
Abstract
Introduction
For children with central nervous system (CNS) tumors, survival rates remain significantly lower than other childhood malignancies with a substantial increase in disability of survivors. Given this, it is imperative that these children are identified at the earliest sign of symptom onset. Our institution aimed to identify diagnostic delays, morbidity and mortality, and specific barriers that may exist within our specific healthcare system that result in diagnostic delay.
Methods
A retrospective chart review was performed of newly diagnosed CNS tumors between January 1, 2008 and December 31, 2017.
Results
235 patient cases were reviewed, 34 (14.5%) of which had an associated tumor predisposition syndrome. Median age at the time of diagnosis was 9 years (range 1 day to 25 years), with median number of days from symptom onset to definitive diagnosis of 42 days (interquartile range 14–120 days). Delays longer than 60 days occurred in 95 (47.5%) patients. The 10 year relative survival rate for all tumors was 86.8%.
Conclusions
Our institution had a shorter interval from symptom onset to diagnosis than currently reported in the literature, as well as a decrease in associated morbidity. In addition, for those with longer delays, we were able to characterize the etiology and barriers leading to these delays. With these identified, we are able to utilize this knowledge to further improve education and awareness in community members and healthcare professionals to continue to improve the time to diagnosis in the future.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
Introduction
Central nervous system (CNS) tumors, the 2nd most common cancer diagnosed in children after acute leukemia, accounts for 20% of pediatric malignancies [1]. Annual incidence in the United States (US) is 5.65 cases per 100,000, with 3720 new cases expected to be diagnosed in 2019 [2]. Even with an increase in the 5-year relative survival rate (RSR) to 74.1%, CNS tumors have surpassed acute leukemia as the leading cause of cancer-related death in children [2, 3]. Given that children with CNS tumors present with nonspecific symptomatology, delays in diagnosis can occur, contributing to morbidity and mortality. In 2012, a study conducted at a children’s hospital in Israel, reviewed cases for unacceptable delays in diagnosis. Unacceptable delay was considered if patients were presenting with neurological deterioration that did not receive proper medical attention, had repeated physician visits without adequate attention, or presence of classical symptoms of increased intracranial pressure (iICP) which did not lead to brain imaging. Average diagnosis time was 7.7 months, with an unacceptable delay in 27% of the children [4]. A German study noted a similar delay, identifying headache as the most common presenting symptom [5].
There is also an effort to assess the number of health care provider (HCP) visits prior to diagnosis. A combined retrospective and prospective study of 104 pediatric patients with brain tumors was conducted in Eastern Canada from 1995 to 2000. They identified that 58% of patients required four or more visits to a physician before an accurate diagnosis was established, with 30% requiring seven or more visits [6].
In the US, Nationwide Children’s Hospital piloted an Ohio-based study to identify the time interval between symptom onset and definitive diagnosis in children with newly-diagnosed CNS tumors presenting to a children’s hospital. Of the 146 patient cases reviewed, the median time interval was 42 days [7]. Our institution undertook a contemporaneous study in a different pediatric referral center to determine time of symptom onset and diagnosis for children with CNS tumors.
Materials and methods
This study, based off the HeadSmart study that was validated in the United Kingdom (UK), was conducted as a single site retrospective records review utilizing a convenience sample [8].
Patients
After obtaining institutional review board (IRB) approval, a retrospective chart review was conducted of all patients with CNS tumors diagnosed at Akron Children’s Hospital (ACH), between January 1, 2008 and December 31, 2017. Exclusion criteria included patients treated at ACH who were diagnosed at other institutions (n = 2), and patients with tumors located in or in close proximity to the CNS that were not primary CNS tumors [dermoid cyst (n = 1), lipoma (n = 1), neurothekeoma (n = 1), pineocytoma (n = 1), and pituitary adenoma (n = 2)].
Methods
Data was collected by medical chart review, including: history and physical (H&P) note, emergency department (ED) visit note, and any consult or progress notes from a primary care provider (PCP) or subspecialist 1 year prior to date of first presentation. Additional data collected: age at and year of diagnosis, gender, race, zip code, PCP, tumor type/location per pathology and radiology reports, presenting symptoms, total number of healthcare provider (HCP) visits, total diagnostic interval (TDI), any associated tumor predisposition syndrome (TPS), and outcome (alive or deceased). Of the above data, zip code and PCP were added in order to better identify potential barriers in delay, and whether these were geographical in nature. Total number of ED visits was defined as a visit to either an ED or urgent care, while total number of HCP visits was defined as any visit to the patients’ PCP, an advanced practice provider (APP), ED, or subspecialist; both from symptom onset to definitive diagnosis. TDI was defined as the number of days from the onset of symptoms to imaging diagnosis, which includes patient interval [the time point when patients first note symptoms (date of first symptom)] and diagnostic interval [the time point of patients’ first presentation to a provider to date of diagnosis (date of admission to the hospital because of malignancy)] [9].
Statistics
Analysis began with examination and description of data, with stratifications by TPS, consisting of full summary statistics and distributional assessments for continuous data and frequencies/proportions for categorical data. Primary analyses were descriptive. Exploratory analyses included a comparison of baseline demographics to determine group comparability followed by a comparison of clinical characteristics. Statistical testing included the Wilcoxon Rank Sum Test for non-normally distributed discrete and continuous data, the χ2 Test of Independence (or Fisher’s Exact Test for cell counts of n < 5) for categorical data, the Kruskal–Wallis Test for independent variables on a continuous or ordinal dependent variable, and the Dwass, Steel, Critchlow–Fligner (DSCF) Test for multiple comparisons based on pairwise rankings.
Statistical analyses were completed using SAS 9.4/14.2©. Unless otherwise noted, all testing was two-tailed and evaluated at the Type I Error Rate of alpha = 0.05 level of statistical significance.
Results
Patient characteristics
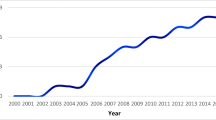
Over the 10 year span of the study, 243 patient cases were identified from the institutional oncology registry; 235 that were eligible for further evaluation (Fig. 1). There was an average of 24 newly diagnosed cases annually (15–32 cases per year). Of the cases reviewed, 127 (54.0%) were male and 108 (46.0%) were female. Predominant race was Caucasian (202; 86.0%), followed by African American (24; 10.2%), Hispanic (5; 2.1%), Asian (3; 1.3%), and self-identified “other” (1; 0.4%).

Flowchart of all patients
Median (IQR) age at diagnosis was 9 years (4.0–14.0) with a range of 1 day to 25 years. For the purposes of this study, patients were divided into four ordinal categories: 0–4, 5–9, 10–14, and ≥ 15 years of age, with a similar distribution across all age groups (Table 1).
There were 34 (14.5%) patients with a TPS: 27 (79.4%) with neurofibromatosis type 1 (NF1), 3 (8.8%) with neurofibromatosis type 2 (NF2), 3 (8.8%) with tuberous sclerosis (TS) and 1 (2.9%) with Von-Hippel-Lindau (VHL). The cohort did contain patients with other TPS, such as Li-Fraumeni, DICER syndrome, Constitutional Mismatch Repair Syndrome, and germline SMARCB1 and p53 mutations; however, the primary focus of this study was phakomatoses.
Symptomatology
Patients were reported to have 30 different presenting symptoms. The most common presenting symptom was headache (123; 52.3%), followed by nausea/vomiting (84; 35.7%), unsteadiness (58; 24.7%), visual disturbances (56; 22.6%), and abnormal gait (52; 22.1%). Only headache (p = 0.0038) and nausea/vomiting (p ≤ 0.0001) were statistically significant for a dependent relationship with TPS. 69 (29.4%) patients presented with symptoms of iICP at diagnosis, with 29 (42.0%) patients having high grade tumors and 40 (57.9%) patients having low grade tumors. Patients with spinal cord tumors (n = 12) had a different set of presenting symptoms, corresponding to tumor location, including pain (9; 75%) and weakness/numbness (8; 67%). Complete symptomatology is summarized in Table 2.
As patients with phakomatoses are at increased risk for CNS tumors, the American Academy of Pediatrics, International Tuberous Sclerosis Complex Consensus Group, and American Association for Cancer Research have published diagnostic guidelines and surveillance recommendations for patients with NF1 or NF2, TS, and VHL, respectively [10,11,12]. Of the 34 patients with these conditions, imaging was obtained for different reasons, by their PCP, geneticist, or oncologist. 19 (56%) patients had imaging per the respective surveillance recommendations, with four patients being followed closely until an increase in tumor size was noted that prompted biopsy or resection. Another 15 patients, in the TPS group, underwent imaging, in addition to the recommended surveillance, for symptoms, such as headaches or vision changes.
Tumor characteristics
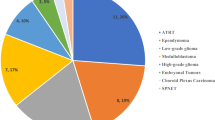
In 2016, the WHO (World Health Organization) classification and grading of CNS tumors was changed to incorporate histological and molecular parameters, in hopes of facilitating clinical, experimental, and epidemiological studies that may lead to advancements in the area of CNS tumors [13]. While many tumor pathology diagnoses in our database were based on the 2007 classification, an effort was made to reclassify using the 2016 classification. In line with national statistics, the most common tumor type was WHO Grade I Astrocytoma, including pilocytic astrocytoma, optic pathway glioma, and subependymal giant cell astrocytoma (SEGA). This accounted for 42% of the patient population.
When evaluating optic pathway gliomas separately, these accounted for approximately 9%, which is expected given the percentage of patients with NF1. Most were diagnosed radiographically and histology was only obtained if concerns were raised based on history and/or atypical imaging findings.
The third most common tumor type was WHO Grade IV Medulloblastoma (17; 7.2%).
Of the 31 deceased patients, 27 (87.1%) had WHO grade III or VI tumors.
In keeping with the reported literature, the most common tumor location was infratentorial, consisting of 55.7% of tumors, followed by supratentorial (92; 39.1%), and spinal cord (12; 5.1%).
Tumor characteristics are summarized in Table 3.
Time to diagnosis
Of all 235 patients, the median (IQR) TDI was 42 days (14–120) with a range of 0–5475 days. 15 patients were listed as having a zero day TDI because their tumor was found incidentally as part of a work up for first syncopal episode, first seizure, or trauma evaluation. As previously discussed, patients with a TPS may be diagnosed with a tumor based on surveillance, thereby making it difficult to identify time to diagnosis. Therefore, these patients were analyzed separately. Of the 201 patients that did not have a TPS, data was available for 200. 95 (47.5%) had a TDI ≥ 60 days, with a median (IQR) of 150 (60–365). Of those 95 patients, 69 (72.6%) had a TDI ≥ 90 days, with majority of these patients having a diagnosis of low grade gliomas. There was no evidence of a significant difference in TDI by WHO tumor grading (p = 0.3406) or a dependent relationship between patients who had a TDI ≥ 60 days and WHO tumor grade (p = 0.2142).
The median TDI for all infratentorial, supratentorial, and spinal cord tumors was 30, 60 and 60 days, respectively. When excluding patients with a TPS, the median TDI was similar with the exception of spinal cord tumors, which was 90 days. There was evidence of a significant difference in TDI by location (p = 0.0202) and age (p = 0.0019). Post hoc pairwise testing using the DSCF Method provides evidence of a significant difference in TDI between supratentorial and infratentorial tumors only (p = 0.0354).
Median (IQR) TDI of the 31 deceased patients was 28 days (1–365), with 10 (32.3%) patients having a TDI ≥ 60 days.
Healthcare provider visits
The number of HCP visits was also reviewed. Of the 201 patients that did not have a TPS, data was available on 200. The average number of visits was 2.4. Amongst these, subspecialty visits occurred in highest frequency, followed by ED visits, then PCP. Subspecialists that patients were seen by prior to diagnosis included neurology, neurosurgery, ophthalmology, orthopedics for gait concerns, endocrinology for symptoms such as growth arrest, and ear, nose and throat for concerns of headaches secondary to sinusitis. The 95 patients that did not have a TPS and had a TDI ≥ 60 days, mean number of visits was slightly higher at 3.4; with visits to PCP and subspecialists also being higher at 0.8 and 1.7, respectively. There was no evidence of a significant difference in number of visits by tumor location or age at diagnosis.
Morbidity and mortality
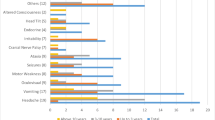
The 10 year RSR for all tumors, malignant and non-malignant tumors was 86.8%, 71.7% and 92%, respectively (p = 0.000059). There was no significant difference in RSR by tumor location (p = 0.06) or age at diagnosis (p = 0.3221) however there was for TDI (p = 0.04). 115 of all 235 (48.9%) patients were reported to have tumor or treatment related complications. These included panhypopituitarism (11; 9.6%), diabetes insipidus (12; 10.4%), hypothyroidism (19; 16.5%), growth hormone deficiency or pubertal delay (32; 27.8%), encephalopathy (4; 3.5%), secondary adrenal insufficiency (15; 13.0%), seizures (18; 15.7%), hearing loss (16; 13.9%), vision changes/loss (19; 16.5%), neurocognitive/neuropsychiatric or neurologic dysfunction (93; 80.9%), mutism (4; 3.5%), and obesity (32; 27.8%).
Discussion and conclusion
Children with CNS tumors often present with nonspecific symptoms that make early diagnosis difficult. Early recognition of characteristic symptoms and the pattern of symptom onset by parents and HCP is crucial in avoiding a diagnostic delay [14, 15]. A systematic review and meta-analysis (1991–2005) identified 56 signs and symptoms with the three most common being headache, nausea and vomiting, and motor abnormality; very similar to our patient population [16]. In addition, while cardinal symptoms of iICP (headache, nausea, and vomiting) may present as waxing and waning symptoms and per Chu et al., become the most common group of presenting features in the final month before diagnosis, only 69 (29.4%) of our patients presented with these at diagnosis [14]. Of those, 40 (57.9%) had low grade tumors. It was also noted that iICP was more likely to occur in patients without TPS.
In comparison to the 2018 CBTRUS report, our patient population has a higher rate of WHO Grade I Astrocytoma (42.1% vs. 15.3%), possibly related to referral bias, reflection of our subspecialties, and favorable tumor location [2]. The large population of NF1 patients (27; 11.5%) likely contributes to the increased number of low grade tumors. In addition, our institution diagnosed patients from 83 of 88 counties in Ohio during this timeframe. We have 36 subspecialties and 111 outreach clinics. This expansive reach of our services lends itself to referral bias.
When evaluating TDI, there are very limited studies in the US and many in countries such as Japan, Germany, Scotland, Switzerland, Israel, and Austria. In the US, the median diagnostic interval ranges from 31 to 42 days, while in Europe and Asia, it ranges from 20.5 days (Japan) to 200 days (Israel) [4,5,6,7, 17,18,19,20,21,22,23,24,25,26]. The UK launched the ‘HeadSmart: Be Brain Tumour Aware’ campaign in 2011, when their average diagnosis time was 13 weeks (91 days). Four years later, it was reduced to 6.7 weeks (47 days) [8]. Our institution found that the median (IQR) TDI was 42 (14–120) and 150 (60–135), in the total patient population and patients without a TPS, respectively. This highlights that while we have been proactive in surveilling patients for CNS tumors in those with a TPS, we have room for improvement in our general population. Though we did find a significant difference in TDI by location and age, we did not by WHO tumor grading. This is likely due to the low number of high grade tumors in our database. In an effort to identify why our patient population had a shorter TDI, we reviewed number of HCP visits prior to diagnosis.
On average, for the patients reviewed, the number of HCP visits was 2.4 Data regarding healthcare visits remains sparse. In addition to the previously mentioned studies in London and Canada, Coven et al. reported an average number of healthcare visits of 2.4 prior to diagnosis, similar to our study [6, 7, 27]. In our review, there was not one variable that had a particular effect on the number of visits.
Many studies have been conducted to understand the relationship between diagnostic delay and overall survival in childhood brain tumors. Similar to our results, these studies suggest that diagnostic delay may not result in decreased survival; however the long term complications can be detrimental. Complications range from chemotherapy related side effects such as cardiac, renal, and reproductive to radiation related side effects such as neurocognitive, endocrine, and neuropsychiatric. A study reviewing 127 patients (Japan) found that symptoms such as visual and endocrinologic problems, along with weakness, tended to persist even after initial treatment. Pre-diagnostic symptom interval of the patients with persistent symptoms was also significantly longer than that of patients whose symptoms had resolved, supporting the hypothesis that though diagnostic delay may not impact overall survival; there may be irreversible damage to neuronal cells resulting in significant morbidity [22]. Childhood brain tumor survivors have also been found to have increased risk of obesity and secondary malignancies depending on treatment regimens. In our cohort, less than half of all patients reported long term complications, with majority being neuroendocrine or neurocognitive in nature. These results are similar or slightly better than those previously reported in the literature, including the 2018 Childhood Cancer Survivorship Study (80.9% vs. 88%) [28,29,30,31,32]. In addition, the 10 year RSR for all malignant and non-malignant tumors was 71.7% and 92%, respectively; similar to the 2018 CBTRUS report (70.7% and 95.5%, respectively) [2]. These results may be due to the high rate of low grade tumors requiring only surgical resection in comparison to high grade tumors requiring radiation and chemotherapy, resulting in these complications.
A significant weakness in our study was record bias. While efforts were made to reduce impact, such as limiting years reviewed to our current electronic medical record system, reviewing both paper and electronic forms of the medical record, and validating diagnoses with the International Classification of Diseases for Oncology (ICD-O) codes, some bias remains due to the inherent nature of a retrospective chart review. Another weakness is location. From 2011 to 2015, for children aged 0–19 years, the average annual age-adjusted incidence rate in Ohio for all CNS tumors was 6.46 per 100,000 (3.91 for malignant and 2.55 for non-malignant).With seven children’s hospitals in Ohio [most states averaging 3 (0–11)], this provides opportunity for patients to present at another institution for initial diagnosis or complete their oncologic care elsewhere.
In summary, our institution had an acceptable TDI, low mortality rate, and comparable morbidity and survival rate, perhaps due to being a referral center as well as availability of general pediatricians and subspecialists in the remote areas of Northeast Ohio that we serve. We establish that stratification of TDI reporting by TPS is imperative and should be a standard for future studies. In a successor study, we plan to expand the TPS reviewed, evaluate each type of interval as per The Aarhus checklist and assess for a change in diagnostic and referral practice over time [9]. Meanwhile, we hope to further improve education and awareness of childhood brain tumors by offering educational seminars for community pediatric providers, as well as student and trainees.
Data availability
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
References
Hastings C, Torkildson JC, Agrawal AK, Children’s Hospital Medical Center (Oakland Calif.) (2012) Handbook of pediatric hematology and oncology: Children’s Hospital & Research Center Oakland. Wiley-Blackwell, Chichester
Ostrom QT, Gittleman H, Truitt G, Boscia A, Kruchko C, Barnholtz-Sloan JS (2018) CBTRUS statistical report: primary brain and other central nervous system tumors diagnosed in the United States in 2011–2015. Neuro Oncol 20:iv1–iv86. https://doi.org/10.1093/neuonc/noy131
Curtin SC, Minino AM, Anderson RN (2016) Declines in cancer death rates among children and adolescents in the United States, 1999–2014. NCHS Data Brief 257:1–8
Shay V, Fattal-Valevski A, Beni-Adani L, Constantini S (2012) Diagnostic delay of pediatric brain tumors in Israel: a retrospective risk factor analysis. Childs Nerv Syst 28:93–100. https://doi.org/10.1007/s00381-011-1564-0
Molineus A, Boxberger N, Redlich A, Vorwerk P (2013) Time to diagnosis of brain tumors in children: a single-centre experience. Pediatr Int 55:305–309. https://doi.org/10.1111/ped.12095
Mehta V, Chapman A, McNeely PD, Walling S, Howes WJ (2002) Latency between symptom onset and diagnosis of pediatric brain tumors: an Eastern Canadian geographic study. Neurosurgery 51:365–372 (Discussion 372–363)
Hollingsworth E, Stanek JR, Finlay JL, Coven SL (2018) Delays in diagnosis for children with newly diagnosed central nervous system tumors. Neuro-Oncol Pract 5:227–233. https://doi.org/10.1093/nop/npy002
Aware HBBT (2016) A new clinical guideline from the Royal College of Paediatrics and Child Health with a national awareness campaign accelerates brain tumor diagnosis in UK children—”HeadSmart: be brain tumour aware”. Neuro Oncol 18:445–454. https://doi.org/10.1093/neuonc/nov187
Weller D, Vedsted P, Rubin G, Walter FM, Emery J, Scott S, Campbell C, Andersen RS, Hamilton W, Olesen F, Rose P, Nafees S, van Rijswijk E, Hiom S, Muth C, Beyer M, Neal RD (2012) The Aarhus statement: improving design and reporting of studies on early cancer diagnosis. Br J Cancer 106:1262–1267. https://doi.org/10.1038/bjc.2012.68
Hersh JH, Genetics AAoPCo (2008) Health supervision for children with neurofibromatosis. Pediatrics 121:633–642. https://doi.org/10.1542/peds.2007-3364
Northrup H, Krueger DA, Group ITSCC (2013) Tuberous sclerosis complex diagnostic criteria update: recommendations of the 2012 International Tuberous Sclerosis Complex Consensus Conference. Pediatr Neurol 49:243–254. https://doi.org/10.1016/j.pediatrneurol.2013.08.001
Rednam SP, Erez A, Druker H, Janeway KA, Kamihara J, Kohlmann WK, Nathanson KL, States LJ, Tomlinson GE, Villani A, Voss SD, Schiffman JD, Wasserman JD (2017) Von Hippel-Lindau and hereditary pheochromocytoma/paraganglioma syndromes: clinical features, genetics, and surveillance recommendations in childhood. Clin Cancer Res 23:e68–e75. https://doi.org/10.1158/1078-0432.CCR-17-0547
Louis DN, Perry A, Reifenberger G, von Deimling A, Figarella-Branger D, Cavenee WK, Ohgaki H, Wiestler OD, Kleihues P, Ellison DW (2016) The 2016 World Health Organization classification of tumors of the central nervous system: a summary. Acta Neuropathol 131:803–820. https://doi.org/10.1007/s00401-016-1545-1
Chu TP, Shah A, Walker D, Coleman MP (2015) Pattern of symptoms and signs of primary intracranial tumours in children and young adults: a record linkage study. Arch Dis Child 100:1115–1122. https://doi.org/10.1136/archdischild-2014-307578
Chu TPC, Shah A, Walker D, Coleman MP (2017) Where are the opportunities for an earlier diagnosis of primary intracranial tumours in children and young adults? Eur J Paediatr Neurol 21:388–395. https://doi.org/10.1016/j.ejpn.2016.10.010
Wilne S, Collier J, Kennedy C, Koller K, Grundy R, Walker D (2007) Presentation of childhood CNS tumours: a systematic review and meta-analysis. Lancet Oncol 8:685–695. https://doi.org/10.1016/S1470-2045(07)70207-3
Hayashi N, Kidokoro H, Miyajima Y, Fukazawa T, Natsume J, Kubota T, Kojima S (2010) How do the clinical features of brain tumours in childhood progress before diagnosis? Brain Dev 32:636–641. https://doi.org/10.1016/j.braindev.2009.10.001
Stocco C, Pilotto C, Passone E, Nocerino A, Tosolini R, Pusiol A, Cogo P (2017) Presentation and symptom interval in children with central nervous system tumors. A single-center experience. Childs Nerv Syst 33:2109–2116. https://doi.org/10.1007/s00381-017-3572-1
Kameda-Smith MM, White MA, St George EJ, Brown JI (2013) Time to diagnosis of paediatric posterior fossa tumours: an 11-year West of Scotland experience 2000–2011. Br J Neurosurg 27:364–369. https://doi.org/10.3109/02688697.2012.741731
Dobrovoljac M, Hengartner H, Boltshauser E, Grotzer MA (2002) Delay in the diagnosis of paediatric brain tumours. Eur J Pediatr 161:663–667. https://doi.org/10.1007/s00431-002-1088-4
Azizi AA, Heßler K, Leiss U, Grylli C, Chocholous M, Peyrl A, Gojo J, Slavc I (2017) From symptom to diagnosis-the prediagnostic symptomatic interval of pediatric central nervous system tumors in Austria. Pediatr Neurol 76:27–36. https://doi.org/10.1016/j.pediatrneurol.2017.08.006
Fukuoka K, Yanagisawa T, Suzuki T, Shirahata M, Adachi JI, Mishima K, Fujimaki T, Matsutani M, Nishikawa R (2014) Duration between onset and diagnosis in central nervous system tumors: impact on prognosis and functional outcome. Pediatr Int 56:829–833. https://doi.org/10.1111/ped.12369
Kukal K, Dobrovoljac M, Boltshauser E, Ammann RA, Grotzer MA (2009) Does diagnostic delay result in decreased survival in paediatric brain tumours? Eur J Pediatr 168:303–310. https://doi.org/10.1007/s00431-008-0755-5
Flores LE, Williams DL, Bell BA, O’Brien M, Ragab AH (1986) Delay in the diagnosis of pediatric brain tumors. Am J Dis Child 140:684–686
Pollock BH, Krischer JP, Vietti TJ (1991) Interval between symptom onset and diagnosis of pediatric solid tumors. J Pediatr 119:725–732
Coven SL, Hollingsworth E, Stanek J, Walker D, Finlay JL (2016) EPI-03: establishing a baseline time-frame for symptom onset to definitive diagnosis of children with newly-diagnosed CNS tumors in Central Ohio. Neuro Oncol 63:S70–S71
Edgeworth J, Bullock P, Bailey A, Gallagher A, Crouchman M (1996) Why are brain tumours still being missed? Arch Dis Child 74:148–151
Foreman NK, Faestel PM, Pearson J, Disabato J, Poole M, Wilkening G, Arenson EB, Greffe B, Thorne R (1999) Health status in 52 long-term survivors of pediatric brain tumors. J Neurooncol 41:47–53
Pietilä S, Mäkipernaa A, Sievänen H, Koivisto AM, Wigren T, Lenko HL (2009) Obesity and metabolic changes are common in young childhood brain tumor survivors. Pediatr Blood Cancer 52:853–859. https://doi.org/10.1002/pbc.21936
Pietilä S, Korpela R, Lenko HL, Haapasalo H, Alalantela R, Nieminen P, Koivisto AM, Mäkipernaa A (2012) Neurological outcome of childhood brain tumor survivors. J Neurooncol 108:153–161. https://doi.org/10.1007/s11060-012-0816-5
Pietilä S, Mäkipernaa A, Koivisto AM, Lenko HL (2017) Growth impairment and gonadal axis abnormalities are common in survivors of paediatric brain tumours. Acta Paediatr 106:1684–1693. https://doi.org/10.1111/apa.13975
Vuotto S, Krull K, Li C, et al (2019) Neurologic morbidities, emotional distress, and functional independence in adult survivors of childhood cancer treated with CNS-directed therapies: a report from the childhood cancer survivor study
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflicts of interest
All authors declare that they have no conflict of interest.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. For this type of study conducted, formal consent is not required.
Informed consent
For this type of study conducted, formal consent is not required.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Patel, V., McNinch, N.L. & Rush, S. Diagnostic delay and morbidity of central nervous system tumors in children and young adults: a pediatric hospital experience. J Neurooncol 143, 297–304 (2019). https://doi.org/10.1007/s11060-019-03160-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11060-019-03160-9