26, 47-50].
Like in many other studies, in the present cohort the recurrence rate was significantly higher in WHO grade II patients compared to WHO grade I patients [10, 51, 52], which has prompted many surgeons to refer patients with WHO grade II tumors for fractionated stereotactic radiotherapy or radiosurgery. While many authors report prolonged progression free survival or long term survival after surgery alone [11, 15, 53, 54] the benefit of adjuvant radiotherapy is still being debated for atypical meningioma patients [55]. A currently recruiting study (ROAM/EORTC-1308 trial) will improve scientific evidence on, whether radiotherapy following WHO grade II meningioma resection prolongs recurrence free survival [56].
Our second major finding here is, that WHO grade II and III meningiomas were significantly more frequent in the younger age group (20–40 years) compared to older age groups. Confirming data derived from previous studies [30, 47]. However, age was not a significant predictor of grade II meningiomas in a recently published study by Magill et al. [25].
We found no gender associated correlation with respect to atypical or malignant meningioma grading. Contrary to our data, grade II and III meningiomas have been reported to be significantly more frequent in (young) men in a variety of studies [1, 25, 28, 30, 47]. Epidemiological studies described only a slight male predominance and age-specific incidence rates revealed increasing risk with age in both men and women for atypical and malignant meningiomas [1].
Our third major finding is that larger tumors are significantly more often diagnosed as grade II tumors. Other authors have reported similar data and concluded that tumor volume was a robust pre-operative indicator of higher-grade meningioma [21, 25]. Magill et al. also found that atypical meningioma was significantly related to meningioma size in univariate and multivariate analysis. The size of 3.2 cm was identified as a cut-off point carrying the risk of being an atypical meningioma [25]. A recent study found that 20% of giant meningiomas were WHO grade II or III meningiomas and tumor location also influenced recurrence-free survival [57]. Hale et al. found that tumor volume was the most robust predictor of a higher grade meningioma [21].
The forth finding is, that meningiomas with extended peritumoral edema were significantly more frequently classified as WHO grade II tumors. Peritumoral edema was a predictor for atypical meningiomas and the degree of edema was positively correlated with higher grade along with tumor necrosis and a draining vein [21]. Including MRI and demographic variables of patients with intracranial meningiomas (tumor volume, degree of peritumoral edema, presence of necrosis, tumor location patients sex and presence of draining vein) machine learning algorithms can be developed to predict meningioma grade with great accuracy [22].
Beside tumor size, location and extent of resection, obviously there are other factors that may influence the biological behaviour of the meningioma. Recently DNA methylation profiling added complementary information to known chromosomal rearrangements that are associated with tumor grades and showed that even some WHO I meningioma can have a high tendency to recur, while on the other side WHO grade III meningioma may display a more benign course than expected [58, 59]. These findings may even lead to another modification of the WHO classification in the future, to one based on molecular genetics. Furthermore, in addition to established mutations in the NF2 gene in meningioma patients, more recently mutations have been found in TRAF7, SMO, KLF4, PI3K and AKT1 [60, 61]. Multiple independent groups have shown that TERT promoter mutations are associated with shorter time to recurrence, survival, and overall poor prognosis [62-65]. While all these molecular factors have not been evaluated for the current data set yet, we have considered methylation profiling in selected cases where difficult therapeutic decisions have to be made during follow-up.
Limitations of the study
We are aware of the primary limitation of the study being retrospective and having included a limited number of patients, especially with respect to meningiomas of higher grades and their follow up. Also, DNA methylation based or molecular diagnostic was not performed on a routine basis, such data would be useful in future studies.
Conclusion
In our series, atypical histology of meningioma was associated with younger age, location on the convexity, larger tumor size and lager peritumoral edema. This might influence patient counselling regarding surgical therapy, especially in incidentally diagnosed convexity meningiomas in younger patients.
Abbreviations
- WHO:
-
World Health Organization
- CSF:
-
Cerebrospinal fluid
- GTR:
-
Gross total resection
- MRI:
-
Magnetic resonance imaging
- mRS:
-
Modified Rankin Scale
- RS:
-
Radiosurgery
- fSRT:
-
Fractionated stereotactic radiotherapy
References
Wiemels J, Wrensch M, Claus EB (2010) Epidemiology and etiology of meningioma. J Neurooncol 99:307–314. https://doi.org/10.1007/s11060-010-0386-3
Davis FG, Kupelian V, Freels S, McCarthy B, Surawicz T (2001) Prevalence estimates for primary brain tumors in the United States by behavior and major histology groups. Neuro-oncology 3:152–158. https://doi.org/10.1093/neuonc/3.3.152
Porter KR, McCarthy BJ, Freels S, Kim Y, Davis FG (2010) Prevalence estimates for primary brain tumors in the United States by age, gender, behavior, and histology. Neuro-oncology 12:520–527. https://doi.org/10.1093/neuonc/nop066
Baldi I, Engelhardt J, Bonnet C, Bauchet L, Berteaud E, Gruber A, Loiseau H (2014) Epidemiology of meningiomas. Neurochirurgie. https://doi.org/10.1016/j.neuchi.2014.05.006
Seifert V (2010) Clinical management of petroclival meningiomas and the eternal quest for preservation of quality of life: personal experiences over a period of 20 years. Acta Neurochir 152:1099–1116. https://doi.org/10.1007/s00701-010-0633-6
Jung HW, Yoo H, Paek SH, Choi KS (2000) Long-term outcome and growth rate of subtotally resected petroclival meningiomas: experience with 38 cases. Neurosurgery 46(3), 567–574, (discussion 574–565)
Couldwell WT, Kan P, Liu JK, Apfelbaum RI (2006) Decompression of cavernous sinus meningioma for preservation and improvement of cranial nerve function. Technical note. J Neurosurg 105:148–152. https://doi.org/10.3171/jns.2006.105.1.148
Gozal YM, Alzhrani G, Abou-Al-Shaar H, Azab MA, Walsh MT, Couldwell WT (2019) Outcomes of decompressive surgery for cavernous sinus meningiomas: long-term follow-up in 50 patients. J Neurosurg. https://doi.org/10.3171/2018.10.Jns181480
Karsy M, Jensen MR, Guan J, Ravindra VM, Bisson EF, Couldwell WT (2019) EQ-5D quality-of-life analysis and cost-effectiveness after skull base meningioma resection. Neurosurgery. https://doi.org/10.1093/neuros/nyz040
Jenkinson MD, Weber DC, Haylock BJ, Mallucci CL, Zakaria R, Javadpour M (2015) Atypical meningoma: current management dilemmas and prospective clinical trials. J Neurooncol 121:1–7. https://doi.org/10.1007/s11060-014-1620-1
Aghi MK, Carter BS, Cosgrove GR, Ojemann RG, Amin-Hanjani S, Martuza RL, Curry WT, Jr., Barker FG (2009) Long-term recurrence rates of atypical meningiomas after gross total resection with or without postoperative adjuvant radiation. Neurosurgery 64(1), 56–60, (discussion 60)
Jo K, Park HJ, Nam DH, Lee JI, Kong DS, Park K, Kim JH (2010) Treatment of atypical meningioma. J Clin Neurosci 17:1362–1366. https://doi.org/10.1016/j.jocn.2010.03.036
Rogers L, Gilbert M, Vogelbaum MA (2010) Intracranial meningiomas of atypical (WHO grade II) histology. J Neurooncol 99:393–405. https://doi.org/10.1007/s11060-010-0343-1
Gousias K, Schramm J, Simon M (2016) The Simpson grading revisited: aggressive surgery and its place in modern meningioma management. J Neurosurg 125:551–560. https://doi.org/10.3171/2015.9.Jns15754
Adeberg S, Hartmann C, Welzel T, Rieken S, Habermehl D, von Deimling A, Debus J, Combs SE (2012) Long-term outcome after radiotherapy in patients with atypical and malignant meningiomas–clinical results in 85 patients treated in a single institution leading to optimized guidelines for early radiation therapy. Int J Radiat Oncol Biol Phys 83:859–864. https://doi.org/10.1016/j.ijrobp.2011.08.010
Pearson BE, Markert JM, Fisher WS, Guthrie BL, Fiveash JB, Palmer CA, Riley K (2008) Hitting a moving target: evolution of a treatment paradigm for atypical meningiomas amid changing diagnostic criteria. Neurosurg Focus 24:E3. https://doi.org/10.3171/foc/2008/24/5/e3
Backer-Grondahl T, Moen BH, Arnli MB, Torseth K, Torp SH (2014) Immunohistochemical characterization of brain-invasive meningiomas. Int J Clin Exp Pathol 7:7206–7219
Backer-Grondahl T, Moen BH, Torp SH (2012) The histopathological spectrum of human meningiomas. Int J Clin Exp Pathol 5:231–242
Willis J, Smith C, Ironside JW, Erridge S, Whittle IR, Everington D (2005) The accuracy of meningioma grading: a 10-year retrospective audit. Neuropathol Appl Neurobiol 31:141–149. https://doi.org/10.1111/j.1365-2990.2004.00621.x
Simpson D (1957) The recurrence of intracranial meningiomas after surgical treatment. J Neurol Neurosurg Psychiatry 20:22–39
Hale AT, Wang L, Strother MK, Chambless LB (2018) Differentiating meningioma grade by imaging features on magnetic resonance imaging. J Clin Neurosci 48:71–75. https://doi.org/10.1016/j.jocn.2017.11.013
Hale AT, Stonko DP, Wang L, Strother MK, Chambless LB (2018) Machine learning analyses can differentiate meningioma grade by features on magnetic resonance imaging. Neurosurg Focus 45:E4. https://doi.org/10.3171/2018.8.Focus18191
Goldbrunner R, Minniti G, Preusser M, Jenkinson MD, Sallabanda K, Houdart E, von Deimling A, Stavrinou P, Lefranc F, Lund-Johansen M, Moyal EC, Brandsma D, Henriksson R, Soffietti R, Weller M (2016) EANO guidelines for the diagnosis and treatment of meningiomas. Lancet Oncol 17:e383–391. https://doi.org/10.1016/s1470-2045(16)30321-7
Nowak A, Dziedzic T, Krych P, Czernicki T, Kunert P, Marchel A (2015) Benign versus atypical meningiomas: risk factors predicting recurrence. Neurol Neurochir Pol 49:1–10. https://doi.org/10.1016/j.pjnns.2014.11.003
Magill ST, Young JS, Chae R, Aghi MK, Theodosopoulos PV, McDermott MW (2018) Relationship between tumor location, size, and WHO grade in meningioma. Neurosurg Focus 44:E4. https://doi.org/10.3171/2018.1.Focus17752
Sade B, Chahlavi A, Krishnaney A, Nagel S, Choi E, Lee JH (2007) World Health Organization grades II and III meningiomas are rare in the cranial base and spine. Neurosurgery 61(6), 1194–1198.https://doi.org/10.1227/01.neu.0000306097.38141.65, (discussion 1198)
Couldwell WT, MacDonald JD, Taussky P (2014) Complete resection of the cavernous sinus-indications and technique. World Neurosurg 82:1264–1270. https://doi.org/10.1016/j.wneu.2013.08.026
Liang RF, Xiu YJ, Wang X, Li M, Yang Y, Mao Q, Liu YH (2014) The potential risk factors for atypical and anaplastic meningiomas: clinical series of 1239 cases. Int J Clin Exp Med 7:5696–5700
Champeaux C, Weller J, Katsahian S (2019) Epidemiology of meningiomas. A nationwide study of surgically treated tumours on French medico-administrative data. Cancer Epidemiol 58:63–70. https://doi.org/10.1016/j.canep.2018.11.004
Wang DJ, Xie Q, Gong Y, Mao Y, Wang Y, Cheng HX, Zhong P, Che XM, Jiang CC, Huang FP, Zheng K, Li SQ, Gu YX, Bao WM, Yang BJ, Wu JS, Xie LQ, Zheng MZ, Tang HL, Zhu HD, Chen XC, Zhou LF (2013) Histopathological classification and location of consecutively operated meningiomas at a single institution in China from 2001 to 2010. Chin Med J 126:488–493
Sanai N, Sughrue ME, Shangari G, Chung K, Berger MS, McDermott MW (2010) Risk profile associated with convexity meningioma resection in the modern neurosurgical era. J Neurosurg 112:913–919. https://doi.org/10.3171/2009.6.Jns081490
Reinert M, Babey M, Curschmann J, Vajtai I, Seiler RW, Mariani L (2006) Morbidity in 201 patients with small sized meningioma treated by microsurgery. Acta Neurochir 148(12), 1257–1265. https://doi.org/10.1007/s00701-006-0909-z, ( discussion 1266)
Voss KM, Spille DC, Sauerland C, Suero Molina E, Brokinkel C, Paulus W, Stummer W, Holling M, Jeibmann A, Brokinkel B (2017) The Simpson grading in meningioma surgery: does the tumor location influence the prognostic value? J Neurooncol 133:641–651. https://doi.org/10.1007/s11060-017-2481-1
Sindou M (2001) Meningiomas invading the sagittal or transverse sinuses, resection with venous reconstruction. J Clin Neurosci 8(Suppl 1):8–11. https://doi.org/10.1054/jocn.2001.0868
Sindou M (2014) Meningiomas involving major dural sinuses: should we attempt at radical removal and venous repair? World Neurosurg 81:46–47. https://doi.org/10.1016/j.wneu.2013.07.119
Sindou M, Hallacq P (1998) Venous reconstruction in surgery of meningiomas invading the sagittal and transverse sinuses. Skull Base Surg 8:57–64
Caroli E, Orlando ER, Mastronardi L, Ferrante L (2006) Meningiomas infiltrating the superior sagittal sinus: surgical considerations of 328 cases. Neurosurg Rev 29:236–241. https://doi.org/10.1007/s10143-006-0020-1
Tomasello F, Conti A, Cardali S, Angileri FF (2013) Venous preservation-guided resection: a changing paradigm in parasagittal meningioma surgery. J Neurosurg 119:74–81. https://doi.org/10.3171/2012.11.jns112011
Alvernia JE, Dang ND, Sindou MP (2011) Convexity meningiomas: study of recurrence factors with special emphasis on the cleavage plane in a series of 100 consecutive patients. J Neurosurg 115:491–498. https://doi.org/10.3171/2011.4.jns101922
Jadid KD, Feychting M, Hoijer J, Hylin S, Kihlstrom L, Mathiesen T (2015) Long-term follow-up of incidentally discovered meningiomas. Acta Neurochir 157:225–230. https://doi.org/10.1007/s00701-014-2306-3
Sindou M, Nebbal M, Guclu B (2015) Cavernous sinus meningiomas: imaging and surgical strategy. Adv Tech Stand Neurosurg 42:103–121. https://doi.org/10.1007/978-3-319-09066-5_6
Schmieder K, Engelhardt M, Wawrzyniak S, Borger S, Becker K, Zimolong A (2010) The impact of microsurgery, stereotactic radiosurgery and radiotherapy in the treatment of meningiomas depending on different localizations. GMS Health Technol Assess. https://doi.org/10.3205/hta000080
Hamm K, Henzel M, Gross MW, Surber G, Kleinert G, Engenhart-Cabillic R (2008) Radiosurgery/stereotactic radiotherapy in the therapeutical concept for skull base meningiomas. Zentralbl Neurochir 69:14–21. https://doi.org/10.1055/s-2007-992138
Combs SE, Ganswindt U, Foote RL, Kondziolka D, Tonn JC (2012) State-of-the-art treatment alternatives for base of skull meningiomas: complementing and controversial indications for neurosurgery, stereotactic and robotic based radiosurgery or modern fractionated radiation techniques. Radiat Oncol 7:226. https://doi.org/10.1186/1748-717x-7-226
Sughrue ME, Rutkowski MJ, Aranda D, Barani IJ, McDermott MW, Parsa AT (2010) Factors affecting outcome following treatment of patients with cavernous sinus meningiomas. J Neurosurg 113:1087–1092. https://doi.org/10.3171/2010.3.jns091807
Cohen-Inbar O, Lee CC, Schlesinger D, Xu Z, Sheehan JP (2015) Long-term results of stereotactic radiosurgery for skull base meningiomas. Neurosurgery. https://doi.org/10.1227/neu.0000000000001045
Zhou P, Ma W, Yin S, Li Y, Jiang S (2013) Three risk factors for WHO grade II and III meningiomas: a study of 1737 cases from a single center. Neurol India 61:40–44. https://doi.org/10.4103/0028-3886.107928
Kane AJ, Sughrue ME, Rutkowski MJ, Shangari G, Fang S, McDermott MW, Berger MS, Parsa AT (2011) Anatomic location is a risk factor for atypical and malignant meningiomas. Cancer 117:1272–1278. https://doi.org/10.1002/cncr.25591
Mahmood A, Caccamo DV, Tomecek FJ, Malik GM (1993) Atypical and malignant meningiomas: a clinicopathological review. Neurosurgery 33:955–963
Maier H, Ofner D, Hittmair A, Kitz K, Budka H (1992) Classic, atypical, and anaplastic meningioma: three histopathological subtypes of clinical relevance. J Neurosurg 77:616–623. https://doi.org/10.3171/jns.1992.77.4.0616
Zaher A, Abdelbari Mattar M, Zayed DH, Ellatif RA, Ashamallah SA (2013) Atypical meningioma: a study of prognostic factors. World Neurosurg 80:549–553. https://doi.org/10.1016/j.wneu.2013.07.001
Budohoski KP, Clerkin J, Millward CP, O'Halloran PJ, Waqar M, Looby S, Young AMH, Guilfoyle MR, Fitzroll D, Devadass A, Allinson K, Farrell M, Javadpour M, Jenkinson MD, Santarius T, Kirollos RW (2018) Predictors of early progression of surgically treated atypical meningiomas. Acta Neurochir 160:1813–1822. https://doi.org/10.1007/s00701-018-3593-x
Aboukais R, Baroncini M, Zairi F, Reyns N, Lejeune JP (2013) Early postoperative radiotherapy improves progression free survival in patients with grade 2 meningioma. Acta Neurochir 155(8), 1385–1390. https://doi.org/10.1007/s00701-013-1775-0, (discussion 1390)
Bagshaw HP, Burt LM, Jensen RL, Suneja G, Palmer CA, Couldwell WT, Shrieve DC (2017) Adjuvant radiotherapy for atypical meningiomas. J Neurosurg 126:1822–1828. https://doi.org/10.3171/2016.5.Jns152809
Hasan S, Young M, Albert T, Shah AH, Okoye C, Bregy A, Lo SS, Ishkanian F, Komotar RJ (2014) The role of adjuvant radiotherapy following gross total resection of atypical meningiomas. World Neurosurg. https://doi.org/10.1016/j.wneu.2014.12.037
Jenkinson MD, Javadpour M, Haylock BJ, Young B, Gillard H, Vinten J, Bulbeck H, Das K, Farrell M, Looby S, Hickey H, Preusser M, Mallucci CL, Hughes D, Gamble C, Weber DC (2015) The ROAM/EORTC-1308 trial: radiation versus observation following surgical resection of atypical meningioma: study protocol for a randomised controlled trial. Trials 16:519. https://doi.org/10.1186/s13063-015-1040-3
Narayan V, Bir SC, Mohammed N, Savardekar AR, Patra DP, Nanda A (2018) Surgical management of giant intracranial meningioma: operative nuances, challenges, and outcome. World Neurosurg 110:e32–e41. https://doi.org/10.1016/j.wneu.2017.09.184
Sahm F, Schrimpf D, Stichel D, Jones DTW, Hielscher T, Schefzyk S, Okonechnikov K, Koelsche C, Reuss DE, Capper D, Sturm D, Wirsching HG, Berghoff AS, Baumgarten P, Kratz A, Huang K, Wefers AK, Hovestadt V, Sill M, Ellis HP, Kurian KM, Okuducu AF, Jungk C, Drueschler K, Schick M, Bewerunge-Hudler M, Mawrin C, Seiz-Rosenhagen M, Ketter R, Simon M, Westphal M, Lamszus K, Becker A, Koch A, Schittenhelm J, Rushing EJ, Collins VP, Brehmer S, Chavez L, Platten M, Hanggi D, Unterberg A, Paulus W, Wick W, Pfister SM, Mittelbronn M, Preusser M, Herold-Mende C, Weller M, von Deimling A (2017) DNA methylation-based classification and grading system for meningioma: a multicentre, retrospective analysis. Lancet Oncol 18:682–694. https://doi.org/10.1016/s1470-2045(17)30155-9
Bi WL, Zhang M, Wu WW, Mei Y, Dunn IF (2016) Meningioma genomics: diagnostic, prognostic, and therapeutic applications. Front Surg 3:40. https://doi.org/10.3389/fsurg.2016.00040
Abedalthagafi M, Bi WL, Aizer AA, Merrill PH, Brewster R, Agarwalla PK, Listewnik ML, Dias-Santagata D, Thorner AR, Van Hummelen P, Brastianos PK, Reardon DA, Wen PY, Al-Mefty O, Ramkissoon SH, Folkerth RD, Ligon KL, Ligon AH, Alexander BM, Dunn IF, Beroukhim R, Santagata S (2016) Oncogenic PI3K mutations are as common as AKT1 and SMO mutations in meningioma. Neuro-oncology 18:649–655. https://doi.org/10.1093/neuonc/nov316
Clark VE, Erson-Omay EZ, Serin A, Yin J, Cotney J, Ozduman K, Avsar T, Li J, Murray PB, Henegariu O, Yilmaz S, Gunel JM, Carrion-Grant G, Yilmaz B, Grady C, Tanrikulu B, Bakircioglu M, Kaymakcalan H, Caglayan AO, Sencar L, Ceyhun E, Atik AF, Bayri Y, Bai H, Kolb LE, Hebert RM, Omay SB, Mishra-Gorur K, Choi M, Overton JD, Holland EC, Mane S, State MW, Bilguvar K, Baehring JM, Gutin PH, Piepmeier JM, Vortmeyer A, Brennan CW, Pamir MN, Kilic T, Lifton RP, Noonan JP, Yasuno K, Gunel M (2013) Genomic analysis of non-NF2 meningiomas reveals mutations in TRAF7, KLF4, AKT1, and SMO. Science 339:1077–1080. https://doi.org/10.1126/science.1233009
Abedalthagafi MS, Bi WL, Merrill PH, Gibson WJ, Rose MF, Du Z, Francis JM, Du R, Dunn IF, Ligon AH, Beroukhim R, Santagata S (2015) ARID1A and TERT promoter mutations in dedifferentiated meningioma. Cancer Genetics 208:345–350. https://doi.org/10.1016/j.cancergen.2015.03.005
Furtjes G, Kochling M, Peetz-Dienhart S, Wagner A, Hess K, Hasselblatt M, Senner V, Stummer W, Paulus W, Brokinkel B (2016) hTERT promoter methylation in meningiomas and central nervous hemangiopericytomas. J Neurooncol 130:79–87. https://doi.org/10.1007/s11060-016-2226-6
Goutagny S, Nault JC, Mallet M, Henin D, Rossi JZ, Kalamarides M (2014) High incidence of activating TERT promoter mutations in meningiomas undergoing malignant progression. Brain Pathol 24:184–189. https://doi.org/10.1111/bpa.12110
Sahm F, Schrimpf D, Olar A, Koelsche C, Reuss D, Bissel J, Kratz A, Capper D, Schefzyk S, Hielscher T, Wang Q, Sulman EP, Adeberg S, Koch A, Okuducu AF, Brehmer S, Schittenhelm J, Becker A, Brokinkel B, Schmidt M, Ull T, Gousias K, Kessler AF, Lamszus K, Debus J, Mawrin C, Kim YJ, Simon M, Ketter R, Paulus W, Aldape KD, Herold-Mende C, von Deimling A (2016) TERT Promoter Mutations and Risk of Recurrence in Meningioma. J Natl Cancer Inst. https://doi.org/10.1093/jnci/djv377
Acknowledgement
The authors are grateful to Dr. Hanns Ackermann, Goethe University Frankfurt/ Main, Germany for his support and counselling of statistical tests. We thank Dr. Charles L. Rosen, M.D., PhD. for his editorial assistance.
Funding
No funding was received for this research.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
All authors certify that they have no affiliations with or involvement in any organization or entity with any financial interest (such as honoraria; educational grants; participation in speakers' bureaus; membership, employment, consultancies, stock ownership, or other equity interest; and expert testimony or patent-licensing arrangements), or non-financial interest (such as personal or professional relationships, affiliations, knowledge or beliefs) in the subject matter or materials discussed in this manuscript.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed consent
For this type of study formal consent is not required.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Ressel, A., Fichte, S., Brodhun, M. et al. WHO grade of intracranial meningiomas differs with respect to patient’s age, location, tumor size and peritumoral edema. J Neurooncol 145, 277–286 (2019). https://doi.org/10.1007/s11060-019-03293-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11060-019-03293-x